
Abstract
Objective
To analyse the association between serum interleukin (IL)-23 mRNA levels and clinical characteristics in patients with systemic lupus erythematosus (SLE).
Methods
Serum IL-23 and IL-17 mRNA levels were quantified using real-time reverse transcription–polymerase chain reaction in patients with SLE and healthy controls. Disease activity was assessed using the SLE Disease Activity Index-2k.
Results
A total of 108 patients with SLE and 60 control subjects were recruited. IL-23 mRNA levels were significantly higher in patients with SLE compared with healthy controls, and in patients with SLE and renal involvement compared with SLE alone. IL-23 mRNA levels were not different between patients with active or inactive SLE, but the IL-17/IL-23 ratio was significantly higher in patients with active disease. IL-17 and IL-23 mRNA levels were strongly correlated.
Conclusions
Serum IL-23 mRNA was elevated in patients with SLE and renal disease, and the IL-17/IL-23 ratio was higher in patients with active SLE. These findings suggest that IL-23 may play an important role in SLE pathogenesis, and that the IL-17/IL-23 ratio may be useful biomarker for active disease.
Introduction
Systemic lupus erythematosus (SLE) is a chronic idiopathic systemic autoimmune disease characterized by the production of various autoantibodies, complement activation, immune complex deposition and subsequent inflammation, which results in severe damage particularly affecting the joints, skin, brain and kidneys.1,2 Although SLE involves both innate and adaptive immune dysregulation, 3 the relative importance of the cytokines operative in these systems is unclear.
Since the identification of Th17 cells as a third subset of CD4+ T-effector cells,4,5 there has been much interest regarding their role in the pathogenesis of autoimmune diseases including rheumatoid arthritis (RA), 6 systemic sclerosis, 7 multiple sclerosis 8 and SLE. 9 The activation and maturation of Th17 lymphocytes relies on adequate T-cell receptor expression, co-stimulatory molecules and cytokines such as interleukin (IL)-6 and IL-21, which play a pivotal role in the differentiation of naïve CD4-positive cells. 10
Interleukin-23 is another important cytokine in the development, expansion and proliferation of the Th17 cell population.10,11 High serum levels of IL-23 have been demonstrated in patients with SLE.12–14 Taken together, these findings suggest that abnormally active IL-23 may contribute to the pathogenesis of SLE. Research on the potential relationship between IL-23 and the clinical characteristics of SLE has been limited due to lack of data from longitudinally followed patient cohorts. The present study aimed to examine the association between serum IL-23 levels and disease expression in SLE, with respect to disease activity and organ involvement, in Chinese Han patients followed-up over a 2-year period. The relationship between serum IL-23 and IL-17 levels was also examined.
Patients and methods
Study population
Consecutive patients aged >18 years who met the 1982 American College of Rheumatology (ACR) criteria 15 for the classification of SLE were recruited from the Department of Rheumatology and Immunology, China–Japan Union Hospital of Jilin University, Changchun, China between April 2010 and June 2013. Patients who were receiving therapy with biological agents were excluded from the study. Control subjects were recruited from among individuals who had not been diagnosed with SLE and were seeking a routine health check-up at the Physical Health Examination Centre of Jilin University. All patients and control subjects included in this study provided written informed consent. The study protocol was approved by the local ethics committees of the China–Japan Union Hospital of Jilin University and the Jilin Province People’s Hospital, Changchun, China.
Clinical assessments and procedures
Disease activity was recorded once per month at each clinic visit according to the SLE Disease Activity Index-2k (SLEDAI-2k). 16 Other variables recorded at study entry included patient age, sex, ethnicity, disease duration and drug therapy. Patients were recorded as having SLE with renal disease if renal criteria of the ACR classification were met or if there was involvement in the renal domains of the SLEDAI-2k at any time during the 2-year study period. Active renal disease was defined as a score >0 in any of the renal domains of the SLEDAI-2k. Patients received standard-of-care therapy throughout the study and patient follow-up was scheduled by the treating physician.
At each monthly clinic visit, a 5-ml sample of peripheral venous blood was drawn from each study participant following an overnight fast and left at room temperature for 60 min. Blood samples were then centrifuged at 1000
Quantitative RT–PCR analysis of IL-23 and IL-17 mRNA
Total RNA (including microRNAs) was extracted from 200 µl of serum using the QIAGEN miRNeasy Mini Kit (QIAGEN GmBH, Hilden, Germany) according to the manufacturer’s instructions. The purity and concentration of RNA were determined using a dual-beam ultraviolet spectrophotometer (Eppendorf, Hamburg, Germany). Reverse transcription was performed using a TaqMan® Reverse Transcription Kit (Applied Biosystems, Foster City, CA, USA) in a total reaction volume of 100 µl with 2 µg of total RNA. Quantitative real-time reverse-transcription polymerase chain reaction (RT–PCR) was performed in a total reaction volume of 25 µl using TaqMan® Fast Mix (Applied Biosystems). The specific primers used were as follows: IL-23, forward 5′- ACACATGGATCTAAGAGAAGAGG -3′and reverse, 5′- CTATCAGGGAGCAGAGAAGG -3′; IL-17 A, forward,5′ CTCCAGAAGGCCCTCAGACTAC-3′ and reverse, 5′-AGCTTTCCCTCCGCATTGACACAG-3′; β-action forward 5′-GATCATTGCT CCTCCTGAGC-3' and reverse 5′-ACTCCTGCTTGCTGATCCAC-3′. Assays were performed using a 7500 Fast real-time PCR system (Applied Biosystems). PCR conditions were as follows: preliminary denaturing at 95℃ for 2 min, followed by 40 cycles of denaturation at 95℃ for 10 s and annealing/extension at 58℃ for 20 s. Amplification specificity was checked by melting-curve analysis. The 2 -ΔΔCT method was used to calculate the relative abundance of target gene expression generated by Rotor-Gene Real-Time Analysis Software (version 6.1.81, Corbett Research Pty Ltd, Sydney, Australia). For each cDNA, the target gene mRNA level was normalized to the β-actin mRNA level. All experiments were performed in triplicate.
Statistical analyses
Statistical analyses were performed using GraphPad Prism® software, version 5.0d, 2010 (GraphPad Software Inc., San Diego, CA, USA) and SPSS® 19.0 (SPSS Inc., Chicago, IL, USA) for Windows®. Data were expressed as mean ± SD, unless otherwise indicated. Unpaired Student’s t-test was used in this study. Correlations between IL-23 and IL-17 levels and SLE disease activity or renal involvement were determined using Spearman’s Rank test. Mann–Whitney U-test and χ2-test were used to compare groups of continuous and categorical data, respectively. A P value of <0.05 was considered statistically significant.
Results
A total of 108 patients with SLE and 60 control subjects were recruited. Patients and control subjects were Chinese Han people and were matched for age and sex. Of the patients with SLE, 88 (81.5%) were female and 20 (18.5%) were male. The mean age of patients with SLE at diagnosis was 43 ± 13.3 years and the mean age at disease onset was 32 ± 15.2 years. Nephritis was observed in 72.2% (78/108) of patients. Nearly two-thirds of the patients (71/108, 65.74%) were treated with prednisone or equivalent. A total of 32 patients were lost to follow-up after transferring to another hospital; the remaining 76 patients (70.4%) were followed-up longitudinally for 2 years. In these patients, disease activity at study entry was highly variable with a median (range) SLEDAI-2k score of four (0–26); 32 patients had SLEDAI-2k scores equal to or higher than the median (active disease, SLEDAI-2k ≥4) and 44 patients had scores lower than the median (inactive disease, SLEDAI-2k <4).
At study entry, serum IL-23 mRNA levels were significantly higher in the 108 SLE patients compared with the 60 healthy controls (P < 0.05; Figure 1A). There were no significant differences in serum IL-23 mRNA concentrations among SLE patients (n = 108) according to age or sex (data not shown), and no significant difference was observed between patients with inactive or active SLE (Figure 1B). IL-23 levels were not significantly different between patients with SLE who received treatment with prednisone (n = 71) compared with patients who did not receive prednisone (n = 37; Figure 1C).
Serum concentrations of interleukin (IL)-23: A, in 108 patients with systemic lupus erythematosus (SLE; abbreviated as SEL in graphs) and 60 healthy control subjects (Student’s t-test); B, in relation to disease activity, measured by SLE Disease Activity Index-2k (SELDAI-2k in graph), in patients with SLE (n = 32 with active disease; n = 44 with inactive disease; Mann–Whitney U-test); C, in patients with SLE, with (n = 71) or without (n = 37) steroid treatment (χ2-test).
In patients followed-up for 2 years, the ratio of IL-17/IL-23 mRNA was significantly higher in patients with active SLE compared with those with inactive disease (P < 0.05; Figure 2) and healthy control subjects (P < 0.01; Figure 2). A strong positive correlation between serum IL-23 and IL-17 mRNA levels was determined at study entry and after 2 years’ follow-up (r = 0.701, P < 0.05).
Systemic lupus erythematosus (SLE) Disease Activity Index-2k (SELDAI-2k in graph) correlated with interleukin (IL)-17/IL-23 ratio in SLE. IL17/IL-23 ratio for patients with active SELDAI-2k (n = 32) was significantly higher than that for inactive SELDAI-2k (n = 44) and healthy control subjects (n = 60); Student’s t-test.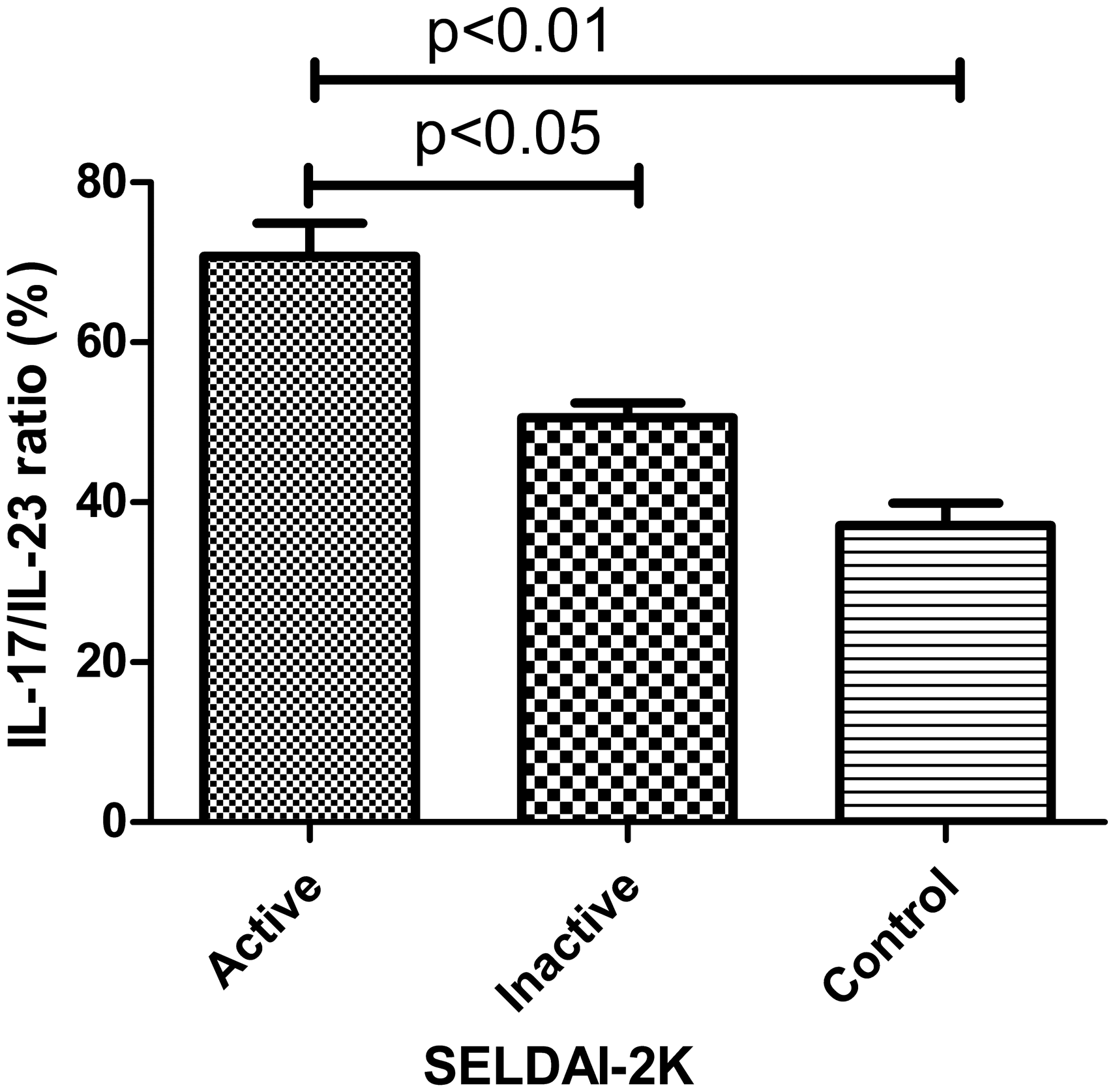
Serum IL-23 concentrations were significantly increased in patients determined to have SLE and renal disease according to the ACR classification, or involvement in the renal domains of the SLEDAI-2k (n = 78), compared with patients without renal involvement (n = 30, P < 0.05; Figure 3) or healthy control subjects (P < 0.01; Figure 3).
Serum interleukin (IL)-23 concentrations in patients with systemic lupus erythematosus, with (n = 78) or without (n = 30) renal involvement, and healthy control subjects (n = 60).
Discussion
The role of IL-23 in the pathogenesis of autoimmune diseases is now well accepted. In the present study, serum IL-23 mRNA levels were found to be significantly elevated in patients with SLE compared with healthy controls, which is in agreement with previously published reports,12,13 and indicates that IL-23 may also play an important role in the pathogenesis of SLE.
Systemic lupus erythematosus is a highly heterogeneous disease. Characterization of subgroups of patients with SLE into specific disease phenotypes, such as those with major organ involvement, may facilitate the investigation of disease pathogenesis. For example, lupus nephritis affects over 50% of patients with SLE and is a major cause of morbidity. 17 Despite significant advances in the understanding of interactions between immune cells, soluble factors and resident kidney cells, the precise pathophysiological mechanisms that underlie the development of lupus nephritis remain unclear. 18 This uncertainty means that treatment of lupus nephritis depends on the use of nonselective and toxic immunosuppressive regimens. 19 Characterization of the cytokines involved in the pathogenesis of SLE and development of lupus nephritis may identify potential therapeutic targets. In the current study, serum IL-23 levels were shown to be significantly elevated in patients with SLE and renal involvement. These results suggest that IL-23 is involved in the pathogenesis of renal disease in SLE and, as such, could represent a possible biomarker for renal involvement in SLE and a therapeutic target in this subgroup of patients. Published research has demonstrated that the IL-23/IL-17 pathway is activated in lupus-prone mice and is associated with increased immunoglobulin deposition and complement activation in the kidney, 20 further indicating an important role for IL-23 in SLE renal pathology.
Imbalances in cell subset ratios relevant to Th17 activity, such as Th17/regulatory T cells, Th1/Th2, or Th17/Th1, correlate with disease activity in autoimmune conditions including RA, SLE, lupus and inflammatory bowel disease.21–24 Cytokine ratios within the same axis may also be a marker of immune pathway activation, as has been reported for the IL-17F/IL-22 ratio in chronic hepatitis C infection 25 or for the IL-17/transforming growth factor-β ratio in schizophrenia. 26 A significant positive correlation has been demonstrated between the IL-17/IL-6 ratio and SLE disease activity as assessed by SLEDAI-2k, 27 which is consistent with data from the present study showing a positive correlation between the IL-17/IL-23 ratio and disease activity. Although the current study demonstrated a significant elevation in serum IL-23 mRNA levels in patients with SLE compared with healthy controls, IL-23 protein levels were not evaluated and further study is required to determine if this cytokine is also increased in SLE.
In conclusion, the present study demonstrated that serum IL-23 mRNA levels were significantly elevated in patients with SLE compared with healthy controls, and in patients with SLE and renal disease compared with patients without renal involvement. Serum IL-23 concentrations did not differ by patient age and sex, or by steroid treatment. The present study also demonstrated that the IL-17/IL-23 ratio may act as maker for disease activity as determined by the SLEDAI-2k. Collectively, these findings suggest that IL-23 may be a potential biomarker and therapeutic target in SLE, including in SLE with renal involvement.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
The authors gratefully acknowledge the financial support provided by The Development of Science and Technology Plan Projects of Jilin (no. 2011Z015).