
Abstract
Objective
Multidisciplinary trauma teams are the standard of care in the USA, but staffing differences and lack of advanced trauma life support training hinder replication of this system in Chinese hospitals. We investigated the effect of simulation team training on initial trauma care.
Methods
Over 15 months, we compared grade I trauma patients cared for by the trained team and those cared for using traditional practice on times from emergency room arrival to tests/procedures. Propensity-score analysis was performed to improve between-group comparisons.
Results
During the study, 144 grade I trauma patients were treated. Trained team patients showed shorter times from emergency room arrival to initiation of hemostasis (31.0 [13.5–58.5] vs. 113.5 [77–150.50] min), blood routine report (8 [5–10.25] vs. 13 [10–21] min), other blood tests (21 [14.75–25.75] vs. 31 [25–37] min), computed tomography scan (29.5 [20.25–65] vs. 58.5 [30.25–71.25] min) and tranexamic acid administration (31 [13–65] vs. 90 [65–200] min). Similar results were obtained for the propensity-score matched cohort.
Conclusion
Simulation team training could help reduce time to blood routine reports, scans and hemostasis. Assessment of available resources and development of targeted team training could improve care in resource-limited hospitals.
Keywords
Introduction
Trauma is the leading cause of morbidity and mortality among children and teenagers worldwide.1–3 There are several scoring systems to triage trauma patients and permit efficient allocation of medical resources to the most severely injured individuals.4,5 Clinical investigators have made great efforts to improve medical outcomes in severely injured patients. The key to successful treatment of such patients is prompt initiation of necessary tests and procedures;6–8 delayed initiation of these can be fatal in certain circumstances. Thus, teamwork between doctors and nurses is vitally important in the initial management of trauma patients. In the USA, the development of specialized trauma centers and widespread use of advanced trauma life support (ATLS) training has greatly improved major trauma outcomes.9–11 Duplication of this system has been successful in many countries. However, trauma teams comprise staffs from multiple departments and activation of a full trauma team for every trauma patient imposes a substantial burden on institutions with limited medical resources.12–14 This is even more challenging in countries like China, where ATLS training is not available. One of the authors (YH) has completed ATLS training in the USA. We decided to analyze the process of trauma care at one large trauma center in Hangzhou, China. We proposed a novel teamwork pattern based on this analysis that comprised nurses and doctors from the emergency department (ED). We hypothesized that structured teams would improve the efficiency of emergency room (ER) care even without formal ATLS training.
Methods
Settings and patients
This was a retrospective study conducted in a university-affiliated hospital from April 2014 to July 2015. The training program was a quality improvement program that was prospectively implemented (not for the purpose of the present study). Medical records were retrospectively reviewed for this study. Patients admitted to the hospital ED were triaged according to the local triage criteria. Patients with grade I trauma were potentially eligible for the study. The criteria for grade I trauma were as follows: 1) airway obstruction requiring tracheal intubation or tracheal tube already in place; 2) deterioration in respiration, including apnea, respiratory distress (>35/min) and slowed respiration (<12/min); 3) signs of shock such as pale and clammy skin, weak pulse, tachycardia, refill time >3 s and receipt of blood transfusion; 4) Glasgow Coma Scale (GCS) <12; 5) special injuries, such as stab injuries to head, neck, trunk and groin region, flail chest and open injury on chest. Patients were excluded if they were 1) pediatric patients; 2) pregnant; and 3) had do-not-resuscitate orders. The study used data from a database that were de-identified; thus, ethical approval was waived.
Control group
Before the team training program, there was no standard algorithm for the management of trauma patients in our ED. Trauma patients were managed by emergency physicians and there was no trauma team waiting at the bedside. The on-call physician performed the initial patient assessment and if there was a surgical problem, specialty surgeons would be consulted. However, because of limited human resources at the time and lack of heuristic management of the trauma care system, there could be delays in the first assessment by surgical specialists.
Composition of the team
The team was composed of six ED nurses and doctors (Figure 1). The team leader (TL) was an ED physician with more than 10 years of experience in the management of trauma patients. The TL was responsible for coordinating the team and consulting with patients or their surrogates. A resident (J1) was positioned at the head of the patient and was responsible for airway management. Other tasks of J1 were judgment of consciousness and pupil reactivity, cervical collar fixation, focused abdominal sonography for trauma scan (FAST), recording of progress notes, nasal gastric tube insertion and central venous catheter placement. Another physician (J2) with more than 5 years of experience in the management of trauma patients was at the bedside and was responsible for systematic evaluation of airway, breathing, circulation, disability and exposure (ABCDE approach); hemostasis by compression; pelvic girdle fixation; urinary catheter insertion and chest tube placement. A nurse (N1) was on the patient’s right side and was responsible for oxygen delivery, establishment of venous lines, monitoring vital signs and mechanical ventilation connection. The second nurse (N2) stood on the patient’s left and was responsible for preparation of instruments for procedures. She also helped to obtain blood samples for tests. A third nurse (N3) was at the desk and was responsible for recording, medical order entry into the electronic system, arranging consultations with other departments and obtaining results of examinations, such as computed tomography (CT) and ultrasound.
Schematic diagram of the bedside composition of the team. (TL) team leader: usually a physician but could vary based on procedural needs; (J1) airway control physician; (J2) primary assessment physician; (N1) primary nurse; (N2) secondary nurse; (N3) scribe/orders nurse.
Study design and variable collection
Simulation training schedule for Phase 4.
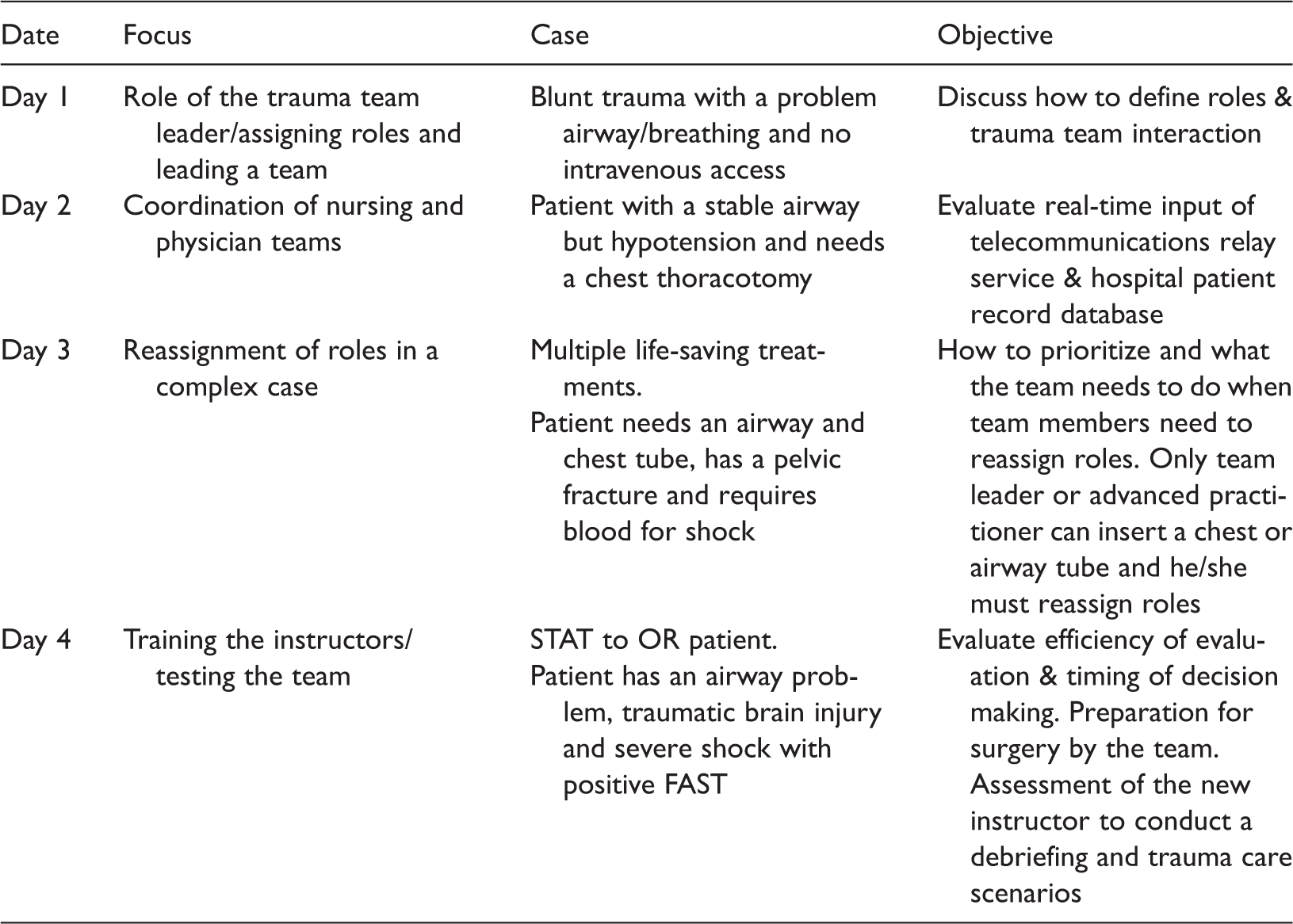
FAST: focused abdominal sonography for trauma scan; OR: operation room; STAT: at once.
Times from ER arrival to tests and procedures
We observed a range of times between ED arrival and the implementation of tests and procedures, which are important for trauma patients. These tests and procedures were green channel open, cervical collar, venous line establishment, first fluid infusion, oxygen delivery, artificial airway establishment, central venous catheter, chest tube insertion, chest band, urinary catheter, hemostasis, blood routine report, other blood tests, CT scan, X-ray, ultrasound, electrocardiogram, consultation call, trauma team arrival, packed red blood cell (PRBC) preparation, PRBC transfusion, hemostatic administration, analgesics and leaving the resuscitation room.
Statistical analysis
Continuous variables were expressed as median and interquartile range because of the limited sample size. Data for the team and control groups were compared using the rank-sum test. Categorical variables were expressed as number and percentage and compared using the chi-square test. 19 Owing to the limited sample size, it was impossible to match the team and control groups on all variables. Furthermore, a multivariable regression model requires the predictors to be normally distributed and it was difficult to meet this criterion with our small sample size. 20 Propensity-score analysis is a non-parametric method that can help to reduce the model dependence.21–23 This was performed by regressing the team group variable on variables with P < 0.2 in a bivariate analysis. Propensity score or distance was calculated for each subject and represented the probability of assignation to the team group conditional on relevant variables. The nearest neighbors matching method was used to select a matched cohort and the balance between the team and control groups in the matched cohort was graphically assessed. In the matched cohort, we compared differences in times from ED arrival to tests and procedures. All statistical analyses were performed using R software (version 3.2.3; the R Foundation). 24 A two-tailed value of P < 0.05 was considered to be statistically significant.
Results
Demographics and baseline characteristics.
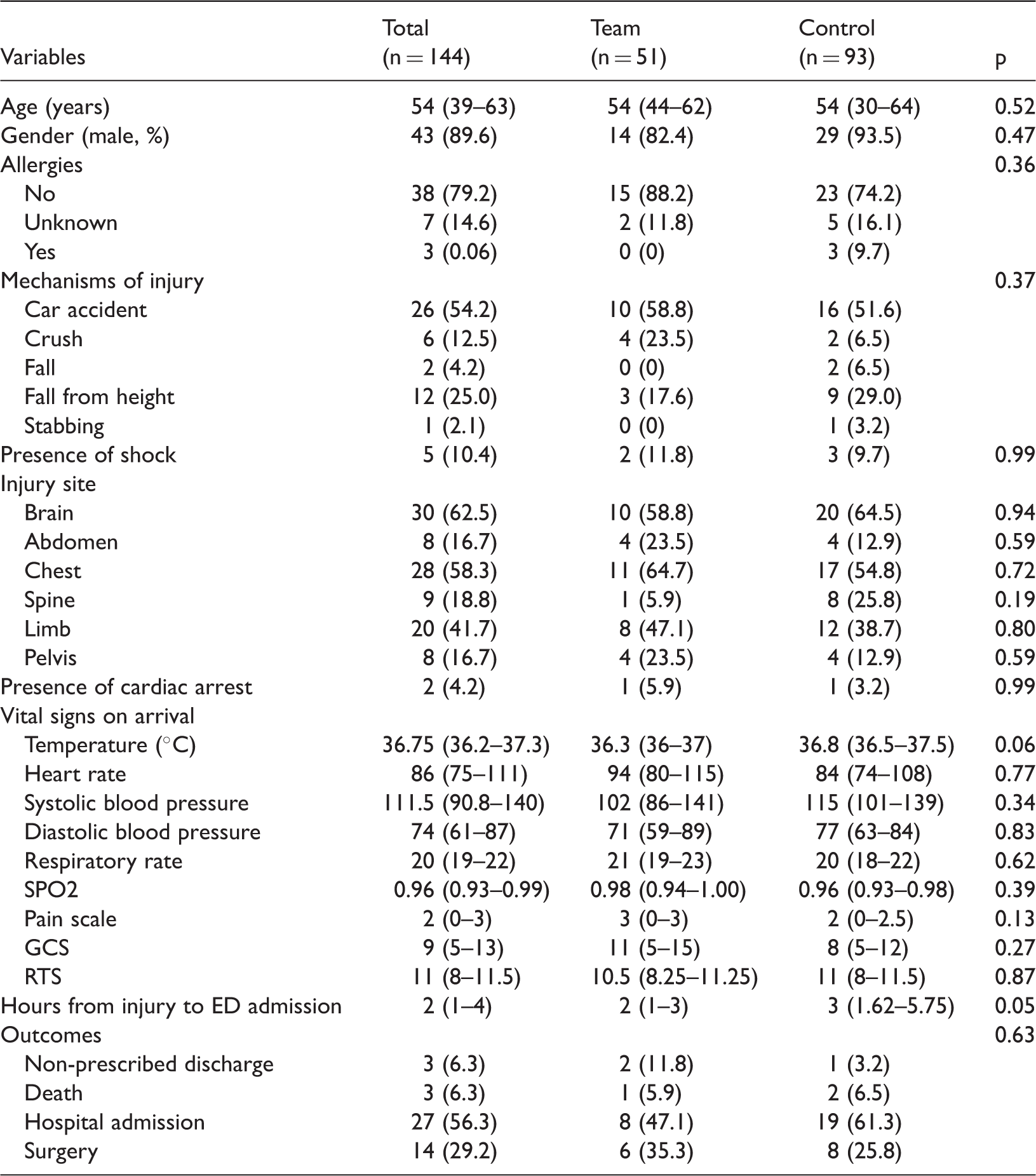
GCS: Glasgow Coma Scale; RTS: Revised Trauma Score; SPO2: saturation of peripheral oxygen.
Comparison of time from emergency room arrival to tests and procedures between team and control groups.

CT: computed tomography; CVC: central venous catheter; EKG: electrocardiogram; IQR: interquartile range; PRBC: packed red blood cell.
A logistic regression model was fitted by regressing team group on other variables, including mechanisms of injury, oxygen delivery methods, body temperature on ED arrival, pain scale and hours from injury to ED admission. The first two variables did not meet the statistical entry criteria, but we felt they may have influenced the team group assignation. Using the nearest neighbor method, 51 out of the 93 subjects in the control group were matched to the 51 subjects in the team group. Note that the unmatched subjects were unlikely to be assigned to the team group conditional on given clinical variables. Their propensity scores were outside the common support region. Figure 2 shows the distribution of propensity scores in the matched and raw cohorts. The team and control group propensity-score distributions were more comparable in the matched cohort. The matched cohort produced similar results to that of the raw cohort (Table 4). The team group showed significantly shorter times to blood routine report (8 [5–11] vs. 13 [10–21]; P < 0.01), CT scan (29.5 [18.5–36.5] vs. 47 [35.5–77] min; P = 0.01) and hemostasis (31 [13.5–58.5] vs. 107 [58.5–121] min; P =0.04) than the control group.
Distribution of propensity scores in matched and raw cohorts. Differences in time to tests and procedures between team and control groups in propensity-score matched cohort. CT: computed tomography.

Discussion
Our original plan was to use workflow analysis and team training to develop a new trauma care model at Hangzhou Hospital. We intended to compare the functionality of the new teams to historical controls. The study showed that structuring teamwork was feasible and helped to more promptly initiate important tests and procedures. The traditional practice approach to managing severely injured patients was more chaotic and the resuscitation was less effective. The key to a team’s success is to inform every member of his or her responsibilities. Our preliminary results showed that a successful team could ensure that the treatment process was smooth and effective. Compared with the control practice, teamwork significantly shortened the time from ER arrival to blood routine report, CT scan and hemostasis. Because the team was composed of medical staffs from ER, it could take action before the arrival of the multidisciplinary trauma team. The primary task of the initial team is to promptly initiate life-saving tests and interventions and speed is vitally important. This task is somewhat different from the task of a multidisciplinary trauma team. Most of the time, the activation of a full trauma team is unnecessary and imposes a great burden on limited medical resources.5,25,26
Hemostasis by surgical procedures and administration of TXA is important for severely injured patients. There is a recommendation that TXA should be given promptly after injury and that time to administration is associated with mortality outcomes.27–30 Thus, every effort should be made to shorten the time from injury to TXA administration. In the present study, the teamwork enabled a significant decrease in the time from ER arrival to TXA administration. This is an important intermediate step in turning teamwork management into improved survival for severely injured patients. Research on hemostatic resuscitation for injured patients also emphasizes the importance of prompt initiation of hemostatic interventions. 31 Massive, prolonged hemorrhage is responsible for coagulopathy. Blood routine reports are essential to monitor injured patients for massive hemorrhage. Thus, prompt initiation of the first blood routine report is essential to assess illness severity. In addition, blood routine reports can help to dictate further treatments, such as PRBC transfusion, surgical intervention and hemostasis.32–34
The biggest limitation of this study was the small sample size, so the results are mainly useful for hypothesis generation. In addition, objective outcomes such as mortality, morbidity and length of hospital stay were not investigated. We examined multiple study endpoints, which raises the issue of multiple testing. 35 However, several endpoints in our study showed P values of less than 0.01, making it unlikely that the results were false positives. We can therefore be more confident that the observed differences were not a result of multiple testing. The study was not a randomized controlled experiment and the results may show confounding. We used propensity-score analysis to balance baseline characteristics between the team and control groups. The advantage of propensity-score matching is that it is a non-parametric method in which the relationships between variables are less dependent on their distributions. 36 Propensity-score analysis also permits analysis of observational data such as randomized experiments. 37 The results for the propensity-score matched cohort were consistent with those for the raw cohort.
In conclusion, the study used workflow analysis to develop an ideal team then trained the teams using a crew resource management simulation. Our results showed that using teamwork could help to reduce the time to blood routine report, CT scan and hemostasis in the initial management of severely injured patients. We suggest that this approach be replicated at other centers. The findings then need to be validated in larger trials and other patient-important end points such as mortality, morbidity and financial cost need to be investigated. These findings are useful because they demonstrate that a simple technique that does not require complex training can result in improved patient care efficiency. Chinese hospitals could employee the methods used in this study to improve care efficiency.
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.