
Abstract
Objective
To investigate the diagnostic value of Delta-like 1 ligand (DLL1) in cerebrospinal fluid (CSF) and serum, in tuberculous meningitis (TBM).
Methods
Patients with a definite diagnosis of central nervous system infection (TBM, viral meningitis/encephalitis or bacterial meningitis) were prospectively enrolled alongside patients with intracranial metastatic tumour and patients with no diagnosis (who served as controls). DLL1 content in CSF and serum was measured quantitatively by enzyme-linked immunosorbent assay; analyses were blinded.
Results
A total of 173 patients were enrolled: 62 with TBM; 38 with viral meningitis/encephalitis; 26 with bacterial meningitis; 17 with intracranial metastatic tumour; 30 with no diagnosis. CSF DLL1 content was highest for TBM; there were no differences in CSF DLL1 between the other groups. Serum DLL1 content was highest for the TBM and intracranial metastatic tumour groups, with significant differences between the TBM group and the viral meningitis/encephalitis, bacterial meningitis and nondiagnosed groups. There were no differences in serum DLL1 between the viral meningitis/encephalitis, bacterial meningitis and nondiagnosed groups, or between the TBM group and the tumour group.
Conclusion
As a new biomarker, DLL1 may be of great clinical importance in the diagnosis of TBM.
Introduction
Tuberculosis is a devastating disease that causes over two million deaths every year.1,2 Tuberculous meningitis (TBM) is its most severe manifestation and carries serious, long-term consequences. 3 The case fatality rate for untreated TBM is almost 100% and delay in treatment often leads to permanent neurological damage. 4 Therefore, prompt diagnosis and early treatment are crucial for successful TBM management.5–8 However, due to the complex manifestations of TBM and the considerably high use of antibiotics in its management, many cases of TBM are atypical. In such cases, laboratory results can be negative: the cerebrospinal fluid (CSF) cytology of infection of the central nervous system (CNS) is often nonspecific9,10 and pathology is rarely detected. Thus, there are difficulties with diagnosis and high rates of misdiagnosis when using traditional CSF and serological tests in patients with suspected TBM.10,11 A faster, more sensitive and more specific test for the diagnosis of TBM is urgently needed in clinical practice, and developing improved diagnostic techniques has become a clinical research priority.12–15
Mycobacterium tuberculosis is the causative agent of tuberculosis in humans. The M. tuberculosis cell wall is constructed primarily of peptidoglycan, which is bound to arabinogalactan and mycolic acid in a covalent fashion. Research findings have indicated that mycolic acid and fatty acid metabolism are closely related to M. tuberculosis survival, virulence and avoidance of attacks by the immune system.16–20 These factors demonstrate the importance of M. tuberculosis to host-fat metabolism.20–23
Delta-like 1 ligand (DLL1) is an L-type transmembrane protein consisting of 723 amino acids. It is a member of the Notch ligand family, which is a group of transmembrane receptors that is involved in the development of many organs and cellular differentiation. Of particular interest to this work, the Notch1 signal influences the formation of fat cells by regulating the activation of fatty acids and, thus, plays a crucial role in fat metabolism.24,25 In M. tuberculosis infection, there is an accelerated exfoliation of the DLL1 ligand, which helps the Notch1 signal promote the differentiation of fat cells.
Thus, because DLL1 participates in fat metabolism,26,27 it could be used as an indicator of M. tuberculosis infection. To explore DLL1 as a potential new tool for the diagnosis of TBM, the present study adopted an enzyme-linked immunosorbent assay (ELISA) for the quantitative measurement of DLL1 in CSF and serum samples from different patient groups: those with infection of the CNS, those with intracranial metastatic tumour and those with no diagnosis. The present study aimed to estimate the diagnostic accuracy of DLL1 as an indicator of M. tuberculosis infection, and the processes followed adhered to the reporting requirements of the Standards for Reporting of Diagnostic Accuracy initiative. 28
Patients and methods
Patients
This study sequentially and prospectively enrolled patients who were admitted to the neurology or paediatrics departments at the First Affiliated Hospital of Zhengzhou University, Zhengzhou, China between October 2008 and February 2012. Patients with CNS infection were diagnosed according to clinical manifestation, laboratory examination, CSF examination and imaging findings,29–32 and were categorized according to diagnosis: TBM; viral meningitis/encephalitis; bacterial meningitis. As control groups, patients with intracranial metastatic tumour with lung cancer and those with no CNS infection, tumour or immunological or haematopoietic system diseases, who consequently required differential diagnosis, were enrolled. The study protocol was approved by the Ethics Committee of Zhengzhou University. Written informed consent was obtained from the patients or their families.
CSF and serum collection
Cerebrospinal fluid (2 ml) was collected through lumbar puncture. During the same consultation, peripheral venous blood (2 ml) was taken, stored in an anticoagulant-free vacuum blood collection tube at room temperature for 30 min and centrifuged at 2000
DLL1 quantification
Delta-like ligand 1 in CSF and serum was quantified by ELISA (Korea Adipo Gen Company, Incheon, Republic of Korea), according to the manufacturer’s instructions. The calibration used DLL1 concentrations in the range of 0.125–8 ng/ml.
Standard CSF investigations
Standard CSF investigations, such as biochemistry and cytology, were performed as described elsewhere. 33
Statistical analyses
All data were analysed using SPSS® version 13.0 (SPSS Inc., Chicago, IL, USA). Quantitative data were expressed as mean ± SD. Multiple-group comparisons were tested by analysis of variance with a post-hoc Student–Newman–Keuls test. Pearson’s correlation coefficient analysis was conducted. The cut-off value was tested by receiver operating characteristic (ROC) analysis. Statistical significance was set at P ≤ 0.05.
Results
This study enrolled 173 patients, aged between 2 and 74 years. There were 62 patients with TBM (23 male and 39 female aged 7–56 years, 22.1 ± 14.8 years), 38 patients with viral meningitis/encephalitis (16 male and 22 female aged 6–60 years, 17.9 ± 12.9 years), 26 patients with bacterial meningitis (15 male and 11 female aged 2–37 years, 14.9 ± 8.4 years), 17 patients with intracranial metastatic tumour (10 male and seven female aged 40–74 years, 57.4 ± 9.7 years) and 30 patients with no diagnosis (15 male and 15 female aged 4–52 years, 20.6 ± 14.8 years).
Comparison of Delta-like ligand 1 (DLL1) levels in the cerebrospinal fluid of patients with infections of the central nervous system, intracranial metastatic tumour or no diagnosis.

P-values are for the comparisons of mean DLL1 levels in the tuberculous meningitis group with the other individual groups (analysis of variance).
Between-group analysis: F = 46.39; df = 4; P ≤ 0.001 (analysis of variance).
Comparison of Delta-like ligand 1 (DLL1) levels in the serum of patients with infections of the central nervous system, intracranial metastatic tumour or no diagnosis.

P-values are for the comparisons of mean DLL1 levels in the tuberculous meningitis group with the other individual groups (analysis of variance).
Between-group analysis: F = 41.82; df = 4; P ≤ 0.001 (analysis of variance).
NS, not statistically significant.
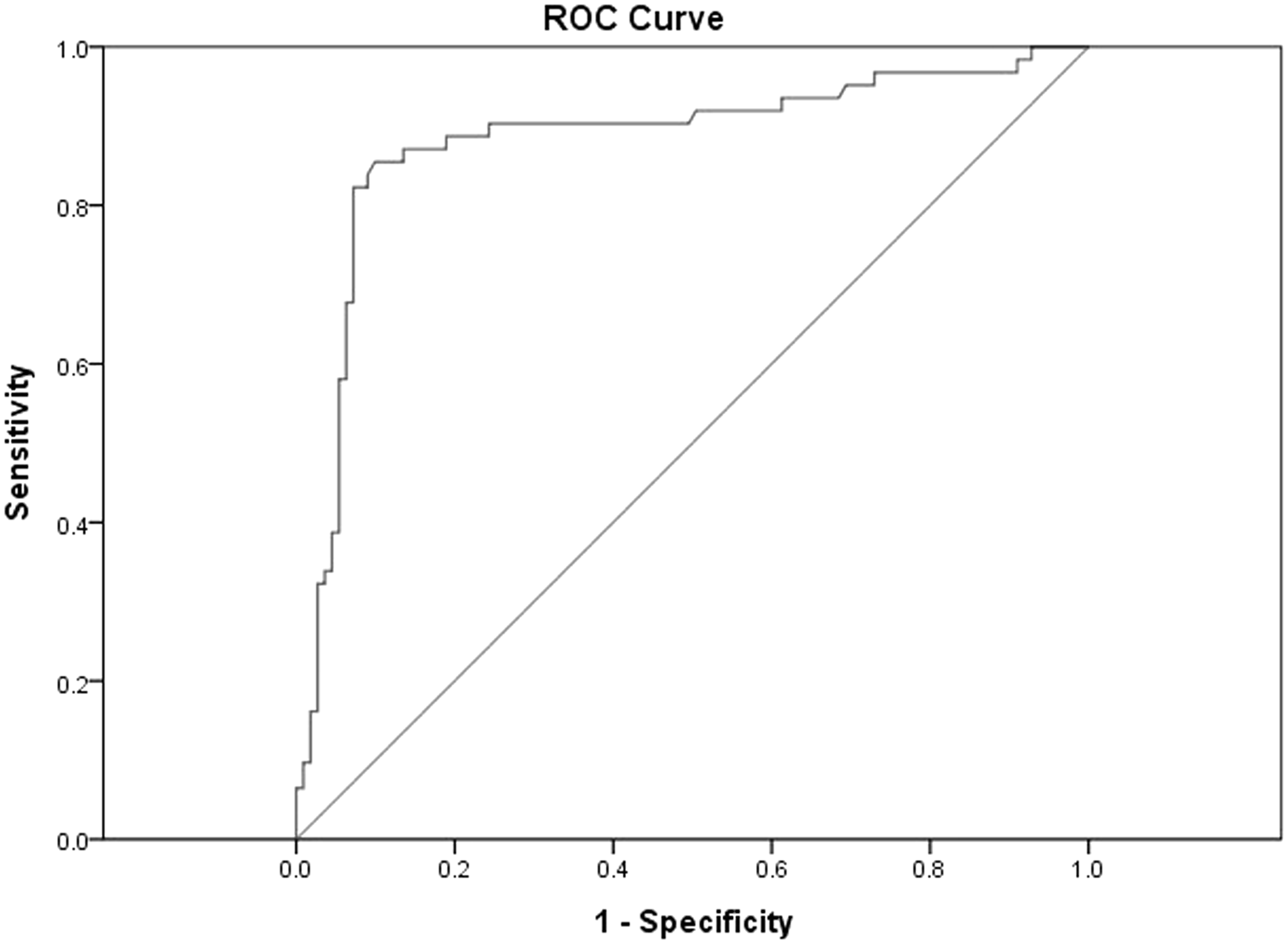
We performed a receiver operating characteristic curve analysis and determined that a cut-off of 1.0 ng/ml for CSF DLL1 could be used to distinguish TBM patients from viral meningitis/encephalitis, bacterial meningitis and nondiagnosed patients (Figure 1), with 69% of all CSF DLL1 levels > 1.0 ng/ml. For serum DLL1, this analysis determined that a cut-off of > 6.0 ng/ml could be used to distinguish TBM patients from viral meningitis/encephalitis and bacterial meningitis, with 71% of all serum DLL1 levels > 6.0 ng/ml (Figure 2).
Receiver operating characteristic (ROC) curve analysis of Delta-like ligand 1 (DLL1) levels in the cerebrospinal fluid of patients with infections of the central nervous system. Area under the curve, 0.976. Receiver operating characteristic curve analysis of Delta-like ligand 1 (DLL1) levels in the serum of patients with infections of the central nervous system. Area under the curve, 0.882.
The CSF DLL1 content and the serum DLL1 content were positively correlated with each other (r = 0.393, P ≤ 0.01). The CSF DLL1 content was not correlated with cell density, levels of CSF protein, glucose or chloride, or CSF pressure (r ≈ 0; data not shown).
Discussion
Delta-like 1 ligand is the human autoploid of Delta, the Notch ligand in Drosophila, and is an L-type transmembrane protein consisting of 723 amino acids. 34 As a Notch ligand, it is formed by one short C-terminal region in cytoplasm and a C-Delta/Serrate/LAG-2 region, following a series of eight repeated sequences of epidermal growth factor. 35 The gene has been cloned using polymerase chain reaction amplification with a pair of primers based on a sequence of the Delta gene. 27 The Notch family is a group of transmembrane receptors that function in the development of multiple organs and cells, and determine the direction of cellular differentiation. 36 Specifically, inhibition, gene mutation or abnormal activation of the Notch signalling pathway may correlate with the development of CNS diseases such as Alzheimer’s disease, Parkinson’s disease, stroke, brain tumour and cerebral ischaemia–reperfusion injury.24,37 Moreover, the Notch1 signal influences the formation of fat cells by regulating the activation of fatty acids, and plays a crucial role in fat metabolism.24,25 In the context of tuberculosis, which is a chronic wasting disease that leads to disordered fatty acid metabolism and excessive activation of fat cells, accelerated exfoliation of DLL1 as the Notch ligand helps the Notch signal to promote fat-cell differentiation. 25 Consequently, the present study adopted an ELISA method for the quantitative measurement of DLL1 content in CSF and serum from patients with CNS infectious diseases, to explore whether DLL1 represented a potential new tool for the diagnosis of TBM.
Results of the present study indicate that, in the TBM group, DLL1 levels in CSF were significantly higher than in other groups: 54/62 patients (87%) in the TBM group displayed levels > 1.0 ng/ml, while no individual exhibited levels > 1.0 ng/ml in the viral meningitis/encephalitis, purulent meningitis or control groups. DLL1 levels in CSF had no correlation with cell density, levels of CSF protein, glucose or chloride, or CSF pressure; consequently, we believe that the DLL1 content of CSF has potential value for the diagnosis of atypical cases of TBM. In the present study, in the TBM group, the serum DLL1 level was also markedly higher than the level observed in other CNS infections. DLL1 measurement in serum was conducted in 62 TBM patients, among whom 51 cases (82%) exhibited levels >6.0 ng/ml, while one case from the viral meningitis/encephalitis group, one case from the purulent meningitis group and no case from the nondiagnosed group displayed DLL1 levels in serum >6.0 ng/ml. We therefore propose that a cut-off value for DLL1 of 6.0 ng/ml in serum could be used in the diagnostic confirmation of TBM (Figure 2).
The present study findings showed that DLL1 levels in both CSF and serum increased significantly in TBM, and that the DLL1 content in CSF correlated positively with the DLL1 content in serum. DLL1 levels did not correlate with cell density or levels of protein, glucose, chloride or CSF pressure. Again, this indicates that DLL1 could be valuable for the differential diagnosis of atypical cases of TBM. Moreover, this diagnostic tool could also differentiate between TBM and viral meningitis/encephalitis or bacterial meningitis. Although patients with intracranial metastatic tumours had higher serum DLL1 levels than those with viral meningitis/encephalitis or bacterial meningitis (indeed, serum DLL1 levels did not differ significantly between cases of TBM and patients with intracranial metastatic tumours), the mean DLL1 level in the tumour group was lower than that in the TBM group, but this difference was not found to be statistically significant. The authors do not consider there would be clinical confusion between the diagnosis of TBM and intracranial metastatic tumours, given that these tumours are diagnosed most effectively using cytology, CT and MRI. 38 However, establishing the DLL1 level would be useful in situations when a differential diagnosis is needed.
In nondiagnosed patients in the present study, DLL1 concentrations were very low. Given that these patients by definition had not been diagnosed with TBM, it is reassuring that their DLL1 levels also did not suggest the presence of TBM.
The present study indicates that DLL1 levels in CSF and serum increase significantly in the context of TBM, and that the DLL1 content of CSF is positively correlated with the DLL1 content of serum. However, the mechanism by which DLL1 is increased is unclear. Although excessive exfoliation of DLL1 may help the Notch signal to promote the differentiation of fat cells, it may involve either or both of the following mechanisms. First, the Notch signal pathway is highly important for T-cell differentiation.39–42 In the event of a deficiency in the Notch receptor, lymphocytes would develop as B cells rather than T cells, 43 and activation of the Notch signal pathway could lead to the development of a T-cell lineage rather than a B-cell lineage: DLL1 exfoliation mediated by ADAM (a disintegrin and metalloprotease) seems to contribute to the downregulation of Notch signalling in adjacent cells, which limits the production of T cells. 44 Secondly, DLL1 is located in the adherens junctions in neurocyte processes, where it functions as a scaffolding protein. When adherens junctions are damaged by TBM, DLL1 can be released, which increases DLL1 content. 45
The strengths of the present study are that the analyses of CSF and serum samples were blinded to the diagnosis of the patient and that it enrolled a total of 173 patients who belonged to different diagnostic groups. A limitation is the narrow range of the DLL1 calibration standard (0.125–8 ng/ml). Also, this study did not investigate further the non-TBM patients with CSF DLL1 > 1 ng/ml or serum DLL1 > 6 ng/ml, to explain why they had high DLL1 concentrations. These limitations should be considered in future investigations.
In conclusion, the present study showed that DLL1 levels in CSF and serum appear to be high in patients with TBM, and are very low or undetectable in those with viral meningitis/encephalitis or bacterial meningitis. In patients with intracranial metastatic tumours, the DLL1 content in serum increases, whereas DLL1 levels in the CSF remain relatively low. Elevated concentrations of DLL1 in serum and the CSF may indicate TBM. The measurement of DLL1 in CSF and serum represents a potential tool for TBM diagnosis.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.