
Abstract
Objective
Diagnosis of gastric intestinal metaplasia (GIM) relies on gastroscopy and histopathologic biopsy, but their application in screening for GIM is limited. We aimed to identify serological biomarkers of GIM via screening in Guangdong, China.
Methods
Cross-sectional field and questionnaire data, demographic information, past medical history, and other relevant data were collected. Blood samples were collected for pepsinogen (PG)I, PGII, gastrin-17, and Helicobacter pylori antibody testing, and gastroscopy and histopathologic biopsy were performed. Single factor and logistic regression analyses were used to evaluate the correlation between these indicators and GIM, and decision tree models were used to determine the cut-off points between indicators.
Results
Of 443 participants enrolled, 87 (19.6%) were diagnosed with GIM. Single factor analysis showed that pepsin indicators (PGI, PGII, and PGI/PGII ratio) and the factors Mandarin as native language, urban residency, hyperlipidemia, and age were associated with GIM. Logistic regression analysis showed that PGI and age were associated with GIM.
Conclusions
Age is an important factor for predicting GIM progression; age >60 years increased its risk. Detection of GIM was higher in individuals with PGI levels >127.20 ng/mL, which could be used as a threshold indicating the need to perform gastroscopy and histopathologic biopsy.
Keywords
Introduction
Gastric cancer is the fifth-most commonly diagnosed malignancy and the third most common cause of cancer-related mortality worldwide. 1 Although its incidence in China has been declining in recent years, it remains much higher than the global average. As early as 1975, Correa et al. 2 proposed a model for the stages of human intestinal type gastric cancer, where in normal gastric mucosa progresses to chronic superficial gastritis, then to chronic atrophic gastritis, intestinal metaplasia, dysplasia, early gastric cancer, and, finally, to advanced gastric cancer. Gastric intestinal metaplasia (GIM) is the transformation of gastric mucosal epithelium and its glands into intestinal mucosal epithelium and glands under pathological conditions. As a premalignant lesion of gastric cancer, GIM involves a precancerous change of the gastric mucosa with intestinal epithelium and is associated with an increased risk of dysplasia and cancer. 3 The European management of precancerous conditions and lesions in the stomach (MAPS) guidelines noted that GIM, as a marker of a high risk of gastric cancer, would increase the risk of gastric cancer.4–6 The global prevalence of GIM is 25%; developed countries, such as the United States (11.7%) and Japan (6.2%), have prevalence rates close to or below this average, whereas developing countries see comparatively higher rates.7–10 For example, the prevalence of GIM is 28.9% in Vietnam, and 30% to 32% in mainland China.11,12 Therefore, the key to reducing the incidence of gastric cancer in China is to take intervention measures at the GIM stage. At present, GIM is diagnosed by invasive means such as gastroscopy, which may lead to poor compliance in patients. Additionally, scarce medical resources limit the ability of staff to perform gastroscopy and histopathologic biopsy. If individuals at higher risk of GIM can be identified through serological screening, the detection of GIM can be more beneficial. Some studies have shown that pepsinogen (PG) has significance in screening chronic atrophic gastritis, one of the precancerous lesions of gastric cancer. 13 However, there have been no reports on the screening of serum PG in intestinal metaplasia. In this study, we conducted precancerous disease screening and serological analysis of the general population of Guangdong, China. We aimed to investigate the significance of predictive variables of GIM-related factors, such as PG, to develop a more targeted GIM screening process.
Materials and methods
Ethics
This study was performed in accordance with the ethical standards laid down in the 1965 Declaration of Helsinki and its later amendments and approved by the ethics committee at the First Affiliated Hospital of Guangdong Pharmaceutical University. All participants gave written informed consent before inclusion in the study.
Participants
From 2015 to 2016, 91 townships in Guangdong Province were investigated. The participants were long-term residents from 18 to 80 years old who were recommended or volunteered for gastroscopy and serological examination (both including pathological examination). Exclusion criteria were (1) a history of upper gastrointestinal surgery; (2) long-term use of anticoagulant drugs or antiplatelet drugs, or the presence of coagulation dysfunction such that endoscopic biopsy could not be performed; (3) a lack of signed informed consent; (4) not being considered suitable for this study by researchers; and (5) gastric cancer.
Questionnaire survey
After participants gave informed consent, questionnaires were administered by professionals who interviewed the participants. The questionnaire was designed based on the literature of GIM and its related factors, according to the epidemiology and incidence of GIM in Guangdong Province, combined with relevant measures of gastric cancer screening. The questionnaire collected information on demographic characteristics, lifestyle, diet, medical history, and family history. 8 Smoking was defined as smoking more than one cigarette a day continuously or cumulatively for more than 6 months. Alcohol consumption was defined as ethanol consumption >40 g/day for men (>20 g/day for women) or a history of heavy drinking within 2 weeks (ethanol >80 g/day). Ethanol consumption was calculated as alcohol consumption (mL) × alcohol content (%) × 0.8 (proportion of ethanol). Mandarin was defined as daily communication occurring only in Mandarin. Helicobacter pylori (Hp) infection was defined as positive serum Hp antibody.
Serological testing
In the morning, 10 mL of fasting venous blood was drawn into collection tubes (Kangjian Medical, Taizhou City, China) and serum was harvested by centrifugation at 1006.2 ×g for 10 minutes. Serum PGI, PGII, gastrin-17 (G-17), and Hp antibodies were then detected by enzyme-linked immunosorbent assay (ELISA). The testing reagents were purchased from Huian Biotechnology Company (Shenzhen, China).
Gastroscopy and histopathologic biopsy
All participants were examined by gastroscopy (GIF H260Z, Olympus, Tokyo, Japan) and underwent histopathologic biopsy. The biopsy criterion was as follows. If no suspicious pathological mucosa was found under the gastroscope, viable tissue was taken 2 cm from the pylorus at the large curvature of the gastric antrum and 8 cm from the cardia at the large curvature of the gastric body.14,15 If a suspected lesion was found under the gastroscope (i.e., change in local mucosal color and/or surface structure), five pieces of viable mucosal tissue of the suspected lesion were taken with disposable biopsy forceps after magnifying and staining endoscopy observation in addition to the above routine biopsies. All tissues were fixed in 10% formaldehyde solution after removal and sent to the laboratory for examination.
Grouping of participants
Based on the results of gastroscopy and histopathologic biopsy, the participants were divided into two groups: GIM group and healthy gastric mucosa group.
Efficiency validation of decision tree model
In accordance with different cut-off point values, an individual would have serological screening to determine whether their values exceeded the established cut-off point values. If the predicted risk of a participant was higher than the given cut-off point value, the participant would be included in the population with positive intestinal metaplasia. Sensitivity and specificity values (data not shown) were calculated.
Statistical analysis
Epidata 3.1 (www.EpiData.dk) was used to establish the database, and SPSS software, version 20.0 (IBM Corp., Armonk, NY, USA) was used for statistical analysis. Descriptive analysis was performed on basic information, previous medical history, family history, and gastroscopy results. Detection rates were compared using the χ2 test. Logistic regression analysis was performed to analyze factors related to GIM. The test level was set at α = 0.05 (p < 0.05).
Results
A total of 518 participants were enrolled in the study, all of whom completed questionnaires and underwent serological tests, gastroscopy, and histopathologic biopsy. After eliminating samples with incomplete data, 443 effective samples were included (an effective rate of 85.5%). Case inclusion was continuous. There were 228 men and 215 women, accounting for 51.5% and 48.15% of the study population, respectively. GIM was detected in 87 participants, for an overall detection rate of 19.6%.
Comparison of PG between the GIM and healthy gastric mucosa groups
Serum PG results showed that differences in concentrations of PGI (Z = 1.44, p = 0.032) and PGII (Z = 1.63, p = 0.010) were significant between the GIM and healthy gastric mucosa groups. The median PGI and PGII values of the GIM group were 129.24 and 12.49 ng/mL, respectively, both of which were higher than that of the healthy group. Conversely, the median PGI/PGII ratio (PGR) in the healthy group was 12.24 ng/mL, which was higher than that of the GIM group (p = 0.008). There was no significant difference in G-17 level between the groups (Z = 1.24) (Table 1).
Comparison of serum PGI, PGII, and G-17 levels between participants with healthy gastric mucosa and those with gastric intestinal metaplasia
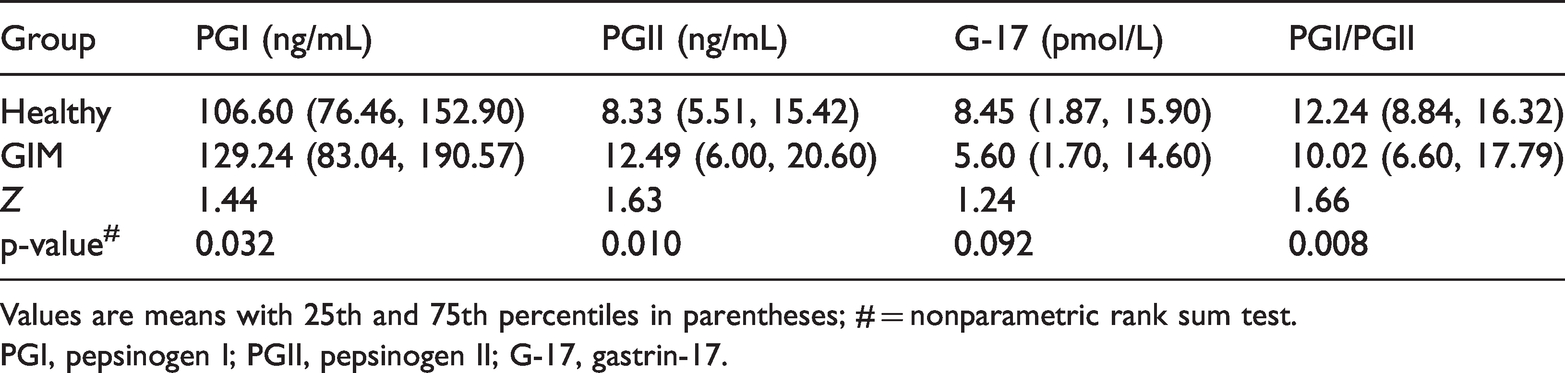
Values are means with 25th and 75th percentiles in parentheses; # = nonparametric rank sum test.
PGI, pepsinogen I; PGII, pepsinogen II; G-17, gastrin-17.
Correlation analysis between PG and GIM
PGI, PGII, and PGR were used as independent variables for a decision tree analysis of GIM. A receiver operating characteristic curve was used as the continuous variable to obtain the following results. Optimal prediction of GIM was obtained when PGI was 127.20 ng/mL and PGII was 11.30 ng/mL (the point of tangency). According to the decision tree classification cut-off points, PGI was divided into groups: ≤127.20 and >127.20 ng/mL, and PGII was divided into groups ≤11.30 and >11.30 ng/mL. The detection rate of GIM was higher when PGI was >127.20 ng/mL than when PGI was ≤127.20 ng/mL (χ2 = 8.63, p = 0.03) (Figure 1). The detection rate of GIM was higher when PGII was >11.30 ng/mL than when PGII was ≤11.30 ng/mL (χ2 = 10.45, p = 0.011) (Figure 2). The detection rate of GIM was lower when the PGR was between 11.960 and 17.870 compared with >17.870 or <11.960 (χ2 = 13.907, p = 0.034) (Figure 3).

Decision tree analysis of gastric intestinal metaplasia (GIM) and pepsinogen I (PGI), indicating higher detection of GIM when PGI was > 127.20 ng/mL than when PGI was ≤127.20 ng/mL
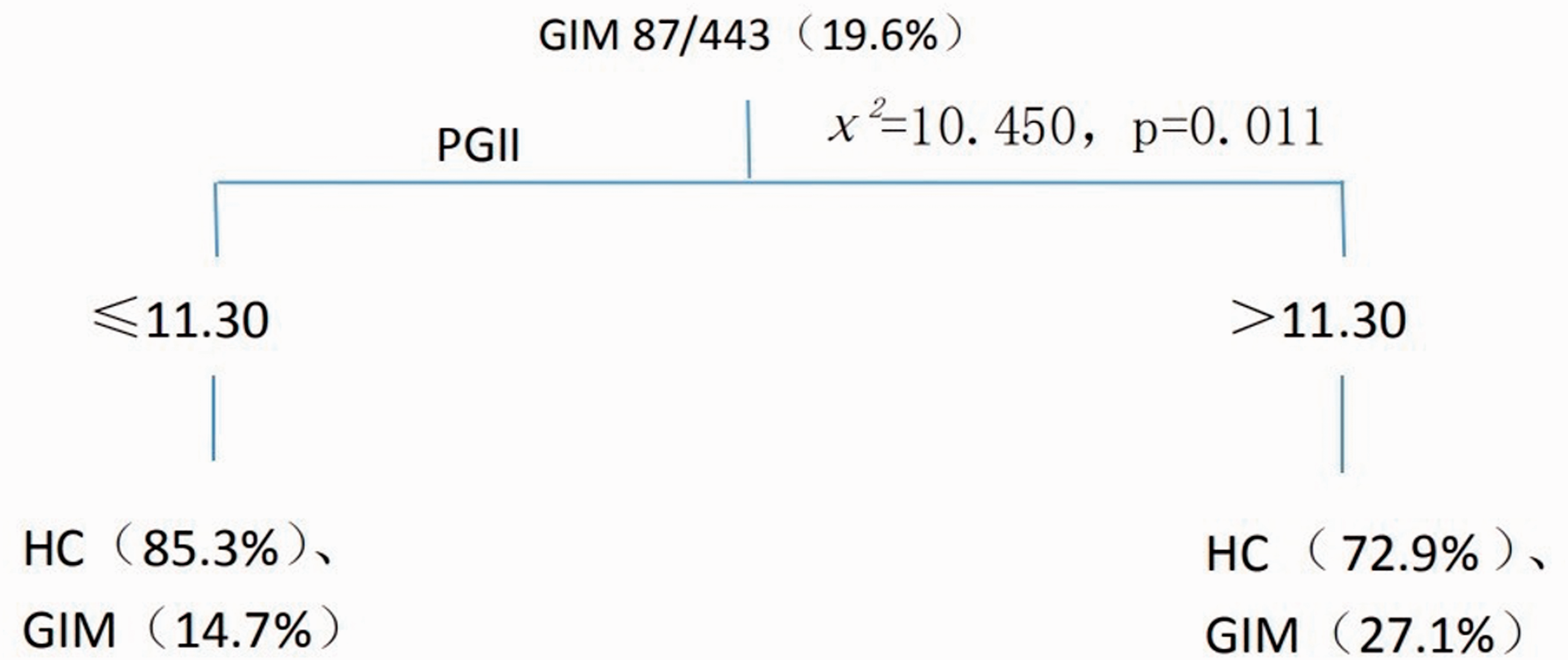
Decision tree analysis of gastric intestinal metaplasia (GIM) and pepsinogen II (PGII), indicating higher detection of GIM when PGII was > 11.30 ng/mL than when PGII was ≤11.30 ng/mL

Decision tree analysis of gastric intestinal metaplasia (GIM) and pepsinogen I/pepsinogen II ratio (PGR), indicating lower detection of GIM when PGR was between 11.960 and 17.870 compared with >17.870 or <11.960
Correlations between social demography, lifestyle, family history of gastrointestinal cancer, and GIM
The distribution of GIM differed in participants with different languages (χ2 = 10.44, p = 0.015); the proportion of GIM in the Mandarin group (29.8%) was higher than that in other language groups. The distribution of GIM in different age groups was significant (χ2 = 20.48, p < 0.001): the detection rate of GIM was higher in the older age group than in the younger age group, and the incidence was highest in those > 60 years old. The proportion of GIM in urban residents was higher than that in rural or township residents (χ2 = 6.98, p = 0.03). The detection rate of GIM in patients with a history of hyperlipidemia was higher than that in patients without hyperlipidemia or without examination (χ2 = 8.08, p = 0.018). We found no significant differences in the distribution of GIM in patients of different sexes and with or without smoking and drinking habits, family history of gastrointestinal cancer, Hp infection, diabetes, or hypertension (Table 2).
Comparison of the detection rate of gastric intestinal metaplasia in different populations

Logistic regression analysis of GIM
Logistic regression analysis was performed for the correlation factors that were significant in the single factor analysis; that is, PGI, PGII, PGR, Mandarin as the native language, age, urban residence, and history of hyperlipidemia. Regression results showed that age and PGI were statistically significant, and the odds ratio (OR) value of age was 1.66 (p < 0.001), indicating that in participants over 40 years old, GIM risk increased by a factor of 1.66 for every 10 years of age over the age of 40 years. The risk of GIM in individuals with PGI > 127.20 ng/mL was 1.59 times higher than that individuals with PGI ≤ 127.20 ng/mL (p = 0.047) (Table 3).
Logistic regression analysis of gastric intestinal metaplasia

OR, odds ratio; CI, confidence interval; PGI, pepsinogen I level.
Discussion
At present, gastric cancer remains the third leading cause of death related to cancer worldwide. 1 GIM is an important precancerous lesion that may increase the risk of gastric cancer.16,17 Therefore, clarifying the screening indicators of GIM is very important in early gastric cancer screening. At present, the diagnosis of GIM mainly relies on gastroscopy and histopathologic biopsy, but endoscopy is an invasive procedure that is poorly tolerated, and dynamic monitoring of GIM is difficult. Therefore, it would be of great clinical value to establish a noninvasive method, such as serological examination, to screen for changes in the intestinal metaplasia of the gastric mucosa.
Studies have suggested that serum PGR may be a biomarker of precancerous gastric lesions. 18 Consistent evidence demonstrates that the absolute value of PGI combined with PGR is the best serological indicator to judge the status of the gastric fundus mucosa, and it is known as a “serological biopsy” of gastric mucosa. 19 Tu et al. 20 noted that a very low PGI level (<30 ng/mL vs. >70 ng/mL) resulted in increased incidence of precancerous lesions or gastric cancer, and that a higher PGII level or a lower PGR was associated with a dose–response relationship with precancerous lesions or gastric cancer.
In this study, PGI level was correlated with GIM, but PGII, PGR, and G-17 were not. The safety value range of PGI was ≤ 127.20 ng/mL, and the detection rate of intestinal metaplasia of gastric mucosa was 1.59 times higher in participants with PGI > 127.20 ng/mL than in participants with PGI ≤ 127.20 ng/mL. This index and threshold value can be used as a useful reference for the screening of GIM. However, serological screening for GIM has not yet been reported. It is generally believed that PG and G-17 are closely related to development of gastric mucosal lesions, reflecting atrophy of the gastric mucosa, and can better predict the risk of gastric cancer.21–23
The incidence of GIM was higher in people over 40 years old in our study, with the detection risk of GIM increasing by a factor of 1.66 for every 10 years over the age of 40 years. Furthermore, GIM incidence was the highest in those over 60 years old. Therefore, screening of GIM should be increased in people over 40 years old. Bellolio et al. 24 reported that the risk of GIM over the age of 50 years was significantly increased, and Jiang et al. 25 reported that the incidence of GIM in Yangzhou, China, was highest between 50 and 60 years old.
In conclusion, age and serum PGI level were risk factors related to GIM in Guangdong, China. Screening of GIM should be increased in people over 40 years old, and a PGI value > 127.20 ng/mL can be used as a serological indicator for gastroscopy. However, our study population consisted only of residents in Guangdong, China, and the sample size was limited. Further evaluation is needed before this indicator can be applied in clinical practice, and the accuracy of the critical threshold value needs to be verified in multi-center studies with larger sample sizes and high-quality clinical data.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a fund from Science, Technology & Innovation Commission of Guangzhou Municipality, the project of people’s livelihood science and technology (no. 201803010037).
Author contributions
Xujuan Liu was involved in the study concept and design, data interpretation, and drafting of the manuscript. Min Zhang performed statistical analysis of the samples and analyzed the data. Riyu Luo and Keran Mo recruited the participants and collected the clinical samples. Xingxiang He was involved in the study and design and critical revision of the manuscript.