
Abstract
Objective
To investigate the relationship between levels of toll-like receptor 4 (TLR4) protein in aortic tissue and the severity of atherosclerosis in patients undergoing coronary artery bypass graft (CABG) surgery.
Methods
Samples of ascending aorta and renal artery were collected from patients undergoing CABG surgery or kidney donation, respectively. TLR4 levels were determined by immunohistochemistry. Coronary angiography was performed to determine atherosclerosis severity via Gensini score.
Results
TLR4 was present at high levels in aortic tissues from patients (n = 46), and was absent from renal artery tissue (controls; n = 11). There was a significant positive correlation between Gensini score and TLR4 level in the patient group.
Conclusions
TLR4 may play an important role in atherosclerosis and could be a potential therapeutic target for treatment of coronary artery disease. Discarded aortic tissue obtained during CABG surgery provides a new approach to the study of the pathogenesis of atherosclerosis.
Introduction
The response-to-retention hypothesis is widely accepted to explain the pathogenesis of atherosclerosis.1–3 This hypothesis states that lipoproteins (mainly low-density lipoprotein [LDL]) are retained in the intima of arteries under certain conditions and are oxidatively modified by the extracellular matrix. These oxidized lipoproteins stimulate the transformation of monocytes to macrophages that then convert to foam cells by phagocytosis of oxidized LDL, resulting in local vascular nonadaptive inflammation.4–7
Toll-like receptors (TLRs) are pathogen recognition receptors present on the surface of mammalian somatic cells. 8 TLRs are closely related to the innate immune system; they initiate signalling pathways within cells and activate the immune response by recognizing specific structures that are shared by pathogens but not by host cells.9–11 To date, 13 members of the TLR family have been identified, of which TLR4 is closely linked to atherosclerosis. 12
The aim of the current study was to investigate the relationship between levels of TLR4 in aortic tissue and the severity of atherosclerosis in patients who underwent coronary artery bypass graft (CABG) surgery.
Patients and methods
Study population
The study enrolled patients scheduled to undergo CABG surgery at Qianfoshan Hospital, Jinan, China, between September 2012 and September 2013. Indications for CABG included: unstable angina with medication failure; disease of the left main coronary artery or the bifurcate part of arteries; disease of all coronary vessels, especially combined with cardiac dysfunction or diabetes; disease of two coronary vessels, combined with high-grade stenosis of proximal left anterior descending artery; (v) disease with percutaneous coronary intervention failure. Exclusion criteria were: aged <18 years; concomitant valvular surgery or MAZE procedures. Samples of ascending aortic tissue were collected during surgery. Healthy subjects who were donating a kidney to a blood relative were recruited as controls, and provided renal artery tissue free from atherosclerotic lesions. Data regarding body mass index (BMI), smoking status, hypertension (blood pressure ≥140/90 mmHg) and diabetes mellitus were obtained from all participants.
The Ethics Committee of Qianfoshan Hospital, Jinan, China, approved the study, and all subjects provided written informed consent prior to enrolment.
Laboratory analyses
Peripheral blood was taken from all study participants 1 day after enrolment following an overnight fast. Blood (20 ml) was drawn into tubes containing anticoagulant (sodium citrate, 3.2%), mixed, centrifuged (−4℃, 2500
Immunohistochemistry
Each participant provided a minimum of two samples of arterial tissue. Tissue was fixed in formalin, embedded in paraffin wax and cut into 3-µm sections. Immunohistochemistry for TLR4 was performed using a Ready-to-use Handy Immunohistochemistry MaxVision™ Kit (Maixin Biotechnology Development Co., Ltd, Fuzhou, China), according the manufacturer’s instructions. Briefly, sections were de-waxed and hydrated, and endogenous peroxidase was inactivated by incubation in 3% hydrogen peroxide. Sections were then incubated with rabbit antihuman TLR4 polyclonal antibody (1:100 dilution; Beijing Biosynthesis Biotechnology Co., Beijing, China) at 4℃ overnight. Incubation with secondary antibody was performed according to the manufacturer’s instructions (Maixin Biotechnology Development Co., Ltd) and labelled cells were visualized using a 3,3′-Diaminobenzidine (DAB) developing kit (Maixin Biotechnology Development Co., Ltd) according to the manufacturer’s instructions. Sections were then counterstained with haematoxylin, dehydrated, and fixed with neutral resin.
Staining was evaluated using a fully automated microscopic image analysis system (FSX100, Olympus Tokyo, Japan). The integrated optical density of each sample was determined, and the mean value for each patient was calculated and defined as TLR4 level.
Coronary angiography
In the patient group, coronary angiography was performed on both the left and right arteries and on multiple locations, according to the Judkins method. 13 Angiography was recorded and analysed offline by cardiologists (F.Z. and D.W.), who quantitatively assessed the atherosclerotic lesions.
Coronary artery assessment
Coronary calcification was quantified according to National Heart, Lung, and Blood Institute standards 14 : none (no shadow); mild (light, blurred shadows visible during beating, with no clear shadows when the heart is not beating); moderate (clear shadows visible during beating and no shadows seen when the heart is not beating); and severe (shadows clearly visible at all times).
Coronary artery stenosis was scored based on the American Heart Association 15-segment model (Gensini score), which multiplies a score based on degree of occlusion, with a factor related to the importance of the lesion location in the coronary arterial tree. 15
Statistical analyses
Data were presented as mean ± SD. Student’s t-test and χ2-test were used to analyse continuous normally distributed variables and categorical variables, respectively. The relationship between TLR4 and Gensini score was evaluated using linear correlation analysis. Statistical analyses were performed using SPSS® version 12.0 (SPSS Inc., Chicago, IL. USA) for Windows®. P-values <0.05 were considered statistically significant.
Results
Demographic and clinical characteristics of patients undergoing coronary artery bypass graft surgery and healthy control subjects included in a study to investigate the correlation between levels of toll-like receptor 4 protein in arterial tissue and severity of atherosclerosis.
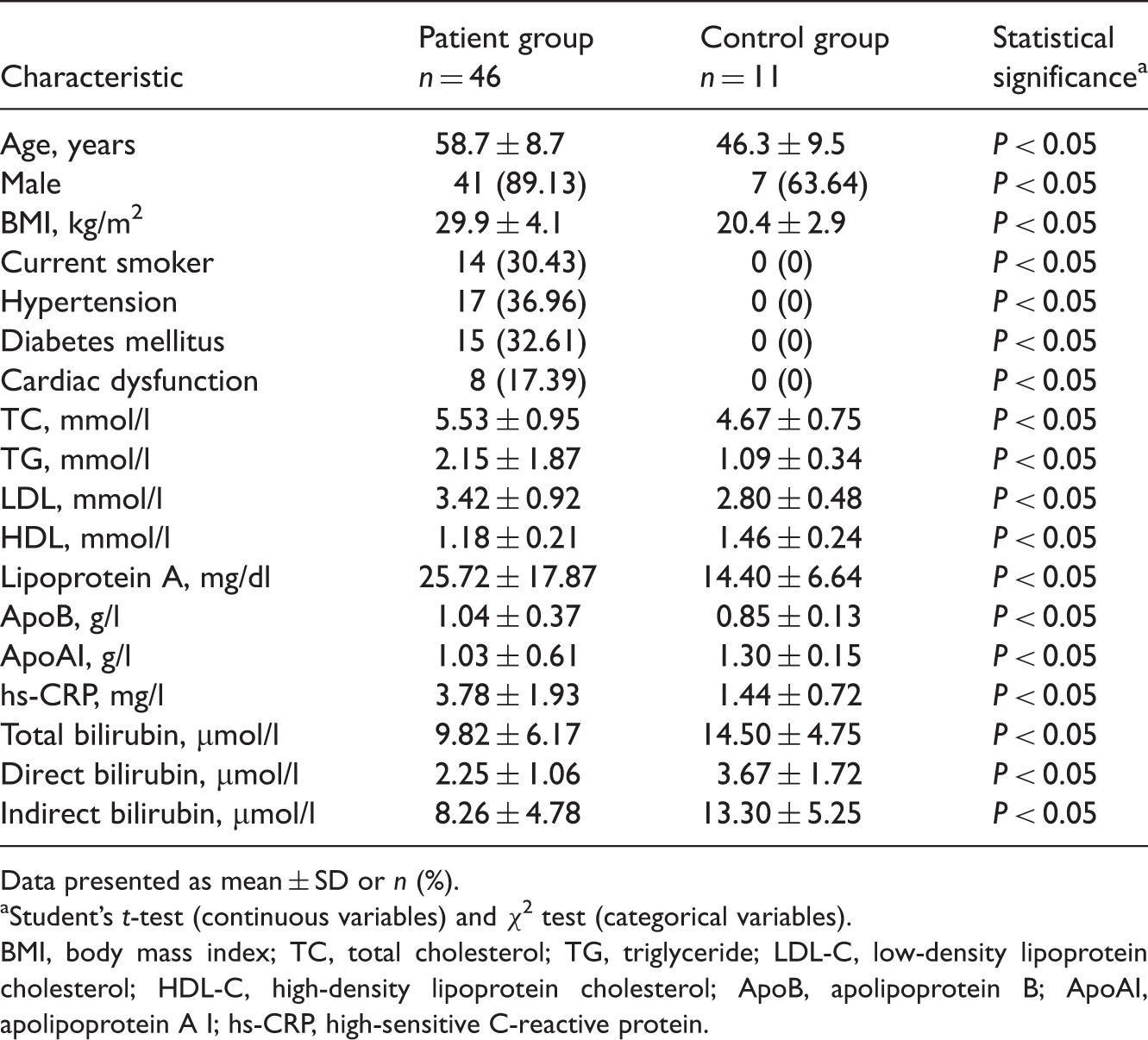
Data presented as mean ± SD or n (%).
aStudent’s t-test (continuous variables) and χ2 test (categorical variables).
BMI, body mass index; TC, total cholesterol; TG, triglyceride; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; ApoB, apolipoprotein B; ApoAI, apolipoprotein A I; hs-CRP, high-sensitive C-reactive protein.
Plasma TC, TG, LDL-C, LpA, ApoB and hs-CRP values were significantly higher, and HDL-C, ApoAI TBIL, DBIL and IBIL values were significantly lower, in the patient group than the control group (P < 0.05 for each comparison; Table 1).
Representative light photomicrographs of TLR4 immunohistochemical staining are shown in Figure 1. The presence of TLR4 was indicated by clusters or strips of uneven, diffuse, dark-brown staining in tissue from patients (Figure 1(b)). Tissue samples from control subjects were free of TLR4-specific staining (Figure 1(a)).
Representative light photomicrographs of toll-like receptor 4 (TLR4) immunohistochemistry in (a) nonatherosclerotic renal artery, and (b) atherosclerotic ascending aorta. TLR4 indicated by clusters or strips of uneven, diffuse, dark-brown staining in (b). Scale bar, 50 µm. The colour version of this figure is available at: http://imr.sagepub.com.
The mean Gensini score in the patient group was 75.72 ± 18.38 and the mean TLR4 level was 651.56 ± 131.97. There was a significant positive correlation between Gensini score and TLR4 levels in aortic tissue in the patient group (r = 0.791, P < 0.05; Figure 2)
Linear correlation analysis of the relationship between coronary artery stenosis (Gensini score
15
) and toll-like receptor 4 (TLR4) levels in tissue samples from the ascending aorta of 46 patients undergoing coronary artery bypass graft surgery.
Discussion
High levels of TLR4 are present on macrophages and endothelial cells in human atherosclerotic lesions. 16 TLRs are type I transmembrane proteins with extracellular domains, transmembrane regions and intracellular domains. 17 TLR4 induces an immune response via signal transduction, leading to the secretion of inflammatory factors and cytokines.18,19 The TLR4 pathway is triggered by the formation of foam cells from macrophages, which induces TLR4 expression 20 and impairs endothelial cells via activating nuclear factor-κB (NF-κB) and upregulating NF-κB downstream genes.21,22 TLR4 is present at high levels in atherosclerotic lesions infiltrated by macrophages and is co-located with macrophages. 23 Therefore, TLR4 may play a significant role in the initiation and development of atherosclerosis. 24
The extent of atherosclerosis is positively correlated with plasma TC, LDL-C and TG concentrations, and negatively correlated with HDL-C concentration. 25 Plasma TC, LDL-C and TG values were significantly higher and HDL-C values significantly lower in patients than in controls, in the present study. Plasma ApoB, ApoAI and LpA are also closely related to atherosclerosis.26,27 Around 90% of ApoB is distributed in LDL-C, and serum ApoB levels may therefore reflect LDL-C concentrations. Plasma ApoB concentrations were significantly higher in patients than controls in the present study. ApoAI is the main structural protein of HDL-C and plays a role in resisting atherosclerosis via activating lecithin:cholesterol acyltransferase, resulting in the esterification of cholesterol and reverse cholesterol transport. 28 Plasma ApoAI concentrations were significantly lower in patients than in controls in the current study, therefore it is our view that. LDL-C:ApoB, LDL-C:LpA and HDL-C:ApoAI ratios may be clinically more valuable than their absolute values.
C-reactive protein is a biomarker of atherosclerotic inflammation 29 and is regarded as a predictor of cardiovascular events. 30 Plasma hs-CRP concentrations were significantly higher in patients than in controls in the present study. Bilirubin is known to eliminate free radicals and retard oxidation, and a significant decrease in plasma bilirubin may be a risk factor for atherosclerosis. 31 Plasma TBIL, DBIL and IBIL values in patients in the current study were significantly lower than values in the control group.
Experimental and clinical studies have found that high TLR4 levels in aortic tissue thin the atheroma fibrous cap and make the lipid core larger, resulting in unstable atheroma and a significant increase in the incidence of sudden cardiovascular events. 32 TLR4 may represent a new biomarker for the inflammatory response in atherosclerotic lesions.
A study of 2995 autopsy subjects found a close correlation between the extent of aortic and coronary atherosclerosis, indicating that the extent of aortic atherosclerosis reflects the severity of coronary atherosclerosis. 33 The Gensini score is a quantitive index of the distribution, size and extent of coronary atherosclerotic stenosis. We found a significant positive correlation between Gensini score and TLR4 level in aortic tissue in the present study.
The present study has several limitations, most notably the control group. We used renal artery tissue from healthy kidney donors as control, since aortic tissue can rarely be collected from healthy individuals, there is no evidence that TLR4 expression is tissue specific, and the renal artery and aorta have similar structure and blood flow shear stress. The control group differed significantly from the patient group in all demographic and clinical characteristics, many of which may have been responsible for the findings, irrespective of the severity of atherosclerosis. The use of immunohistochemical staining rather than direct quantification of TLR4 further limits the validity of this study.
The majority of studies of atherosclerosis have been performed using animal models, with very few conducted using human autopsy subjects. Animal models are developed artificially over a short time, whereas human atherosclerosis progresses naturally over decades. It is therefore difficult to equate these types of study in terms of aetiology, pathophysiology and pathogenesis. The current study of discarded aortic tissue obtained during CABG surgery provides a new approach to the study of the pathogenesis of atherosclerosis. TLR4 may play an important role in atherosclerosis and could be a potential therapeutic target for treatment of coronary artery disease.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This study was supported by the Foundation for Outstanding Young Scientists in Shandong Province (No. 2009BSB01312).