
Abstract
Objective
Nosocomial infection caused by carbapenem-resistant Acinetobacter baumannii is a worldwide problem and treatment options remain controversial. This study investigated the in vitro effect of various antibiotic combinations against carbapenem-resistant A. baumannii strains.
Methods
Antibiotic susceptibility of A. baumannii strains was analysed. In vitro synergistic efficacy of colistin combined with tigecycline, cefoperazone/sulbactam or piperacillin/tazobactam was tested against carbapenem-resistant A. baumannii strains. Synergy studies were performed using an eplisometer test-strip method.
Results
Of the 50 carbapenem-resistant A. baumannii strains tested, 96% were susceptible to colistin and 64% were susceptible to tigecycline. Colistin–tigecycline, colistin–cefoperazone/sulbactam and colistin–piperacillin/tazobactam combinations were found to have synergistic effects against six (12%), two (4%), and one (2%), respectively, of the strains tested.
Conclusions
Colistin combined with tigecycline, cefoperazone/sulbactam or piperacillin/tazobactam revealed synergistic effects in some carbapenem-resistant A. baumannii strains. These results, together with the shortage of treatment options and the risk of developing resistance to colistin, suggest that clinicians should use colistin combined with other antibiotics or β-lactamase inhibitors when treating carbapenem-resistant A. baumannii infection.
Keywords
Introduction
Gram-negative bacteria, such as multidrug-resistant Acinetobacter baumannii, have become an increasing problem in the treatment of nosocomial infection. The inappropriate use of broad-spectrum antibiotics and the developing resistance mechanisms of bacteria have been key factors in the emergence and spread of resistant infections.1–3 Problems encountered with antibiotic treatments, and an increase in acquired and intrinsic resistance mechanisms against antibiotics, have caused Acinetobacter spp. to become alarming factors in nosocomial infection. 4 Acinetobacter spp. commonly display a number of antibiotic resistance mechanisms, including: AmpC β-lactamase/D-alanine carboxypeptidase and extended spectrum β-lactamase enzymes for resistance against β-lactams; carbapenemases, outer membrane proteins and excretion pumps for resistance against carbapenems; chromosome and plasmid-borne resistance mechanisms against fluoroquinolones. In addition, oxacillinase-type carbapenemases are commonly found in Acinetobacter spp.5–7 The development of resistance to carbapenems (which are the most important antibiotics in the treatment of Acinetobacter spp. infections), has increased the use of polymyxins, which are the only effective antibiotic group. The high success rates of combination treatments in cases of possible resistance against colistin, and in carbapenemase-producing Gram-negative bacterial infections, have resulted in increased use of colistin in combination with other antibiotics. 8
The β-lactamase inhibitors sulbactam and tazobactam appear to be highly effective against multidrug-resistant Acinetobacter spp., 9 with sulbactam reported to have bactericidal efficacy over Acinetobacter spp.10–12 Sulbactam combined with β-lactam antibiotics remains an effective treatment option for Acinetobacter spp. infections. 13 Tigecycline and polymyxins are currently the preferred choices of antibiotics for infections caused by carbapenem-resistant Acinetobacter spp. 8
Tigecycline is the semisynthetic derivative of minocycline 14 that has been modified to evade many of the mechanisms of resistance to tetracycline. 15 In particular, tigecyline is used for the treatment of complicated skin and skin structure infections, and intra-abdominal infections. 15 Tigecycline is not effective, however, against Pseudomonas spp. or Proteus spp. 15 The possibility of bacterial resistance developing against tigecycline, during treatment, has resulted in increased use of tigecycline in combination with colistin. Combined treatment (using either colistin and tigecycline or colistin and β-lactamase inhibitors) is considered suitable for carbapenem-resistant Acinetobacter spp. infections.8,16,17
Colistin is frequently used to treat infections caused by carbapenem-resistant A. baumannii, due to its efficacy. 8 The aim of the present study was to perform in vitro research, using the eplisometer method, 18 to investigate the efficacy of colistin combined with either tigecycline, or with β-lactam antibiotics/β-lactamase inhibitors, in the treatment of these infections. Carbapenem-resistant Acinetobacter spp. are among the most common causes of nosocomial infection encountered in our hospital, where antibiotic susceptibility testing is routinely undertaken with disk diffusion analysis methods.
Materials and methods
This study was performed at the Faculty of Medicine, Gaziantep University, Sahinbey Research and Training Hospital, Gaziantep, Turkey, between March and May 2012. Eplisometer (Etest®; bioMerieux, Marcy l’Etoile, France) disk diffusion testing is costly to undertake; consequently only a limited (consecutive) number of the bacterial strains that were isolated were analysed, governed by the number of Etest® kits available. Carbapenem-resistant strains were identified using a Vitek®2 bacterial identification device (bioMerieux) according to the manufacturer’s instructions. All carbapenem-resistant A. baumannii strains isolated during the study period were stored at −20℃ in a brain heart infusion agar tube, to which 4% glycine was added. This study was approved by the Ethics Committee of Gaziantep University Medical Faculty (190/25.10.2011).
Antibiotic susceptibility tests
Antibiotic susceptibility tests were performed using the Vitek® 2 system (bioMerieux), according to the standards of the Clinical and Laboratory Standards Institute. 19
Synergy test
The synergy test was performed on all carbapenem-resistant A. baumannii strains, using the Etest® method. 18 Minimum inhibitory concentration (MIC) values were assessed: first for colistin, tigecycline, cefoperazone/sulbactam and piperacillin/tazobactam alone, then in combination (colistin–tigecycline, colistin–cefaperazon/sulbactam, colistin–piperacillin/tazobactam) for each carbapenem-resistant A. baumannii strain.
For single antibiotic or antibiotic/β-lactamase inhibitor tests, bacterial suspensions (100 µl), prepared to 0.5 MacFarland standard turbidity, were spread onto 150 mm Müller–Hinton agar plates. Etest® strips (AB Biodisk, bioMerieux) for colistin, tigecycline, cefoperazone/sulbactam and piperacillin/tazobactam were then placed onto the inoculated plates, and the plates were incubated for 24 h at 37℃. MIC values were then recorded.
The synergy tests were performed by preparing fresh passages from the bacterial suspensions. Bacterial suspensions (100 µl), prepared to 0.5 MacFarland standard turbidity, were spread onto 150 mm Müller–Hinton agar plates. Etest® strips (AB Biodisk) for cefoperazone/sulbactam, piperacillin/tazobactam and tigecycline were placed separately onto the plates. The site at which the strip was placed was marked on the plate and the plates were incubated for just 1 h at 37℃. Following incubation, the Etest® strips were aseptically removed from the plates and the Etest® strip for colistin was placed onto the marked space, exactly overlapping the first strip. Plates were then incubated for 24 h 37℃ and the MIC values were recorded.
Calculations
The relationship between drugs used individually or in combination was assessed by calculating the Fractional Inhibitory Concentration (∑FIC) value, according to the following formula:



A calculated ∑FIC value of ≤0.5 represented a synergistic effect (i.e., total effect greater than the sum of the individual antibiotic effects), a value between >0.5 and <2 represented an indifferent (additive) effect (i.e. no additional contribution from including the second antibiotic, compared with when the first antibiotic [colistin, in this case] was used alone), and a value of ≥2 represented an antagonistic effect (i.e., total effect less than the sum of the individual effects). 20
Results
Distribution of 50 carbapenem-resistant Acinetobacter baumannii clinical isolate strains according to clinic and sample type of origin.

Data presented as n of Acinetobacter baumannii clinical isolates.
IICU, internal intensive care unit; PICU, pediatric intensive care unit; CSF, cerebrospinal fluid.
Antibiotic susceptibility of carbapenem-resistant Acinetobacter baumannii strains.
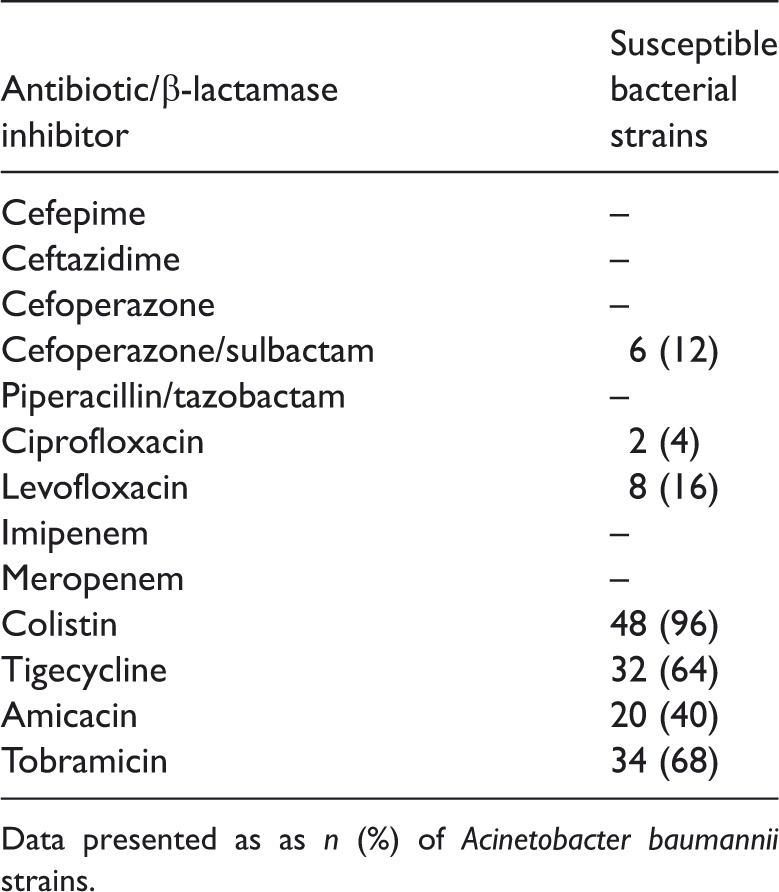
Data presented as n (%) of Acinetobacter baumannii strains.
Minimum inhibitory concentration (MIC) values for colistin, tigecycline, ceforerazone/sulbactam, piperacillin/tazobactam and colistin combined with tigecycline, cefoperazone/sulbactam and piperacillin/tazobactam for bacterial strains in which a synergistic effect was demonstrated.

Data presented as MIC values.
Synergy test results for colistin–tigecycline, colistin–cefoperazone/sulbactam and colistin–piperacillin/tazobactam against carbapenem resistant Acinetobacter baumannii strains.

Data presented as n (%) of bacterial strains.
Discussion
Treatment options for carbapenem-resistant A. baumannii strains are very limited, and these strains are often resistant to many antibiotics including aminoglycosides and quinolones. 8 The noncarbapenem antibiotics, including tigecycline and polymyxins, are important compounds because cross resistance to β-lactam antibiotics has not been detected. 8 The β-lactamase inhibitors sulbactam and tazobactam are highly effective against multidrug-resistant A. baumannii.9,13
Colistin and tigecycline are the only antibiotic agents available for carbapenem-resistant A. baumannii infections; however, resistance to tigecycline in carbapenem-resistant A. baumannii is a problem, with different studies reporting tigecycline resistance rates ranging between 9.5% and 66%.21,22 Multidrug-resistant A. baumannii strains are only susceptible to colistin. 8 Increasing use of colistin and the presence of heteroresistance in clinical isolates of multidrug-resistant A. baumannii, however, has resulted in the development of resistance to colistin. 23
Resistance to colistin has led to research into whether colistin should be used alone or in combination with other treatments. The present study evaluated the treatment options for infections caused by carbapenem-resistant A. baumannii strains. Susceptibility rates of the 50 cabapenem-resistant A. baumannii strains investigated were 96% for colistin, 64% for tigecycline and 12% for cefoperazone/sulbactam. All of the strains were found to be resistant to piperacillin/tazobactam treatment. Combined colistin–tigecycline treatment was found to be synergistic in 12% of the strains tested, which was similar to another study in which the same combination had a synergistic effect in 8.3% of the strains tested. 17 Successful in vivo treatment of multidrug-resistant A. baumannii infection with tigecyline in combination with colistin, meropenem, piperacillin–tazobactam or cotrimoxazole has also been reported, however, the results were not supported by in vitro synergy tests.24,25
Sulbactam and tazobactam are effective against Acinetobacter isolates. 9 In the present study, sulbactam and tazobactam alone were unavailable, therefore either cefoperazone/sulbactam or piperacillin/tazobactam were used in combination with colistin, both of which displayed synergistic effects in 4% and 2%, respectively, of the strains tested. Sulbactam in combination with the aminoglycosides, rifampin and azithromycin has been shown to have synergistic effects against multidrug-resistant Acinetobacter strains.26,27 In the present study, however, the strains tested were resistant to carbapenem and the highest synergistic activity was shown with the colistin–tigecycline combination. The present study did not evaluate colistin–carbapenem or colistin–sulbactam combinations.
Studies in which monotherapy and combination therapy were compared show that combination therapy is superior to monotherapy, regarding both efficacy and resistance development in carbapenemase-producing Gram-negative bacteria.8,28 Although colistin is effective against carbapenem-resistant and multidrug-resistant A. baumannii strains, monotherapy may cause emergence of resistant strains, particularly for infections caused by colistin heteroresistant A. baumannii. 29 Increased use of colistin appears to be a substantial risk for the development of resistance.
Combinations of rifampicin with either colistin or carbapenem have been reported to have synergistic effects against Pseudomonas aeruginosa, Klebsiella pneumonia and Acinetobacter strains, and show a bactericidal effect – even though the strain may be resistant to carbapenems or rifampicin alone,8,30 and combination therapies are more effective against carbapenem-resistant Acinetobacter strains. 16 In another study, no synergy was detected with combinations of colistin with carbapenems or rifampicin; however decreases in carbapenem and rifampicin MIC values were detected. 31 Colistin may be used successfully for the treatment of multidrug-resistant and colistin-sensitive Acinetobacter strains. The synergistic effect of each antibiotic is specific to each clinical isolate, and the combination treatment efficacy may vary for every single strain. 8
The present study may be limited by the use of a single test method to assess synergy. The in vitro effects of antibiotics can vary depending on the test methodology, and there is currently no standardized method for in vitro synergy testing of resistant bacterial strains. 32 The sequential Etest strip method used in the present study has been used by others to show synergy.33,34 Another technique comprising incorporation of the first treatment into the agar prior to inoculation with the test bacteria, followed by addition of the second treatment as an Etest strip, may provide improved reliability compared with the sequential Etest strip method.31,33
In conclusion, the lack of therapeutic options in the treatment of carbapenem-resistant A. baumannii infections, and lack of novel antibiotics against these strains, has made combination therapy a superior treatment option compared with monotherapy. The role of polymixins, such as colistin, in combination with other antibiotics is to produce rapid permeabilization of the outer membrane, permitting the entry of other agents in to the bacterial cell. 16 Colistin appears to be a good choice in carbapenem-resistant A. baumannii infections, but combination therapy should be the preferred choice of treatment as it improves the possibility of achieving a synergistic effect against the strain being treated and helps to overcome the development of resistance.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.