
Abstract
Objective
Frame-based stereotactic surgical planning systems (SSPSs) have been used for deep brain stimulation and radioneurosurgery. Here, we evaluated the feasibility, safety and efficacy of using a SSPS to aid spontaneous intracerebral haematoma (ICH) treatment.
Methods
Patients with moderate spontaneous putamen haematomas were randomized into two groups: treatment (group A) and control (group B). In group B, the catheter for evacuating haematomas was inserted into a target point, located at the centre of the haematoma, using conventional frame-based stereotactics; urokinase thrombolysis was subsequently delivered through the catheter. In group A, this procedure was assisted by a SSPS, which designed both the target point and trajectory in the haematoma through virtual reality. Duration of evacuating haematomas and number of urokinase injections was compared between groups.
Results
In total, 65 patients were recruited: in group A (n = 30), the duration of evacuating haematomas (35.27 ± 9.17 h) was shorter than in group B (n = 35; 67.77 ± 13.82 h). There were fewer urokinase injections in group A (3.63 ± 1.16) than in group B (6.40 ± 1.29).
Conclusions
The feasibility, efficacy and safety of spontaneous ICH treatment were optimized by the use of a frame-based SSPS.
Keywords
Introduction
Typically, the burdens of intracerebral haematoma (ICH) result from a mass effect, after haemorrhage or as a result of noninflammatory/chemical toxins in the blood and their degradation products. These two elements can play roles either together or separately in secondary impairments such as brain edema, hyperintracranial pressure, neurocyte injury, and decreased perfusion in the local brain and affected hemisphere.1–7 Consequently, ICH removal is beneficial because it reduces not only the mechanical injury but also the level of chemical damage within the brain.8–10
Compared with conservative treatment (in which the haematoma disappears naturally over time 8 and craniotomy (which aggravates the brain injury by incising normal craniocerebral structures), 11 stereotactic surgery combined with thrombolysis has the advantage of evacuating the clot efficiently and with minimal invasion.8,12 In conventional stereotactic ICH removal, the target point is generally limited to the central part of the haematoma with the largest cross-sectional area. A lytic agent is injected into the tip of a catheter inserted at the target point, and the liquid haematoma is drained using the catheter. The limited target point associated with this approach results in a slow rate of clot evacuation. By means of conventional stereotactic puncture and thrombolysis, Montes et al. 13 reported the rate of intracerebral haematoma evacuation was 57% within 3 days and Kim et al. 14 presented the mean period of evacuation at 5.1 days (range 1 – 12 days).
To enhance the efficacy of stereotactic ICH removal, we surveyed literature from neurosurgeons who have performed this procedure. Marquardt et al. 15 reported haematoma removal using multiple target points in a single operation, in which he found that 88.8% of the haematoma could be removed in one procedure, but only in 53.4% of all cases could >90% of the clot be evacuated. Hwang et al. 16 used stereotactic multiplanar reformatted computed tomography (CT)-guided catheter placement for ICH removal, and the median dwelling time of the catheter in the brain was 48.9 h (range 34–62 h) . Both of these modifications increased the speed of clot reduction. Barrett et al. 9 evacuated spontaneous ICHs using frameless stereotactic aspiration and thrombolysis. The above procedures were considered feasible; however, these studies did not have a randomized controlled design.
Currently, frame-based stereotactic surgical planning systems (SSPSs) are only used for deep brain stimulation and radioneurosurgery. 17 In the present study, we performed a randomized controlled clinical trial that used a frame-based SSPS for ICH removal.
Patients and methods
Patients
A randomized control study involving patients with spontaneous ICH was performed between May 2010 and January 2012. During this period, all hospital in-patients who were diagnosed with ICH according to American Heart Association/American Stroke Association (AHA/ASA) criteria 18 were prepared for the study in a dedicated unit. All ICH patients were diagnosed by CT: based on CT imaging, haematoma volume was calculated using the following formula: [A (cm) × B (cm) × C (cm)]/2, where A and B were the length and the width, respectively, of the largest cross-sectional area and C represented the total height from the bottom to the top slice of the haematoma. 19
This study was carried out with the approval of the Medical Ethics Committee at Qilu Hospital, Shandong University, Jinan, Shandong Province, China.
Inclusion and exclusion criteria
Inclusion criteria for patients were: (i) aged 35–80 years; (ii) spontaneous ICH located only in the putamen; (iii) haematoma volume 15–60 ml; (iv) steady Glasgow Coma Scale (GCS) score between 9 and 13 within 24 h of haemorrhage onset; (v) neurological function deficiency presenting as paralysis and/or aphasia; (vi) written informed consent from the participants themselves or their legal representatives.
Exclusion criteria for patients were: (i) ICH resulting from/combined with aneurysm, vascular malformation, brain trauma or intracranial tumour; (ii) bleeding disorders or currently on anticoagulant treatment; (iii) ICH accompanied by serious dysfunction or failure of any other organs.
Patients were randomized into two groups decided by coin toss: treatment (group A) or control (group B).
Treatment protocol
All operations were conducted between 24 and 48 h from the ictus.
In group A, CT scans (64-slice, 2.5 mm-thickness) were performed on patients installed with a stereotactic frame. The primary CT image data were subsequently formatted into Digital Imaging and Communications in Medicine (DICOM) and inputted into a dedicated frame-based SSPS (Brainlab iPlan, version 2.6, Brainlab (Beijing) Medical Equipments Trading, Beijing, China). With the help of this system, the entry and target point (i.e. the trajectory of the puncture of the haematoma) of the catheter were designed, and a puncture with a silicone catheter was performed in line with the designed trajectory. The distance of trajectory through the haematoma (measured by SSPS in advance) determined the length of catheter implanted into the clot. Side holes in this catheter were cut by surgical scissors every 5 mm from the tip; these holes were 1–2 mm in diameter. Thrombolysis and drainage of the haematoma through the catheter was then conducted by Z.D. or S.Z., as follows: the catheter was inserted into the brain along the trajectory and the lytic agent urokinase (20000 IU/2 ml 0.9% saline) was injected into the haematoma immediately after the operation, then the same dose of urokinase was injected every 12 h until the target haematoma volume was reached. The liquefied haematoma then flowed into the catheter via the side holes. Postoperative brain CT scans were performed just before every urokinase injection. The first postoperative CT scan was performed in order to validate the location of the catheter; subsequent CT scans assessed the residual clot. The catheter was removed when the residual clot was less than either 5 ml or 10% of initial volume.
In group B, except for the use of the stereotactic surgical planning system, the procedure was the same as that used for group A. The entry point was determined by neurosurgical experience and the target point was routinely set at the centre of the haematoma, where the cross-sectional area was at its largest.
Figure 1A–C show the overall flow of treatment for spontaneous ICH aided by frame-based SSPS in a typical case.
A 62-year-old female with a 42.3-ml putamen haematoma was treated by stereotactic surgical planning system (SSPS)-aided surgery. (A) The target point, entry point and trajectory were secured, and the length of catheter needed was measured by frame-based SSPS. Any point along the trajectory could be revealed in reconstructed axial, sagittal and coronal plane; (B) Image from the same patient, reconstructed by SSPS just before the first injection of urokinase (20 000 IU/2 ml 0.9% saline). The catheter path through the main intracerebral haematoma (ICH) axis determined by SSPS was validated postoperatively. White arrows point to the side holes of the catheter. Because of different side hole orientations, some holes are not displayed in this picture. Side holes were cut every 5 mm along the catheter length; (C) Reconstructed images (by SSPS) from the same patient, just before removing the catheter. Successful ICH evacuation was observed after five urokinase injections.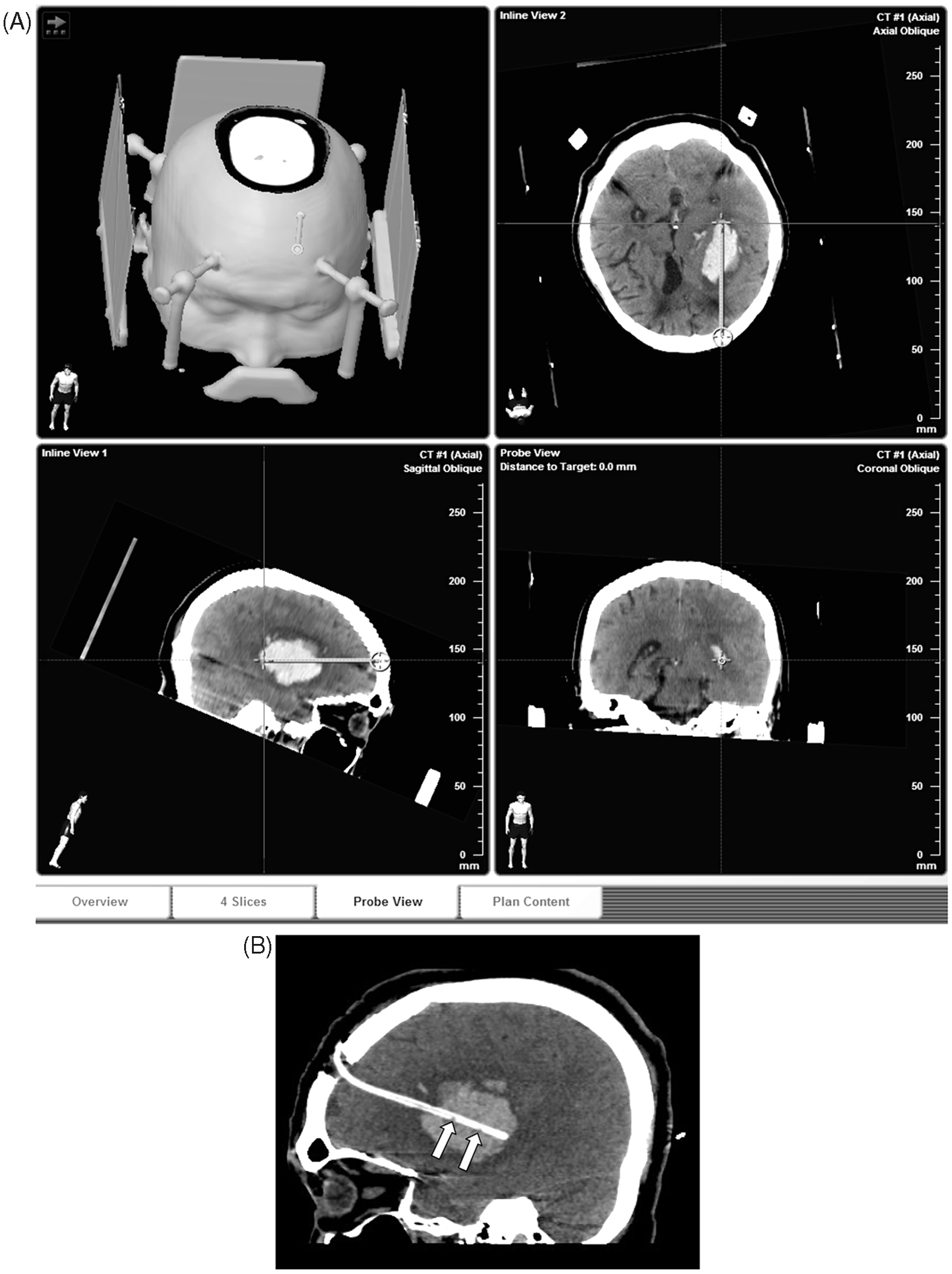
Outcome assessment
The duration of haematoma evacuation (i.e. the time that the catheter remained indwelling in the patient’s brain) and the number of urokinase injections in the two groups were used to assess outcome in this study.
Statistical analyses
All variables were presented as mean ± SD. Categorical data were analysed using the χ2-test; continuous data were analysed using Student's t-test. Differences were considered statistically significant at P < 0.05. Statistical Package for the Social Sciences software (PASW Statistics for Windows®, version 18.0. SPSS Inc., Chicago, IL, USA) was used for the statistical analyses.
Results
Baseline characteristics of two groups of patients included in a study assessing the value of stereotactic surgical planning systems to aid spontaneous intracerebral haematoma treatment.
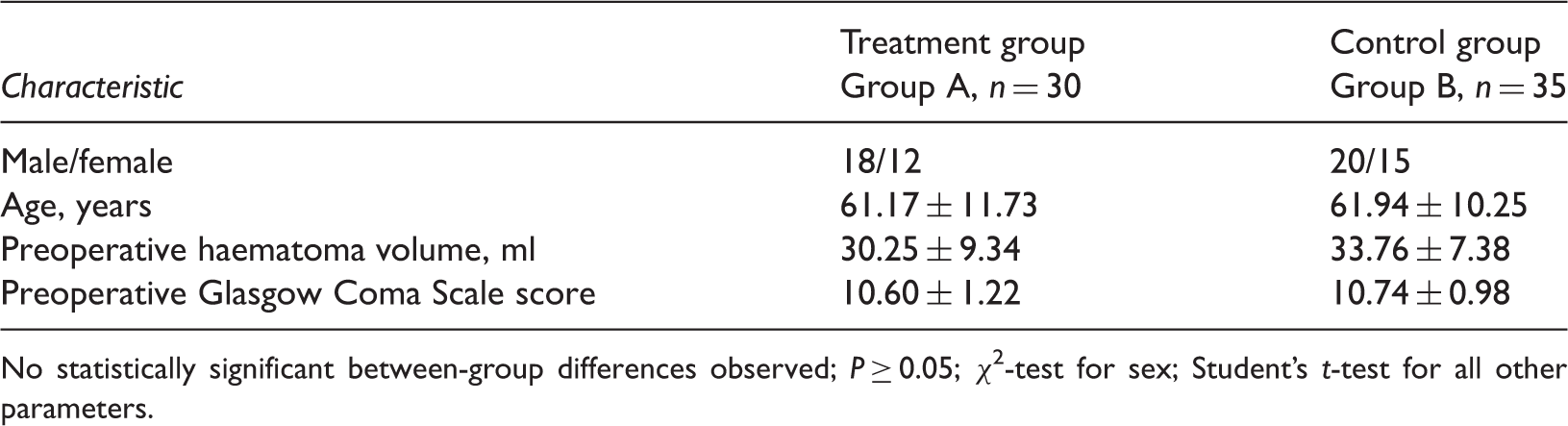
No statistically significant between-group differences observed; P ≥ 0.05; χ2-test for sex; Student’s t-test for all other parameters.
Time taken to evacuate the haematoma and number of urokinase injections (20000 IU/2 ml 0.9% saline) required to dispel the clot in the treatment group compared with the control group, in a study assessing the value of stereotactic surgical planning systems to aid spontaneous intracerebral haematoma treatment.

Student’s t-test.
Discussion
In surgical ICH treatment, the ultimate goal is to remove as much of the clot as quickly and safely as possible. Compared with conventional stereotactics, the SSPS-aided approach described in the present paper designs the optimum trajectory to achieve the goal of clot removal. Consequently, using the SSPS-aided approach may shorten the duration of haematoma evacuation and reduce the requirement for urokinase injection, compared with other approaches.
Several groups1–10,12,15,16 have studied the heavy burden of ICH that results from its mass effect (i.e. the physical attack) and the toxic influence of blood components and blood-degradation products (i.e. the chemical attack). Findings of such research suggest that clot evacuation could play an important role in reducing brain damage and, therefore, improving patient prognosis.
According to the 2010 AHA/ASA guidelines for the management of spontaneous ICH, 11 craniotomy is only recommended for subcortical lobe clots >30 ml in volume or for serious cases of herniation, due to having to cut through uninjured brain to reach the haematoma. For moderate deep ICH, several clinical studies reported minimally invasive clot evacuation through the use of stereotactics to alleviate ICH severity.9,10,12,15,16,20,21 Additionally, in a multicentre randomized controlled trial, stereotactic treatment of ICH by means of a plasminogen activator (SICHPA) 8 was validated as a feasible therapeutic approach, with a favourable safety profile. Compared with the group offered nonsurgical treatment, SICHPA improved the efficacy of clot reductions. 8
Since Backlund and von Holst reported the application of stereotactics for ICH evacuation in 1978, 22 stereotactics has developed gradually, and primarily in two areas: physical haematoma aspirators (such as screw-aspiration or ultrasonic aspiration) and chemical clot lysis (by urokinase or recombinant tissue plasminogen activator). 23 Very little progress has been made in improving the stereotactic concept itself, however. This is because stereotactics typically only considers the target point as the site of action, rather than also considering the role and influence of the needle’s trajectory.
Conventional stereotactic surgery with thrombolysis is generally implemented as follows. From the empirical entry point, a catheter is inserted into the target point (the centre of the hematoma, which is the part with the largest cross-sectional area), then lytic agents are injected into the catheter to lyse the clot via the hole in the catheter tip. However, a major shortcoming of this procedure is that, because there is only one site of action, evacuation efficacy is poor,13,14 resulting in a prolonged indwelling period for the catheter and an increased requirement for lytic agents. This may have underlying risks, such as infection resulting from catheter insertion or injection and neurotoxicity triggered by lytic agents.9,10,24–29 Therefore, many neurosurgeons have sought to improve this technique and have experienced success, but with limitations.9,15,16 To address the issues above, we identified a new method that uses software (frame-based SSPS) to improve the speed of evacuation with added security and accuracy. This method appears to have many potential advantages, compared with conventional approaches. First, the primary CT data are stored as DICOM, thus enabling the intracranial structure to be reconstructed in free orientation and sliced to any planar. This allows operators to select the sections needed to examine the catheter trajectory. Secondly, the software also allows for reconstruction of sections perpendicular to the trajectory, which means that the anatomy along the trajectory can be examined when a puncture is simulated. If the puncture affects any important anatomical structures during simulation, the trajectory can be adjusted. This increases the feasibility of the procedure and improves its safety profile, thereby enhancing operating confidence. Conventional stereotactic puncture uses a blind perforation30,31 so the trajectory is not as flexible as the SSPS approach, since the target and entry points are determined by experience. Third, the distance measurements taken by the software tools in SSPS are in line with the true value. Finally, the process takes <10 min to perform, and uses the neurosurgeon’s preferred trajectory, that passes exactly through the main axis of the haematoma.
Using the frame-based SSPS, the target point is set with the ends of the clot. In our present study, the trajectory was simulated using virtual reality, which was important for keeping the trajectory away from anatomical structures. The trajectory distance through the haematoma was measured by the software. Consequently, the necessary catheter length could be determined in advance, and side holes could be cut to suit the specific circumstances. Together, these procedures sped up clot evacuation. The shorter duration of haematoma evacuations that we observed in group A compared with group B facilitated a shorter catheter indwelling time in the brain, thereby lowering the time-dependent risk of infection.25–27 Theoretically, shortening the duration of haematoma evacuation means that clots disappear more quickly compared with standard interventions, which could have a beneficial effect on alleviating the mechanical injury and chemical damage caused by ICH. Fewer urokinase injections were observed in group A; this had beneficial effects, such as lowering the risk of infection (by reducing the number of injections that were administered).13,24–27 Indwelling catheter procedures are also associated with an increased risk of infection,13,24–27 therefore reducing the timeframe of such procedures may be beneficial for patients. In addition, augmented urokinase doses may increase the risk of bleeding13,23,24 and have potential neurotoxicity.25–29 The lower numbers of urokinase injections reported in group A meant that patients in this group were exposed to lower doses of urokinase. Because any kind of medication has dose-dependent side-effects, a lower requirement for urokinase is likely to have a beneficial impact on safety.
In conventional stereotactic surgery of spontaneous ICHs, the spot of action for thrombolysis and drainage is the catheter tip alone, and the maximum cross-sectional area at the centre of the clot is decided using only two dimensions. Our novel stereotactic technique was aided by frame-based SSPS, which used three-dimensional views of the brain and the ICH. This resulted in practical differences in our clinical study. Therefore, using the frame-based SSPS improved the efficacy, feasibility, and safety of clot evacuation. Furthermore, our report demonstrates the joining of medicine with digital science. Our research presented here indicates that future medicine, especially surgery, should promote minimal invasiveness with maximal individuality, accuracy and standardization, achieved by the application of digital science.32–34 This concept provides an interesting opportunity for future practice.
Because the present study was carried out at a single centre and with a relatively small amount of data, the results were not conclusive. Future studies will aim to investigate the procedure in multiple centres and with larger numbers of cases. We plan to investigate the relationship between the volume of ICH and the dose of lytic agents, and whether the SSPS may lower the dose of lytic agents required. Another limitation of our study was that the results have not been related to follow-up outcome. Future studies will evaluate the short-term outcome (30 days) and long-term prognosis (6 months) of ICH patients who are treated with SSPS.
In conclusion, findings of the current randomized controlled study illustrate the benefits of a frame-based SSPS for the treatment of moderate spontaneous ICH. The frame-based SSPS demonstrated feasibility, together with advanced efficacy and safety, compared with standard approaches. Therefore, frame-based SSPS-aided surgery shows promise and may become the preferred procedure for clot removal, following additional research.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.