
Abstract
Objective
To compare two remifentanil doses (1 µg/kg and 2 µg/kg) in order to determine the preferred dose in intellectually disabled patients undergoing day care dental surgery under sevoflurane-induced general anaesthesia.
Methods
Patients were randomly assigned to receive either 1 µg/kg (group 1) or 2 µg/kg (group 2) remifentanil; both groups received 8% sevoflurane anaesthesia induction. All other conditions were identical in both groups. Heart rate (HR), mean arterial pressure (MAP) and intubation conditions were assessed.
Results
A total of 27/30 (90.0%) patients in group 1 and 29/30 patients (96.7%) in group 2 had acceptable intubation conditions. Remifentanil administration resulted in significant reductions in HR compared with baseline levels, in both groups. There were no significant between-group differences in HR at any timepoint. MAP decreased significantly compared with baseline in group 2 only.
Conclusion
Successful tracheal intubation in intellectually disabled patients can be accomplished with a combination of 1 µg/kg or 2 µg/kg remifentanil and 8% sevoflurane anaesthesia induction, without the requirement for neuromuscular blocking drugs.
Introduction
The perioperative management of intellectually disabled patients can be challenging and, as a result, their dental treatment is generally performed under general anaesthesia on an day care basis. 1 Difficulties during preoperative assessment and insufficient medical examination may result in unforeseen problems with tracheal intubation in these patients. The risk of unpredictable airway problems makes it necessary to avoid the use of neuromuscular blocking drugs (such as rocuronium) during anaesthetic induction. 2
The use of an opioid drug in sevoflurane-induced anaesthesia may depress laryngeal reflexes and improve intubation conditions.3,4 The opioid remifentanil is preferred in day care surgery because of its short duration of action. 5
The aim of the present study was to compare two remifentanil doses (1 µg/kg and 2 µg/kg), in order to determine the preferred dose in intellectually disabled patients undergoing day care dental surgery. In all cases, anaesthesia was induced with 8% sevoflurane, ideally without the use of neuromuscular blocking drugs.
Patients and methods
Study population
The study recruited intellectually disabled patients 6 with American Society of Anesthesiologists 7 physical status I or II, scheduled for dental treatment under general anaesthesia at the Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, Ege University, Izmir, Turkey, between March 2010 and October 2010. Exclusion criteria were: body mass index >35 kg/m2; cardiovascular disease; reactive airway disease; gastroesophageal reflux; renal or hepatic impairment; allergies to any of the study drugs.
The study was conducted with the approval of the Ege University Human Ethics Committee and written informed consent was obtained from the parents or their relatives. For ethical reasons, a placebo group was not included in the study since tracheal intubation without opioid use was deemed harmful.
Anaesthesia
Patients received 0.5 mg/kg oral midazolam 30 min before surgery; electrocardiography, pulse oximetry, noninvasive blood pressure, capnography and inhalational agent were monitored under sedation. Induction of anaesthesia was accomplished via face mask with a Bain circuit, using 8% sevoflurane in 100% oxygen for 2 min with gas flow set to 5 l/min. Immediately after loss of consciousness, intravenous (i.v.) access was secured and 0.01 mg/kg atropine was infused. After baseline measurements (heart rate [HR], mean arterial pressure [MAP]), patients were randomly allocated to one of two groups according to a computer-generated random number table. Patients in group 1 received 1 µg/kg remifentanil; those in group 2 received 2 µg/kg remifentanil i.v. In all cases, tracheal intubation was attempted 90 s after remifentanil administration by the same experienced anaesthetist. If intubation could not be accomplished after two attempts, 0.6 mg/kg rocuronium i.v. was administered.
Measurements
Intubation conditions scoring system 8 used in a study comparing remifentanil 1 µg/kg and 2 µg/kg (administered intravenously) in intellectually disabled patients undergoing day care dental surgery, receiving 8% sevoflurane induction anaesthesia.

Intubation conditions were considered acceptable if the score for each parameter was <2. If any of the measured values was ≥2, intubation conditions were considered unacceptable.
Patients were immediately treated for any side-effects of remifentanil that were observed, including muscle rigidity, hypotension, bradycardia and arterial oxygen saturation <91%. Hypotension (MAP <25% from baseline) was treated with 5–10 mg ephedrine i.v.; bradycardia (HR <50 beats per min) was treated with 0.5 mg atropine i.v.
Statistical analyses
Data were presented as mean ± SD, median (range) or n. Normally distributed data were analysed using Student's t-test; non-normally distributed data were analysed with Mann–Whitney rank sum test, with Bonferroni correction as appropriate. Categorical data were analysed using Fisher’s exact test. Statistical analyses were performed using SPSS® software, version 13.0 (SPSS Inc., Chicago, IL, USA) for Windows®. P-values < 0.05 were considered statistically significant.
Results
Demographic characteristics of intellectually disabled patients undergoing dental surgery using 8% sevoflurane-induced general anaesthesia, included in a study comparing the effect of 1 µg/kg (Group 1) and 2 µg/kg (Group 2) remifentanil, administered intravenously.

Data presented as median (range) or n.
No statistically significant between-group differences; P ≥ 0.05, Student’s t-test.
Numbers of participants with acceptable and unacceptable intubation rating scores, 8 in a study investigating 1 µg/kg (Group 1) or 2 µg/kg (Group 2) remifentanil, administered intravenously to intellectually disabled patients undergoing dental surgery using 8% sevoflurane-induced general anaesthesia.

Other’ categories include patients with scores ≥2 (i.e. unacceptable scores) for the specific parameter listed.
Data presented as n.
No statistically significant between-group differences; P ≥ 0.05, Mann–Whitney U-test.
Administration of opioid resulted in a significant decrease in HR compared with baseline in both groups (P < 0.001 for each comparison; Figure 1), but there were no statistically significant between-group differences in HR at any timepoint.
Heart rate (beats per min) in intellectually disabled patients undergoing dental surgery using 8% sevoflurane-induced general anaesthesia, who also received 1 µg/kg or 2 µg/kg remifentanil, administered intravenously (n = 30 per group). Data presented as mean ± SD; ***P < 0.001 versus baseline, Student's t-test.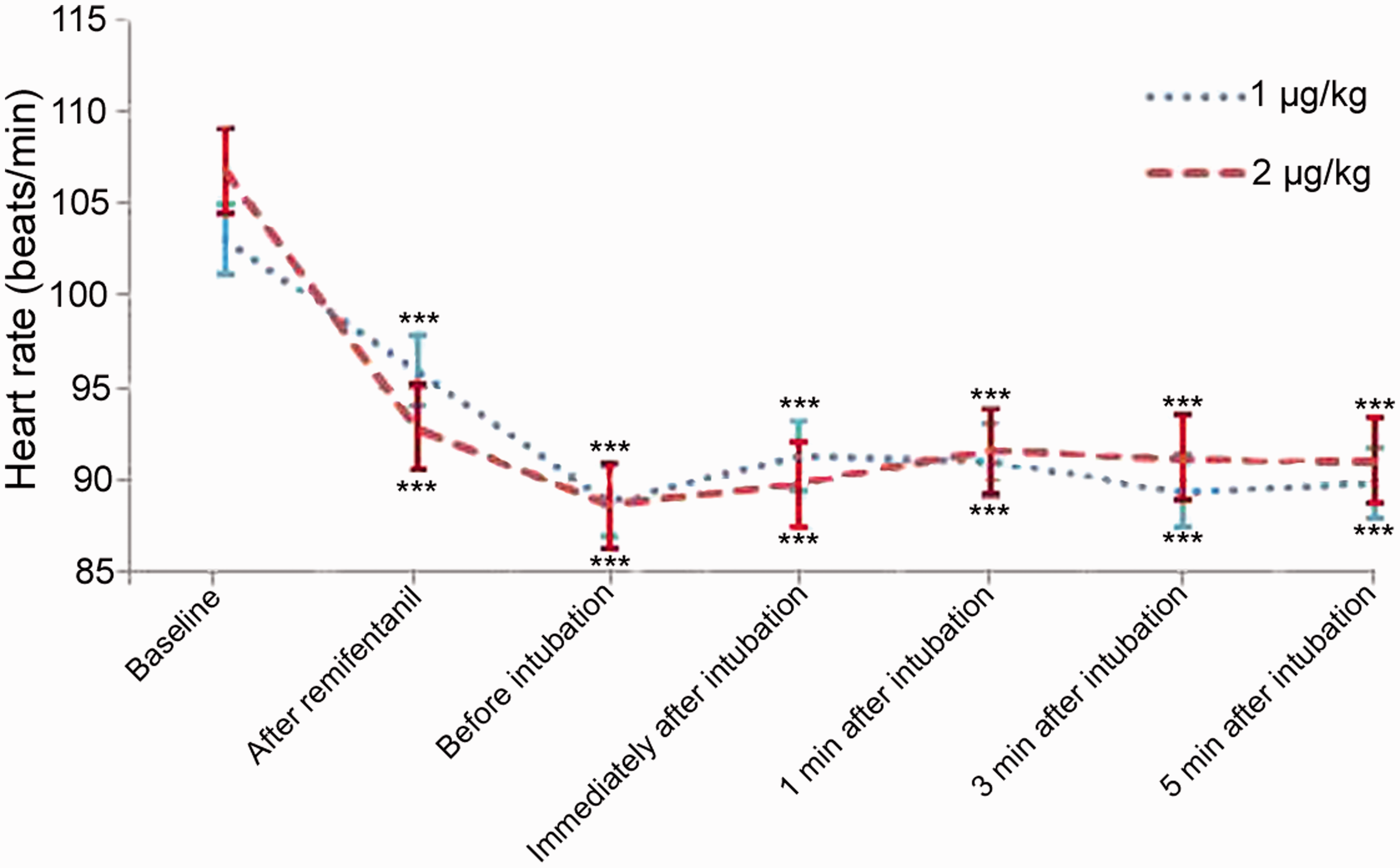
The mean basal MAP was 68.6 ± 9.7 mmHg in Group 1 and 79.6 ± 14 mmHg in Group 2 (this difference was not statistically significant). Administration of opioid resulted in a significant decrease in MAP compared with baseline in group 2 only (P < 0.001; Figure 2).
Arterial pressure (in mmHg) in intellectually disabled patients undergoing dental surgery using 8% sevoflurane-induced general anaesthesia, who also received 1 µg/kg or 2 µg/kg remifentanil, administered intravenously (n = 30/group). Data presented as mean ± SD; ***P < 0.001 versus baseline, Student's t-test.
No patient suffered from clinically significant bradycardia, hypotension, hypoxia or muscle rigidity.
Discussion
The present study found that both 1 µg/kg and 2 µg/kg remifentanil resulted in acceptable intubation conditions, without the use of rocuronium, in 90.0% and 96.7% of mentally disabled patients undergoing sevoflurane anaesthesia, respectively.
The low blood gas solubility coefficient of sevoflurane makes it useful for anaesthetic induction in patients with difficult airways.9–11 Sevoflurane has also been shown to result in superior intubation conditions than propofol/succinylcholine and propofol/alfentanil in children. 12
Appropriate doses of remifentanil can suppress the haemodynamic response to tracheal intubation without neuromuscular blocking drugs, yet allow rapid emergence and return of spontaneous ventilation. 13 These characteristics make remifentanil a practical opioid choice in day care anaesthesia. 5 The analgesic effects of remifentanil account for its positive effects on tracheal intubation conditions.3,4,14 It has been suggested that opioids block afferent nerve impulses caused by stimulation of the pharynx, larynx and trachea during intubation. 15
The present findings are consistent with other studies that reported good-to-optimal conditions for tracheal intubation in 89% and 100% of patients with 1 µg/kg and 2 µg/kg remifentanil, respectively. 3 In addition, 4 µg/kg remifentanil intranasal administration in children significantly improved intubation conditions, compared with placebo. 16
The most common side-effects of remifentanil administration are muscular rigidity, bradycardia and hypotension. 17 There were no cases of muscle rigidity in the present study, however. Sevoflurane induction decreases muscle rigidity following opioid administration,3,18,19 and midazolam has also been shown to have muscle relaxing effects. 20 In addition, benzodiazepine premedication has been shown to prevent muscle rigidity following opioid administration. 21 It seems likely, therefore, that the absence of remifentanil-mediated muscle rigidity in the present study was due to the combined effects of high dose sevoflurane induction and midazolam premedication.
Sevoflurane and remifentanil can cause serious bradycardia and asystole, 22 which can be ameliorated by prophylactic administration of anticholinergic agents (such as atropine). 23 All patients in the present study received atropine before remifentanil administration, in order to prevent serious bradycardia and asystole. As a result, no patient suffered from clinically significant bradycardia.
Hypotension is another undesirable side-effect of remifentanil, 3 and is more likely to occur if a longer time (3 min versus 2 min) is allowed to elapse between remifentanil administration and intubation. 11 Intubation was performed 90 s after remifentanil administration in the present study, and hypotension was not observed in any patient. This may have been due to the sympathetic stimulus and increase in blood pressure caused by intubation occurring before the hypotensive effect of remifentanil had commenced. 24 This finding suggests that intubation should not be unnecessarily delayed after remifentanil administration, although further studies are required to confirm this hypothesis.
In conclusion, induction of anaesthesia with sevoflurane plus remifentanil at two different doses (1 or 2 µg/kg) produces optimal tracheal intubation conditions – without the need for neuromuscular blocking drugs – in premedicated, intellectually disabled patients undergoing day care dental surgery. There were no significant between-dose differences in effect, and both doses are suitable for use. This regimen is useful for cases of outpatient (day case) surgery where it is necessary to avoid the undesirable side-effects of muscle relaxing agents and antagonists.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.