
Abstract
Objective
To examine factors affecting systolic blood pressure (SBP) variability during a single clinic visit, in treated hypertensive patients.
Methods
Hypertensive patients were recruited to this observational study. Blood pressure was measured using an automated blood pressure monitor when each patient arrived at the outpatient clinic and again when they saw the physician. Mean SBP and SBP variability during a single clinic visit were calculated. The cardio–ankle vascular index (CAVI), as a marker of arterial stiffness, was also measured.
Results
A total of 57 treated hypertensive patients (mean age 71 years) were included in the study. The mean SBP was positively correlated with age (r = 0.457), while SBP variability was positively correlated with age (r = 0.383), CAVI (r = 0.330), and glycosylated haemoglobin (r = 0.345) and triglyceride levels (r = 0.299).
Conclusion
Variability in SBP during a single clinic visit showed better correlations with arterial stiffness and risk factors for atherosclerosis than did mean SBP. Large SBP variability during a single clinic visit may reflect progression of atherosclerosis, in treated hypertensive patients.
Keywords
Introduction
Arterial stiffness is attracting attention as an index for assessing atherosclerosis, as it is an independent predictor of cardiovascular mortality, fatal or nonfatal coronary events, and fatal strokes in patients with hypertension.1,2 The cardio–ankle vascular index (CAVI) is a new index of arterial stiffness. 3 As the most conspicuous feature of the CAVI is a lack of dependence on blood pressure, this index has recently become utilized for assessing arterial stiffness in clinical settings. 4 The CAVI is high in ageing patients and in those with atherosclerotic diseases such as coronary artery disease, 5 carotid atherosclerosis, 6 and chronic kidney disease; 7 the index is also related to many coronary risk factors such as hypertension, 8 diabetes, 9 dyslipidaemia and smoking.9,10 Furthermore, the CAVI decreases with control of diabetes 11 and hypertension, 12 as well as abstention from smoking. 10 These factors suggest that the CAVI is a surrogate marker for atherosclerosis.
Visit-to-visit variability in systolic blood pressure (SBP) for two or more clinic visits has been demonstrated to be a strong predictor of stroke, independent of the mean value of SBP.13,14 However, visit-to-visit variability is not always convenient to measure. During a single clinic visit, multiple measurements of blood pressure in the physician′s office may be subject to the ‘white-coat effect’,15–17 depending on whether medical personnel are present. However, the value of single-visit SBP variability has not been studied: there are few data about the relationships between such data and arterial stiffness, in patients with hypertension.
We hypothesized that SBP variability during a single clinic visit may reflect arterial stiffness as assessed by the CAVI in a better way than the mean SBP value during a single clinic visit. In the present study, the associations between SBP variability and arterial stiffness in treated hypertensive patients were examined during a single clinic visit, and their association was compared with that of the mean SBP.
Patients and methods
Subjects and study protocol
This observational study was conducted between April 2011 and April 2012. This study included consecutive patients who had been diagnosed with hypertension at the Department of Integrated Medicine, Kagawa University Hospital (Kagawa, Japan) and who had regularly visited the outpatient clinic. Hypertension was defined as SBP ≥ 140 mmHg and/or diastolic blood pressure (DBP) ≥ 90 mmHg. All patients were treated with at least one antihypertensive drug, with no changes to the antihypertensive drug regimen being made for ≥ 1 year prior to their enrolment in this study, or during the 1-year observation period when blood pressure data were obtained. Patients with a history of heart failure or obvious heart disease were excluded. None of the patients had a history of atherosclerotic cardiovascular disease or stroke. Patients with renal dysfunction, with serum creatinine levels ≥ 1.5 mg/dl at the time of analysis, were excluded from the present study.
Blood pressure was measured at the outpatient clinic every 1–2 months during the 1-year observation period for each patient, which started in April 2011. At the end of the 1-year observation period, in April 2012, measurement of the CAVI was performed in each patient (to assess arterial stiffness) and blood samples were taken in the morning after an 8-h overnight fast. Blood was collected into tubes containing 1.8 mg/ml ethylenediamine tetra-acetic acid and was analysed immediately (serum and plasma analyses), using standard laboratory techniques. Plasma concentrations of total cholesterol, high-density lipoprotein cholesterol (HDL–C), triglycerides, glycosylated haemoglobin (HbA1c), uric acid, haemoglobin, and high-sensitivity C-reactive protein were measured. Serum creatinine levels were also measured.
The study protocol was approved by the Ethics Committee of Kagawa University (reference number: 22-39). Written informed consent was obtained from all participants.
Blood pressure measurement
All patients measured their own blood pressure when they arrived at the outpatient clinic and again when they saw the physician. When they arrived at the clinic, they measured their blood pressure in the upper right arm, in the sitting position, using an automated oscillometric sphygmomanometer (HEM-1040 OMRON Spotarm™ blood pressure monitor; Omron, Kyoto, Japan) without a human observer. Then, when they saw the physician, they again measured their blood pressure in the supine position using the same automated oscillometric sphygmomanometer, but this time with a human observer. The differences between the SBPs of the two measurements were calculated to assess SBP variability during a single clinic visit. The mean of the two SBP measurements was also calculated. These SBP measurements were performed at the outpatient clinic every 1–2 months during a 1-year period, and the mean of the data was calculated for each patient.
Assessment of arterial stiffness by CAVI
The CAVI was measured using an automatic vascular screening system (VaSera VS-1000; Fukuda Denshi, Tokyo, Japan), with the patient resting in a supine position. Pulse wave velocity (PWV) was obtained by dividing the vascular length by the time it took for the pulse wave to propagate from the aortic valve to the ankle. SBP and DBP were measured at the brachial artery. The formula used to calculate the CAVI was as follows: CAVI = a[(2ρ/ΔP)×ln (SBP/DBP) PWV 2 ]+b, where ΔP is SBP – DBP, ρ is blood density, and a and b are scale conversion constants to match aortic PWV. The principle underlying the CAVI has been described previously. 3 The equation is derived from Bramwell-Hill’s equation and the stiffness parameter ß, and the CAVI was adjusted for blood pressure, based on the stiffness parameter ß. Therefore, the CAVI reflects the stiffness of the aorta, femoral artery and tibial artery as a whole; theoretically, it is not affected by blood pressure. All of these measurements and calculations were performed on a VaSera™ VS-1000 automatic vascular screening system. For each patient, electrocardiogram electrodes were placed on both wrists, a microphone for detecting heart sounds was placed on the sternum, and cuffs were wrapped around both arms and both ankles. After automatic measurements, values of the right and left CAVI were calculated. The mean values of the right and left CAVI scores were then used for analysis.
Statistical analyses
Data are expressed as mean ± SD. Statistical analyses were performed using the SPSS® statistical package, version 18.0 (SPSS Inc., Chicago, IL, USA) for Windows®. A paired t-test was used to compare the mean SBP values obtained from the two measurement time points, i.e. when patients arrived at the clinic and when they saw the physician. Correlations between SBP parameters and other variables were assessed by univariate analyses. Subsequently, stepwise multiple regression analysis was performed to select factors independently associated with SBP parameters. A P-value < 0.05 was considered to be statistically significant.
Results
Clinical and demographic characteristics of patients with hypertension (n = 57), included in a study examining factors affecting systolic blood pressure variabilit.

Data presented as mean ± SD or n (%) of patients.
Demographic measurements, disease history and smoking data were obtained at baseline (April 2011); blood analyses and CAVI data were obtained at the end of the study period (April 2012).
Means were calculated from composites of SBP data for individuals over the 1-year study period, and for composites of data on CAVI for individuals in single examinations undertaken at April 2012.
BMI, body mass index; ARB, angiotensin II receptor blocker; ACEI, angiotensin-converting enzyme inhibitor; CCB, calcium channel blocker; HDL–C, high-density lipoprotein cholesterol; HbA1c, glycosylated haemoglobin; hsCRP, high-sensitivity C-reactive protein; CAVI, cardio–ankle vascular index; SBP, systolic blood pressure.
Figure 1 shows the changes in SBP for all patients during a single clinic visit. Compared with the SBP when patients arrived at the clinic, the SBP taken in the physician’s presence increased in 32 out of 57 patients (56%), but decreased in 25 out of 57 patients (44%). There was no significant overall difference between the mean ± SD SBP when patients arrived at the clinic (125 ± 13 mmHg) and the level when they saw the physician (127 ± 11 mmHg). The mean ± SD individual difference between the two SBP measurements (i.e. the SBP variability) was 11 ± 4 mmHg.
Changes in systolic blood pressure (SBP) for all treated hypertensive patients during a single clinic visit (n = 57). There was no significant overall difference between the mean ± SD SBP when patients arrived at the clinic (125 ± 13 mmHg) and the level when they saw the physician (127 ± 11 mmHg). Central black horizontal lines show the mean value for each time point; extremities of the vertical lines show the SD.
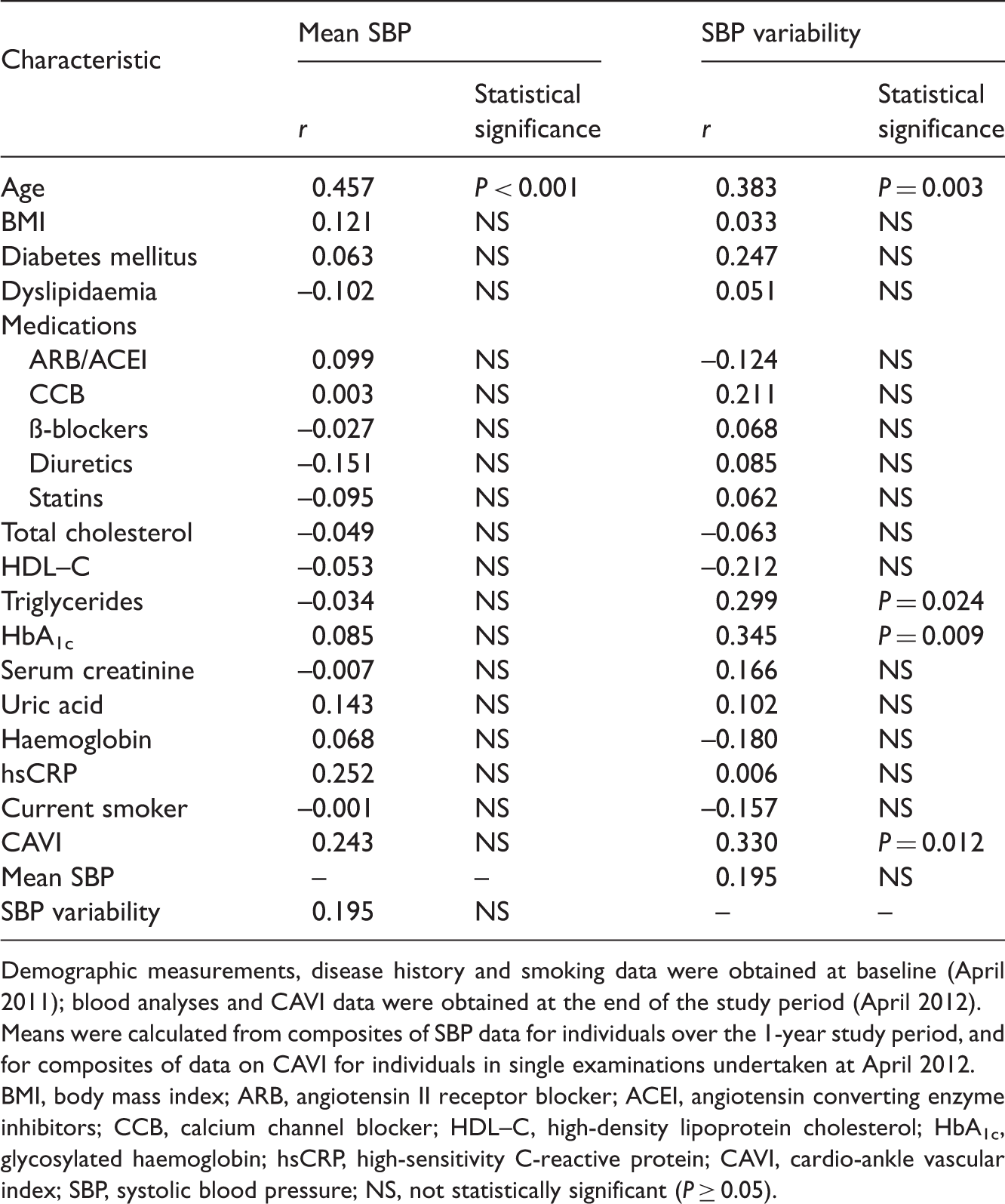
Linear regression analyses were performed to examine the correlations between the mean SBP and SBP variability during a single clinic visit and other clinical characteristics (Table 2). There was no significant correlation between the mean SBP and SBP variability during a single clinic visit. The mean SBP showed a significant positive correlation with age (r = 0.457, P < 0.001). SBP variability showed significant positive correlations with age (r = 0.383, P = 0.003), triglycerides (r = 0.299, P = 0.024), HbA1c (r = 0.345, P = 0.009), and CAVI (r = 0.330, P = 0.012) (Figure 2).
Relationships between cardio–ankle vascular index (CAVI), mean systolic blood pressure (SBP) and SBP variability during a single clinic visit in treated hypertensive patients (n = 57). Although the CAVI was not correlated with mean SBP (r = 0.243, P ≥ 0.05), it was positively correlated with SBP variability during a single clinic visit (r = 0.330, P = 0.012); NS, no statistically significant differences observed. Linear regression analyses of the relationship between the mean systolic blood pressure (SBP) values and SBP variability during a single clinic visit, and other clinical characteristic. Demographic measurements, disease history and smoking data were obtained at baseline (April 2011); blood analyses and CAVI data were obtained at the end of the study period (April 2012). Means were calculated from composites of SBP data for individuals over the 1-year study period, and for composites of data on CAVI for individuals in single examinations undertaken at April 2012. BMI, body mass index; ARB, angiotensin II receptor blocker; ACEI, angiotensin converting enzyme inhibitors; CCB, calcium channel blocker; HDL–C, high-density lipoprotein cholesterol; HbA1c, glycosylated haemoglobin; hsCRP, high-sensitivity C-reactive protein; CAVI, cardio-ankle vascular index; SBP, systolic blood pressure; NS, not statistically significant (P ≥ 0.05).
Stepwise multiple regression analysis of mean systolic blood pressure during a single clinic visit and significantly associated characteristic.

Statistical significance of this model of multiple regression analysis for predicting mean systolic blood pressure during a single clinic visit.
Stepwise multiple regression analysis of systolic blood pressure variability during a single clinic visit and significantly associated characteristic.

Statistical significance of this model of multiple regression analysis for predicting systolic blood pressure variability during a single clinic visit.
HbA1c, glycosylated haemoglobin.
Discussion
The present study sought to elucidate the factors influencing the mean SBP and SBP variability for two blood pressure measurements during a single clinic visit, in treated hypertensive patients. The present study demonstrated that: (i) a similar proportion of patients experienced an increased SBP as the proportion that experienced a decreased SBP in the presence of a physician (32 patients [56%] versus 25 patients [44%]); (ii) there was no significant overall difference between the mean SBP measurement upon arrival and that when patients saw the physician; (iii) an SBP variability of 11 ± 4 mmHg between the two measurements during a single clinic visit was observed; (iv) the mean SBP during the single clinic visit (mean of two measurements) was positively correlated with age, while SBP variability was positively correlated with age, triglycerides, HbA1c, and CAVI, which are atherosclerosis-related parameters; (v) only age was independently associated with the mean SBP during a single clinic visit, whereas age and HbA1c, which are atherosclerosis-related parameters, were independently associated with SBP variability during a single clinic visit.
In the present study, SBP variability during a single clinic visit did not reflect a ‘white-coat effect’ because while SBP was higher in the physician’s presence in 56% of patients (32/57), it was lower in 44% (25/57). All patients had to walk for some distance before they arrived at the outpatient clinic and measured their blood pressure. Therefore, they were exposed to different potential stressors at both measurement times. This may explain why the overall patient group (n = 57) did not show a statistically significant difference of the SBP changes during a single clinic visit, in the present study (Figure 1).
Other studies demonstrated an association between systemic atherosclerotic change and 24-h18,19 or visit-to-visit 20 blood pressure variability. However, there are few data about the relationship between atherosclerosis and SBP differences between two measurements during a single clinic visit. To our knowledge, this is the first study to present such data. The most striking finding from this current study was that SBP variability during a single clinic visit showed better correlations with arterial stiffness, as assessed by the CAVI, and risk factors for atherosclerosis, such as triglycerides and HbA1c, than did the mean SBP (Table 2). Therefore, considerable SBP variability during a single clinic visit may reflect the progression of atherosclerosis in patients with treated hypertension. Clinical examination and treatment of atherosclerosis-related diseases may be needed in patients with large single-visit SBP variability. Recently, visit-to-visit variability in SBP has been shown to be a predictor of stroke.13,14 The present study focused on the associations between arterial stiffness and SBP variability and mean SBP during a single clinic visit. We found that SBP variability during a single clinic visit showed better correlations with arterial stiffness (as assessed by the CAVI) than did mean SBP in patients with treated hypertension. This finding suggests that attention should be paid to the timing of SBP measurement at each clinic visit, because values may easily change according to different stressors in patients with increased arterial stiffness. For example, determination of the timing of SBP measurement during each clinic visit may be needed to assess the visit-to-visit variability in SBP.
In the present study, age and HbA1c were identified as independent determinants of SBP variability during a single clinic visit (Table 4). This is understandable because age is an important risk factor for atherosclerosis.21,22 Although the CAVI is a parameter of arterial stiffness, which reflects one important factor of atherosclerosis, this index was not selected as an independent determinant of SBP variability in this current study. It is well known that the CAVI increases with advancing age.3,4 This may be why the CAVI was eliminated during stepwise multiple regression analyses. However, HbA1c as an independent determinant of the SBP variability during a single clinic visit may suggest that single-visit SBP variability in patients with glucose intolerance or diabetes may be an indicator of the progression of atherosclerosis. 23
In conclusion, SBP variability during a single clinic visit showed better correlations with arterial stiffness and risk factors for atherosclerosis than did mean SBP. Large SBP variability during a single clinic visit may reflect the progression of atherosclerosis, in patients with hypertension.
Footnotes
Declaration of conflicting interest
The Authors declare that there are no conflicts of interest.
Funding
This study was supported in part by a Grant-in-Aid to Shoichi Senda (Scientific Research [B] No. 23300190) for Scientific Research from the Ministry of Education, Culture, Sports, Science and Technology, Japan and the Japan Society for the Promotion of Science.