
Abstract
Objective
Randomized, controlled, blinded trial to evaluate the effectiveness of strategic targeted exercise for preventing falls in elderly people.
Methods
Elderly people were randomly allocated to either a control group that received conventional exercise, or a training group that received conventional exercise plus proprioception and cognitive exercises. Subjects were asked to exercise three times a week (40 min per session) for 8 weeks. In the pre- and post-training sessions, all participants were assessed using a static postural control test with eyes open and closed, the Berg Balance Scale (BBS) and the joint position sense test of the lower limbs.
Results
After 8 weeks, there were statistically significant improvements in the training group (n = 50) compared with the control group (n = 50) for mediolateral sway distance with eyes open and eyes closed, anteroposterior sway distance with eyes open but not with eyes closed, BBS scores and joint position sense test for the left but not the right knee.
Conclusion
This study demonstrated that strategic targeted exercise could produce more beneficial effects on balance and proprioception function than conventional exercise alone, in elderly people.
Introduction
Falls and fall-related injuries are common and serious medical problems for elderly people. Each year, ∼35–45% of community-dwelling people aged over 65 years, and 50% of elderly people, report a fall.1,2 In the elderly, impaired motor performance is often associated with motor retardation, decreased muscle force and decreased balance function. 3 The fifth most common cause of death is unintentional injury in people aged >65 years; in addition, 66.7% of unintentional injury is related to falls and their complications. 1
Multiple factors play a role in falls and related injuries, although balance disorder is the cause of the majority of falls in older, compared with younger, adults. 4 Balance is the ability to maintain the body’s centre of mass within the limits of its base of support when standing and sitting, or while moving to a new base when walking. 5 In humans, correct balance relies on the integration of the senses (such as sight and touch) and the ability to control movement. 6 With age, these abilities decline and become harder to control, which results in an increased risk of falling, even in the absence of specific neurological or musculoskeletal problems.
Research has demonstrated that physical activity is an important strategy for improving proprioceptive function and balance.7,8 Additionally, good cognitive function (in particular, attention) is necessary to maintain proper balance and gait; subjects with an increased risk of falls display a heightened adverse response to dual tasking.9–11 One study defined targeted physical exercise, or targeted training, as the systematic, repeated and controlled activation of particular muscle groups for particular sequences of goal-directed actions. 12
It is unknown whether strategic targeted exercise, compared with conventional exercise, has a specific effect on balance and proprioception function in elderly people. Thus, the present study examined the effects of 8 weeks’ strategic targeted exercise – including strength, stretching, aerobic, proprioception and cognitive exercises – in conjunction with conventional exercise, compared with conventional exercise alone, on balance and proprioception in elderly people.
Subjects and methods
Study population
Elderly subjects were recruited from Nanjing Road and Jingning Road Community Centres for the elderly in Shanghai, China, between May and September 2008. The study was conducted at Huadong Hospital Affiliated to Fudan University, Shanghai, China. Inclusion criteria for the study were: no regular physical exercise habits; aged 60–85 years; a score of ≥22 for the Mini Mental Status Examination (MMSE), 13 to show that subjects had no cognitive impairment. In addition, every subject had to be independent in activities of daily living according to the Independent Activity of Daily Living (IADL) test. 14 Subjects were excluded from the study if they had any of the following: cardiovascular pathologies (such as symptomatic cardiovascular diseases or uncontrolled hypertension); cognitive impairments, as revealed by the MMSE; regular physical exercise habits; any musculoskeletal disease of lower limbs (such as low back pain, serious arthritis or ankylosing spondylitis); any pathology affecting lower extremity function (such as stroke or Parkinson’s disease); any other disabling neurological illness.
The project was approved by the Ethics Committee of Huadong Hospital Affiliated to Fudan University, and written informed consent was obtained from all participants before the study commenced. The trial was registered in the Chinese Clinical Trial Registry (http://www.chictr.org). Registration number: ChiCTR-TRC-12002253.
Study design and procedures
This was two-arm, randomized, controlled trial, stratified by centre, with blinding of both subjects and assessors to treatment group; subjects involved in each type of exercise programme were given no information on the exercises that the other group underwent. Elderly subjects were randomly assigned to the control or training groups by an independent collaborator, within 2 days of study entry, using a computer-generated random-number sequence and opaque closed envelopes. Exercises for both groups were performed at outpatient visits, three times per week (40 min per session) for 8 weeks.
All participants completed a questionnaire that included questions about patient characteristics and outcomes including: sex, age, weight, height, past and present job status, medical history, exercise habits (frequency and time/session). The MMSE and the IADL test were also performed. Subjects completed all assessments at baseline and after the 8-week intervention.
All assessments were carried out by three independent, experienced physical therapists blinded to treatment allocation; these assessors had no contact with any subject during the study. Subjects were instructed not to discuss their treatment with the assessors. All assessments were done using the same practical instructions and took place in one rehabilitation centre (Huadong Hospital Affiliated to Fudan University).
Study training programmes
Subjects were assigned to carry out strategic targeted exercise or conventional exercise interventions three times per week for 8 weeks. Both exercise programmes were led by registered physical therapists. The control group received a conventional exercise programme alone; the training group received proprioception and cognitive exercises in addition to a conventional exercise programme.
Conventional exercise intervention
The main aims of this exercise programme were to improve physical function and teach elderly people how to cope with their falls. The intervention included muscle strengthening, stretching and aerobic exercises, and health education. The classes started with a warm-up session and ended with a cool-down session. After this, there was a short relaxation session and at the end of the class a brief educational message was provided as a ‘tip of the day’. The warm-up and cool-down sessions lasted for ≥6 min and involved marching on the spot, knee lifts, heel digs, shoulder rolls, knee bends and stretching of the major muscle groups. During the 8 weeks of the study, exercises gradually increased in difficulty and training load on an individual basis, if the subject felt that the exercises were too easy.
Proprioception exercise intervention
The proprioception exercise protocol emphasized static and dynamic balance exercises, including transitions between differing sensory conditions and functional everyday movements. Each session incorporated a similar general plan: (1) warm-up; (2) static balance exercises, such as squats (two-leg stance) and one leg stance; (3) dynamic balance exercises such as jogging end to end, sideways walking or running with crossovers, forward walking or running in a zigzag line, and backward walking or running in a zigzag line; (4) cool-down. The warm-up and cool-down sessions were carried out as described above. During the 8 weeks of the study, exercises gradually increased in difficulty and training load on an individual basis, if the subject felt the exercises were too easy.
Cognitive dual-task training
The cognitive training programme was based on a dual-task concept. Each session incorporated a similar general plan: (1) warm-up; (2) subjects were asked to give a response to continuous simple addition/subtraction questions (such as 3 + 2 = 5, 100 − 7 = 93) while performing static balance exercises for 15 min; (3) dynamic balance exercises while performing cognitive tasks simultaneously, such as sideways walking or running with crossovers while performing addition/subtraction questions; (4) cool-down. The warm-up and cool-down sessions were carried out as described above. The subject was challenged with increasingly difficult tasks during the 8 weeks of the study, if they felt the exercises were too easy.
Outcome measures
Static balance test
Postural control was evaluated by a Biodex Balance System Device (Biodex Medical Systems, New York, NY, USA). Briefly, each participant stood barefoot on a platform and performed a balance test; the level of difficulty while standing on the platform was manipulated by altering the resistance of the platform to deviations (level 8, easiestl; level 1, hardest). The foot position was standardized using a preformed triangle (heels together with feet forming an angle of 20°). Subjects were instructed to keep their hands at their sides. For safety purposes they were permitted to touch the handrails, but only to re-establish balance during extreme postural deviations. The participants were then instructed to find a position at which they could maintain platform stability. Each recording lasted for 60 s, with a 60 s rest between each trial. Mediolateral sway distance, anteroposterior sway distance and centre of pressure area were assessed in both groups while subjects had their eyes open and eyes closed.
Berg Balance Scale
The Berg Balance Scale (BBS) is widely used to test a person's static and dynamic balance abilities. For functional balance tests, the BBS is generally considered to be the gold standard. 15 The test comprises 14 simple balance-related tasks, ranging from standing up from a sitting position to standing on one foot. BBS scores range from 0 to 56 points; higher scores indicate better balance.
Joint position passive matching test
Subjects were seated in a standardized starting position of 90° of hip flexion and knee extension. First, the investigators moved the subject’s knees from the starting position to either 30° or 60° flexion, then subjects passively moved their knees while wearing sleep goggles (eyes closed) to two flexion angles (30° and 60°), as instructed by the investigator. The error within which the subject reproduced the initial position was calculated. The mean of three absolute error values was taken and termed the absolute angle error (°).
Statistical analyses
All statistical analyses were performed using the SPSS® statistical package, version 17.0 (SPSS Inc., Chicago, IL, USA) and Microsoft Excel® 2003 for Windows®. Data were expressed as mean ± SD. Changes in variables between pre- and post-training values, and between groups, were analysed. An independent-samples t-test and the χ2-test were used to compare both groups at baseline. A two-way analysis of variance (group × time) was used to assess the effects of treatment depending on group allocation. An intention-to-treat analysis was performed, by carrying the last value forward in the case of missing values at the second assessment. A P-value < 0.05 was considered to be statistically significant.
Results
A total of 100 elderly subjects were recruited into the study: 50 were allocated to each group. Patient disposition is outlined in Figure 1. After 8 weeks, 95 subjects remained and attended all of the intervention sessions in the study: three participants from the training group and two from the control group were lost to follow-up. The groups were well matched at baseline, with no significant differences in demographics and clinical characteristics (Table 1).
Patient disposition for elderly people randomized into either a control group (which performed a conventional exercise programme) or a training group (which performed a conventional exercise programme plus proprioception and cognitive exercises three times a week [40 min per session] for 8 weeks). Baseline demographics and clinical characteristics for elderly people randomized into a control group that performed a conventional exercise programme or a training group that performed a conventional exercise programme plus proprioception and cognitive exercises three times a week (40 min per session) for 8 week. Data presented as mean ± SD or n of subjects. χ2-test; bindependent-samples t-test. NS, there were no statistically significant differences (P ≥ 0.05); MMSE, Mini Mental Status Examination; ML, mediolateral; AP, anteroposterior; COP, centre of pressure; JPS, joint position sense.

After 8 weeks’ training, results of the static balance test showed a significant improvement in the training group versus the control group in the mediolateral sway distance with eyes open or closed (P < 0.05), and in the anteroposterior sway distance with eyes open (P < 0.05) (Figure 2). There was no significant difference in the centre of pressure between the two groups (Figure 2).
Static balance function test results in elderly people randomized into a control group (n = 48) that performed a conventional exercise programme or a training group (n = 47) that performed a conventional exercise programme plus proprioception and cognitive exercises three times a week (40 min per session) for 8 weeks. Mediolateral sway distance (ML), anteroposterior sway distance (AP) and centre of pressure area (COP) were assessed when subjects had (A) eyes open and (B) eyes closed. Data presented as mean ± SD; *P < 0.05 for training group versus control group, two-way analysis of variance (group × time).
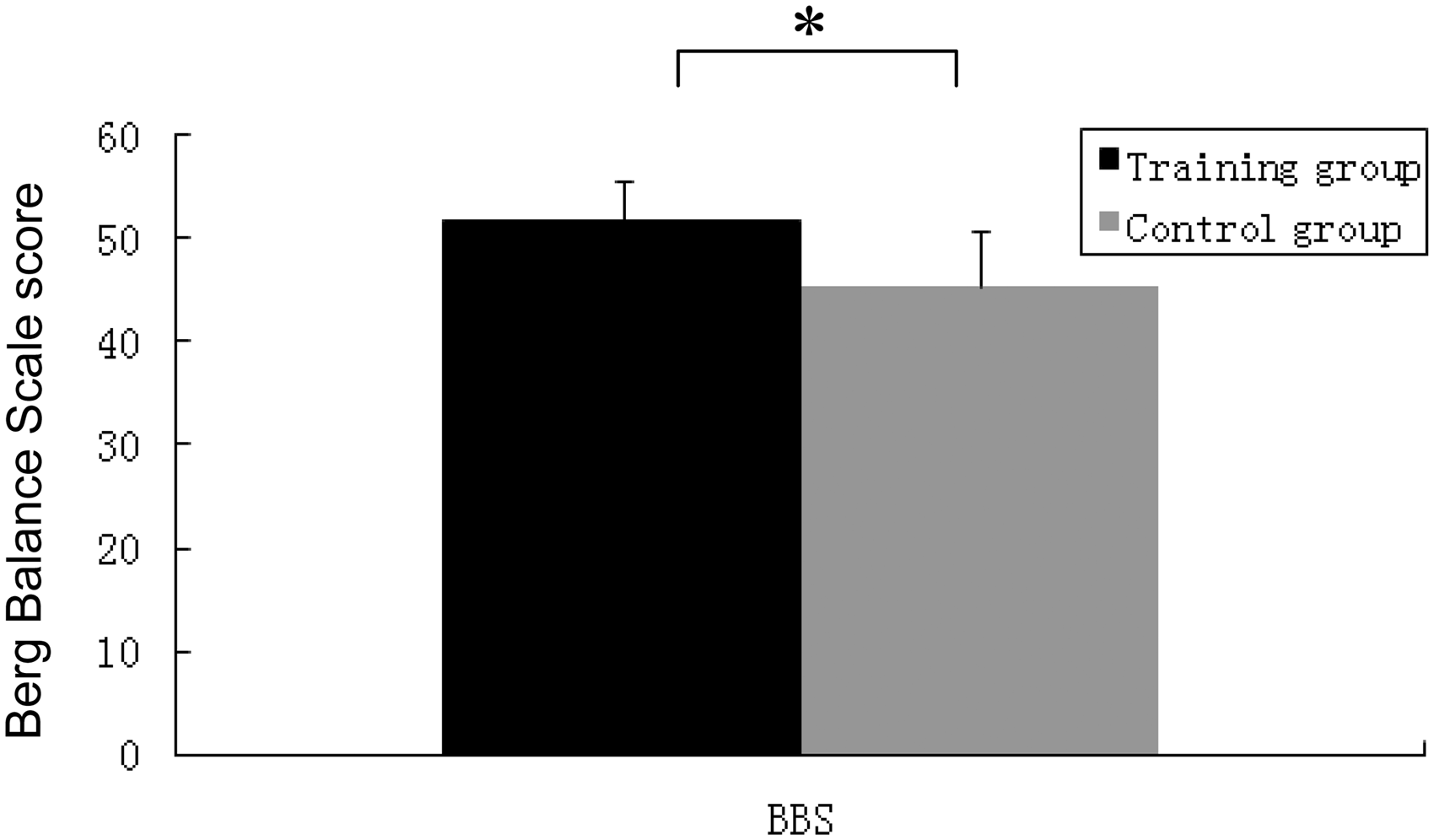
After 8 weeks’ training, there was a significant difference between the training and control groups in the joint position sense test for the left (P < 0.05), but not the right, knee (Figure 3), and a significantly greater improvement in BBS scores in the training group versus the control group (P < 0.05) (Figure 4).
Joint position passive matching test results in elderly people randomized into a control group (n = 48) that performed a conventional exercise programme or a training group (n = 47) group that performed a conventional exercise programme plus proprioception and cognitive exercises three times a week (40 min per session) for 8 weeks. The error within which the subject reproduced initial position set by the investigator was calculated and the absolute angle error was the mean of three absolute error values. Data presented as mean ± SD; *P < 0.05 for training group versus control group, two-way analysis of variance (group × time). Berg Balance Scale (BBS) results in elderly people randomized into a control group (n = 48) that performed a conventional exercise programme or a training group (n = 47) that performed a conventional exercise programme plus proprioception and cognitive exercises three times a week (40 min per session) for 8 weeks. Data presented as mean ± SD; *P < 0.05 for training group versus control group, two-way analysis of variance (group × time).
Discussion
The present randomized controlled study demonstrated that, in elderly people, an 8-week strategic targeted exercise programme combined with conventional exercise produced more beneficial effects on balance and proprioception function than conventional exercise alone. Static balance performance, joint position sense and BBS scores were all significantly improved in the strategic targeted exercise group compared with the control group.
Exercise can improve balance-related outcomes and reduce falls in elderly people.16–19 An integrated approach to balance and strength training was adopted in one study and was effective in reducing the fall rate in elderly people. 20 A systematic literature review suggested that multifactorial assessment and targeted intervention could potentially reduce falls and fall-related injuries among elderly people. 21 This study, however, only compared subjects who had participated in integration of balance and strength training with those who received no rehabilitation training. 21 In contrast, the present study examined the effects of strategic targeted exercise compared with a conventional exercise programme on balance function and joint position sense. The strategic targeted exercise programme also included muscle strength, balance, proprioception and cognitive exercises.
The present study showed significant improvements in mediolateral sway distance, anteroposterior sway distance, the joint position sense test for the left knee and BBS scores in the training group compared with the control group. The results were consistent with other studies,22–24 showing that strategic targeted exercise is superior to conventional exercise alone, for elderly people. There seems to be consensus that focusing on fall prevention, rather than simply treating any resulting injuries, will be more effective in reducing the economic burden of falls. Thus, greater resources are needed for the provision of prevention and intervention services.
There were several limitations to the present study. First, the sample size was too small to draw any firm conclusions. Secondly, the findings cannot be generalized to elderly people living in nursing homes or hospital settings. Further multicentre, randomized, controlled trials with larger sample sizes are needed.
In conclusion, the present study showed that balance function and joint position sense significantly improved in elderly people treated with strategic targeted exercise, compared with conventional exercise alone. Further long-term follow-up studies are needed to substantiate these findings.
Footnotes
Acknowledgements
The authors thank all subjects for their willingness to participate in this study.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This study received financial support from the Shanghai Natural Science Foundation of China (Grant No. 06JC14027) and the National Science Foundation for Young Scholars of China (Grant No.81101391).