
Abstract
Objectives
The primary objective of this study was to compare the bioavailability of paracetamol, phenylephrine hydrochoride and guaifenesin in a new oral syrup with an established oral reference product. The secondary objective was to compare the safety of the new syrup and the reference product.
Methods
This was a single-centre, open-label, randomized, reference-replicated, crossover study. Healthy adult volunteers received one dose of syrup and two separate doses of a reference oral liquid formulation in a randomized sequence over three study periods, with a washout interval of ≥7 days between study periods. Blood samples were taken regularly postdose and analysed for paracetamol, phenylephrine hydrochoride and guaifenesin concentrations; adverse events were recorded.
Results
This study enrolled 45 subjects. For paracetamol and guaifenesin, the syrup and reference product were considered to be bioequivalent. Bioequivalence was not shown for phenylephrine hydrochoride. All adverse events were mild or moderate, most of which were considered formulation related.
Conclusions
The syrup did not reach bioequivalence with the reference product, as bioequivalence could not be shown for phenylephrine hydrochoride. This may be due to differences in the excipients between the two products. Both the syrup and the reference product had a good safety profile and were well tolerated.
Introduction
Paracetamol, phenylephrine hydrochloride and guaifenesin have been combined in over-the-counter remedies intended to relieve symptoms associated with colds and influenza (such as pain, nasal congestion, headache, fever and chesty cough) for a number of years.1–3
Paracetamol is a synthetic nonopiate acetyl ester derivative of p-aminophenol that produces analgesia and antipyresis. 4 The mode of action is believed to be through inhibition of prostaglandin synthesis. 4 Peak plasma drug concentration after administration (Cmax) is expected between 10 and 60 min, and elimination half-lives (t½) between 1 and 3 h have been reported. 4 Paracetamol is metabolized by hepatic enzymes, with 85–90% being transformed by glucuronidation and sulphation to inactive metabolites that are eliminated in the urine; a smaller amount is conjugated with cysteine and mercapturic acid, and only 5% of the drug is eliminated unchanged in the urine.4,5
Phenylephrine hydrochloride is a sympathomimetic selective α1-receptor agonist 6 and an effective nasal decongestant; 7 it activates β-adrenergic receptors only at much higher doses than those in over-the-counter remedies (>25 mg). 8 After oral administration, phenylephrine hydrochloride is readily and completely absorbed, with Cmax usually occurring between 45 min and 2 h; 9 systemic bioavailability is ∼38%. 9 Most of the orally administered drug is metabolized by sulphation, largely in the gut wall prior to reaching the liver, and elsewhere by oxidative deamination by monoamine oxidase.10,11 Both phenylephrine hydrochloride and its metabolites are eliminated in urine. 10 Elimination t½ between 2 and 3 h have been reported. 11
Guaifenesin belongs to the class of drugs known as expectorants and exerts its effects via indirect and direct mechanisms. The rate of mucociliary clearance is enhanced by guaifenesin 12 and guaifenesin has demonstrated an expectorant effect in patients with productive coughs. 13 Following oral administration, guaifenesin is rapidly and completely absorbed from the gastrointestinal (GI) tract, and Cmax of the unchanged active substance is observed between 15 and 30 min. 14 It is metabolized mainly into β-(2-methoxyphenoxy) lactic acid. 13 Plasma elimination t½ is ∼1 h. 14 Guaifenesin is excreted rapidly and almost completely through the kidneys: 81% and 95% of an administered dose appear in the urine within 4 and 24 h, respectively. 15
The primary objective of the present study was to compare bioavailability of the active ingredients paracetamol, phenylephrine hydrochloride and guaifenesin in a new oral liquid (syrup) formulation with the bioavailability of the same active ingredients in a reference oral liquid formulation. The secondary objective was to compare the safety of the new syrup and the reference product.
Methods
Study population
The study was conducted in PAREXEL International Unit, University of the Free State, Bloemfontein, South Africa. Participants were contacted by mobile phone text messages from a healthy volunteer database. Subjects who completed the study received compensation (4140 Rand). Participants volunteered for inclusion in the study. Male and female volunteers of any ethnic origin between 18 and 45 years of age and able to give written informed consent were included. Participants had to have a body mass index 18.5–30 kg/m2 and had to be in good physical health, with 12-lead electrocardiogram (ECG) and biochemical and haematological laboratory test results within the normal range.
Standard exclusion criteria, such as hypersensitivity to any of the test or reference substances, were applied. In addition, the study excluded subjects with the following contraindications to the reference product: hepatic or severe renal impairment; heart disease; hypertension; hyperthyroidism; diabetes; narrow angle glaucoma; porphyria; phaeochromocytoma. Other exclusion criteria were: any relevant history of disease which may significantly alter the absorption, distribution, metabolism or excretion of any drug substance; history within 5 years of malignancy or neoplastic disease (except basal-cell skin cancer); history of orthostatic hypotension, fainting or blackouts; clinically relevant chronic or acute infectious illnesses or febrile infections within 2 weeks prior to the first scheduled study period. Systolic blood pressure, diastolic blood pressure or pulse rate outside the normal range; ECG abnormalities; biochemical, haematological or any other laboratory variables outside the normal range; positive test results for HIV antibodies (Ab), hepatitis C virus-Ab, hepatitis B or C virus surface antigens, or hepatitis B virus immunoglobulin M; women who were pregnant or at risk of becoming pregnant; smoking within 3 months of study participation; history of alcohol and drug abuse; unwillingness to avoid alcohol and caffeine/theophylline-containing drinks within 24 h of, or during, study participation; inability or unwillingness to give appropriate consent or to be available for study visits. Participants were prohibited from ingesting substances that induce or inhibit cytochrome P450 3A4 or other such enzymes within 2 weeks of starting, and during, the study period.
Ethical approval
The study was approved by the Research Ethics Committee at the Research Division of the Faculty of Health Sciences, at the University of the Free State, 339 Bloemfontein 9300, Republic of South Africa (approval number 157/2011).
Study design
This was a single-centre, open-label, randomized, three-period, reference-replicated, crossover study. A crossover replicate design was chosen because the extensive first-pass metabolism of phenylephrine hydrochloride would lead to a high interindividual and possibly high intraindividual variation in the oral bioavailability of phenylephrine hydrochloride, as described in the literature;9,16,17 this design is recommended for highly variable drug products. 18
The study comprised a total of 5.5–7 weeks for each subject: 2 weeks of screening/inclusion and three study periods, each consisting of a 36-h in-house confinement (12-h overnight fast before and 24-h blood sampling period after formulation administration), with a washout interval of 7–10 days between each study period. The study was conducted between 10 January 2012 and 8 February 2012.
For each study period, subjects received either one single dose of the test syrup (T) or one single dose of the reference product (R). The reference product was administered twice (i.e. in two study periods). Subjects were randomized using computer-generated code to one of three formulation sequences: TRR, RRT or RTR.
Syrup and reference formulations
One single 30-ml dose of the test syrup (Novartis Consumer Health, Lincoln, NE, USA) and one single 20-ml dose of the reference product (Beechams® All-In-One; Wrafton Laboratories, Braunton, UK) contained 500 mg paracetamol, 10 mg phenylephrine hydrochloride and 200 mg guaifenesin. These dosages are the same as in products licensed in the USA and UK as Theraflu® and Beechams® All-In-One, respectively. The syrup also contained the excipient maltitol (9.5 g per unit dose), sodium benzoate, edetate disodium, sodium citrate, citric acid, propylene glycol, ethyl alcohol, acesulphame potassium, flavour 316282, FD&C Yellow no.6, Nat Orange flavour 576854, purified siliceous earth and purified water. The reference product also contained the excipient sorbitol (3.3 g per unit dose), glycerol, alcohol (96%), propylene glycol, sodium cyclamate, acesulphame potassium, sodium citrate, xanthan gum, citric acid, coughsweet flavour, Sunset Yellow (E110), Patent Blue V (E131) and water. Content assays were undertaken for both products, to confirm that their formulations were within the specified ranges. A poststudy assay was also undertaken to confirm the stability of phenylephrine in the syrup formulation. Both test and reference products were tested by analytical methods developed and validated internally by Novartis Consumer Health. The validation studies were completed as per International Conference on Harmonisation analytical method validation guidelines (Q2[R1]) 19 and executed under protocol.The syrup and the reference product were administered following an overnight fast using syringes as dosing devices.
In-house confinement
Subjects reported to the investigational clinic in the evening of day 1, ≥12 h before dosing on day 2 and received a standardized meal before fasting started. They remained in confinement until the morning of day 3. To standardize gastric emptying, subjects sat upright on the edge of their beds for 20 min after dosing. Thereafter, they were asked to lie on their right sides for the remainder of the first hour postadministration. Except for bladder voiding and ingestion of food and beverages, subjects remained recumbent until 8 h after administration of study medication, after which there were no restrictions concerning posture or movement. Subjects were given standardized food and drink during the in-house confinement (which avoided alcohol, caffeine/theophylline-containing products [i.e. coffee, green tea, tea, cola, cacao]), and foods or drinks that have an influence on pharmacokinetics (e.g. broccoli, Brussels sprouts, grapefruit, grapefruit juice, star fruit). Subjects were requested to refrain from unaccustomed strenuous exercise or sport during the study period.
Blood sampling and pharmacokinetic analyses
Samples of venous blood (65 ml) were collected from a forearm vein in each subject into tubes containing ethylenediamine tetra-acetic as an anticoagulant, to determine plasma concentrations of paracetamol, phenylephrine hydrochloride (unchanged) and guaifenesin at predose, 5, 10, 15, 20, 30, 40, 50, 60, 75, 90, 120, 150 and 180 min, and 4, 5, 6, 8, 10, 12, 16 and 24 h post dose, in each study period. Within 30 min of collection, blood samples were centrifuged at ∼2700
Plasma samples were assayed for paracetamol, phenylephrine hydrochloride and guaifenesin with a validated liquid chromatography with tandem mass spectrometry method (AB SCIEX, Framingham, MA, USA). One bioanalytical method was developed for the simultaneous determination of paracetamol and guaifenesin; a separate bioanalytical method was developed for the determination of phenylephrine hydrochloride. Concentrations were presented in mass per volume units. These bioanalytical methods were developed by the Bioanalytical Services Division, PAREXEL International Bloemfontein, South Africa. The methodology was fully validated to demonstrate compliance with the acceptance criteria of the standard operating procedures (SOPs) that were current at the Bioanalytical Services Division at the time of the analytical phase of study 147-A-102. The SOPs of the Bioanalytical Services Division are aligned with international regulatory guidelines. Personnel performing bioanalytical analyses were blinded to the randomization.
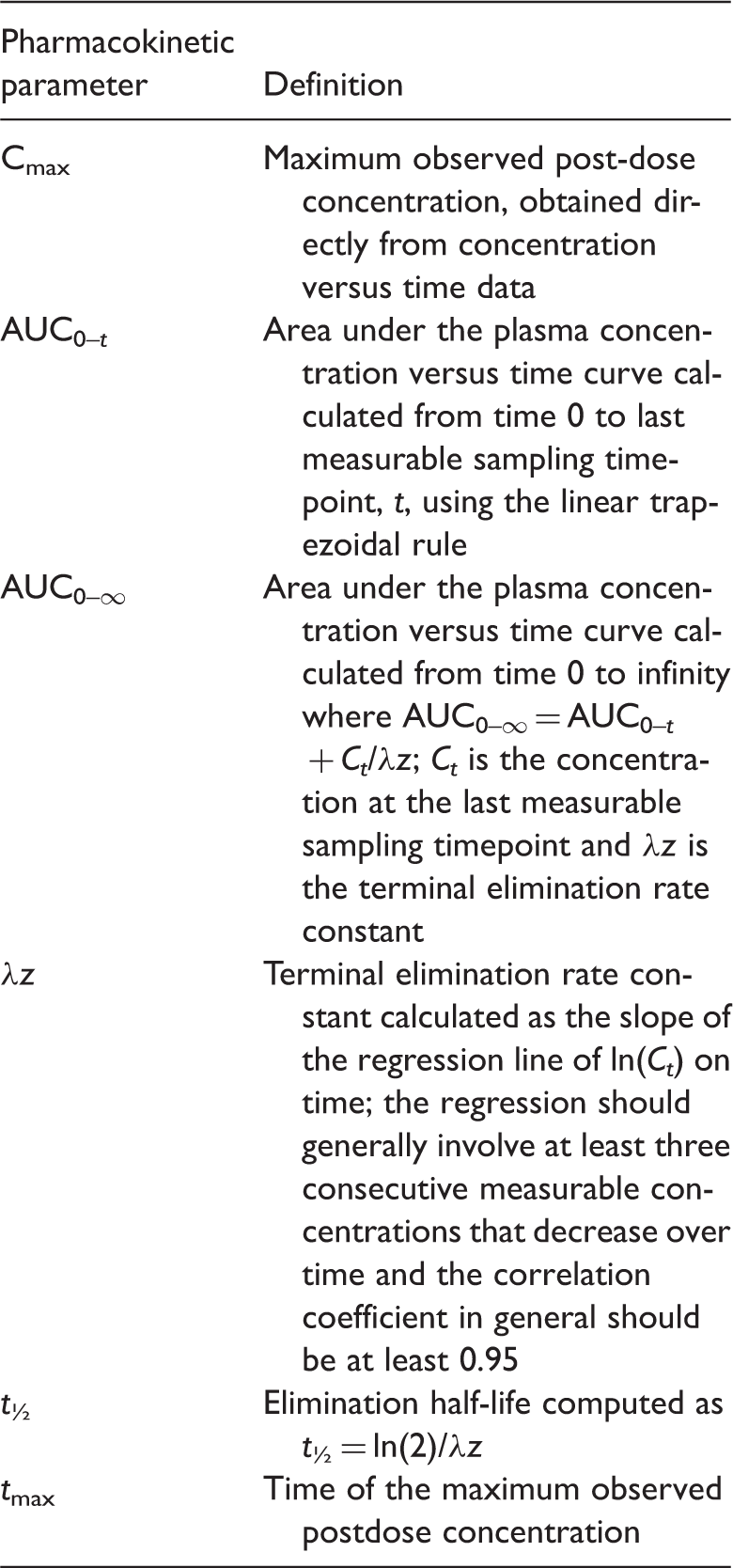
Definitions of pharmacokinetic parameters in a study comparing the bioavailability of a new oral syrup with an established oral liquid product, each containing 500 mg paracetamol, 10 mg phenylephrine hydrochloride and 200 mg guaifenesin per dose in adult healthy volunteers.
Physical and safety assessments
Standard physical examinations were conducted at screening and final visit. Vital signs were measured at screening, predose and just before discharge, during each study period. Adverse events (AEs) were recorded throughout the study.
Statistical analyses
The safety population consisted of all subjects who received at least one dose of formulation. The pharmacokinetic population consisted of all subjects who completed at least one period with each of the two formulations and who had no major protocol deviations that could impact the pharmacokinetics of paracetamol, phenylephrine hydrochloride or guaifenesin. In total, there was only one major protocol deviation: one subject took a prohibited medication during the washout period after the first treatment period. This subject was discontinued from the study due to the use of prohibited medication and was excluded from the pharmacokinetic population because he did not receive at least one dose of each treatment.
Demographic and other baseline data were presented using descriptive statistics for the safety population. Categorical variables were summarized by the number and percentage of subjects with each relevant characteristic. Continuous variables were summarized by calculating the mean, SD, median and minimum and maximum values.
For the pharmacokinetic population, plasma concentrations of paracetamol, phenylephrine hydrochloride and guaifenesin at each timepoint were summarized by calculating the arithmetic mean, SD, arithmetic coefficient of variation (CV), and the median, minimum and maximum values for each formulation; arithmetic means were plotted by formulation at each timepoint. Cmax, area under the plasma concentration versus time curve (AUC)0– t , AUC0–∞, λz and t½ (Table 1) for paracetamol, phenylephrine hydrochloride and guaifenesin were summarized by calculating the arithmetic mean and SD, geometric mean, between-subject geometric CV, median and minimum and maximum values for each formulation. tmax was summarized by calculating the median, first and third quartiles and minimum and maximum values for each formulation (Table 1). The difference between syrup and reference product for tmax was also summarized for each parameter.
Log-transformed AUC0– t and Cmax were compared between the two formulations using analysis of variance (ANOVA), with terms for sequence, formulation, period and subject nested within sequence as fixed effects. A 90% confidence interval (CI) of the ratio of untransformed pharmacokinetic variables was derived by exponentiating the 90% CI for difference in the log scale.
If the within-subject variability for the reference product assessed during the study confirms that the reference is a highly variable product (i.e. intrasubject variability of its rate and/or extent of absorption is >30%), then the EMA guideline defines expanded acceptance criteria for Cmax based on the within-subject variability for the reference product assessed during the study. 18
In detail, if the within-subjectt CV of Cmax for the reference product was >30%, then bioequivalence between the test and reference formulations was declared only if the three following conditions were met: (1) the 90% for Cmax was within a widened acceptance range, exp (±0.76swr), where swr is the within-subject SD of the log-transformed values of Cmax of the reference product. The acceptance range could be widened to a maximum of 69.84–143.19%; (2) the geometric mean ratio for Cmax was within the range 80.00–125.00%; (3) the 90% CI for AUC0– t was within the range 80.00–125.00%.
Where the within-subject CV for Cmax of the reference product was ≤30%, then the conditions for determining bioequivalence between the test and reference formulations were the standard ones, i.e.: the 90% CIs for both AUC0– t and Cmax were within the range 80.00–125.00%.
Phoenix WinNonlin version 5.2 by (Pharsight, Mountain View, CA, USA) was used for pharmacokinetic parameter derivation. SAS® version 9.1 (SAS Institute, Cary, NC, USA) was used for other statistical analyses.
Results
Demographics of subjects in the safety population of a study comparing the bioavailability of a new oral syrup with an established oral liquid product, each containing 500 mg paracetamol, 10 mg phenylephrine hydrochloride and 200 mg guaifenesin per dose in adult healthy volunteers aged 18–45 years.

Data presented as mean ± SD or n (%). BMI, body mass index.
For the reference product, the control assay gave a value for phenylephrine hydrochloride content of 99.8%, whereas the assay result for the syrup was 100.5% for phenylephrine hydrochloride. A poststudy assay confirmed the level of phenylephrine hydrochloride in the syrup (98.6%) to be within specification (95.0–105.0%). The stability of the syrup formulation in the dosing device (syringe) was confirmed (99.2% of phenylephrine after 14 h in the syringe). No post-study assay content was performed for paracetamol or guaifenesin.
The untransformed mean plasma paracetamol concentrations over time by formulation in the pharmacokinetic population are shown in Figure 1a. Values for Cmax, AUC0–
t
and AUC0–∞ for paracetamol were slightly higher for the syrup formulation than for the reference product; however, the geometric mean ratios (syrup/reference product) of Cmax, AUC0–
t
and AUC0–∞ for paracetamol were ∼1. Paracetamol was absorbed rapidly, with median tmax occurring at 40 min for both the syrup and the reference product. The mean terminal t½ of paracetamol was similar for the two formulations (∼5 h).
Untransformed mean plasma drug concentrations in 42 healthy adult volunteers over 24 h in a study comparing the bioavailability of a new oral syrup with an established oral liquid product, each containing 500 mg paracetamol, 10 mg phenylephrine hydrochloride and 200 mg guaifenesin per dose: (a) paracetamol; (b) phenylephrine hydrochloride; (c) guaifenesin. For the reference product, two replicate concentrations for each subject were taken at each timepoint. The colour version of this figure is available at: http://imr.sagepub.com.
Summary of pharmacokinetic parameters for paracetamol, phenylephrine hydrochloride and guaifenesin in the pharmacokinetic population of adult healthy volunteers in a study comparing the bioavailability of a new oral syrup with an established oral liquid product, each containing 500 mg paracetamol, 10 mg phenylephrine hydrochloride and 200 mg guaifenesin per dose.

Within bioequivalence range.
CI, confidence interval; CV, coefficient of variation; see Table 1 for definitions of Cmax, AUC0– t and AUC0–∞.
The untransformed mean plasma phenylephrine hydrochloride concentrations over time by formulation in the pharmacokinetic population are shown in Figure 1b. Values for Cmax, AUC0– t and AUC0–∞ for phenylephrine hydrochloride were higher for the reference product than for the syrup formulation. The geometric mean ratios (syrup/reference product) of Cmax, AUC0– t and AUC0–∞ for phenylephrine hydrochloride approximated to 0.8. Phenylephrine hydrochloride was rapidly absorbed, with median tmax occurring at ∼0.5 h for both the syrup and the reference product. The mean terminal t½ of phenylephrine hydrochloride was longer for the reference product (∼4 h) compared with the syrup (∼3.7 h).
Table 3 shows the least-squares geometric means for phenylephrine hydrochloride calculated by back-transforming the least-squares means calculated from natural log-transformed Cmax, AUC0– t and AUC0–∞. The syrup/reference product ratios of these least-squares geometric means are also presented. The Cmax ratio was ∼77% and the associated 90% CI was 71.51–82.54%. The intraindividual CV for Cmax for the reference product was 16.9%; therefore the scaled approach described in the study protocol to expand the CI for Cmax was not used. Both the point estimate and the lower limit of the 90% CI for Cmax (76.82% and 71.51%, respectively) were outside the bounds required for the demonstration of bioequivalence (80.00–125.00%). The AUC0– t ratio was 80.37% and the associated 90% CI was 77.17–83.71%: the point estimate for AUC0– t was within the bounds, but the lower limit of the 90% CI was outside the bounds required for the demonstration of bioequivalence (80.00–125.00%). The AUC0–∞ results were very similar to the AUC0– t results.
The untransformed mean plasma guaifenesin concentrations over time by formulation in the pharmacokinetic population are shown in Figure 1c. The values for Cmax, AUC0– t and AUC0–∞ for guaifenesin were similar for the two formulations. The geometric mean ratios (syrup/reference product) of Cmax , AUC0– t and AUC0–∞ for guaifenesin were ∼1. Guaifenesin was rapidly absorbed, with median tmax occurring at ∼0.5 h for both the syrup and the reference product. The mean terminal t½ of guaifenesin was ∼0.8 h for both formulations.
Table 3 shows the least-squares geometric means for guaifenesin calculated by back-transforming the least-squares means calculated from natural log-transformed Cmax, AUC0– t and AUC0–∞. The syrup/reference product ratios of these least-squares geometric means are also presented. The Cmax ratio was 98% and the AUC0– t and AUC0–∞ ratios were both 96%. The 90% CIs for the three ratios were all within the standard bounds required for the demonstration of bioequivalence (80.00–125.00%). There was higher within-subject variability for Cmax compared with AUC0– t and AUC0–∞ as indicated by the CV. The within-subject CV for Cmax for guaifenesin with the reference product was 30.26%, resulting in a scaled CI of 79.86–125.23%. The effect of formulation sequence was tested in the ANOVA model using subject nested within sequence as the error term. No sequence effect was observed (P-values >0.15 for all pharmacokinetic parameters and all analyses).
Overall incidence of mild and moderate adverse events per system organ class in the safety population in a study comparing the bioavailability of a new oral syrup with an established oral liquid (reference) product.

Date presented as n (%).
Discussion
The results of the present study show that, whereas the 90% CIs for the geometric mean ratios for paracetamol and guaifenesin of both the reference product and the syrup were within the acceptance range (80–125%), the geometric mean ratios for phenylephrine hydrochloride were not within the acceptance range. Therefore, bioequivalence between the reference product and the syrup was not reached in this study.
It is only possible to speculate about the reasons for the slower absorption of phenylephrine hydrochloride with the syrup than with the reference product. One strong possibility is the difference in excipients – maltitol in the syrup and sorbitol in the reference product – which could affect the rate and extent of drug absorption.20,21 Oral bioavailability depends on factors such as intestinal transit, absorption from the lumen, first-pass metabolism in the small bowel (which is the primary absorption site for drugs) and subsequent first-pass hepatic extraction; it is well known that sorbitol (and other polyols) can accelerate intestinal transit or even cause diarrhoea, which leads to less contact time between the active moiety and the intestinal wall. 22 Also, the effect of sorbitol on the bioequivalence status may vary with drugs of low and high intestinal permeability:23–25 osmolytes such as sorbitol affect the absorption of low-permeability compounds, 23 which is partly attributable to the osmotic pressure of the osmolyte leading to an increased GI fluid volume, which subsequently decreases the concentration gradients of compounds in the GI tract. Another potential mechanism may be sorbitol’s enhancement of GI motility, which reduces the compound’s contact time with the small bowel. Analysis of the present study data provides evidence that phenylephrine hydrochloride is rapidly absorbed: the absorption profile of phenylephrine hydrochloride has a sharp peak, with median tmax of 0.5 h and median AUC0–2h being 70% of AUC0– t (i.e. 70% of phenylephrine hydrochloride absorption and elimination occurs within 2 h after dosing). There have also been reports of possible interactions of sorbitol with high-permeability drugs (including risperidone 26 and metoprolol 21 ), which suggest that other mechanisms exist by which osmolytes affect the absorption of high-permeability drugs. However, there are insufficient data available to explain this mechanism. It is also plausible that a substantial fraction of maltitol in the syrup remains intact during absorption of the active ingredients, as hydrolysis of maltitol into glucose and sorbitol is slow; 20 in other words, there is the possibility that most absorption of phenylephrine occurs before the hydrolysis of maltitol. The maltitol could create a change in osmotic conditions sufficiently large as to affect the absorption of certain high-permeability drugs such as phenylephrine hydrochloride, while not affecting absorption of paracetamol or guaifenesin.
The lack of bioequivalence for phenylephrine hydrochloride in this study could also be due to differences in the assay results, the effect of the dosing device, the nature of the study design or the power of the study. The observed lack of bioequivalence was not caused by a content assay difference between the two formulations. The stability of the two formulations in the dosing device (syringes) was confirmed. The study is a replicate design and assessed the phenylephrine hydrochloride Cmax intraindividual coefficient of variability as 16.9%, which is far from the criteria of highly variable drugs. The method for phenylephrine hydrochloride bioanalytical assessment (free phenylephrine hydrochloride) has been validated according to the current European Union requirements. 27 The power of the current study was >90% for all tested parameters and, thus, the study was adequately designed to test bioequivalence.
Therefore, the present study has investigated potential reasons for the differences in bioequivalence for paracetamol and guaifenesin and for phenylephrine hydrochloride, and has excluded any cause related to the experimental conditions. The differences between the two formulations in the excipients, sorbitol versus maltitol, may have played a role in the different bioavailability of phenylephrine hydrochloride observed between the syrup and the reference product.
The number of subjects experiencing AEs was 20.5% in the test syrup group and 20.9% in the reference group, but for the test syrup three-quarters of these (15.9%) experienced AEs that were mild in severity. Only two subjects (4.5%) experienced AEs of moderate severity in the test syrup group and none experienced a severe AE in any group.
Further research is needed to investigate the influence of maltitol and sorbitol on the absorption of phenylephrine. In particular, the speed of hydrolysis of maltitol into glucose and sorbitol needs to be investigated, in relation to the rate of absorption of phenylephrine, to confirm whether this was the factor leading to differences in bioequivalence between the test syrup and reference solution. A direct reaction between maltitol and phenylephrine is unlikely. However, the chemical structure of maltitol could also be investigated, in order to assess the possibility of a chemical interaction between maltitol and phenylephrine.The main failing of this study has been to assume that differences in excipients between the test and reference compounds would not unduly influence the outcomes.
In conclusion, in the present study, the novel syrup did not reach bioequivalence with the reference product, because bioequivalence could not be shown for phenylephrine hydrochloride. However, for paracetamol and guaifenesin, the 90% CIs of the least-squares geometric mean ratios for Cmax and AUC0– t were well within the predefined limits of 80–125%. For phenylephrine hydrochloride, the 90% CIs of the least-squares geometric mean ratios for Cmax and AUC0– t crossed the lower boundary, which may not be associated with differences in therapeutic effects. Single doses of both the syrup and reference product were well tolerated and were associated with a good safety profile.
Footnotes
Declaration of conflicting interest
The authors are employees of Novartis Consumer Health S.A., Nyon, Switzerland.
Funding
This study was funded by Novartis Consumer Health S.A., Nyon, Switzerland.
Acknowledgements
The authors would like to thank Marcia Hammond, a professional medical writer with DPP-Cordell, Norwich, United Kingdom, for editorial support during the final stages of manuscript preparation.