
Abstract
Objectives
To investigate the safety and therapeutic efficacy of autologous olfactory ensheathing cell (OEC) transplantation in cervical spinal cord injury (SCI).
Methods
Patients with cervical SCI of >6 months’ duration were treated with autologous OECs, injected into the area surrounding the SCI under magnetic resonance imaging guidance, twice a week for 4 weeks. Patients were evaluated before treatment and at 3, 6, 12 and 24 months post-treatment, using the American Spinal Injury Association (ASIA) Impairment Scale, the ASIA sensory and motor score and the Functional Independence Measure (FIM) score.
Results
Eight patients were recruited to the study. Three months after treatment, ASIA and FIM scores had improved significantly compared with pretreatment, though by 1 year no further significant improvements in the ASIA score were seen. The return of substantial sensation and motor activity in various muscles below the injury level was observed in three patients during follow-up. In addition, bladder function was restored in two patients. There were no serious complications postoperatively or during the follow-up period.
Conclusions
This study provides preliminary evidence of the safety and possible efficacy of autologous OEC transplantation.
Keywords
Introduction
Spinal cord injury (SCI) is a serious health problem that often leads to devastating dysfunction and disability. 1 In China, there are ∼400,000 people living with SCI, and it is estimated that 10,000 new cases occur every year, the majority of which result from motor vehicle incidents or sports injuries, violence or falls from a height. 2 Treatments for SCI include surgical stabilization of the spinal column, decompression surgery, administration of high-dose steroids and rehabilitation.3–5 Although substantial progress has been made in the survival of injured individuals, attempts to restore function have remained essentially ineffective. 6
Cell therapy has become one of the most promising therapeutic approaches for SCI. 7 Some animal studies have suggested that transplantation of bone marrow stromal cells, neural progenitor cells or olfactory ensheathing cells (OECs) can promote functional improvement after SCI.8–10
It has been demonstrated that bone marrow stromal cells (BMSCs) are able to differentiate into mature neurons or glial cells, under specific experimental conditions. 11 Transplanted BMSCs have been shown to improve neurological deficits in SCI models by generating neural or myelin-producing cells. 12 However, in clinical trials, BMSC transplantation has not been shown to enhance functional recovery significantly, after SCI. 13
The neurosensory cells of the olfactory mucosa are a population of adult neurons that are continually renewed throughout life. 14 It has been shown that the major component of olfactory mucosa – OECs – guide axons growing from the neurons of the olfactory mucosa to form synapses in the olfactory bulb. 15 Moreover, OECs are pluripotent stem cells that can show Schwann cell-like properties. 16 Transplantation of human OECs into rat spinal cord lesions showed that OECs were able to remyelinate axons. 17
To date, there are few clinical studies investigating the treatment of SCI using human OECs. The present study examined the therapeutic and adverse effects of transplanting autologous OECs into the area surrounding cervical SCI.
Patients and methods
Patients
Patients with cervical SCI of >6 months’ duration, attending the Luoyang Orthopaedic–Traumatological Hospital, Luoyang, China, between January 2008 and December 2011, were enrolled sequentially in this study. The diagnosis of SCI had been confirmed by magnetic resonance imaging (MRI). All of the patients were healthy prior to the injury and had no other major diseases or impairments. Inclusion criteria for the study comprised: aged between 18 and 50 years; presence of cervical SCI categorized as grade A, B or C on the American Spinal Injury Association (ASIA) Impairment Scale; 18 the absence of ‘significant’ nasal or paranasal sinus pathology. Exclusion criteria included: spinal vertebral instability; major concurrent medical illness (such as carcinoma, autoimmune disease or diabetes mellitus). All patients had been treated with neurosurgical stabilization, standard therapy (such as surgery and pharmacological therapies) and rehabilitation.
The study protocol was approved by the Ethics Committee of the Luoyang Orthopaedic–Traumatological Hospital. All procedures were performed after obtaining written informed consent from the study participants.
Isolation and culture of OECs
Autologous OECs were isolated according to a method described previously. 19 Briefly, olfactory mucosa biopsies were taken under local anaesthesia from the root of the medial aspect of the middle turbinate of each patient, using endoscopic guidance. Samples were washed using Dulbecco’s modified Eagle’s medium (DMEM)/Ham’s F12 (Gibco, Carlsbad, CA, USA), the olfactory epithelium was removed, and the remaining laminae propriae were triturated using a 20-gauge needle and incubated with collagenase IA (Sigma-Aldrich, Bornem, Belgium) for 10 min at 37°C. They were then passed through a 40-µm nylon mesh cell strainer (Becton Dickson, Franklin Lakes, NJ, USA) to produce a single-cell suspension in phosphate buffered saline at pH 7.4. Cells were cultured in DMEM/Ham’s F12 supplemented with 10% fetal bovine serum (Gibco) and penicillin/streptomycin (100 IU/ml and 100 mg/ml, respectively) (Invitrogen, Carlsbad, CA, USA) in a humidified incubator at 37°C and 5% CO2. The medium was changed every 2–3 days. When confluency was reached, ∼2 weeks later, the cells were subcultured for subsequent propagation to attain the number of cells required for transplantation. OECs were cultured continuously for 1 month, to provide cells for transplantation over a 4-week period.
Preparation of cells for transplantation
Cell viability was assessed using trypan blue exclusion; cells with a viability of ≥95% were used for transplantation. The morphological phenotype of the OECs was confirmed using microscopy, and culture samples were incubated in nutrient media for 14 days to test for sterility. In addition, a sample of the final product was sent for Mycoplasma testing.
Cells were dissociated with 0.25% trypsin/0.53 mM ethylenediamine tetra-acetic acid (Invitrogen); enzymatic activity was then stopped using culture medium. Next, 10 ml of the cell suspension was centrifuged (1000 r.p.m.; 37°C for 10 min) and the cell pellet was washed three times with saline. The entire cell pellet was then suspended in 1 ml of saline and was delivered to the operating room. Cells were resuspended with the addition of a further 1 ml of saline before being loaded into a syringe for transplantation; each 2-ml injection contained approximately 1 million cells.
Implantation of OECs
All surgical procedures were performed by the same surgical team. Prophylactic antibiotics (cefoxitin, 2 g) were administered shortly before surgery. After aseptic preparation, the patient was positioned in the lateral decubitus position. Local anaesthesia was given by subcutaneous injection at the site of the procedure. Cell preparations 2 ml in volume were injected slowly into the dura at each of six locations evenly distributed around the caudal border of the lesion, under MRI guidance. The needle was held in position for 3 min after injection, then flushed with 1 ml of saline to prevent cell leakage through the injection track. Each puncture site was sealed and covered with Tegaderm® (3M, St Paul, MN, USA) for 24 h. The procedure took ∼3 h to complete. Each patient received two sets of injections per week, for 4 weeks.
Patient assessment
Prior to transplantation of autologous OECs, all patients underwent MRI and neurological examinations. Follow-up neurological examinations were carried out at 3, 6, 12 and 24 months after the end of the treatment period.
Pre- and post-treatment neurological evaluations were performed by two independent neurologists (Y.J.R. and W.X.Z.) according to the ASIA International Standards for Neurologic and Functional Classification of Spinal Cord Injury 18 and the Functional Independence Measure (FIM). 20 The five-grade ASIA Impairment Scale is based on neurological responses, touch and pinprick sensations in 28 dermatomes, and the strength of 10 key muscles on each side of the body. Injuries are graded as follows: A, complete lesion, with no motor or sensory function in the sacral segments S4–S5; B, incomplete lesion with sensory but no motor function preserved below the neurological level, including the sacral segments S4–S5; C, incomplete lesion with motor function preserved below the neurological level, and where more than half of the key muscles below the neurological level have a muscle grade of <3; D, incomplete lesion with motor function preserved below the neurological level, and where at least half of the key muscles below the neurological level have a muscle grade of ≥3; E, normal function. In addition, the sum of the ASIA sensory scores for pinprick and light touch (0, absent; 1, impaired; 2, normal; maximum score 56 on each side for each type of sensory score) and motor score (ranging from 0 indicating no active movement to 5 indicating movement against full resistance; maximum score 50 on each side) was recorded for each patient, with a maximum possible score of 324.
The FIM evaluates functional ability in six areas (self care, sphincter management, transfers, locomotion, communication and social cognition) and gives an indication of the patient’s degree of independence.
Statistical analyses
Results were expressed as the mean ± SE. Differences between pre- and post-treatment ASIA and FIM scores were examined using analysis of variance followed by the least significant difference post-hoc test. Bonferroni’s correction was used to adjust for multiple comparisons. A P-value <0.05 was considered to be statistically significant. All statistical analyses were performed using SPSS® software, version 17.0 (SPSS Inc., Chicago, IL, USA).
Results
Baseline demographic and clinical characteristics of eight patients with cervical spinal cord injury (SCI), recruited to a study investing the safety and therapeutic efficacy of autologous olfactory ensheathing cell transplantatio.

ASIA, American Spinal Injury Association (Impairment Scale).
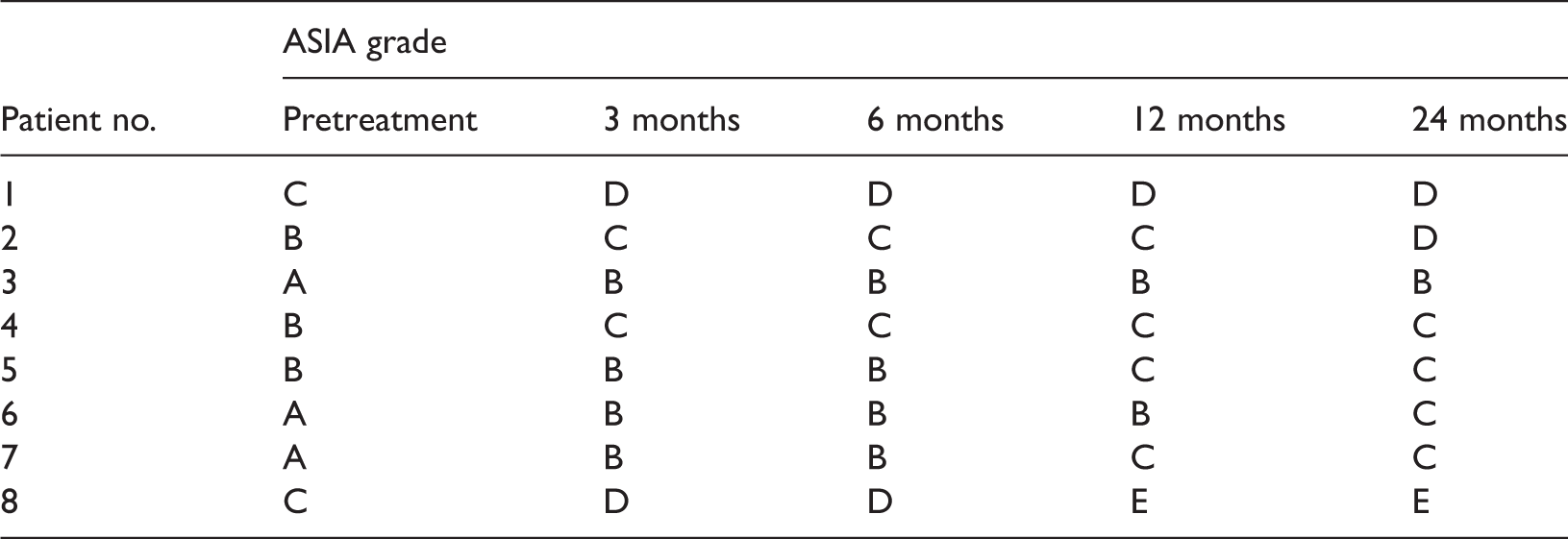
Transplantation of OECs was performed between 8 and 15 months after injury. No patients were lost to follow-up. The results of pre- and post-treatment neurological examinations are presented for individuals in Table 2 and summarized for the study group in Figure 1. Treatment was associated with improved ASIA and FIM scores compared with pretreatment, in all patients. Three months after treatment, mean ASIA and FIM scores had improved significantly compared with pretreatment (P < 0.05) (Figure 1). Subsequent significant increases in ASIA scores were seen between 3 and 6 months (P = 0.02) and between 6 and 12 months (P = 0.01); 1 year after treatment, no further significant improvements were observed. Significant increases in FIM scores were seen between 3 and 6 months (P = 0.01) and between 12 and 24 months (P = 0.01).
Neurological scores in eight patients with cervical spinal cord injury, before (and 3, 6, 12 and 24 months after) transplantation with autologous olfactory ensheathing cells. ASIA, American Spinal Injury Association score; FIM, Functional Independence Measure score. Values presented as mean ± SE. *P < 0.05 compared with pretreatment using analysis of variance and least significant difference post-hoc test. Neurological examination scores in eight patients with cervical spinal cord injury, before (and 3, 6, 12 and 24 months after) transplantation with autologous olfactory ensheathing cell. ASIA, American Spinal Injury Association (Impairment Scale); FIM, Functional Independence Measure.

American Spinal Injury Association (ASIA) Impairment Scale grades in eight patients with cervical spinal cord injury, before (and 3, 6, 12 and 24 months after) transplantation with autologous olfactory ensheathing cell.
Discussion
To date, surgical treatment of SCI has not achieved satisfactory outcomes. 21 In a preclinical study in SCI rat models, treatment with BMSC transplantation improved motor scores as well as sensory function. 13 In addition, several studies have been performed using in vitro expanded neural stem/progenitor cells implanted into rats with spinal cord injury. 12 These cells survived and differentiated into neurons, astrocytes and oligodendrocytes, and treatment had a positive effect on functional outcome. 12 However, ‘significant’ functional recovery after transplantation with these cells has rarely been achieved in human clinical trials. 6
In the peripheral nervous system, OECs have been shown to be able to regrow to their original destinations and restore function after axotomy. 18 OECs are a type of glial cell found in the olfactory mucosa; they are continually renewed throughout life, to form new olfactory nerve fibres that leave the olfactory mucosa and pass through the cribriform plate, forming terminals in the glomerular layer of the olfactory bulb. 22 In vitro coculture with neurons has demonstrated that OECs can form myelin, 11 and long-distance regeneration of spinal axons has been observed after transplantation of cultured OECs into rat spinal cord lesions. 15 However, related clinical studies with OECs are rare.
In the present clinical study, patients with SCI received multiple transplants of OECs by injection into the area surrounding the injury. Neurological examination 3, 6, 12 and 24 months after treatment showed improvements in ASIA and FIM scores, in all eight patients. Three and 6 months after treatment, mean ASIA and FIM scores had improved significantly compared with pretreatment, though by 1 year after treatment, no further significant improvements in the ASIA score were observed. The substantial return of sensation and motor activity in various muscles below the injury level was observed in three patients during follow-up. In addition, bladder function was restored in two patients.
The results of the present study suggest that human OECs transplanted into the spinal cord may have a role in functional recovery, in patients with SCI. OECs may improve neurological function by remyelinating axons. In addition, it has been reported that transplanted OECs can modify the behaviour of host glial cells, and also induce rapid and intense vascularization. 23 Applied early after injury, they may reduce the secondary (spreading) effects of spinal lesions. 24 However, the exact therapeutic mechanisms involved are not yet clear.
In the present study, OEC transplantation in patients with SCI was not associated with any serious adverse effects. The use of autologous OECs for therapy has several advantages. Problems related to immunological rejection or graft-versus-host reactions, which frequently occur in allogenic cell transplantation, 25 can be avoided. In addition, autologous OEC transplantation is not associated with ethical problems. Biopsy of the human olfactory mucosa is relatively straightforward and can be performed under either general or local anaesthesia, and isolation of OECs can be easily undertaken. 19 Furthermore, in the present study there were no serious complications postoperatively or during the follow-up period. Thus, multiple transplantation of OECs appeared to be a safe, effective and uncomplicated therapeutic technique in SCI. These characteristics suggest that OEC transplantation therapy may have a wider application in other neurological diseases.
There are several limitations with the present study. First, adequate control groups were absent, so it cannot be determined whether this technique was superior to other methods. Secondly, neurological improvements were assessed using ASIA and FIM scores, so small improvements without significant score changes would not have been identified. Thirdly, the study population was relatively small, so the incidence of adverse events or recovery can only be approximated from the observed rates; further large-group studies are therefore needed.
In conclusion, the clinical study described here has established the feasibility of autologous OEC-based therapy in SCI. There were no specific safety problems or serious complications associated with this treatment, and it may be associated with improved neurological function.
Footnotes
Declaration of conflicting interest
The Authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.