
Abstract
Objective
This study was performed to evaluate the clinical outcomes in adult polytraumatized patients with thoracic injury and femoral shaft fractures treated with double-plating fixation.
Methods
From November 2010 to October 2014, 15 polytraumatized patients with femoral shaft fractures were enrolled in this retrospective study. Radiographic findings and functional outcomes were assessed at 1, 3, 6, and 12 months postoperatively.
Results
Fourteen (93%) of the 15 femoral shaft fractures achieved bony union, with a mean time to union of 9.2 months. The mean Nonarthritic Hip Score and Lysholm Knee Score was 89.4 and 87.2 points, respectively. The range of motion of the knee joint was comparable between the injured and uninjured legs (116° and 121°, respectively).
Conclusions
Our findings suggest that lower limb function returns to normal after orthogonal double-plating fixation, which is an alternative technique to intramedullary nailing for femoral diaphyseal fractures in patients with severe chest injury.
Keywords
Introduction
Approximately 30% of femoral shaft fractures occur in polytraumatized patients with high-energy injuries. 1 These patients present with a high incidence of morbidity and mortality because of the lack of appropriate treatment methods.2,3 Despite early operative treatment using intramedullary nails (IMNs), femoral fractures predispose patients with severe thoracic trauma to enhanced pulmonary dysfunction and systemic complications, possibly because of pulmonary fat embolization and the aggravated “second hit” phenomenon.4,5 Several scholars have recommended plate fixation in patients whose injuries are unsuitable for intramedullary fixation.6,7
In this retrospective cohort study, we evaluated the results of orthogonal double-plating fixation of comminuted femoral fractures with respect to the achievement of anatomical reduction, mechanical stability, and less femoral canal interference. We assessed clinical outcomes in skeletally mature patients with thoracic trauma and comminuted femoral shaft fractures using this fixation technique. We also investigated surgical complications and functional outcomes using the Nonarthritic Hip Score and Lysholm Knee Score. These measurement parameters have high reliability and validity and are commonly used in clinical studies of femoral shaft fractures.8–10
Materials and methods
Demographic characteristics of patients treated with double-plating fixation (n = 15).
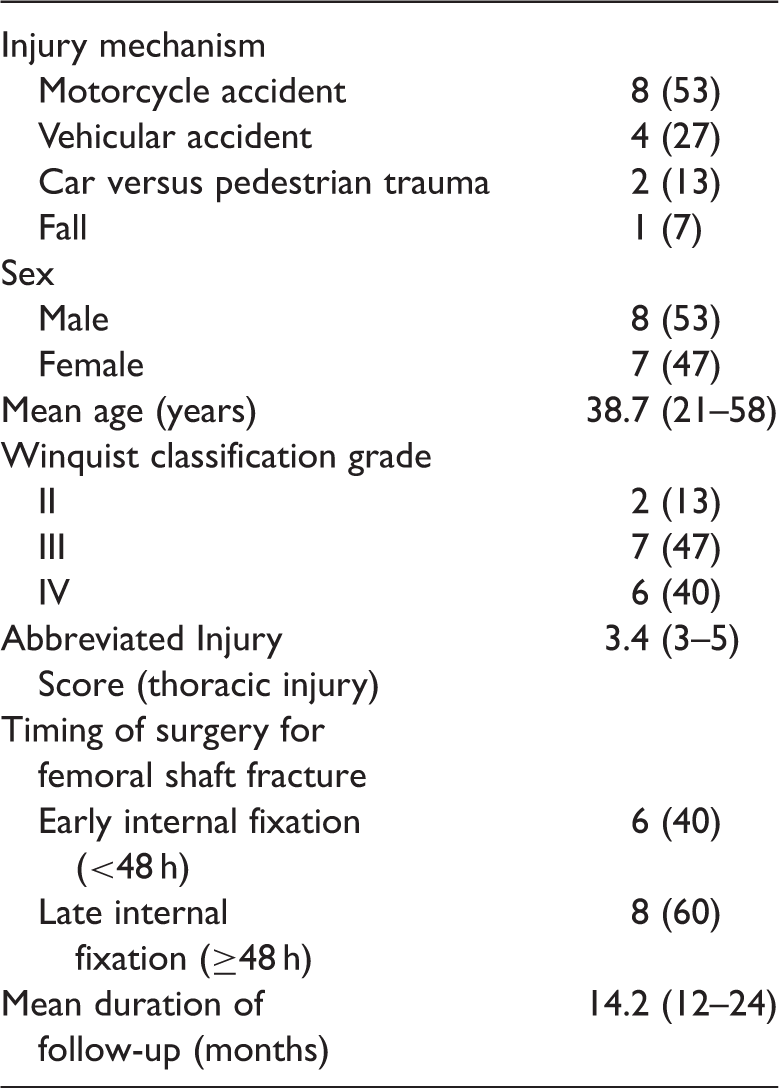
Data are presented as n (%) or mean (range).
Operative technique and protocol
Most of the enrolled patients had sustained multiple injuries; therefore, initial management followed the Advanced Trauma Life Support protocol. Tibial tubercle traction or external fixation was conducted for patients waiting for internal fixation. All operations were performed by a senior surgeon (R.X.) with >20 years of orthopedic trauma experience. The patients were placed in the supine position on a radiolucent flat table and administered general anesthesia. A longitudinal incision (6–10 cm) was made at the anterior aspect of the fracture zone. The vastus intermedius muscle was separated from the vastus lateralis in the direction of the fibers and retracted medially. The fracture site was exposed, and the periosteum and blood supply to the bone fragments were preserved. The fracture was directly reduced through manual traction and clamp-assisted reduction. The limb length, fracture rotation, and angulation were then adjusted. A locking compression plate with a 3.5-mm hole was positioned on the anterior surface of the femoral shaft and fixed with a minimum of three screws (six cortices) placed in the major proximal and distal fracture fragments. If necessary, a lag screw was used to achieve absolute stability of the large wedge fragment. Small (4- to 5-cm) distal incisions were then made over the lateral aspect of the femur with deep dissection through the iliotibial tract and vastus lateralis muscle. A second locking compression plate (4.5-mm hole) was placed perpendicular to the first plate through a minimally invasive submuscular technique. The plate was then locked with locking screws over the proximal percutaneous small incisions, thereby omitting one or two holes. This procedure increased the fracture span and allowed for micromovement of the fragments to enhance callus formation. The operative time and postoperative blood loss were then recorded. A drain was used for 48 h to prevent postoperative hematoma. All patients were given antibiotics after surgery.
Postoperative rehabilitation was divided into three phases. On the second postoperative day, all patients started physical therapy (phase 1, postoperative weeks 0–4). Active mobilization and isometric exercises of the lower extremity were allowed without any restriction in the range of motion (ROM). The patients were allowed to lift their leg while using crutches to avoid weight bearing. Upon discharge from the hospital, the patient was enrolled in an outpatient physical therapy program 2 to 3 days per week. Strengthening exercises were added into phase 2 (postoperative weeks 4–10). The patients were also encouraged to perform quadriceps strengthening and knee ROM exercises. Phase 3 (postoperative weeks 10–18) focused on balance, proprioception, and gait training activities. Partial weight bearing was also advised 10 to 12 weeks postoperatively. Full weight bearing was only permitted after the appearance of a bridging callus or clinical union at the femoral shaft fracture site.
The patients were followed up postoperatively for a minimum of 12 months or until the occurrence of fracture union. The patients were evaluated through radiological and functional examinations at 1, 3, 6, and 12 months postoperatively. Blinding and randomization of the patients according to treatment arms were not done because the study was retrospective. Fracture healing was defined by resolution of pain and tenderness at the fracture site upon weight bearing and the presence of cortical bridging on at least three of the four cortices on the anteroposterior and lateral radiographic views. Nonunion was defined as failure of clinical and radiological healing 1 year after the operation (persistent fracture line, lack of bridging trabeculae, or lack of cortical continuity of more than one cortex with unimproved radiographic findings on sequential follow-up X-ray studies). The secondary outcome parameters included the Nonarthritic Hip Score, Lysholm Knee Score, knee ROM, in-hospital complications, implant failure, malalignment, infection, and the need for revision surgery. To accurately measure knee flexion ROM, each motion was measured three times with a hand-held universal goniometer, and the values are reported as mean flexion. Before measurement of ROM, the patient lay in the supine position and maximally bent his or her own knee.
Statistical analysis
The data analysis was conducted with PASW Statistics for Windows, version 18 (SPSS Inc., Chicago, IL). Means and standard deviations were calculated. The data were analyzed with Student’s t-test and the Mann–Whitney U-test as appropriate.
Results
Intraoperative outcomes
The mean operative time was 92.7 ±14.2 minutes (range, 70–190 min). The estimated blood loss was 302.9 ± 41.2 mL (range, 168– 432 mL), with an average perioperative transfusion requirement of 3.8 ± 0.4 units (range, 2–5 units). No intraoperative complications were reported.
Postoperative outcomes
At the final follow-up, no patient exhibited flexion contracture of the knee, and all patients obtained satisfactory knee flexion ROM (116.4° ± 6.9°) with at least 105° of knee flexion. The mean knee flexion of the affected leg was similar to that of the unaffected leg. The results revealed significant differences in ROM among four time points (p < 0.0001) (Figure 1). At the last visit, the mean Nonarthritic Hip Score and Lysholm Knee Score was 89.4 ± 7.8 points (range, 73–91 points) and 87.2 ± 8.4 points (range, 78–96 points), respectively. Approximately 79% and 83% of the patients had a Nonarthritic Hip Score and Lysholm Knee Score of ≥ 85 points, respectively.
Ranges of motion continued to improve until 6 months after double-plating fixation. *p < 0.05, **p < 0.01, #No significant difference compared with the 6-month time point.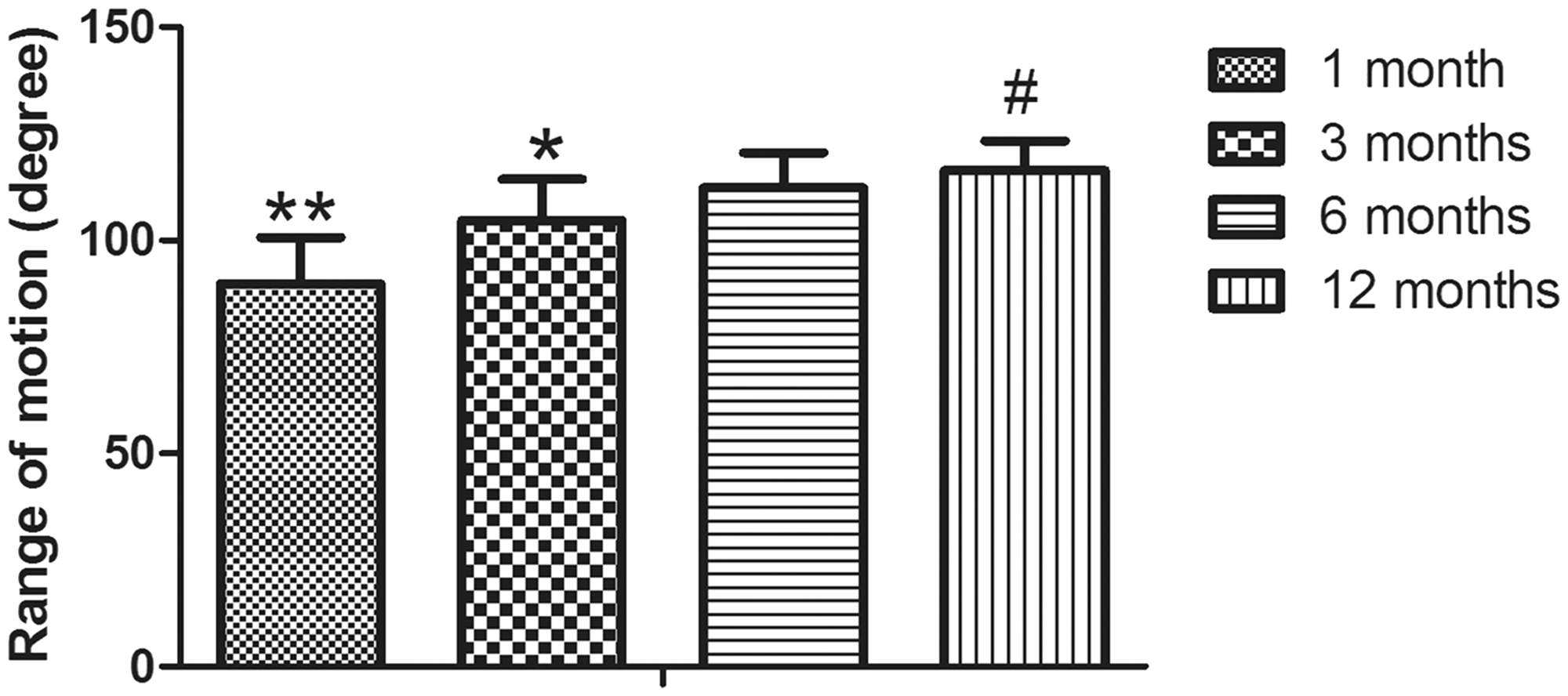
Primary union occurred in 14 patients within an average time of 9.2 months (range, 8–12 months) (Figure 2). One noncompliant patient with postoperative tobacco use showed delayed union, which healed uneventfully after the patient quit smoking. No additional cases of significant axial/rotational malalignment or limb length discrepancy were noted. Moreover, no patients developed deformities requiring revision surgery. One patient manifested a superficial wound infection that was successfully treated with antibiotic therapy.
(A, B) Preoperative radiographs of the injured femur. (C, D) Radiograph 9 months after the operation shows union of the femur.
Discussion
Fixation with IMNs is the preferred standard treatment method for simple femoral shaft fractures, but it does not provide sufficient stability for comminuted femoral shaft fractures. Based on the Winquist classification system of diaphyseal femoral fractures, an increase in the Winquist grade may reveal a high degree of comminution and instability as well as less cortical bone contact. 11 The use of an indirect/closed reduction technique for a comminuted fracture may result in inaccurate reduction and malunion.11,12 In severely comminuted fractures, the inability to rely on fracture lines to assess the reduction quality complicates the determination of accurate length and rotation and the maintenance of anatomical reduction of the fracture. Thus, severely comminuted fractures may be a negative prognostic factor for malunion because of postoperative shortening and malratotation. 11 Lin et al. 13 observed fragmentary displacement of > 1 cm (reversed butterfly fragment) in comminuted femoral shaft fractures after the IMN affected bone healing. A large reversed butterfly fragment may lead to technical difficulties in anatomical restoration, such that a residual gap persists after closed reduction. A larger gap between fragments may also induce soft tissue interposition, which turns the endosteum inside out, compromises the vascular bed, and complicates callus bridging; these phenomena are associated with a high risk of delayed union and nonunion. 13
Some recent studies have focused on the risk of pulmonary complications associated with reamed IMNs, especially in patients with polytrauma and severe thoracic injuries.14,15 Fat embolism syndrome and pulmonary dysfunction may also develop in patients with multiple injuries including long bone fractures. 14 Although early fixation of fractures is beneficial, an IMN may exacerbate pulmonary dysfunction by increasing intramedullary pressure and embolization of marrow fat. 14 Christie et al. 14 revealed the presence of bone marrow emboli in the pulmonary system using transesophageal echocardiography. In the presence of lung injuries and hemodynamic shock, alternative fixation can be used to avoid further pulmonary damage.6,15,16 Polytraumatized patients who undergo plate fixation may have a lower incidence of cardiopulmonary complications because of less femoral canal interference.
In their biomechanical study, Choi et al. 17 used synthetic composite bone to evaluate the stiffness of comminuted periprosthetic femoral shaft fractures. They found increased stiffness to axial loading, lateral bending, and torsion when an anterior locked plate was combined with a lateral locked plate in comparison with the single-plate design. In accordance with the tension band concept, orthogonal double-plating was applied to patients with periprosthetic femoral fractures and femoral shaft nonunion, and they were satisfied with the outcomes.18–20 Mechanical stability considerably affects local vascularization and tissue differentiation during callus healing. We speculated that double-plating (anterior and lateral plating) provides a biomechanically superior fracture fixation construct to stabilize comminuted femoral fractures compared with single lateral plating. Recent studies have revealed satisfactory clinical outcomes in patients with femoral shaft fractures treated with minimally invasive techniques and plate–screw fixation in accordance with biological fixation principles.6,12,21,22 Most of the patients in the present study achieved satisfactory ROM and muscle strength after the operation. The ROM values continued to improve until 6 months after the surgery, but only small changes were seen after 6 months. At the final follow-up, the Nonarthritic Hip Score and Lysholm Knee Score were correlated with excellent function and low disability.
This study has several limitations, including its retrospective nature and the biases inherent to such study designs. Because of the lack of a control group, a statistical analysis to determine the risk ratio of postoperative complications was not performed. The functional scores obtained at the latest follow-up did not allow us to determine whether statistically and clinically significant functional improvements had occurred over time.
In summary, orthogonal double-plating fixation is a safe and effective alternative technique for treatment of femoral shaft fractures in patients with an injured chest. This technique can be used when IMN fixation is unsuitable for adult polytraumatized patients.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by the Fund for Distinguished Young Doctors from Shanghai Municipal Commission of Health and Family Planning to Dr. Tao Cheng.