
Abstract
Objective
A case–control study to investigate the association of the 9p21 single nucleotide polymorphisms (SNPs) rs10757274 and rs10757278 (known to be associated with coronary artery disease [CAD] risk) with peripheral arterial disease (PAD), in a Han Chinese population.
Methods
The rs10757274 and rs10757278 genotypes of patients with PAD, and age- and sex-matched control subjects, were determined. Multivariate unconditional logistic regression analyses were performed, with adjustments for age, sex, hypertension, dyslipidaemia, diabetes and smoking status.
Results
The study included 420 patients with PAD and 418 control subjects. Variant forms of both SNPs were associated with increased risk of PAD in the total study population, when excluding patients with CAD or stroke (additive genetic model). The GG haplotype increased the risk of PAD, but this association did not remain significant after further sensitivity analysis. Both SNPs were associated with PAD risk in patients aged <65 years, but not in those aged ≥65 years (additive model).
Conclusions
9p21 is associated with PAD. When stratified according to age, 9p21 increases PAD risk in individuals aged <65 years, but not in those aged ≥65 years.
Introduction
Numerous genome-wide studies have shown that common sequence variants on chromosome 9p21 are closely associated with increased risk of atherosclerotic diseases including coronary artery disease (CAD),1–4 myocardial infarction5–7 and stroke,8–10 with the single nucleotide polymorphisms (SNPs) rs10757274 and rs10757278 linked particularly with CAD.1,11,12 The homozygous GG genotype of rs10757278 is associated with CAD severity, extent and progression in Caucasian populations, 13 and both loci are also significantly associated with ischaemic stroke risk.9,14 The increased risk of atherosclerosis is mediated via effects on the expression of cyclin-dependent kinase inhibitor 2 A (CDKN2A, also known as INK4/ARF).9,15,16
Peripheral arterial disease (PAD) is a common form of atherosclerotic disease that has a similar aetiology and pathogenesis to CAD and ischaemic stroke. 17 PAD increases the risk of disability, all-cause mortality and cardiovascular mortality.18–20 The SNPs rs10757274 and rs10757278 may be associated with PAD development but data are inconsistent,11,21–25 and the association between rs10757278/rs10757274 and PAD in the Han Chinese population remains largely unexplored. The present study therefore investigated the relationship between rs10757278 and rs10757274 and PAD prevalence in a Han Chinese population.
Patients and methods
Study Population
This population-based case–control study recruited consecutive, unrelated, Han Chinese patients with PAD, aged ≥45 years, who were attending the Department of Vascular Surgery, Tangshan Gongren Hospital, Hebei Medical University, Tangshan, China, for treatment or physical examination between January 2006 and December 2011. Patients with heart failure, renal failure, hepatic disease, venous embolism, intracerebral haemorrhage, severe inflammatory disease, endocrine disease, immunological disease or malignant tumours were excluded from the study.
The diagnosis of PAD was based on an ankle–brachial index (ABI) of ≤0.9 for either leg. Left and right ABIs were measured as the ratio of the supine left or right ankle systolic blood pressure, divided by the highest of the right or left brachial systolic blood pressure; the mean of two measurements for each leg was calculated (COLIN VP 1000; Colin, Komaki, Japan). The lower ABI of the two legs was selected for analysis. Patients with ABI ≥1.4 were excluded from the study (to exclude the effects of incompressible and calcified arteries 26 ). CAD was defined as a history of coronary artery revascularization or percutaneous coronary angiography (≥70% stenosis in a major coronary artery) or myocardial infarction, diagnosed according to World Health Organization criteria. 27 Ischaemic stroke was diagnosed by computed tomography, magnetic resonance imaging or a documented cerebral stroke.
Age- and sex-matched control subjects aged ≥45 years, with ABI >0.9–<1.4, were recruited from individuals undergoing routine health checks at the Health Examination Centre, Tangshan Gongren Hospital, Tangshan, China. Control subjects were required to be free of atherosclerotic diseases including PAD, CAD and stroke, and were subject to the exclusion criteria for patients, listed above. For all study participants, data regarding demographic characteristics, medical history and smoking status were collected by questionnaire interview or review of medical records. All study participants were categorized as never smokers, former smokers (ceased smoking >1 year before enrolment) or current smokers.
The study was approved by the Ethics Committee of Tangshan Gongren Hospital and written informed consent was provided by all participants prior to enrolment.
Laboratory Analyses
Hypertension was defined as systolic blood pressure ≥140 mmHg, and/or diastolic blood pressure ≥90 mmHg, and/or history of hypertension, and/or current antihypertensive medication. Dyslipidaemia was defined as total cholesterol ≥5.72 mmol/l, and/or triglyceride ≥1.7 mmol/l, and/or high-density lipoprotein cholesterol (HDL-C) ≤0.91 mmol/l, and/or low-density lipoprotein cholesterol (LDL-C) ≥3.64 mmol/l. Venous blood samples were collected from each participant in the morning after an overnight fast; serum total cholesterol, triglyceride, HDL-C and LDL-C levels were determined immediately at the Biochemistry Laboratory, Tangshan Gongren Hospital, using the AU5400® Chemistry System (Beckman Coulter, Brea, CA, USA).
Genotyping
Blood was collected into sterile tubes containing ethylenediaminetetra-acetic acid, and genomic DNA was isolated using a QIAamp DNA mini kit (QIAGEN GmbH, Hilden, Germany), according to the manufacturer’s instructions. Genotyping of rs10757274 and rs10757278 was performed by matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI–TOF–MS), with Sequenom iPLEX™ (Sequenom, San Diego, CA, USA), according to the manufacturer’s instructions. Quality control was performed with 5% of samples, to ensure reproducibility.
Statistical Analyses
Continuous data were expressed as mean ± SD or median (interquartile range), and between-group differences were analysed using independent-samples t-test or the Mann–Whitney U-test. Qualitative variables were expressed as n (%) and compared using the χ2-test. Differences in allelic and genotype frequencies between patients and controls were compared using the χ2-test. Odds ratios (ORs) and 95% confidence intervals (CIs) were estimated by multivariate unconditional logistic regression analysis with adjustments for age, sex, hypertension, dyslipidaemia, diabetes mellitus and smoking status under different genetic models. Statistical analyses were performed using SPSS® software, version 16.0 (SPSS Inc., Chicago, IL, USA) for Windows®. A P-value <0.05 was considered statistically significant.
Linkage disequilibrium between SNPs was estimated using Haploview software, version 4.0 (Broad Institute, Cambridge, MA, USA). 28 Haplotype frequencies were estimated by Phase software, version 2.0 (available at http://en.bio-soft.net/tree/PHASE.html), and further verified using Haploview, version 4.0. Haplotype analysis was estimated by multivariate unconditional logistic regression analysis.
Results
Demographic and clinical characteristics of Han Chinese patients with peripheral arterial disease (PAD) and age- and sex-matched control subjects, included in the study to investigate the association between PAD and the 9p21 single nucleotide polymorphisms rs10757274 and rs10757278.

Data presented as mean ± SD, n (%) of cases or median (interquartile range).
Independent-samples t-test or Mann–Whitney U-test for continuous data; χ2-test for categorical data.
Total cholesterol ≥5.72 mmol/l, and/or triglyceride ≥1.7 mmol/l, and/or high-density lipoprotein cholesterol (HDL-C) ≤0.91 mmol/l, and/or low-density lipoprotein cholesterol (LDL-C) ≥3.64 mmol/l.
Ceased smoking >1 year prior to enrolment.
Systolic blood pressure ≥140 mmHg, and/or diastolic blood pressure ≥90 mmHg, and/or history of hypertension, and/or current antihypertensive medication.
Genotype and allele distribution of 9p21 single nucleotide polymorphisms (SNPs) rs10757274 and rs10757278 in Han Chinese patients with peripheral arterial disease, and age- and sex-matched control subjects.

Data presented as number of alleles [allelic frequency], or n (%) of participants.
χ2-test.
Multivariate unconditional logistic regression analyses of associations between variant forms of the 9p21 single nucleotide polymorphisms rs10757274 and rs10757278 and peripheral arterial disease, in Han Chinese study participants. Analyses were performed for additive, dominant and recessive genetic models and were adjusted for age, sex, hypertension, dyslipidaemia, diabetes and smoking status.
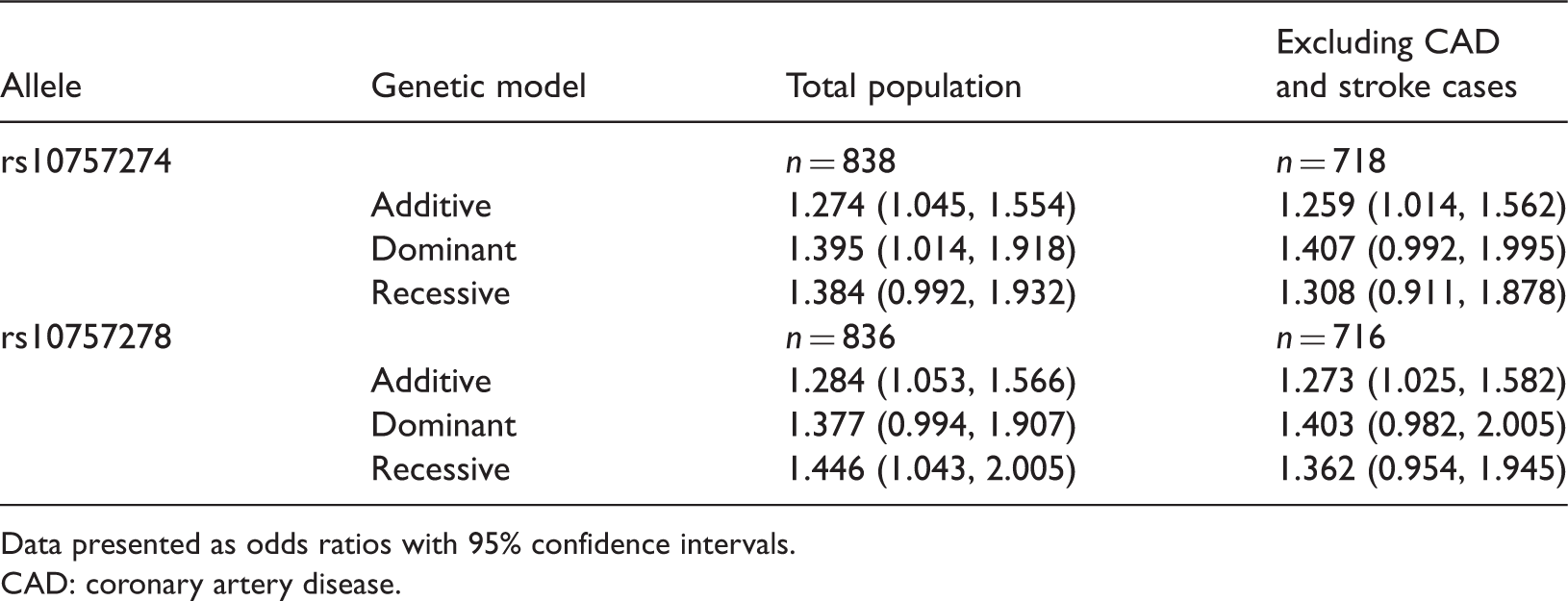
Data presented as odds ratios with 95% confidence intervals.
CAD: coronary artery disease.
Multivariate unconditional logistic regression analyses (adjusted for age, sex, hypertension, dyslipidaemia, diabetes and smoking status) for the association between 9p21 single nucleotide polymorphism rs10757274 and rs10757278 haplotypes and peripheral arterial disease in Han Chinese study participants.

Data presented as n of subjects (frequency). (%)
CAD: coronary artery disease; OR: odds ratio; 95% CI: 95% confidence intervals.
Multivariate unconditional logistic regression analyses of the association between variant forms of the 9p21 single nucleotide polymorphisms (SNPs) rs10757274 and rs10757278 and peripheral arterial disease, in Han Chinese study participants, stratified according to age (<65 and ≥65 years). Analyses were performed for additive, dominant and recessive genetic models and adjusted for age, sex, hypertension, dyslipidaemia, diabetes and smoking status.

Data presented as odds ratios with 95% confidence intervals.
CAD: coronary artery disease.
Discussion
Findings of the present study indicate an association between the 9p21 SNPs rs10757274 and rs10757278 and PAD in a Han Chinese population. The variant GG haplotype was associated with increased risk of PAD in the total study population, but this association did not remain significant when patients with CAD or stroke were excluded from the analysis. This suggests that the association between the GG haplotype and PAD may be confounded by other atherosclerotic diseases, including CAD and stroke. The results of the current study indicate that the CAD risk region on 9p21 could harbour the risk loci conferring susceptibility to PAD in the Han Chinese population.
The C allele of rs1333049 (as the optimal proxy of rs10757278; D′ = 1)24,29 has been shown to be associated with lower ABI and increased risk of PAD than the G allele. 21 Others found a similar association between ABI and rs10757278 and rs1333049,22,23 but further studies indicated no association between rs10757278 and PAD.11,24 The variant forms of rs10757278 and rs10757274 were found to increase the risk of PAD in the present study of a Han Chinese population. Others have found no association between rs10757274 and PAD in African American or Caucasian people. 25 These conflicting results may be attributed to complex genetic and environmental factors.
Studies have indicated that 9p21 was associated with PAD in individuals aged ≥65 years, 21 with no association in those aged <65 years. 25 Age stratification analysis in the present study indicated that both SNPs were significantly associated with PAD in Han Chinese people aged <65 years. There were no associations between either SNP and PAD in those aged ≥65 years in the present study, suggesting that the effects of 9p21 on PAD may change with age. Studies have demonstrated a greater impact of 9p21 on CAD at early ages; 5 as PAD and CAD have similar aetiology and pathogenesis, the effect of 9p21 on PAD may be greater in younger patients than in older patients.
The underlying functional mechanism of how 9p21 genetic variants affect PAD risk remains to be elucidated. The pathogenesis of PAD is similar to that of CAD and ischaemic stroke. Functional studies have demonstrated that 9p21 contributes to CAD via atherosclerosis induced by variants located near CDKN2A, CDKN2B and CDKN2B antisense RNA 1 (CDKN2B-AS1) genes, which are involved in regulating cell proliferation, cell ageing and senescence, and apoptosis.16,30–33 Other research found that 9p21 contributed to CAD development by modulating the inflammatory pathway involved in the atherosclerosis process, 34 or by deposition of coronary artery atheroma.13,35 Despite these data, the mechanism of the interaction between 9p21 and PAD requires further investigation.
In conclusion, the present study indicates that the 9p21 CAD region is associated with PAD. When stratified according to age, variant 9p21 confers additional PAD risk in individuals aged <65 years, but not those aged ≥65 years. The underlying mechanism remains to be elucidated.
Footnotes
Acknowledgements
We thank Huada Genetic Corp., Shenzhen, China, for assistance with genotyping, and Dr Yun-tao Zhou, Dr Guang-ping Li and Dr Xue-mei Zhang for assistance with genetic analyses.
Declaration of Conflicting Interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by grants from the Programme of Hebei Province Science and Technology Department (03276403D-27) and Hebei Province Substantial Research Programme (20110609).