
Abstract
Objective
A prospective, randomized, double-blind, placebo-controlled, parallel-group multicentre study to evaluate the efficacy and safety of diclofenac 4% spray gel for the treatment of acute, uncomplicated ankle sprain.
Methods
Outpatients with acute, uncomplicated, one-sided ankle sprain were randomly assigned to receive diclofenac 4% spray gel or placebo (vehicle) three times daily for 14 ± 1 days. The main efficacy endpoint was the intra-individual response to treatment (≥50% decrease in swelling of the injured ankle after a treatment period of ≤10 days).
Results
The response rate was significantly higher in the diclofenac group (n = 118) than the placebo group (n = 114) (91.5% vs. 82.5%). After 3–4 days’ treatment, diclofenac spray significantly reduced swelling, spontaneous pain, pain on active movement and tenderness compared with placebo. Diclofenac spray was well tolerated, with a low overall rate of adverse events.
Conclusions
Diclofenac 4% spray gel rapidly relieves pain and improves mobility in patients with acute, uncomplicated ankle sprain and is well tolerated. It may be a useful treatment option for other acute soft tissue injuries.
Introduction
Nonsteroidal anti-inflammatory drugs (NSAIDs) are commonly used for the treatment of soft tissue injuries, with the aim of relieving pain and reducing inflammation and swelling.1,2 Topical NSAIDs are available as over-the-counter medications and are used as alternatives to oral formulations: they have been clinically shown to be effective and well tolerated for the short-term management of acute mild-to-moderate pain and inflammation due to injuries such as ankle sprain, and for the longer term management of chronic conditions such as osteoarthritis.3–5 Topical diclofenac is a commonly used NSAID that penetrates the skin to reach joints, muscles and synovial fluid, and preferentially distributes and persists in the target inflamed tissues.6–9 Clinical studies have demonstrated that it is an effective analgesic and anti-inflammatory agent for the treatment of acute and chronic painful conditions, resulting in improved mobility and accelerated healing.3,10–14
The efficacy of a topical NSAID depends upon its ability to penetrate deeply enough to reach the inflamed tissues. 3 The formulation can affect local penetration and pharmacokinetic characteristics, and a balance between lipid and aqueous solubility is required for optimal penetration and therapeutic efficacy. 3 Topical diclofenac is usually formulated as a potassium or sodium salt, and pharmacokinetic analyses have demonstrated that these penetrate rapidly through the skin to reach the underlying tissues. 15 A 4% (w/w) diclofenac spray gel formulation has been developed, containing the micelle-forming agent lecithin in an aqueous–alcohol microemulsion base (MIKA Pharma GmbH, Speyer, Germany). This has shown favourable dermal penetration and low systemic availability, 16 suggesting that it may also be effective in the treatment of acute pain and inflammation. This prospective, randomized, double-blind, placebo-controlled, parallel-group, multicentre study was performed to evaluate the efficacy and safety of diclofenac spray in the treatment of acute uncomplicated ankle sprain, which is considered to be an appropriate model to assess efficacy in acute painful conditions. 12
Patients and methods
Study population
In this prospective, randomized, double-blind, placebo-controlled, parallel-group, multicentre study (n = 15, all based in Hungary), male and female outpatients with acute, uncomplicated, one-sided ankle sprain were recruited between 1 July 1998 and 8 July 1999. Inclusion criteria were: age 18–50 years; acute, uncomplicated, one-sided ankle sprain with swelling ≥12 mm (defined as the difference between the maximum circumference of the injured and the contralateral ankle); injury occurred within 2–18 h before enrolment; presence of spontaneous pain (measured on a 100 mm visual analogue scale [VAS], ranging from 0 [no pain] to 100 [unbearable pain]); pain on active movement (POAM), tenderness and impairment of joint mobility (measured on a 4-category verbal scale: 0, none; 1, slight; 2, moderate; 3, strong), with total pain score for POAM, tenderness and impairment of joint mobility ≥5 and ≤7. Exclusion criteria were: ankle fracture, ligament rupture or severe ankle sprain not considered amenable to treatment with topical NSAIDS alone; use of medication (other than the study drugs and rescue medication [paracetamol]) for the treatment of complaints caused by the affected ankle or other inflammatory or painful conditions (e.g. headache, toothache).
The study was registered and approved by the Hungarian National Institute of Health (no. 4526/40/98). Patients provided written informed consent and were randomly assigned to one of two parallel treatment groups according to the numerical order in which they were enrolled, using a computer-generated random assignment schedule.
Study design
Patients were examined and randomized on visit 1 (V1; day 1), with further visits on day 3/4 (V2), day 7/8 (V3), day 10/11 (V4) and day 14 ± 1 (V5). Patients were randomized to one of the following treatment regimens: A, diclofenac 4% spray gel (0.8–1.0 g spray gel containing 32–40 µg diclofenac sodium; vehicle containing soy bean lecithin) applied topically to the skin with the affected region sprayed completely (using 4–5 × 200 µl actuations of the spray pump) and gently rubbed in if necessary, three times per day at regular intervals of about 7–8 h (corresponding to daily dose of 96–120 mg diclofenac sodium) for 14 ± 1 days; or B, placebo (vehicle only, no active ingredient), applied in the same manner as diclofenac spray, three times per day for 14 ± 1 days. All patients and investigators were blinded to treatment.
Paracetamol 500 mg tablets were allowed as analgesic rescue medication; two packages of 10 tablets were made available for each patient, one for each week of treatment. Nonpharmacological treatment of ankle sprain (e.g. compression bandage, ice packs, freezing spray, etc.), other than resting the leg, was not allowed.
Study objectives and assessments
The primary objective of the study was to verify the efficacy of diclofenac 4% spray gel in the treatment of patients with uncomplicated, one-sided ankle sprain following a sports or accidental injury. The primary endpoint was the intra-individual response to treatment, defined as ≥50% decrease in swelling of the injured ankle from baseline after a treatment period of ≤10 days, and presented as the number of patients with a ‘Yes’ or ‘No’ response. Swelling was calculated as the difference between the maximum circumferences of the patient’s injured ankle and the uninjured ankle (mm). Circumferences were measured personally by the investigator who ran the study in each centre using a tape measure, with the position of the tape measure marked with a dermal pencil. To ensure reproducibility, the measurements were performed according to the ‘figure of eight’ method, which is generally accepted as being validated. 27 The investigators had been properly trained in the use of this method during an investigators’ meeting. Treatment response was derived from the relative change in swelling from baseline, calculated using (swelling [post] – swelling [baseline])/swelling [baseline].
Secondary efficacy variables included change in spontaneous pain score (using the 100-mm VAS), change in presence of spontaneous pain (2-category verbal scale, ‘No’ and ‘Yes’), changes in POAM, tenderness and impairment of passive joint mobility scores, consumption of rescue medication in case of ankle pain (total number of paracetamol tablets; V2–V5), and the investigators’ and patients’ global assessments of therapeutic efficacy (4-category verbal scale: 1, very good; 2, moderate; 3, slight; 4, no effect; V5). Efficacy measurements were taken at all visits, except where indicated.
The secondary study objective was to determine the local and systemic tolerability of diclofenac spray when administered three times daily for 14 days. The major safety parameters were the nature and frequency of adverse events (AEs) reported by patients (V2–V5). Objective assessments comprised clinical laboratory tests (haematology, hepatic and renal function) performed at the beginning and the end of the study (V1 and V5). An overall (global) assessment of tolerability was also made by both the physician and the patient at V5 (4-category verbal scale: 1, excellent; 2, good; 3, moderate; 4, poor).
Statistical analyses
The pivotal efficacy evaluation was conducted in the intention-to-treat sample (ITT; all patients randomized into the study and in whom at least one visit postdose with measurements in all efficacy variables was completed). To investigate study robustness, this was supplemented with an evaluation on the per-protocol sample (PP; patients who completed all planned visits, or premature healing patients in whom healing could be stated as complete, or as almost complete remission of symptoms with all efficacy assessments made until the time of discharge from the trial by the respective investigator).
Acute ankle sprain-related swelling and pain score decline exponentially over time with NSAID treatment, 17 with a similar but slower course seen in untreated patients due to self-healing. 18 Therefore in the ITT sample, missing efficacy data were extrapolated whenever possible using either last-observation-carried-forward (in the case of early full curing), or Dost’s rule as applied to pharmacokinetics.19,20 This approach was used for data regarding swelling, spontaneous pain (VAS), spontaneous pain (verbal score), POAM, tenderness and impairment of passive joint mobility.
The frequencies of patients with and without treatment response were entered into a 2 × 2 contingency table. Confirmative statistics were carried out with hypothesis testing. The significance limit was pre-specified to α = 0.05 (one-sided) and the type II error to β = 0.15 (power 85%).
The study design assumed a 66.6% positive response rate under placebo treatment and an 84% positive response rate under active treatment, based on experience from other trials.21,22 A sample size of 128 patients in each treatment group was required to ensure a total of 111 evaluable patients per group in the ITT sample.
Data were presented as mean (95% confidence intervals) or n (%). Between-group comparisons by visit in non-normally distributed continuous variables (mm circumference, VAS scores, changes in %) were made using rank-sum test with Mann–Whitney U-test. Between-intervention group comparisons of verbal scores were analysed with Fisher’s exact test for 2 × 2 tables, or Cochran–Mantel–Haenszel test for 2 × k (k = 3,4… j) tables grouped by visit. The global efficacy score was dichotomized before contingency testing. Statistical analyses were performed using SYSTAT® version 9 (Systat Software Inc., Chicago, IL, USA) for Windows, 23 or BiAS. 24 Empirical P-values < 0.05 were considered statistically significant. When required, an α-adjustment was applied to control for type-I error multiplicity. In order to evaluate treatment effect in terms of medical-based evidence, the number needed to treat, 25 absolute and relative risk ratio, odds ratio and their respective 95% confidence limits 26 were computed from the response contingency table.
Results
In total, 236 patients were enrolled and randomized to treatment or placebo (diclofenac n = 120, placebo n = 116). Of these, 12 patients withdrew (six in each group): one patient in each group discontinued due to AEs, four patients in each group were lost to follow-up (did not return for the next visit), one patient in the diclofenac group withdrew consent and one patient in the placebo group withdrew because of insufficient efficacy. Four patients (two in each group) were lost to follow-up after V1 (baseline), and were not eligible for the ITT sample. The ITT sample therefore included 232 patients (diclofenac n = 118, placebo n = 114; Figure 1). The PP sample included 224 patients (diclofenac n = 114, placebo n = 110). There were no significant between-group differences in patient characteristics or efficacy variables (Table 1).
Flow chart indicating randomization of patients included in a double-blind, placebo-controlled trial of diclofenac 4% spray gel in the treatment of acute, uncomplicated ankle sprain. Demographic and baseline clinical efficacy variables of patients included in a study to investigate the clinical benefits of diclofenac 4% spray gel (three times per day for 14 ± 1 days) versus placebo for treatment of acute, uncomplicated ankle sprain (intention-to-treat data set, n = 232). Data presented as n (%) or mean ± SD (95% confidence interval). VAS, visual analogue scale (1–100 mm).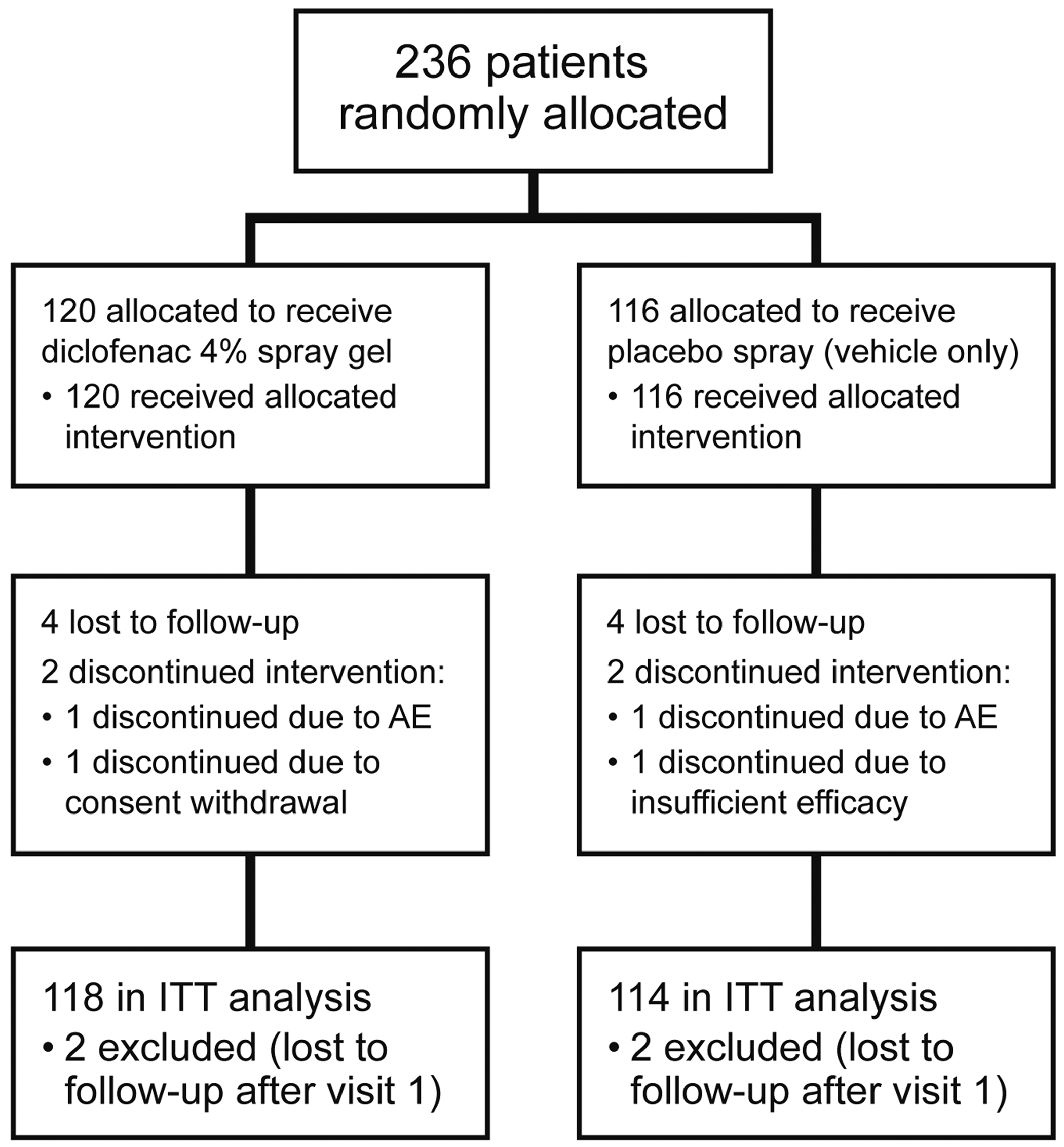

Mean ankle swelling (mm) before and during treatment with diclofenac 4% spray gel (three times per day for 14 ± 1 days) versus placebo for treatment of acute, uncomplicated ankle sprain (intention-to-treat data set, n = 232).

Data presented as mean (95% confidence interval).
Mann–Whitney U-test
V1, baseline; V2, day 3/4; V3, day 7/8, V4, day 10/11; V5, day 14 ± 1; NS, not statistically significant (P ≥ 0.05).
Data regarding the relative change in swelling from baseline (the primary efficacy variable) are shown in Figure 2. Diclofenac treatment was associated with larger decreases in swelling than placebo, statistically significant at all postbaseline timepoints apart from V3 (difference between groups: V2, 9.2% [P = 0.007]; V3, 5.9% [P = 0.09, NS]; V4, 6.7% [P = 0.015]; V5, 4.0% [P = 0.048]). At V5, swelling had decreased from baseline by 87.7% (90.6, 84.8%) in the diclofenac group compared with 83.7% (86.9, 80.5%) in the placebo group (P = 0.048).
Change from baseline in ankle swelling following treatment with diclofenac 4% spray gel (three times per day for 14 ± 1 days) or placebo in patients with acute, uncomplicated ankle sprain (intention-to-treat data set, n = 232). Visit 1, baseline; visit 2, day 3/4; visit 3, day 7/8, visit 4, day 10/11; visit 5, day 14 ± 1.
The response rate was significantly higher in the diclofenac group than the placebo group (91.5% vs 82.5%; P = 0.03). Response rates were evaluated for all post-dose visits (Figure 3), and were significantly higher in the diclofenac group than the placebo group at V2 and V3 (P < 0.01) and V4 (P < 0.05). There was no statistically significant between-group difference at V5.
Proportion of responders (defined as ≥50% decrease in swelling of the injured ankle within ≤10 days) following treatment with diclofenac 4% spray gel (three times per day for 14 ± 1 days) or placebo in patients with acute, uncomplicated ankle sprain (intention-to-treat data set, n = 232). Visit 1, baseline; visit 2, day 3/4; visit 3, day 7/8, visit 4, day 10/11; visit 5, day 14 ± 1.
Clinical benefits of diclofenac 4% spray gel (three times per day for 14 ± 1 days) versus placebo for treatment of acute, uncomplicated ankle sprain, estimated from response rates. a

Data presented as mean (95% confidence interval).
ITT, intention to treat; PP, per protocol.
Response defined as ≥50% decrease in swelling of the injured ankle from baseline after a treatment period of ≤10 days.
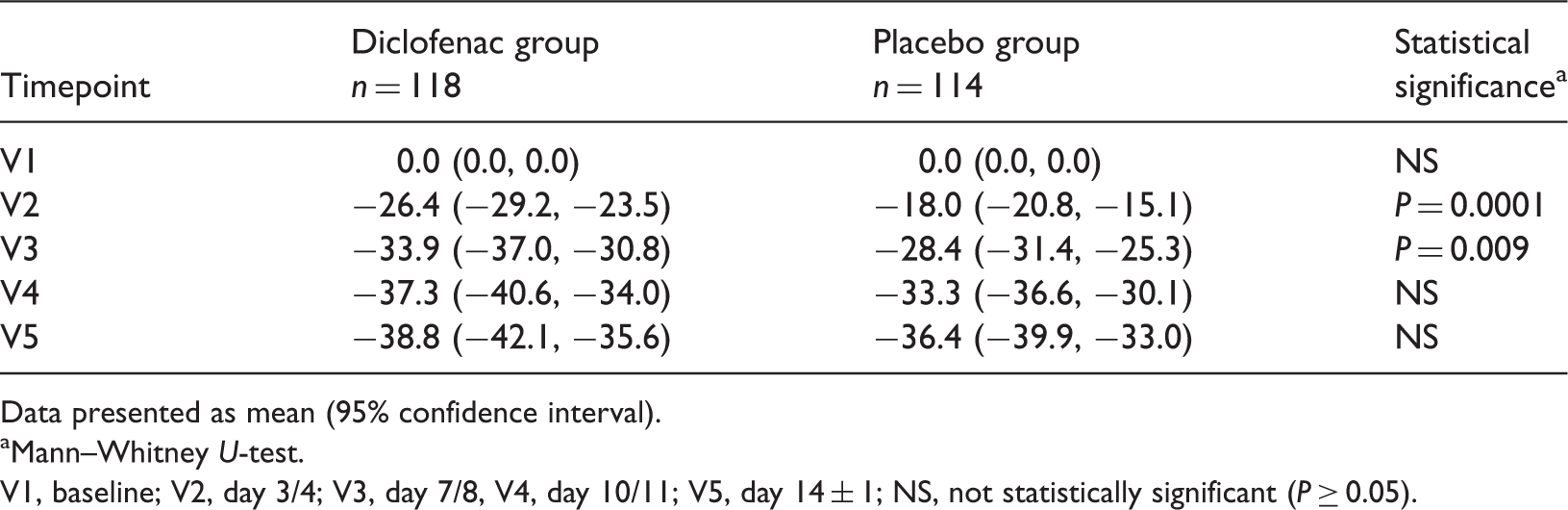
Spontaneous pain VAS scores were significantly lower in the diclofenac group than the placebo group at all timepoints (P < 0.05, Figure 4). Data regarding the change from baseline in spontaneous pain at rest (VAS) scores are shown in Table 4. The change in score from baseline was significantly higher in the diclofenac group than the placebo group at V2 and V3 (P = 0.0001 and P = 0.009, respectively; Table 4).
Spontaneous pain at rest (visual analogue scale, mm) following treatment with diclofenac 4% spray gel (three times per day for 14 ± 1 days) or placebo in patients with acute, uncomplicated ankle sprain (intention-to-treat data set, n = 232). Visit 1, baseline; visit 2, day 3/4; visit 3, day 7/8, visit 4, day 10/11; visit 5, day 14 ± 1. Percentage change from baseline in spontaneous pain (visual analogue scale) before and during treatment with diclofenac 4% spray gel (three times per day for 14 ± 1 days) versus placebo for treatment of acute, uncomplicated ankle sprain (intention-to-treat data set, n = 232). Data presented as mean (95% confidence interval). Mann–Whitney U-test. V1, baseline; V2, day 3/4; V3, day 7/8, V4, day 10/11; V5, day 14 ± 1; NS, not statistically significant (P ≥ 0.05).
Spontaneous pain at rest was reported by all patients at baseline, with the exception of two cases in the diclofenac group. At V4 and V5, significantly more patients in the diclofenac group reported an absence of pain than in the placebo group (P = 0.005 and P = 0.002, respectively). There was no significant between-group difference at V2 and V5 (Figure 5).
Number of patients reporting no spontaneous pain (2-category verbal scale, ‘yes’ or ‘no’) following treatment with diclofenac 4% spray gel (three times per day for 14 ± 1 days) or placebo for acute, uncomplicated ankle sprain (intention-to-treat data set, n = 232). Visit 1, baseline; visit 2, day 3/4; visit 3, day 7/8, visit 4, day 10/11; visit 5, day 14 ± 1.
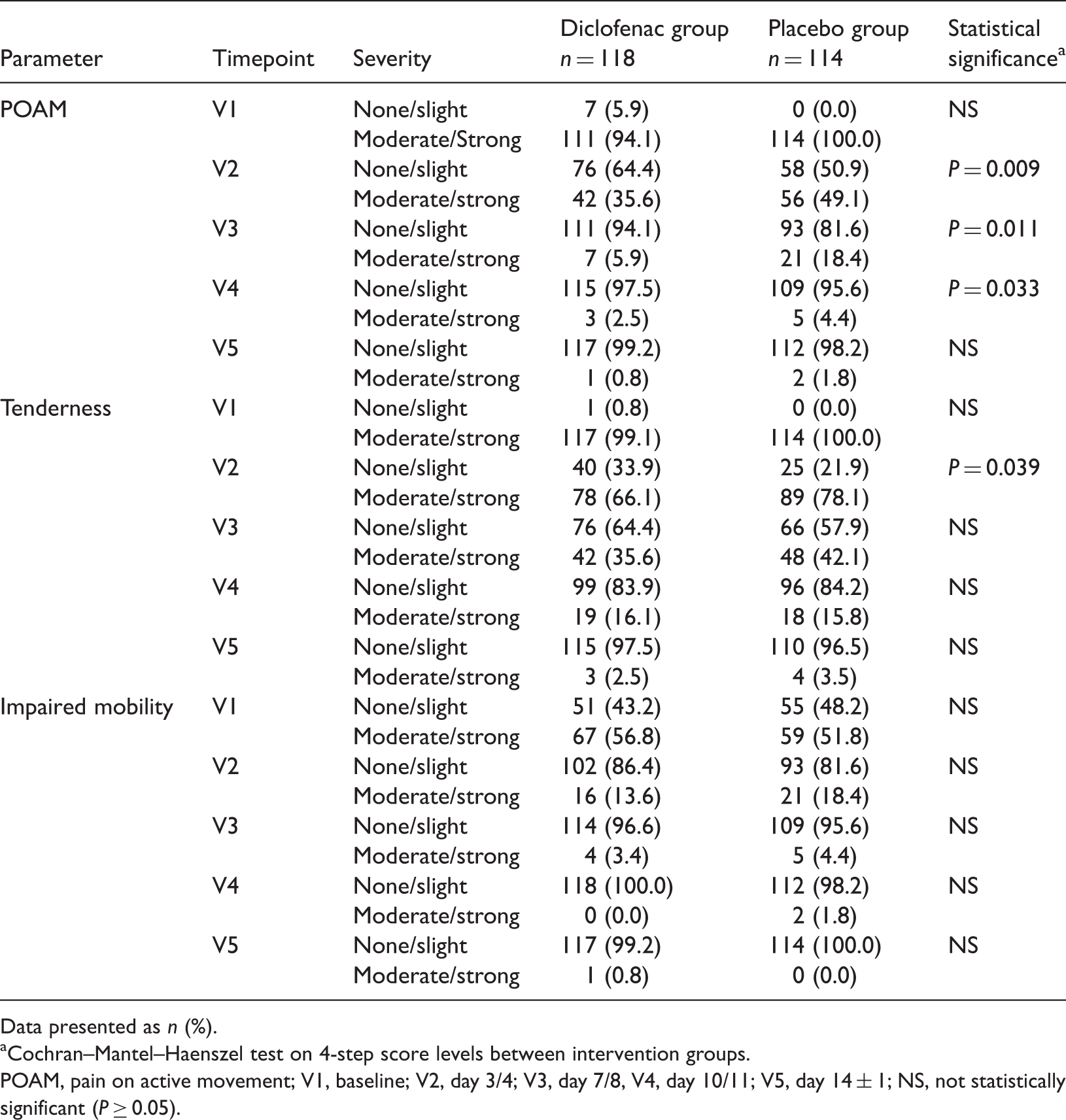
Changes in secondary efficacy variables following treatment of acute, uncomplicated ankle sprain with diclofenac 4% spray gel (three times per day for 14 ± 1 days) or placebo (intention-to-treat data set, n = 232).
Data presented as n (%).
Cochran–Mantel–Haenszel test on 4-step score levels between intervention groups.
POAM, pain on active movement; V1, baseline; V2, day 3/4; V3, day 7/8, V4, day 10/11; V5, day 14 ± 1; NS, not statistically significant (P ≥ 0.05).
The majority of patients (99.1% in the diclofenac group and 100% in the placebo group) reported moderate/strong tenderness at baseline (Table 5). At V2, significantly more patients in the diclofenac group reported none/slight tenderness than in the placebo group (P = 0.039). There were no other between-group differences in tenderness at any timepoint.
At baseline, moderate/strong impairment of joint mobility was reported by 56.8% of patients in the diclofenac group and 51.8% of those in the placebo group (Table 5). There were no significant between-group differences at any timepoint.
Investigators’ and patients’ global assessments of efficacy and tolerability of diclofenac 4% spray gel (three times per day for 14 ± 1 days) or placebo for treatment of acute, uncomplicated ankle sprain (intention-to-treat data set, n = 232).

Data presented as n (%).
Global efficacy scores assessed using a 4-step verbal scale, where 1 = very good, 2 = moderate, 3 = slight, 4 = no effect.
No statistically significant between-group differences (P ≥ 0.05); aCochran–Mantel–Haenszel test; bone-sided Fisher’s exact test after dichotomization.
n = 3 diclofenac and n = 4 placebo judgements missing; dn = 4 diclofenac and n = 4 placebo judgements missing.
In total, 29 patients in the diclofenac group and 19 patients in the placebo group took at least one tablet (range 1–7 tablets) of rescue medication for ankle complaints over the treatment period. There were no significant between-group differences in the number of tablets taken.
Number and severity of adverse events associated with diclofenac 4% spray gel (three times per day for 14 ± 1 days) or placebo for treatment of acute, uncomplicated ankle sprain (all randomized patients, n = 236).

Data presented as n.
NR, not related to study drug; AAT, aspartate aminotransferase; ALT, alanine aminotransferase; AP, alkaline phosphatase.
Discussion
This prospective, randomized, double-blind, placebo-controlled study demonstrated superior efficacy of diclofenac 4% spray gel compared with placebo (vehicle) in reducing swelling and pain resulting from ankle sprain. The number of responders (defined as the rate of subjects achieving ≥50% decrease in swelling of the injured ankle within 10 days of treatment) was significantly higher in the diclofenac group compared with the placebo group at all timepoints up to and including day 10/11 (V4). Diclofenac 4% spray also resulted in a significantly faster decrease in swelling of the injured ankle, which may result in earlier recovery of function and earlier return to normal daily activities. In addition, diclofenac treatment resulted in a small but statistically significant superiority over placebo in some of the secondary efficacy variables, such as spontaneous pain. Both investigators and patients were highly satisfied with the global efficacy of diclofenac spray, which was rated as ‘very good’ in >70% of judgements, although there was no statistically significant difference compared with placebo.
Towards the end of the treatment period in the current study, diclofenac spray was no longer superior to placebo in terms of some efficacy measures, including response rate and pain on active movement. The absolute differences observed in the reduction of spontaneous pain in favour of treatment, while statistically significant compared with placebo, were generally modest. To address the clinical relevance of the differences, it has to be considered that pain in ankle sprain is highly heterogeneous as it is influenced by various factors (including extent of injury) other than subjective sensitivity. Patients in the current study reported mild baseline pain levels as the study was not designed primarily to assess pain endpoints, but rather the response to treatment on the basis of reduced swelling. A mild level of pain at baseline makes differentiation from placebo quite difficult, since uncomplicated ankle sprain is a self-limiting condition that can heal without treatment within a few weeks and, accordingly, pain tends to subside along with the healing process of the injured ankle.
Any comparison of the results of the present study with other intervention studies for ankle sprain – to evaluate the effect of diclofenac spray compared with other established products – is hampered by variations in study design, inclusion criteria, treatment duration, and methods used to assess efficacy. Massey et al. 5 published a systematic review of the use of topical NSAIDs in ankle sprain injury, which mainly included studies published before 2004. A literature survey of more recent studies in ankle sprain injury treated with NSAIDs identified 10 studies published between 2004 and 2012.17,28–36 All of the more recent studies were randomized, double-blind, double-dummy, parallel-group designs.17,28–36 Half of the studies were placebo-controlled, superiority studies.17,29,30,34,35 The majority (nine studies) had pain-on-movement intensity difference from baseline (100 mm VAS) as the primary or secondary endpoint.17,28-33,35,36 Seven studies assessed this endpoint on either day 3 or 4.28–32,35,36 With the above limitations in mind, a comparison can be made on overall clinical outcome. According to the review by Massey et al, 5 the proportion of participants experiencing successful treatment (‘clinical success’ defined as 50% reduction in pain or equivalent measure, such as ‘very good’ or ‘excellent’ global assessment of treatment, or none or slight pain-on-movement measured on a categorical scale) with a topical NSAID was 65% (range 31–100%) compared with 43% (range 8–83%) with placebo. In the present study, the proportion of patients experiencing clinical success (‘very good’ patients’ global assessment of efficacy) on active treatment was 70.3%, which is in accordance with the expected clinical effect of topical NSAIDs or topical diclofenac, which was reported to be 43% (range 39–92%). 5 However, the placebo response in our study was higher than expected, with 58.8% of the participants rating the global assessment of efficacy as ‘very good’. The high placebo response might be attributed to the inclusion criteria, which, while requiring the presence of pain, did not have a threshold of pain severity. Only minor sprains were included in the present study. Such sprains would often be associated with a quick self-resolution of symptomatology, which in turn could be a factor in the heightened placebo response that we observed.
Considering the widespread use of topical NSAIDs, mainly without the guidance of a health professional, a favourable safety profile is of great concern. In this regard, diclofenac spray was well tolerated. The rate of AEs experienced with diclofenac spray was low, and all were mild-to-moderate and disappeared at the end of treatment. Only one AE was thought to be drug related (pruritus, manifesting as local of skin irritation). This finding was in line with the global tolerability reported by investigators and patients, which was similar in both treatment groups.
In conclusion, the efficacy of diclofenac 4% spray gel (three times per day for 14 ± 1 days) for the treatment of acute, uncomplicated ankle sprain following a sports or accidental injury was superior to placebo (vehicle) under randomized, double-blind, placebo-controlled conditions. Diclofenac 4% spray gel was also well tolerated. Diclofenac 4% spray can be used for the relatively rapid relief of the symptoms of acute soft tissue injuries, and may thus help to restore the patient’s mobility.
Declaration of conflicting interest
Robert Novellini is an employee of Mika Pharma GmbH. Bernd Seigfried is a consultant to Mika Pharma GmbH. All other authors declare that there are no conflicts of interest.
Footnotes
Acknowledgements
The draft manuscript was prepared and edited by a professional medical writer (Deborah Nock, DPP-Cordell Ltd; funded by Novartis Consumer Health SA, Nyon, Switzerland), with full review and approval by all authors. Grigorios Fotopoulos (Novartis Consumer Health SA, Nyon, Switzerland) provided scientific advice on preparation of the manuscript.
Funding
This study was funded by MIKA Pharma GmbH.