
Abstract
Objective
To determine the relationship between temporomandibular dysfunction syndrome (TMDS), sex and pain severity.
Methods
Data were collected prospectively from consecutive patients with TMDS. Patients were divided into four subgroups according to signs and symptoms: myofascial pain; intra-articular disorders; extra-articular disorders; degenerative disorders. Intergroup sex distribution differences were evaluated, the pain severity between the four subgroups was compared, and the rates of bruxism and inco-ordination were measured. A visual analogue scale was used to rate the pain.
Results
A total of 255 patients with TMDS were included in the study. A significantly higher rate of extra-articular disorders was found in male patients. Bruxism was found to be significantly more common in females than in males. There was no significant difference in the prevalence of inco-ordination based on sex. The overall pain score was higher in females than in males, but there was no significant difference. The pain score was significantly higher in patients in the degenerative disorders subgroup, compared with other subgroups.
Conclusions
There was no relationship between TMDS and pain and sex. Pain scores were significantly higher in the degenerative disorders subgroup, compared with other subgroups.
Introduction
Temporomandibular dysfunction syndrome (TMDS) includes various clinical conditions that involve the masticatory muscles or temporomandibular joints and their associated structures. 1 Typical signs and symptoms of TMDS are pain, joint sounds, limited mouth opening, chewing disability and mandibular deviation; signs and symptoms may exist alone or in combination. 2 The aetiology of TMDS is multifactorial and is related to dental and medical conditions.2,3 Factors that contribute to TMDS are thought to be anatomical, genetic, trauma, pathophysiological and psychosocial. 4 The purpose of this study was to determine the relationship between TMDS, sex and pain severity.
Patients and methods
Patient population
This prospective study enrolled consecutive patients seeking treatment for TMDS at the Department of Physical Medicine and Rehabilitation, Medical Faculty, Istanbul University, Istanbul, Turkey between February 2012 and February 2013. Patients were initially questioned using a questionnaire based on the Research Diagnostic Criteria for TMDS. 5 The following items were included in the questionnaire: age; sex; social status; general health; antidepressant use; dental status (missing/filled teeth, fixed/removable prosthetic restorations); occlusion type; limited mouth opening; temporomandibular joint sounds; and parafunctions (bruxism, clenching). Patients with fibromyalgia, trigeminal neuralgia, burning mouth syndrome, atypical facial pain, migraine, atypical odontalgia and cervical or neuropathic pain, as well as those with a history of TMDS treatment, were excluded from the study.
The study was approved by the Ethics Committee of the Medical School, Dicle University, Diyarbakir, Turkey. All patients included in the study gave verbal informed consent.
Pain assessment
After demographic information was obtained from each patient, the extent of temporomandibular joint pain was evaluated with a visual analogue scale (VAS), where a score of 0 represented no pain and 10 represented the worst possible pain. Patients were divided into four subgroups, based on the VAS score and their signs and symptoms of TMDS: patients with a taut band in the muscles and painful trigger points (myofascial pain group, G1); patients with joint tenderness, clicking sounds, or crepitation, along with decreasing joint movement (intra-articular disorders group, G2); patients with malocclusion and joint hypermobility (extra-articular disorders group, G3); patients with painful joint degeneration (degenerative disorders group, G4).
Statistical analyses
All statistical analyses were performed using the SPSS® statistical software package, version 16.0 (SPSS Inc., Chicago, IL, USA) for Windows®. Independent-samples t-test was used to compare the pain severity between the four subgroups; χ2-test was used to compare the sex distribution between the groups and to compare rates of bruxism and inco-ordination between both sexes. A P-value < 0.05 was considered statistically significant.
Results
Comparison of sex distribution differences in four groups of patients with temporomandibular dysfunction syndrome, categorized according to the signs and symptoms experienced (n = 255).

Data presented as number of patients (% of the same sex).
χ2-test.
G1, myofascial pain; G2, intra-articular disorders; G3, extra-articular disorders; G4, degenerative disorders; NS, not statistically significant (P ≥ 0.05).
Comparison of the number of patients with temporomandibular dysfunction syndrome who experienced bruxism and inco-ordination, stratified according to sex (n = 255).
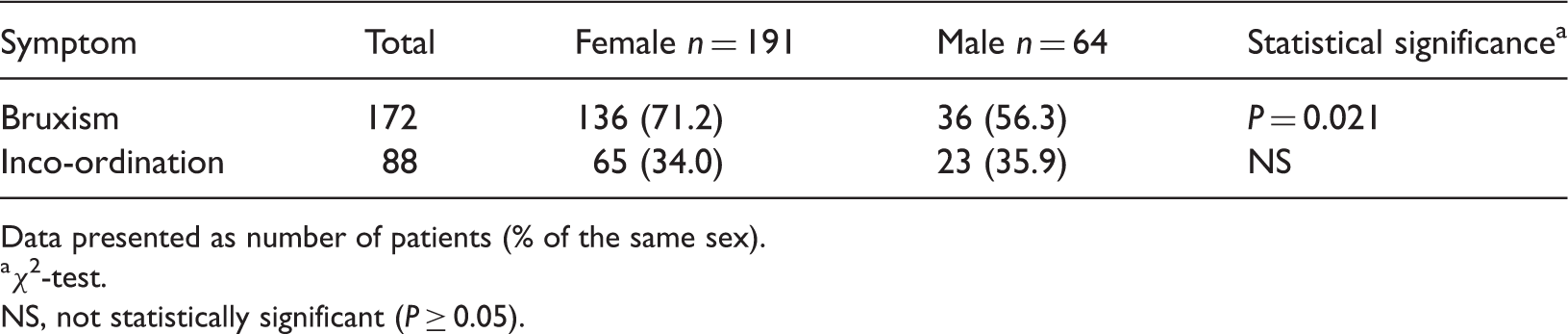
Data presented as number of patients (% of the same sex).
χ2-test.
NS, not statistically significant (P ≥ 0.05).
Mean visual analogue scale (VAS) scores for the four groups of patients with temporomandibular dysfunction syndrome, categorized according to the signs and symptoms experienced (n = 255).

Data presented as mean ± SD.
P < 0.001 compared with G4; independent-samples t-test.
P = 0.02 compared with G4; independent-samples t-test.
G1, myofascial pain; G2, intra-articular disorders; G3, extra-articular disorders; G4, degenerative disorders.
A VAS score of 0 represented no pain; a VAS score of and 10 represented worst possible pain.
Discussion
Temporomandibular dysfunction syndrome is a chronic disorder. In general, epidemiological studies have documented a greater frequency and severity of TMDS in females than in males.5,6 Fillingim et al. 7 reported a higher ratio of female patients (89%), as did another prevalence study in Turkey. 8 Although sex differences have been explained by behavioural, psychosocial, hormonal and constitutional factors, no conclusions have been drawn.5,9 In the present study, females were found to have a higher risk of TMDS (3 : 1) than males. Manfredini et al. 6 made similar observations in a study of 433 patients, in whom the female:male risk ratio was 2.6 : 1.
Psychosocial factors can be a cause of TMDS. 10 In the literature, the most common diagnosis of TMDS is myofascial pain syndrome, which is associated with psychosocial factors. 11 A high incidence of myofascial pain was also found in the current study.
The incidence of TMDS pain in females has been studied widely. 12 Females were reported to have approximately three times the risk of myofascial pain than males in a series of 83 patients. 13 An investigation of 71 patients found that chewing significantly increased pain in patients with a history of chronic masticator muscle pain, and also in females with no such history. 14 According to our current results, females had a higher mean VAS pain score than males but there was no significant difference in pain score, between the two sexes.
Reissmann et al. 15 reported no relationship between VAS scores and TMDS subgroups. In contrast, the mean VAS pain score in G4 was significantly higher than in the other three subgroups in our current study.
Bruxism has been reported to cause hypermobility of the mandibular muscles, leading to TMDS. 16 The association between bruxism and muscle pain can be ascribed to either muscle fibre damage 17 or a reduction in the blood supply. 18 Indeed, it has been shown that perfusion of the masseter muscle is substantially impaired in individuals performing voluntary isometric contractions. 19 In our current study, 172 (67.5%) patients had bruxism. While a significantly higher rate of bruxism was observed in females, a significantly higher rate of extra-articular disorders was observed in males.
In conclusion, in the present study, a higher rate of TMDS was found in females than in males. There was no relationship between pain and sex; however, the pain score was significantly higher in patients in the degenerative disorders subgroup compared with the other three subgroups. In addition, there was a significantly higher rate of bruxism in females than in males, and a significantly higher rate of extra-articular disorders in males than in females.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.