
Abstract
Objective
To investigate cardiac structural changes in elderly patients with obstructive sleep apnoea–hypopnoea syndrome (OSAHS) and the impact on left ventricular systolic and diastolic function.
Methods
The study enrolled elderly patients with OSAHS and age-matched healthy control subjects. Cardiac structure, left ventricular diastolic function and left ventricular systolic function were measured using a Doppler ultrasound scanner and compared between the two groups.
Results
The study included 136 patients with OSAHS and 50 healthy control subjects. There were significant differences in the echocardiography indicators that reflect cardiac structure, including interventricular septum, left ventricle posterior wall thickness, and left ventricular mass and mass index between the two groups. There were significant differences between the two groups in the ventricular septal early diastolic myocardial peak velocity/late diastolic myocardial peak velocity (Em/Am), mitral annulus Em/Am, and left ventricle posterior wall Em/Am. There were also significant differences in the indicators of interventricular septum, mitral annulus and left ventricular posterior wall systolic peak velocity between the two groups.
Conclusion
Elderly patients with OSAHS demonstrated cardiac structural changes and their left ventricular diastolic and systolic functions were significantly diminished.
Introduction
Obstructive sleep apnoea–hypopnoea syndrome (OSAHS) is a common but serious sleep respiratory disease that can impair the function of the cardiovascular system. For example, OSAHS affects cardiac function and output in many ways, and is associated with hypertension, 1 pulmonary hypertension, 2 vascular endothelial injury, tissue ischaemia, 3 systolic and diastolic dysfunction, and arrhythmias.4,5 OSAHS is closely related to the incidence and mortality of cardiovascular disease, especially in the elderly population.6,7 As the symptoms of OSAHS are not very specific and the development complications is usually occult and gradual, many patients do not get an accurate clinical assessment and guided treatment. Consequently, their primary diseases and complications are aggravated and, ultimately, change from functional disorders to organic diseases. 8 For that reason, the early detection, diagnosis, treatment and prevention of the complications associated with OSAHS are clinically important goals. 9 As a result of its rapid development, noninvasive approach, standardized procedure and repeatability features, echocardiography has been widely used in the clinical evaluation of cardiac structure and functional changes. It thus makes the early detection of OSAHS and the relevant cardiac diseases possible. 10
The purpose of this present study was to investigate cardiac structural changes in patients with OSAHS and to determine the impact that OSAHS has on left ventricular systolic and diastolic function.
Patients and methods
Participants
This prospective study enrolled consecutive patients with OSAHS who visited the Key Laboratory of Otorhinolaryngology of the Health Ministry, Department of Otorhinolaryngology, Qilu Hospital, Shandong University, Jinan, Shandong Province, China, between January 2006 and December 2012. Patients with OSAHS were diagnosed following a 32-lead twin polysomnography (PSG) assessment (Respironics, Murrysville, PA, USA). The apnoea–hypopnoea index (AHI) was defined as the total number of apnoea and hypopnoea episodes per hour of sleep. 11 AHI and lowest oxygen saturation were recorded during PSG monitoring as described below. OSAHS was defined as an AHI ≥5 obstructive events per hour of sleep. 12 Patients with OSAHS did not receive any specific treatment for OSAHS prior to inclusion in the study. Exclusion criteria included coronary heart disease, hypertension, obstructive pulmonary disease and type 2 diabetes mellitus.
The control group consisted of healthy subjects selected from patients who visited the Cardiovascular Colour Ultrasound Centre at Qilu Hospital for physical examination. The control subjects did not have OSAHS, as confirmed by PSG assessment. The control subjects also had no history of hypertension, snoring, sleep apnoea or daytime sleepiness. Relatives of the healthy control subjects also provided confirmation that the control subjects did not snore or have sleep apnoea. As for the patient group, control subjects with type 2 diabetes, coronary heart disease, hypertension or obstructive pulmonary disease were excluded. In addition to routine clinical and laboratory examinations, all study participants completed the Epworth Sleepiness Scale (ESS), which scores the likelihood of dozing in eight situations (0, no likelihood; 1, slight likelihood; 2, moderate likelihood; 3, high likelihood), giving a maximum score of 24. 13 The age, weight, height and body mass index (BMI) of all study participants were recorded.
The study was approved by the Ethics Committee of Qilu Hospital (No. 9205). Verbal informed consent was obtained from all study participants.
Polysomnography assessment of sleep apnoea
A 32-lead twin PSG monitor (Respironics) was used to measure various physiological functions during the stages of sleep in patients with OSAHS and the control subjects. Polysmith sleep analysis software version 10.0 (Neurotronics, Gainesville, FL, USA) was used to monitor 10 indicators, including electroencephalogram, submandibular electromyography, eye movement electronystagmogram, muzzle airflow, chest and abdominal movement, oxygen saturation, electrocardiogram, leg movements, body position and snoring. Sleep stages were scored in 30-s epochs using standard criteria. Apnoea was defined as the absence of airflow for ≥10 s. 14 Hypopnoea was defined as a significant reduction in airflow (>50%) for ≥10 s or a moderate reduction in airflow for ≥10 s together with an arousal or oxygen desaturation (≥4%). 15 The muzzle airflow was monitored by the triple thermometer; chest and abdominal movement was monitored by the thoracic/abdominal strain gauge; oxygen saturation was monitored by the pulse oximeter; and posture was monitored by a sleep position indicator sensor (Philips Healthcare, Best, the Netherlands).
Echocardiography
Echocardiography was conducted using GE Vivid 7 ultrasound diagnostic apparatus (GE Healthcare Biosciences, Piscataway, NJ, USA), which includes both a tissue Doppler imaging (TDI) system and traditional ultrasound functions, and can automatically record each set of test results. The participants were in the left lateral decubitus position when their cardiac structures were monitored using a 2.5–4.0 MHz probe and conventional transthoracic echocardiography (M-mode, two dimension, colour Doppler) as previously described. 16 The main indicators included left ventricular diastolic diameter (LV), left atrium diastolic diameter (LA), right ventricular diastolic diameter (RV), right atrium diastolic diameter, arteriae aorta diameter (AO), pulmonary artery diameter, interventricular septum (IVS), left ventricle posterior wall (LVPW) and body surface area (BSA). The Devereux formula was used to calculate the left ventricular mass (LVM) (g) = 0.8 × 1.04 [(IVS + LVPW + LV) 3 − LV3] + 0.6 and the left ventricular mass index (LVMI) = LVM/BSA, where BSA (m2) = 0.006 × height (cm) + 0.013 × body weight (kg) − 0.153. 17
In order to conduct the measurements effectively, the system was switched to the TDI speed mode, the filter was set to the minimum, and the Doppler gain was reduced appropriately. The sample volume was placed on the cross of the anterior mitral valve annulus to measure the mitral annulus; on the IVS muscular segment to measure IVS; and on the papillary muscle short axis to measure LVPW. The systolic myocardial peak velocity (Sm), early diastolic myocardial peak velocity (Em) and late diastolic myocardial peak velocity (Am) were measured separately. All of the images of mitral early diastolic velocity (E), mitral late diastolic in velocity (A), cardiac output (CO), left ventricular ejection fraction (EF), left ventricular shortening fraction (FS) and stroke volume (SV) were recorded and stored. Once recorded, off-line analyses were conducted to calculate the mean values for three continuous cardiac cycles.
Statistical analyses
All statistical analyses were performed using the SPSS® statistical package, version 11.0 (SPSS Inc., Chicago, IL, USA) for Windows®. Data are presented as mean ± SD. The mean values of the two groups were compared using Student's t-test. The correlations between BMI and the main echocardiography indicators were calculated using Spearman’s correlation coefficient because OSAHS is related to weight.18,19 A P-value <0.05 was considered statistically significant.
Results
A total of 136 patients with OSAHS were diagnosed following a PSG assessment (89 male and 47 female; mean age 63.3 ± 10.6 years; range 50–82 years). The control group (n = 50) included 37 men and 13 women with a mean age of 62.2 ± 10.8 years (range 50–76 years).
Comparison of the general, hemodynamic, biological, respiratory characteristics and cardiac structure echocardiography results for elderly patients with obstructive sleep apnoea–hypopnoea syndrome (OSAHS) and healthy elderly control subjects.

Data presented as mean ± SD.
The mean values of the two groups were compared using Student’s t-test.
Abbreviation: BMI, body mass index; DBP, diastolic blood pressure; LDL, low density lipoprotein; HDL, high density lipoprotein; HR, heart rate; PP, pulse pressure; RDI, respiratory disturbance index; SBP, systolic blood pressure; SD, standard deviation; LV, left ventricular diastolic diameter; LA, left atrium diastolic diameter; RV, right ventricular diastolic diameter; RA, right atrium diastolic diameter; AO, arteriae aorta diameter; PA, pulmonary artery diameter; IVS, interventricular septum; LVPW, left ventricle posterior wall; LVM, left ventricular mass; LVMI, left ventricular mass index; NS, no significant between-group difference (P ≥ 0.05).
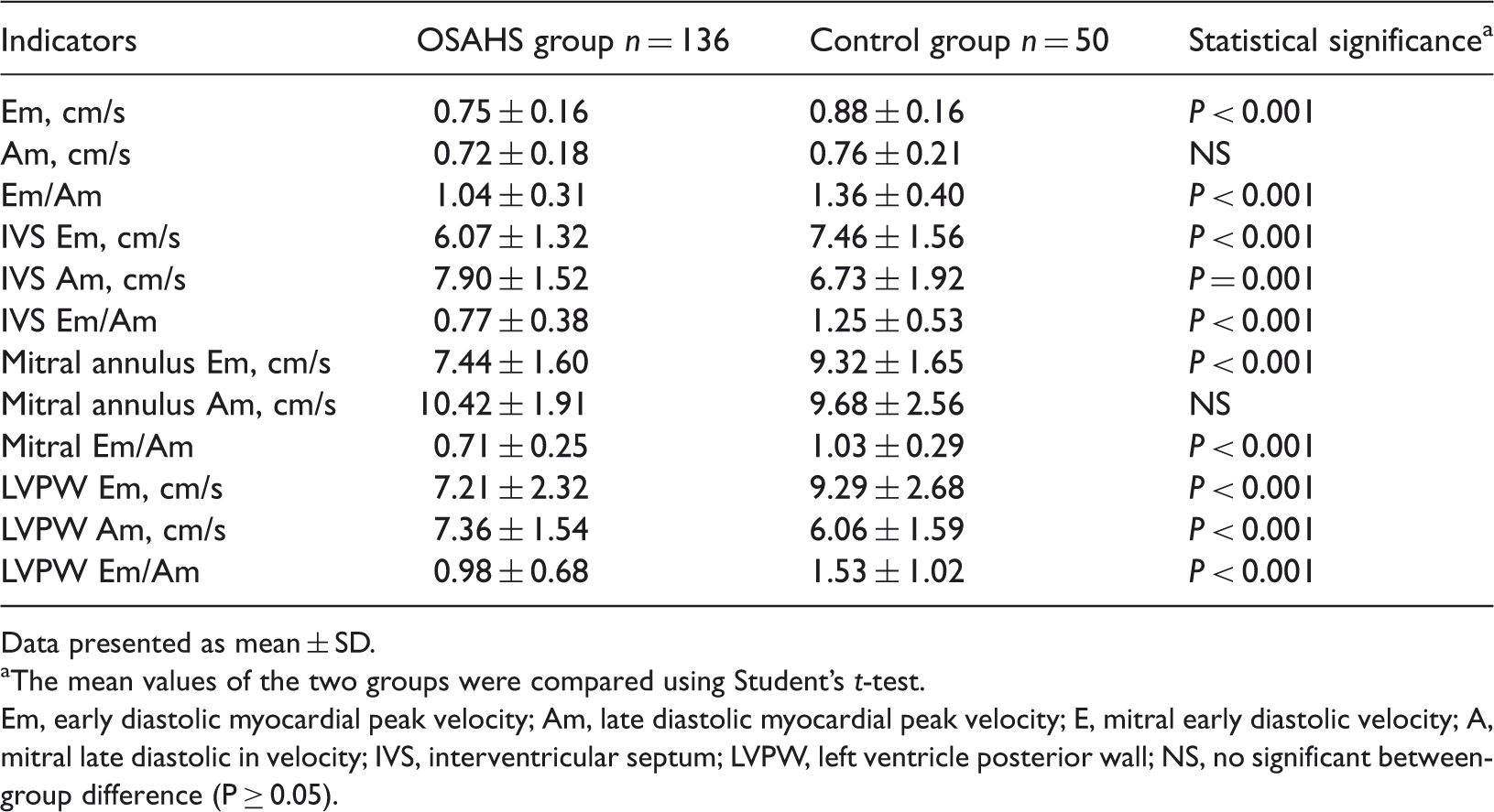
Comparison of left ventricular diastolic function indicators for patients with obstructive sleep apnoea–hypopnoea syndrome (OSAHS) and healthy elderly control subjects.
Data presented as mean ± SD.
The mean values of the two groups were compared using Student’s t-test.
Em, early diastolic myocardial peak velocity; Am, late diastolic myocardial peak velocity; E, mitral early diastolic velocity; A, mitral late diastolic in velocity; IVS, interventricular septum; LVPW, left ventricle posterior wall; NS, no significant between-group difference (P ≥ 0.05).
Comparison of left ventricular systolic function indicators for patients with obstructive sleep apnoea–hypopnoea syndrome (OSAHS) and healthy elderly control subjects.

Data presented as mean ± SD.
aThe mean values of the two groups were compared using Student’s t-test.
CO, cardiac output; SV, stroke volume; EF, left ventricular ejection fraction; FS, left ventricular shortening fraction; IVS, interventricular septum; Sm, systolic myocardial peak velocity; LVPW, left ventricle posterior wall; NS, no significant between-group difference (P ≥ 0.05).
There was no significant difference in the BMI between the OSAHS and control groups. In terms of the cardiac structure, the BMI of patients with OSAHS was significantly related to the LV (r = 0.40, P = 0.028), AO (r = 0.39, P = 0.026), LVM (r = 0.47, P = 0.031) and LVMI (r = − 0.25, P = 0.023). The BMI of the control subjects was significantly related only to RV (r = 0.51, P = 0.039) and IVS (r = 0.47, P = 0.041). In terms of the left ventricular diastolic and systolic function, the BMI of patients with OSAHS was significantly related to Em (r = 0.42, P = 0.033), Em/Am (r = 0.37, P = 0.026), mitral annulus Am (r = 0.53, P = 0.042), mitral annulus Em/Am (r = 0.29, P = 0.016), LVPW Em (r = 0.27, P = 0.023), LVPW Am (r = 0.32, P = 0.027) and LVPW Em/Am (r = −0.29, P = 0.018). The BMI of control subjects was significantly related to the mitral annulus Em (r = 0.38, P = 0.042) and LVPW Am (r = 0.52, P = 0.037).
Conversely, the AHI of patients with OSAHS was significantly related to LV (r = 0.37, P = 0.021), LA (r = 0.43, P = 0.041), RA (r = 0.53, P = 0.049), LVM (r = 0.31, P = 0.042) and LVMI (r = −0.25, P = 0.023). The AHI of the control subjects was not significantly related to these variables. In terms of the left ventricular diastolic and systolic function, the AHI of patients with OSAHS was significantly related to Em (r = 0.56, P = 0.025), Em/Am (r = 0.41, P = 0.032), IVS Em (r = 0.61, P = 0.047), IVS Em/Am (r = 0.51, P = 0.029), mitral annulus Em/Am (r = 0.24, P = 0.019), LVPW Em (r = 0.31, P = 0.029), LVPW Am (r = 0.45, P = 0.033) and LVPW Em/Am (r = −0.26, P = 0.037). The AHI of control subjects was not significantly related to left ventricular diastolic and systolic function.
Discussion
Three physiological mechanisms associated with OSAHS are generally considered to cause left ventricular hypertrophy: (i) the increased haemodynamic load that results from the increased blood pressure that is often observed in patients with OSAHS, which rises continually and does not drop down at night, causing the left ventricle to suffer long-term pressure overload;20,21 (ii) the activation of the sympathetic nervous system and the renin–angiotensin–aldosterone system (RAAS). Patients with OSAHS have an active sympathetic nervous system and RAAS, and increased levels of catecholamines, renin, angiotensin II and aldosterone. By binding with the corresponding receptor, these hormones promote cell growth and protein synthesis, increase collagen synthesis of cardiac fibroblasts, and reduce the degradation of collagen;22,23 (iii) elevated levels of endothelin and reduced levels of nitric oxide, which are observed in patients with OSAHS. 24 Endothelin is involved in cardiac hypertrophy through several mechanisms of action. First, endothelin has powerful vasoconstrictor effects. 24 Endothelin induces the proliferation and hypertrophy of vascular smooth muscle cells, narrows the vascular lumen, thickens the vascular wall and increases peripheral resistance, which results in an increase in the cardiac afterload. 24 Secondly, endothelin increases mitosis in cardiomyocytes and fibroblasts, thus causing cell proliferation, intracellular calcium overload and proto-oncogene expression, which promotes DNA and protein synthesis, and in turn eventually increases cardiac hypertrophy. 24 Thirdly, endothelin and angiotensin II promote the expression of each other’s encoding gene in a positive feedback manner.25,26 This present study found significant differences in IVS, LVPW, LVM and LVMI between the OSAHS group and the control group.
When a patient with OSAHS is in apnoea, the formation of an extreme intrathoracic negative pressure causes rapid changes in the ventricular transmural pressure, which results in an increased myocardial wall pressure and afterload. 27 In addition, the apnoea causes hypoxaemia and hypercapnia, which lead to pulmonary vasoconstriction, pulmonary pressure and increased right ventricular afterload. 27 When coupled with the increased intrathoracic pressure and returned blood volume, the right ventricular volume is overloaded and becomes an easy trigger for right heart failure.28,29 Moreover, as a result of the ventricular interdependence mechanism, the IVS shifts to the left, which reduces the compliance, capacity and pump output of the left ventricle. 30 As a result of the endothelium-dependent diastolic dysfunction, large amounts of endothelin and catecholamine are generated, and this results in increased blood pressure during sleep and daytime hypertension. 31 This increase in blood pressure increases cardiac load and LVMI, and causes ventricular hypertrophy, cardiac remodelling and structural abnormalities. 32 All of these physiological changes inevitably lead to myocardial systolic and diastolic dysfunction.33,34
Tissue Doppler imaging technology has been used to examine right ventricular function in patients with OSAHS, and it was found that patients with OSAHS had different degrees of right ventricular dysfunction regardless of whether they had concomitant hypertension or not.35,36 The TDI myocardial performance indicator is one of the most important indicators that reflect the relationship between the degree of OSAHS and right ventricular subclinical dysfunction.35,36 The study conducted by Ferrier et al. 37 in patients with OSAHS and left ventricular dysfunction showed that, after treatment, the LVEF returned to a normal value, suggesting that OSAHS may cause left ventricular systolic dysfunction during the daytime. Therefore, improving sleep apnoea can improve left ventricular systolic function. The present study also found that elderly patients with OSAHS showed significant left ventricular diastolic dysfunction. The mitral inflow Em/Am was significantly different between the OSAHS group and the control group; so were the mitral annulus Em, mitral annulus Em/Am, LVPW Em, LVPW Am, LVPW Em/Am, IVS Em, IVS Am and IVS Em/Am. These findings suggested that OSAHS might cause haemodynamic changes, increase afterload and thicken the LVPW.
This present study found that there were no significant differences between the two indicators of left ventricular systolic function, CO and SV in OSAHS group and the control group. However, there were statistically significant differences for the indicators FS and EF had between the two groups, as well as for IVS Sm, mitral annulus Sm and LVPW Sm. These findings indicated that the myocardial systolic function of the patients with OSAHS was significantly impaired. This finding was consistent with that of a previous study that used multigated radionuclide ventriculography to measure EF. 38
Obesity has been linked to specific cardiovascular outcomes such as hypertension, stroke, myocardial ischaemia and arrhythmias, and it is also related to OSAHS. 39 The relationship between obesity, OSAHS and heart disease has become an important area of research. Animal research suggests that forced inspiration-induced acute LA distension related to diastolic dysfunction may be an important component of the arrhythmogenic substrate for atrial fibrillation during sleep apnoea episodes in obese patients. 40 In the diseased cardiac patient, the severity of obstructive sleep apnoea was associated with an increased risk of death and risk stratification based on obstructive sleep apnoea severity was shown to be relevant. 41 In this present study, obesity, as determined by the BMI, in patients with OSAHS was associated with more damage to the cardiac structure and left ventricular diastolic and systolic dysfunction than was observed in the control patients with similar levels of obesity.
There are some limitations to this study. Because of insufficient follow-up time, we were not able to observe the effects of long-term continuous positive airway pressure therapy or surgical treatment on cardiac structure and function in patients with OSAHS. Future studies should focus on this.
In conclusion, this present study demonstrated that the cardiac structure was altered in elderly patients with OSAHS, which was characterized by concentric hypertrophy, while their left ventricular diastolic and systolic functions were significantly diminished compared with control subjects. Obesity appeared to participate in the damage to the cardiac structure and left ventricular diastolic and systolic dysfunction in patients with OSAHS. Echocardiography, especially TDI technology, might make the early diagnosis of OSAHS in elderly patients possible, which should help in the prevention of future pathological changes to the heart.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This study was supported by a grant from the National Natural Science Foundation of China (No. 81102019) and by grants from the Natural Science Foundation of Shandong Province, China (No. 2011GGE27059; No. 2012BSE27043; No. ZR2012HM033).