
Abstract
Objectives
To determine the views of Slovenian family physicians on medically unexplained symptoms (MUS) and learn more about potential types of treatment for such patients.
Methods
Five focus groups, comprising 24 family medicine physicians (FMPs) from two Slovenian University centres, were convened. Conversations were led towards the research objectives by professionally trained researchers and followed a preliminarily established protocol. Qualitative content analysis of audio and transcripts of the discussions was performed using ATLAS.ti software to establish categories (‘codes’) relevant to issues regarding MUS.
Results
Slovenian FMPs emphasized the importance of good communication and trust between physicians and patients with MUS. Systemic barriers to effective management of MUS arising from the Slovenian health system were highlighted. FMPs stressed the need for more education in the recognition and treatment of MUS in primary care. From the discussions, 64 codes comprising broader research fields of MUS were developed, then grouped into a further eight categories: communication; doctor–patient relationship; causes of MUS; patient characteristics; physician characteristics; courses of action so far; positive relationship with patients; proposals for treatment.
Conclusions
The results are valuable in terms of investigating the treatment of patients with MUS in Slovenia, thereby opening new avenues of research on the subject of MUS.
Keywords
Introduction
Nearly 20% of all patients visiting family practices suffer from physical symptoms for which, after numerous examinations, no clear organic reason can be found; collectively this is known as ‘medically unexplained symptoms’ (MUS).1,2 Many physicians are often able only to manage their patients' somatic complaints and in doing so ignore the psychosocial context of their illnesses.3,4 In the management of patients with MUS, family medical physicians (FMPs) are often confronted with the patients' own understandings of the disease,5,6 their somatic and psychological problems, 7 and the need for FMPs to offer their patients emotional support and an explanation for their symptoms. 8
In the majority of cases, physicians express negative and dismissive attitudes towards such patients and their problems,9,10 which are worsened by poor communication and difficulty in explaining the patients' symptoms.11,12 Most physicians classify patients with MUS as frequent attenders, but not necessarily as difficult patients. 13 Good communication between the physician and patient is the basis for a successful doctor–patient relationship, which is demonstrated by effective management of the symptoms and satisfaction of patients with MUS. 14
Research indicates that potential causes of patients' problems include chronic illness from childhood, abuse in childhood, stress situations and a low level of family support. 15 Such issues are compounded by psychological problems and stressful social situations, social and financial problems, problems at work, changes in everyday routine, 5 as well as factors of an unhealthy lifestyle (such as insufficient exercise, weight increase and/or social isolation, depression and loss of self-confidence). 16
The healthcare system in Slovenia has undergone substantial change since 1992. The objectives of these changes were primarily economic rather than medical, since the level of services rendered has long been fairly high and there were limited needs for improvement. 17 In practice, there are no firm guidelines that FMPs can follow with patients who have MUS.11,18 There is some evidence that the treatment of MUS depends largely on four basic steps, 19 namely: showing sensitivity to patients and understanding of their problems; broadening communication between the patient and physician, beyond the perspective of the patient's problems; establishing a correlation between the somatic and psychosocial problems of patients; agreement on additional rational examinations and further treatment.
The present study determined the views of Slovenian FMPs on MUS, with the aim of discovering more about potential management strategies for patients with MUS. The study plan included four broad research fields of MUS, namely: views of FMPs on the possible causes of MUS; exploration of the relationship between patients with MUS and their physicians; courses of action so far; potential proposals for appropriate monitoring and treatment.
Methods
Study design
This was a qualitative study. Five focus groups (FGs) were formed, comprising 24 FMPs from family medicine departments of Ljubljana and Maribor Universities, Slovenia. The FMPs were all engaged in everyday practice, working in their own clinics in both urban and rural environments, and in public and private services. A purposive sample (i.e. a nonrepresentative subset of a larger population, constructed to serve a specific need or purpose) was used, representing the variation in physicians’ ages and professional experiences, and their engagement in scientific research work (i.e. the academic sphere). The FGs were conducted between July and September 2011, and the study was approved by the Slovenian National Medical Ethics Committee (reference number: 45/05/11bis).
Discussion protocol used as a framework to guide focus groups of family physicians in a qualitative study of medically unexplained symptoms (MUS).

Audio recordings and transcripts were made for each FG separately, as one FG represented one unit of analysis. FGs were conducted in Slovene and coded in ATLAS.ti (a software package that supports the analysis of qualitative data: an English version of ATLAS.ti 7 [nonwestern], version 7.0.73, was used [Scientific Software Development GmbH, Berlin, Germany]). Initially there was no preliminary translation into English. The correctness of transcripts made from audio recordings was checked independently (by V.I. and Z.K.K.), after which they confirmed their reviews by consensus. Transcripts were entered by V.I. into the English version of ATLAS.ti.
Study analyses
Due to insufficient knowledge about all the factors affecting the Slovenian FMPs' monitoring of patients with MUS, the qualitative analysis method was employed. 20 This method used the FG method, in combination with the preliminarily modelled conversation protocol.21,22
Transcripts were analysed using established methods for qualitative content analysis.23,24 The coding process was carried out using ATLAS.ti, during which relevant categories (which were called ‘codes’) were established; categories could then be described qualitatively.24,25
In order to ensure compliance within the scope of a qualitative research strategy, 26 processing and interpretation were based on the coding instructions 25 for classifying raw data from transcripts of audio recordings of FGs. In this manner, objective, theoretically grounded, measurable categories were obtained; these were used to substantiate the valid arguments regarding the issues of MUS from the perspective of FMPs, as well as to highlight some specific experiences of FMPs in Slovenia.
Results
Characteristics of Slovenian family medical physicians (FMPs) who participated in focus groups (FGs), convened to determine their views on medically unexplained symptoms.
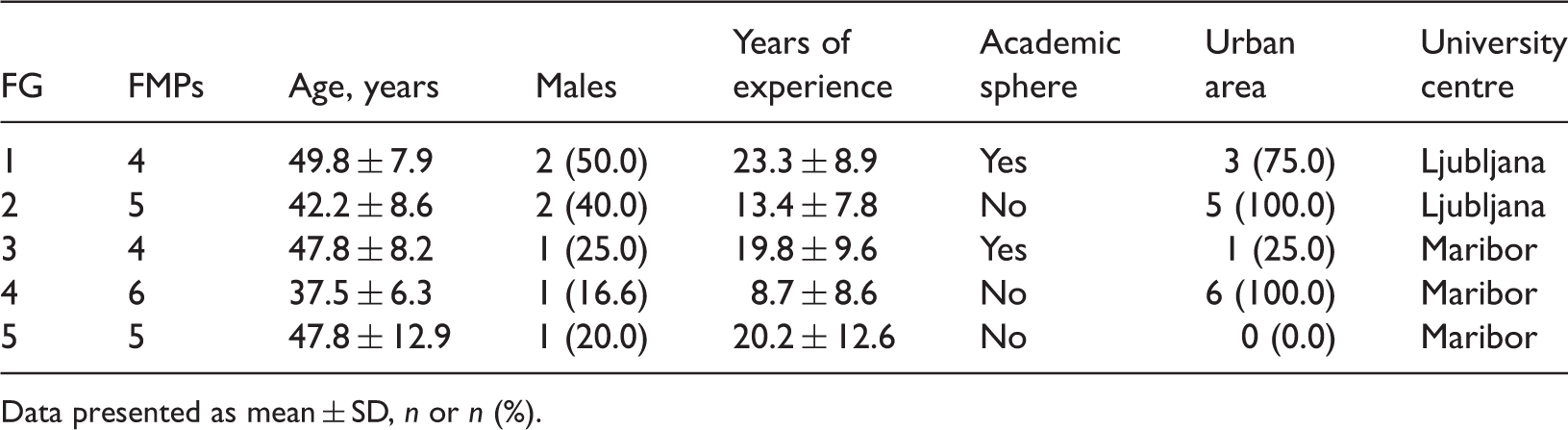
Data presented as mean ± SD, n or n (%).
In the coding process, 64 codes were developed that included broader research fields of MUS. The codes were grouped into eight theoretically grounded, logical categories in accordance with the elaborated theoretical concept:5,9,21 communication; doctor–patient relationship; causes of MUS; patient characteristics; physician characteristics; courses of action so far; positive relationship with patients; proposals for treatment. These are discussed in more detail below.
Category 1: Communication
There were practically no differences between the FGs with regard to the issue of communication. All participants emphasized the importance of communication between the physician and the patient, and that good communication represented a key element in the treatment strategy. FMPs highlighted the patients' difficulties in communicating their problems. Some also found it important that, during this process, the physician should try to tell the patient what is not wrong with them.
FMP5 (male, 10 years' experience): ‘Many consultations with the patient are done on the basis of mutual trust. Patients like the feeling that you took their symptoms seriously and leave open the way to come back to you if the symptoms change.’[FG2]
FMP8 (female, 16 years' experience): ‘Yes, I would also say here, if you succeed in establishing such a relationship, that the patient trusts you and that you take him seriously, then it seems to me that it is easier to communicate.’ [FG2]
Category 2: Doctor–patient relationship
This category consisted of 10 of the broader codes, in which the physicians tried to define their relationships with the patients with MUS. Besides the tiring and negative relationship with those who have MUS, FMPs stressed the importance of a year-long monitoring and treatment schedule for such patients.
FMP18 (female, 5 years’ experience): ‘I used a trick on two such patients. Just to make them stop coming to my clinic without an appointment. I scheduled them once every 3 weeks, and when 3 weeks had passed he came and I examined him thoroughly. After another 3 weeks I examined him again, and again after another 3 weeks. But then he appeared once without an appointment. I “penalized” him by prolonging his appointment to once every 4 weeks.’ [FG4]
FMP24 (female, 17 years' experience): ‘We can always act like we are almost equal, like partners, equal partners with a common problem, which we will or will not solve. But at least we try to solve it together.’ [FG5]
The FMPs also highlighted cases of poor relationships, or relationships where there is no alliance between the physician and the patient; in particular, with respect to the functioning of the Slovenian healthcare system. Here, the FMPs highlighted systemic barriers for the fulfilment of patients’ wishes (limitations of national health insurance, lack of resources, etc). FMPs were also less satisfied with the average time per patient consultation (the mean consultation time in Slovenia is ∼7 min per patient 27 ).
Considering negative relationships with patients, FMPs expressed problems in the sense of how patients with MUS make their work more difficult by tiring them out and causing some irritation.
Some FMPs (in the FG3 and FG5 sessions) placed particular emphasis on the dependency of patients towards their physician.
FMP12 (female, 17 years’ experience): ‘Then, a certain position is established, which could be referred to as dependency. It is either the dependent position of the physician towards the patient, because such a patient makes him or her feel good in the sense of: “Look how he likes me”; “He comes to me”; “Only I can help him”; or “Only I can fulfil his expectations”. And the same holds for the patient: “No, thank God, she will be responsible for everything”; “She will do everything herself”; “You are the best physician ever, only you know how to explain things to me”. In short, yes, there is one danger.’ [FG3]
Category 3: Causes of MUS
Considering this category, the physicians in all FGs emphasized the diversity of patients and that no rule can be laid down regarding their age, sex or social environment. FMPs did not raise any issues in connection with patient demographics/characteristics (such as age and sex) as being possible causes of MUS. Participants in the first FGs mentioned family susceptibility to MUS.
FMP1 (female, 30 years’ experience): ‘Basically, I think that the pattern repeats itself in family after family. For instance, first you see a mother carrying a thick medical record and undergoing numerous examinations, and then you see that her daughter reacts in the same manner; she wants us to deal with every little problem that might affect her health.’ [FG1]
Category 4: Patient characteristics
Considering the patient characteristics category, participants in all FGs emphasized that patients with MUS differed from one another, and request different treatment.
FMP23 (male, 37 years’ experience): “Those who want to undergo examinations are a bit annoying, because they always find a new examination that they want to take. On the contrary, there are also such patients who come and leave after just a short conversation, feeling good and healthy again. Such patients may demand more of the physician's time, as they want to explain the events taking place at home, etc., but they always leave the clinic fully satisfied. We see such patients every 14 days or once a month.” [FG5]
Category 5: Physician characteristics
The participants in all FGs stressed the importance of the physicians' experience; knowledge acquired through formal medical school education was not considered sufficient for the successful treatment of MUS.
FMP3 (male, 30 years’ experience): ‘When we complete our education at the Faculty we think we are almighty and that we can cure anything, and then you come to the clinic and for the first time you realise that you are not capable of doing so. You realise that patients with MUS are the sort of patients who come to you with symptoms and problems, the answer to which cannot be found in any of the textbooks. And then we have a problem, don't we? Such patients have really broadened my horizons, horizons about people in general, their problems, diseases, health. In a way, I am grateful to them for doing so, because they have made me greater as a person, more tolerant, more acceptable to changes. I profited enormously from working with these people, perhaps even more than from some well-controlled hypertensives.’ [FG1]
The FMPs drew attention to deficiencies in their work (or in the work of their colleagues), such as negative personal characteristics, creation of patients with MUS, and so on.
Category 6: Courses of action so far
Participants in all FGs highlighted their practices and different experiences in how they have approached management of patients with MUS. The importance of a correct interpretation of the patient's problems was highlighted. According to some participants’ opinions, the patient should also participate actively in this process, as by doing so the patient can deepen his or her relationship with the physician. They mentioned a strategy, according to which the patient eventually accepts his or her symptoms, and the importance of active participation of patients in the treatment process.
FMP2 (male, 11 years’ experience): ‘There is one patient, a highly operative police officer, who is dealing with a severe spasmodic pain in the abdominal area and has already learned everything there is to know about diagnostics. He said: “You will not be able to cure me anyway. It won't happen, I live with it. When I am in pain, I take Spasmex® or something stronger. There are times when the pain gets stronger, worse, and it has been like that for a couple of years now. I accepted my condition; it is what it is”.’ [FG1]
Category 7: A positive relationship with patients
Three codes were established for this category, which emphasized the importance of comprehensive treatment strategies for patients, susceptibility to their problems and trust between the physician and patient. The importance of a comprehensive treatment strategy for patients with MUS was recognized in all FGs. Susceptibility to patients' problems is the element of a positive attitude, which was seen as important in four FGs. The physicians often act as counsellors for their patients' problems, which have developed as a result of the patients' interactions within the broader social environment.
FMP3 (male, 30 years’ experience): ‘Although neither I nor she know where the pain comes from and what is wrong with her, we trust each other. She believes me and is no more difficult than any other patient. […] Not believing the patient is the first capital mistake. […] To place some sort of trust in him so that he can come at any time and you will take him seriously, that you will always help him. That is a fantastic advantage, because we are there 24 h a day. We are there practically every day and if the patient has this assurance that he can come in the next day after the condition reappears, it means a great deal to him.’ [FG1]
Category 8: Proposal for treatment
This category consisted of eight codes representing a proposal for the successful treatment of MUS in future. In this case, ‘education’ is included as an important subcategory, as the participating FMPs expressed the need for additional interactive education in the form of workshops (including exchange of experience, physician–patient communication and communication skills), knowledge transfer in the form of lectures (given by experts), reading professional literature, and also in organizing consultations on the subjects of legal and formal situations that might occur during the treatment of patients with MUS (systemic barriers, criminal liability, and so on).
The FMPs highlighted the importance of continuous record keeping and consultations with their colleagues (in particular, fellow FMPs) and clinical specialists, in the treatment of patients with MUS.
FMP16 (female, 5 years’ experience): ‘Perhaps a clinical psychologist is one specialist that I would want to have around, mainly because he could run certain tests based on the knowledge that I don't have but would like to see present in the family medicine clinic’‘FG4] FMP17 (male, 8 years’ experience) “A family counsellor, yes. However, we could still use a specialist or two, who would be capable of higher empathy, more motivation for handling such matters.” [FG4]
Discussion
The Slovenian FMPs brought together in these FGs recognized the importance of the treatment of patients with MUS. As the demographic differences between the FMPs in terms of sex, age and working environment did not affect the experiences, description of causes, or formulation of proposals for the treatment of MUS, the potential differences between the participants’ answers can arise only from their rich experience (years of service) and their participation in the academic sphere. This enables this research to be compared with other similar research, conducted in other countries.22,28
The first category (Communication) was universally found to be important. Good communication between the physician and patient (and vice versa) represents an important element in FMP strategy and is necessary for successful treatment of MUS.7,29
The third category (Causes of MUS) represents the aggregate of the different experiences of participating physicians and their views on the potential causes of MUS. Potential causes of MUS include somatic, psychosomatic and psychological problems, some characteristics of patients (being too demanding, mistrustful or lonely, for example), and their previous experiences and traumatic life events. Such causes also comprise various factors arising from the patient's interaction with the environment (stress, or problems within the family or at work, for example).30,31 The FMPs believed that, in some patients, MUS is a result of a family pattern – that the condition appears to run in the family – which also explains their frequent visits to the clinic
The fourth and fifth categories (Patient characteristics; Physician characteristics) can be discussed together. These FGs indicated that experiences of the FMPs were of the utmost importance in recognizing and managing MUS. This conclusion is in agreement with other opinion leaders’ views. 32
The sixth category refers directly to the third objective of the research, the FMPs' experiences with the ‘Courses of action so far’
The categories ‘Doctor–patient relationship’, ‘A positive relationship with patients' and ‘Proposals for successful treatment’ can be merged into one. In this study, FMPs acknowledged that dealing with patients with MUS was often stressful and tiring, which has been reported by other groups of general practitioners. 35 The most frequent ethical dilemmas that occur arise from limited financial resources and situations where patients want to take advantage of healthcare services; such dilemmas can be compared with those reported for patients who do not have MUS. 36 FMPs placed confidence in the physician–patient relationship based on alliance, and understood the importance of being susceptible to their problems, which often exceed the framework of health issues.37,38
From the discussions on the subcategory ‘Education’, the FMPs in this group were very interested in further education in the management of MUS. They advocated organizing different workshops and lectures, covering particular in areas of communication and the legal or systemic issues that can arise with patients with MUS.
The main limitation of the study relates to the methodology that was used. The qualitative approach is used to elucidate interesting ideas from a targeted group of participants and does not address questions regarding the importance of these opinions. Bearing this in mind, the approach used was adequate to cover the broad spectrum of opinions from different groups of FMPs. Qualitative methodology was followed as strictly as possible, in order to avoid other potential biases. Such methodology included: high quality of data collection (i.e., a theoretically determined questionnaire with a focus on research questions);well-trained interviewers; appropriate awareness of the field of research and research aims; consistent nature of the conversation (same questions for all participants); adequate space and environment (silence; recording for all FGs; same refreshments offered, and so on.
The FMPs who agreed to participate were highly motivated physicians and no comparison could be made with others who did not participate. It could be possible, therefore, that outcomes of the present study might not entirely reflect opinions of the entire FMP population in Slovenia.
The eight established categories – Communication, Doctor–patient relationship, Causes of MUS, Patient characteristics, Physician characteristics, Courses of action so far, A positive relationship with patients and proposals for successful treatment (education) – represent the framework of recognized elements, in relation to MUS research at the Slovenian primary care level. The results presented and interpreted here highlight the importance of good communication and trust between physicians and their patients with MUS, draw attention to the systemic barriers of the Slovenian health system (limitations imposed by the National Health Insurance Institute, lack of resources and overburdening of family physicians), and propose interactive education courses and participation of family physicians within the group for professional decision-making (the so-called ‘family counsel’). The results can be compared with other European research 39 and are valuable in terms of investigating the treatment of Slovenian patients with MUS at primary care level, thus opening new avenues of study on the subject of MUS.
Footnotes
Acknowledgements
The authors thank all 24 family physicians who attended the FG discussions and who made this research possible, PhD student Alem Maksuti for his support on the qualitative research methodology/ATLAS Programme and Mrs Shelagh and Mrs Dolinar for reviewing the English language of the manuscript.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.