
Abstract
Objective
Hyperacute stroke affects various patient subgroups who may benefit from different management strategies. Magnetic resonance imaging (MRI) quantitative susceptibility mapping (QSM) is a recent MRI technique for measuring deoxyhemoglobin levels. The results of QSM thus have the potential to act as a quantitative biomarker for predicting the success of endovascular interventions.
Methods
Twenty-five patients with M1 occlusions were evaluated retrospectively. QSM measurements were obtained based on susceptibility-weighted imaging sequences from the most prominent veins in each of the four standard regions of interest: the cortical and thalamostriate veins ipsilateral and contralateral to the side of the stroke. The results were analyzed using Wilcoxon’s signed rank test and compared with presenting National Institutes of Health stroke scale (NIHSS) score.
Results
Cortical veins ipsilateral to the stroke showed the greatest elevation in susceptibility compared with all other vein groups. Both ipsilateral and contralateral thalamostriate vein susceptibilities showed strong inverse correlation with presenting NIHSS score.
Conclusion
Thalamostriate vein susceptibility shows a strong inverse correlation with presenting NIHSS in adult patients with hyperacute stroke who are selected for endovascular intervention by advanced imaging.
Keywords
Background
Stroke is the fourth leading cause of death and the leading cause of serious long-term disability in the United States, 1 with approximately 795,000 cases of new or recurrent stroke each year. 1 Computerized tomography examination remains the standard imaging modality for triaging acute ischemic infarcts at many institutions. 2 However, magnetic resonance imaging (MRI) is playing an increasing role in determining if such patients might benefit from endovascular interventions such as mechanical thrombectomy, particularly beyond 6 hours. Recent studies (EXTEND-IA, 3 MR CLEAN, 4 ESCAPE, 5 and SWIFT PRIME 6 ) have demonstrated that mechanical thrombectomy can be highly efficacious compared with intravenous tissue plasminogen activator therapy when patients are screened using imaging biomarkers able to identify at-risk tissue and its viability, such as large-vessel occlusion,3–5 infarct core volume, 3 , 5 and the extent of collateral circulation. 5 However, it is currently not possible to definitively predict a positive response to recanalization among patients with emergent large vessel occlusion (ELVO) or even small-core ELVO.
Susceptibility-weighted imaging (SWI) is a relatively recent MRI sequence with unique characteristics for evaluating cerebral tissue metabolism in patients with acute ischemic stroke. SWI is highly sensitive to paramagnetic substances such as deoxyhemoglobin, which is paramagnetic in contrast to diamagnetic oxyhemoglobin by virtue of its four unpaired electrons. 7 , 8 SWI uses phase difference to enhance the depiction of magnetic susceptibility difference between regions containing paramagnetic substances, such as iron in deoxygenated blood, and the surrounding tissues.7–9 This phase difference is manifested in patients with acute ischemic stroke by increased prominence of the cerebral veins, given that underperfused tissues respond by increasing the percent oxygen extraction from the blood (misery perfusion).10–12 SWI can therefore show the presence or absence of the last physiologic response (increased oxygen extraction fraction) of ischemic tissue before cellular metabolism can no longer be maintained.13–15 Furthermore, increased prominence of the cerebral veins on SWI has been associated with the presence of vigorous collateral flow. 15 These characteristics of SWI suggest that the presence or absence of prominent veins may serve as a valuable biomarker for tissue viability, and may thus indicate the potential benefit to the patient of endovascular revascularization. However, SWI is a qualitative technique and does not provide a quantitative measurement of venous oxygen saturation or deoxyhemoglobin.
Quantitative susceptibility mapping (QSM) 16 was recently developed to quantify the level of deoxyhemoglobin in cerebral veins using various techniques, 17 , 18 notably by using a SWI mapping (SWIM) program. 9 ,19–22 Although subjective SWI findings have been previously associated with National Institutes of Health stroke scale (NIHSS) scores, 15 , 23 QSM offers an objective method for estimating the venous deoxyhemoglobin burden, which is not as subject to interobserver variability. QSM asymmetry in the cortical veins has recently been described in patients with ischemic stroke; 19 however quantitative susceptibility has not yet been characterized in the deep cerebral (thalamostriate veins) veins, which drain the basal ganglia, and has not been correlated with stroke severity.
In this study, we investigated the relationship between quantitative susceptibility in the superficial versus deep cerebral veins and baseline NIHSS scores in patients with hyperacute stroke who were selected for endovascular intervention by advanced imaging.
Materials and methods
Study design
We conducted a retrospective observational cohort study in patients who presented to our institution with hyperacute anterior circulation stroke from 2012 to 2014. Information on patient demographics, side of stroke, initial NIHSS score, clinical covariates, laboratory data, and medications were collected from electronic medical records. QSM was then utilized to assess the relationships between superficial and deep cerebral venous susceptibilities and the patients’ presenting NIHSS scores. This study was approved by the independent institutional review board at Loma Linda University, who waived the need for patient consent.
Patients
Patients with hyperacute stroke who are being considered for mechanical thrombectomy at our institution undergo computed tomography angiography (or magnetic resonance angiography) plus MRI, unless contraindicated (e.g., cardiac pacemaker), under our hyperacute stroke protocol. Among 52 patients with hyperacute stroke who were selected for mechanical thrombectomy from 2010 to 2012, 15 with posterior circulation stroke, four with intracranial hemorrhage, and eight patients with spoiled SWI sequences were excluded. Twenty-five patients with confirmed large-vessel occlusion, small presenting infarct core volume (<70 cc), and NIHSS score ≥8 were included in our cohort.
Magnetic resonance imaging
MRI was performed using a 3T scanner in the axial plane (Siemens Healthcare, Erlangen, Germany). The following sequences were obtained: axial fluid-attenuated inversion recovery, SWI, and diffusion-weighted imaging with apparent diffusion coefficient maps, with or without perfusion. The SWI parameters were as follows: echo time, 20 ms; repetition time, 30 ms; flip angle, 15°; slice thickness, 2 mm; matrix size 256 × 256 mm; and in-plane resolution, 0.5 × 0.5 mm.
SWI maps were created from the magnitude and phase images of the SWI sequence using post-processing software (SPIN, MR Institute of Detroit, MI, USA). Brain extraction was performed using the brain extraction tool with a high-pass filter of 32 × 32. Iterative SWIM was then applied with a k-space threshold of one with three iterations. QSM measurements were obtained from the most prominent vein in each of the four standard regions of interest: the cortical and thalamostriate veins ipsilateral and contralateral to the stroke, respectively. For each measured vein, a linear region of interest was placed along the long axis and the mean susceptibility and standard deviation was calculated from three repeat measurements and recorded in parts per billion (ppb) (Figure 1). All measurements were performed by a medical student research assistant and verified by a fellow within the diagnostic neuroradiology program.
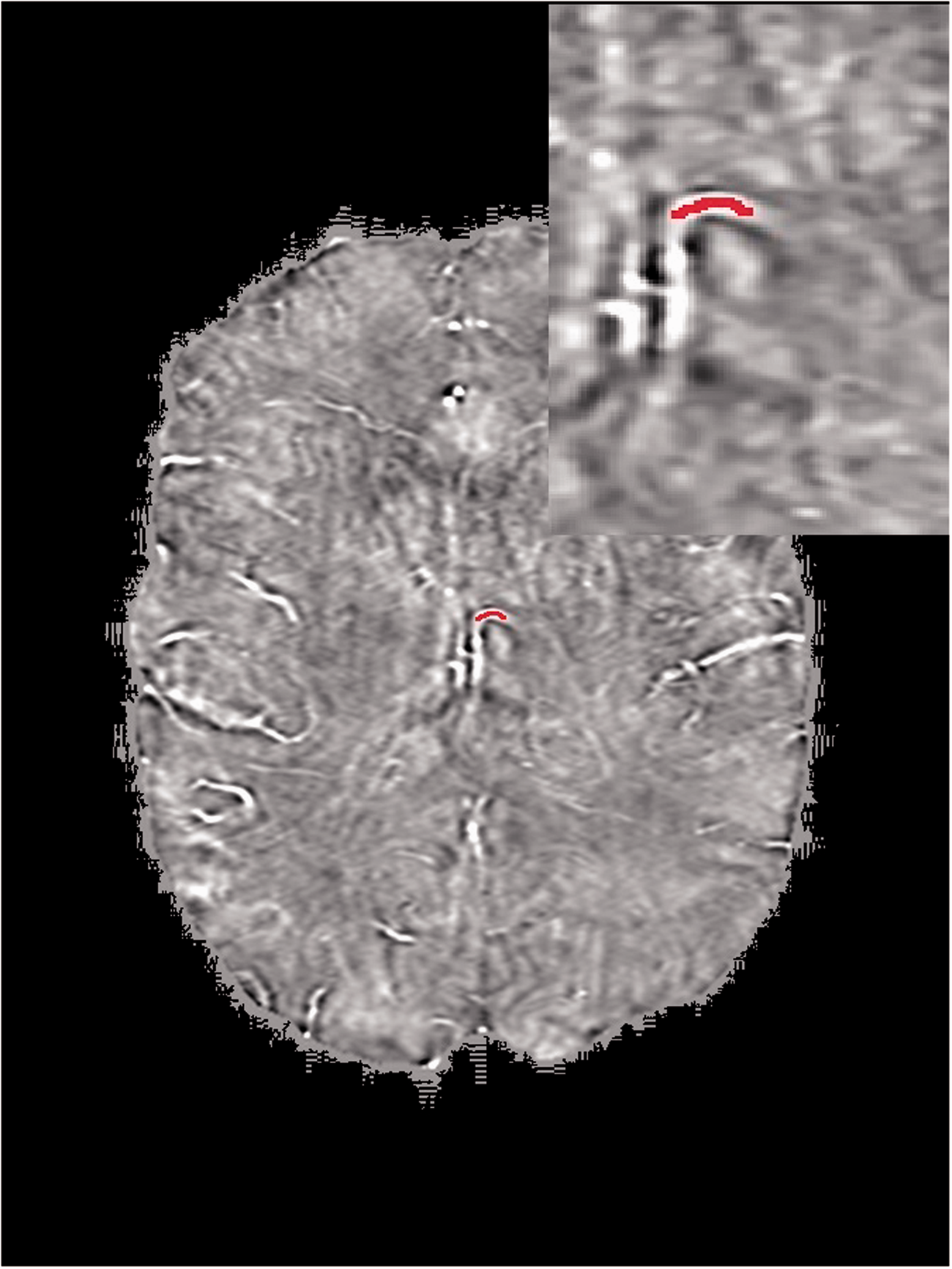
Representative susceptibility-weighted imaging map showing the region of interest (red line) place within the most prominent thalamostriate vein. Inset: magnified region of interest.
Statistical analysis
Pairwise comparisons of mean quantitative susceptibility measurements were made between each venous group using Wilcoxon’s signed rank test. Correlations between susceptibility and presenting NIHSS score were analyzed for each group using Spearman’s rho. Statistical significance was defined as P < 0.05.
Results
Our cohort of 25 patients included 10 men and 15 women, with a median age of 66 years (Table 1). Twenty-one patients had occlusion of the middle cerebral artery and four of the internal carotid artery. The presenting NIHSS scores ranged from 1 to 25. The median stroke-onset to imaging time was 5.5 hours (Table 1).
Characteristics of patients with anterior emergent large vessel occlusion selected for thrombectomy.
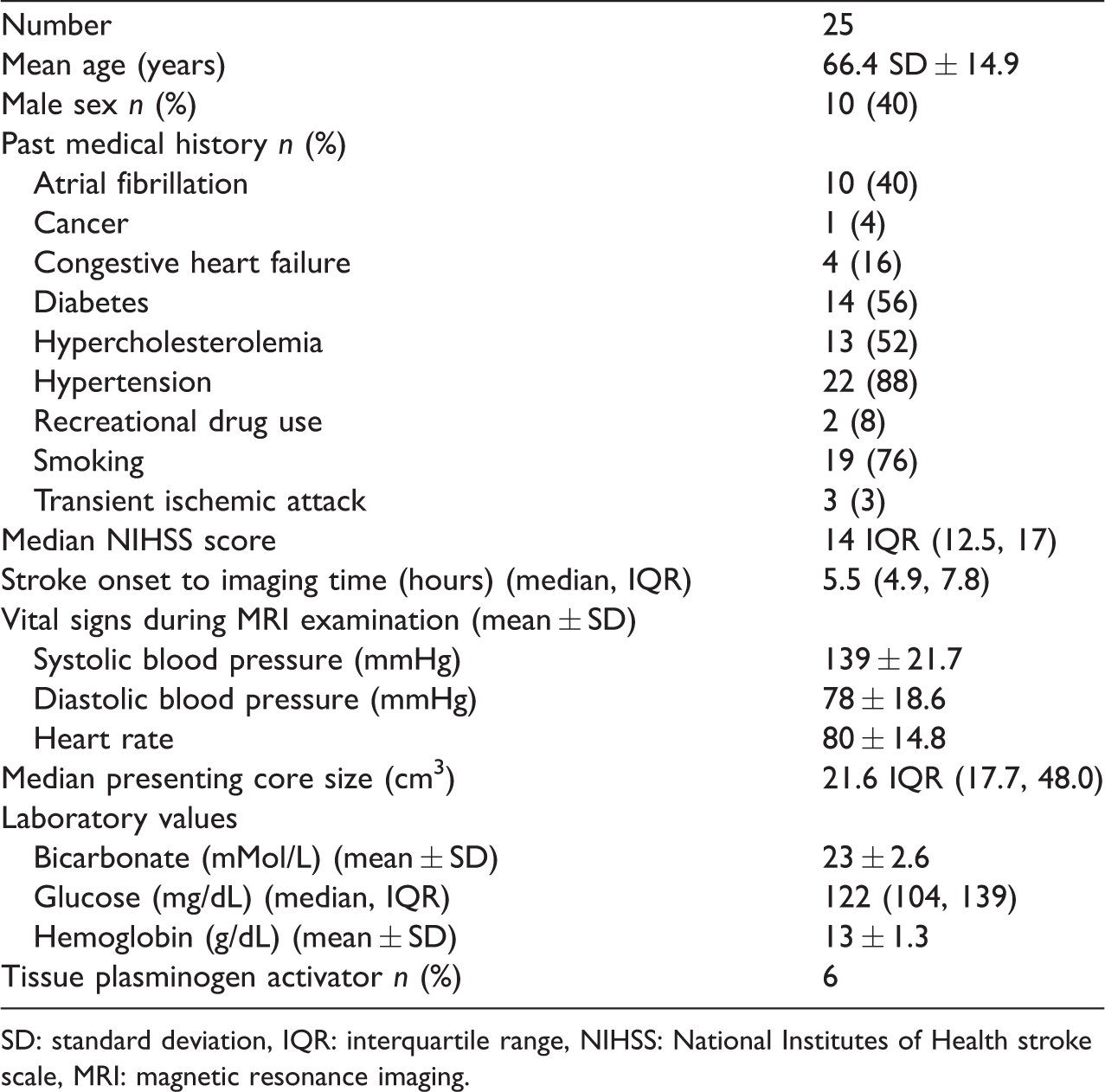
SD: standard deviation, IQR: interquartile range, NIHSS: National Institutes of Health stroke scale, MRI: magnetic resonance imaging.
An obvious initial finding was qualitative asymmetric prominence of the superficial and deep cerebral veins in the cerebral hemisphere ipsilateral to the stroke (Figure 2). Quantitative analysis showed the highest susceptibility in the cortical veins ipsilateral to the stroke compared with the other studied vein groups. The mean susceptibility (95% confidence interval) within the ipsilateral cortical veins was 174 ppb (139–209) compared with 107 ppb (92–120) for the contralateral cortical veins (P = 0.002), 129 ppb (104–155) for the ipsilateral thalamostriate veins (P = 0.05), and 107 ppb (92–123) for the contralateral thalamostriate veins (P = 0.001) (Figure 3). Comparisons between other groups did not reach adjusted statistical significance.
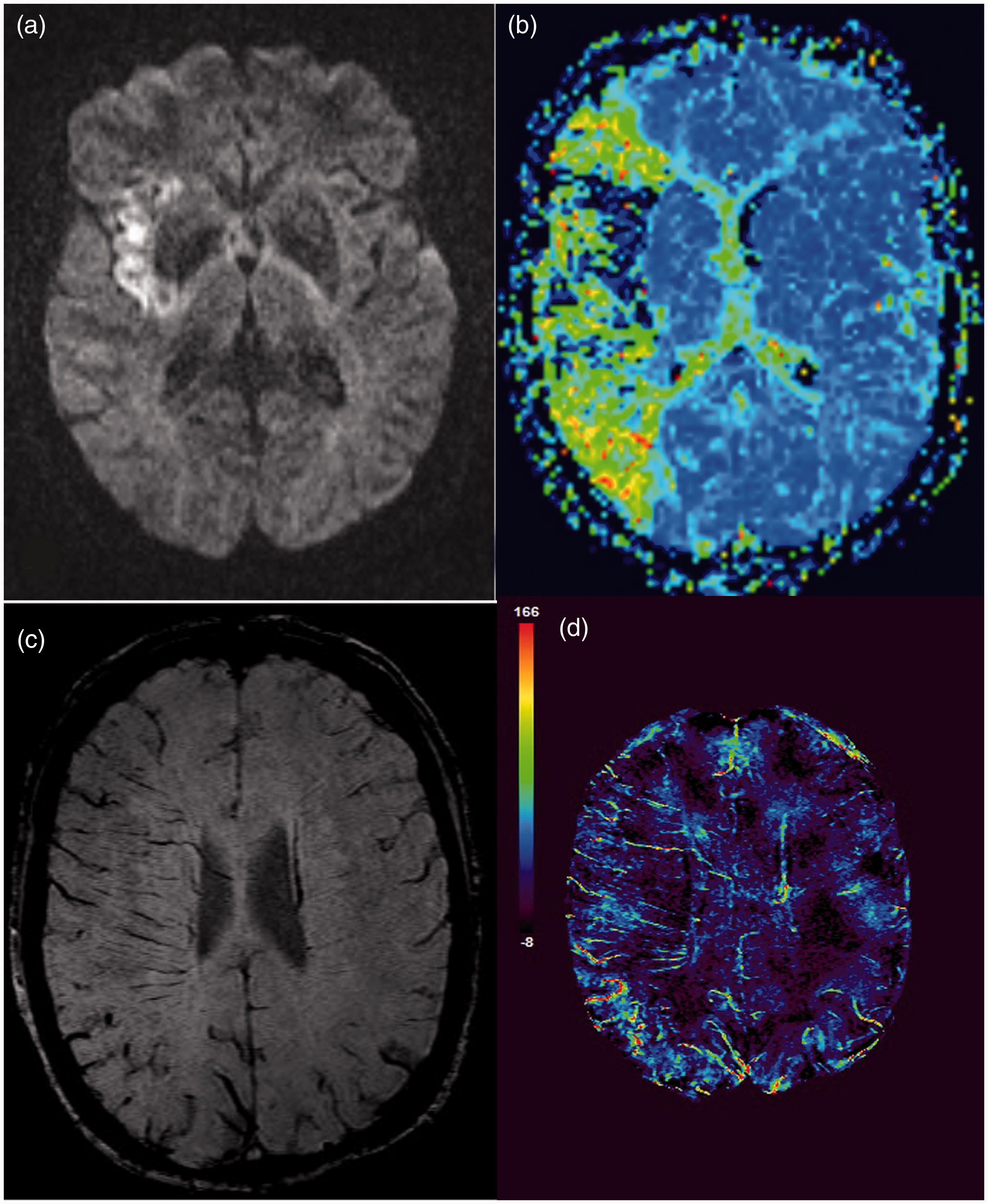
Diffusion-weighted imaging (DWI), mean transit time (MTT), susceptibility-weighted imaging (SWI), and quantitative susceptibility mapping (QSM) in a 61-year-old woman with acute left-sided weakness, NIHSS score of 13, and right M1 occlusion. (a) Axial DWI demonstrates core infarct in the right insula. (b) Axial MTT demonstrates a large mismatched ischemic penumbra in the right middle cerebral artery (MCA) territory. (c) Axial SWI demonstrates increased prominence of the cortical and deep cerebral veins in the right MCA territory. (d) QSM map demonstrates quantifiable susceptibility changes in the cerebral veins in parts per billion.

Susceptibility of cerebral veins in the regions ipsilateral and contralateral to the acute infarct. The cortical veins ipsilateral to the stroke showed the greatest susceptibility followed by the ipsilateral thalamostriate veins.
The susceptibilities of both the ipsilateral and contralateral thalamostriate veins showed strong inverse correlations with the presenting NIHSS score (rho = −0.626, P = 0.001, and rho = −0.498, P = 0.013, respectively) (Figure 4). The correlation between ipsilateral thalamostriate vein susceptibility and presenting NIHSS score was not significantly different after adjusting for the one outlier within the cohort who presented with near complete occlusion of the left internal carotid artery with inadequate collateral support yet extremely high ipsilateral thalamostriate vein susceptibility (rho = −0.597, P = 0.003) (Figure 5).

Correlation between ipsilateral and contralateral thalamostriate vein susceptibility and presenting NIHSS score. Both the (a) ipsilateral and (b) contralateral thalamostriate veins showed a strong inverse correlation with the presenting NIHSS score.
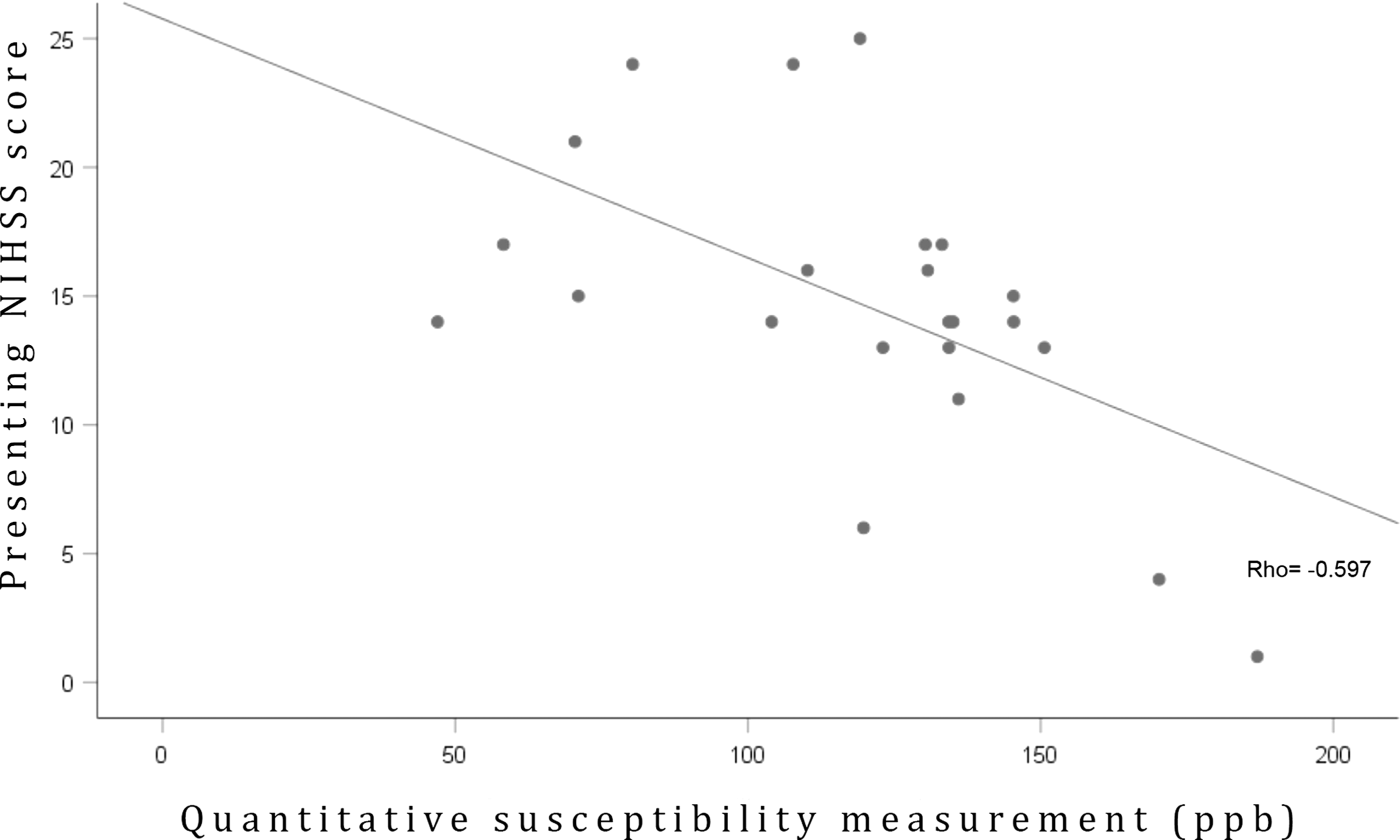
Correlation between ipsilateral thalamostriate vein susceptibility and presenting NIHSS score adjusting for outliers. Excluding a single patient who presented with complete left internal carotid artery occlusion, poor collateral supply, and an extremely high ipsilateral thalamostriate vein susceptibility (360 ppb) did not significantly affect the correlation.
These results demonstrate a strong inverse correlation between ipsilateral deep venous quantitative susceptibility and presenting stroke severity, and increased cerebral venous susceptibility (cortical > thalamostriate) ipsilateral to the occlusion in patients with ELVO stroke.
Discussion
Previous reports correlating cerebral venous susceptibility with neurologic outcome have produced varied results. Park et al. 15 showed that multiple hypointense vessels ipsilateral to the infarct on SWI were associated with lower initial NIHSS score, which was corroborated by the current findings. In contrast, Mucke et al. 23 found that asymmetry of the deep medullary veins on SWI was associated with increased initial stroke severity, and Li et al. 21 reported that decreasing oxygenation of the ipsilateral cerebral veins was associated with poorer outcomes. Zhang et al. 24 recently showed that ipsilateral thalamostriate vein prominence on SWI was associated with reduced reperfusion and a poor outcome following thrombolysis using intravenous thrombolytics. However, to the best of our knowledge, the current study may be the first to compare QSM data and stroke severity using both the cortical and deep venous systems. However, the equivocal nature of the above results indicates the need for further investigations.
The apparently conflicting results also indicate differing conceptual understandings of misery perfusion. Increased cerebral venous susceptibility can indicate the area of viable tissue at risk of infarction 13 , 14 , 25 (i.e., the ischemic penumbra), but also reveals that the tissue is responding appropriately by increasing oxygen extraction, since dark signal and QSM ppb increase with elevated deoxyhemoglobin concentration. In contrast, lack of susceptibility within a tissue suggests that the tissue is metabolically inactive and, in the setting of stroke, most likely unsalvageable. This phenomenon can be observed in the infarct core, where the oxygen extraction fraction has been shown to be markedly decreased. 26 In other words, increased oxygen extraction indicated by increased venous susceptibility indicates an active compensating, homeostatic process, and may therefore correlate with decreased clinical stroke severity, as suggested by the current results.
A continued supply of oxygen within the ischemic penumbra must be maintained by sufficient collateral flow or tissue infarctin will occur. Park et al. 15 showed that increased venous susceptibility was associated with favorable collateralization within the tissue, as well as a greater diffusion-perfusion mismatch volume and decreased diffusion lesion volume. In contrast, Verma et al. 27 found that increased susceptibility was associated with decreased collateral flow, and suggested that the degree of collateral flow determined the level of deoxyhemoglobin in the cerebral veins. Park et al., 15 however, stated that the converse was true: that the degree of collateral flow was determined by the oxygen demand, represented by venous deoxyhemoglobin levels. The above finding of decreased deoxyhemoglobin levels in the ischemic core appears to substantiate the latter claim. 26 If collateral flow is best characterized as a response to increased oxygen demand by the affected tissues, the ability of SWI to estimate deoxyhemoglobin levels would allow it to characterize collateral flow, as another critical factor in determining stroke severity. 28 , 29
The current results also show quantitative susceptibility asymmetry of the cortical veins in acute ischemic stroke with increased venous susceptiblity on the side of the occluded artery, as recently demonstrated by Xia et al. 19 Our study corroborated these findings and expanded on them to include quantitative susceptibility data for the deep cerebral veins. In contrast to the cortical veins, there was no significant asymmetry in QSM between the deep cerebral veins in patients with acute ischemic stroke the median 20% increase of susceptibility in ipsilateral versus contralateral thalamostriate veins did not rise to the level of statistical significance. This may be attributed to the smaller tissue volume served by the deep venous system, decreased basal ganglia collateral supply, or the small sample size of the study. It is also possible that the lack of significance was the result of an increased compensatory response (interhemispheric diaschisis) by the unaffected side during a time of regional ischemic insult.
The current study demonstrated the above findings specifically in patients who underwent endovascular interventions. Some suggest that all patients with ELVO should proceed immediately to mechanical thrombectomy rather than undergoing selection by MRI, 30 while others believe that this strategy fails by exposing the approximately 50% of patients with ELVO with large core infarcts to invasive, futile, and possibly harmful treatment. 31 In particular, MRI plays an important role in the assessment of patients with hyperacute stroke with ELVO who do not present early or do not respond to tissue plasminogen activator. 32
Diffusion-weighted imaging combined with perfusion-weighted imaging is an accepted method for characterizing the ischemic penumbra, and can help to determine if a patient should receive endovascular therapy.3,33,34 The ability of SWI to characterize the ischemic penumbra, reflect adaptive changes in the tissue, and suggest the presence of nontrivial collateral flow suggests that it also may be a valuable tool for aiding patient selection. The current results indicate that QSM values derived from SWI are associated with decreased initial NIHSS score. Given that initial NIHSS score is viewed as the most important predictor of long-term outcomes,35–37 it is plausible that quantitative susceptibility may also be transitively correlated with long-term outcomes in this population.
Our study was limited by its small sample size. Potential cofounders included age, stroke severity, hyperglycemia, time from onset to imaging, and variability of collateral blood supply. However, we believe, that the demonstrated relationship between QSM values and stroke severity provides the basis for further larger studies.
In conclusion, ipsilateral thalamostriate vein susceptibility, derived from QSM data, shows a strong inverse correlation with presenting NIHSS in adult patients with hyperacute stroke who were selected for endovascular intervention by advanced imaging. Quantitative susceptibility values are also asymmetrically elevated in the cortical veins on the ischemic side. Although these results remain to be validated in larger studies, the results suggest that SWI may be an important biomarker for guiding decision making and predicting long-term neurologic outcomes in patients who present with ELVO.
Footnotes
Acknowledgements
We thank Dr. Sam Barnes Ph.D. and Dr. Brenda Bartnik Ph.D. for their assistance with this study.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.