
Abstract
Background
The management of patients with slipped capital femoral epiphysis (SCFE) requires imaging diagnostics of good quality and accurate measurement of the degree of slippage. In Sweden, three different radiological methods are commonly used: the calcar femorale method; the Billing method; and the Head-shaft angle described by Southwick.
Purpose
To evaluate whether any of the three most common methods used in Sweden to measure the slip angle was more useful and reproducible than the others.
Material and Methods
Two experienced orthopaedists measured the slip angle in preoperative hip radiographs. Intra- and inter-observer variability between the two experienced observers and the reported value by clinicians who treated the child with SCFE was evaluated.
Results
The intraclass correlation coefficient (ICC) confidence interval (CI) between the two experienced observers and the reporting clinicians overlapped for the three methods. In 37% of the cases, the difference was more than 5° between the experienced observers’ measurement and the reported value by clinicians. The two experienced orthopaedists' intra- and inter-observer variability was low.
Conclusion
The observer's experience is more important than the method of choice when measuring the slip angle in SCFE. The research group recommends the calcar femorale method due to its feasibility on the versatile and commonly used frog leg lateral view.
Keywords
Introduction
Slipped capital femoral epiphysis (SCFE) mainly affects young teenagers. In a population-based study of Swedish children, the mean age at diagnosis was 11.6 years for girls and 12.6 years for boys. (1,2) In SCFE, the metaphysis displaces relative to the epiphysis, which remains in the acetabulum. Most slips are stable. However, 5%–21% are unstable, defined as a patient with severe pain who cannot ambulate even with crutches (3,4). The SCFE diagnosis is made by comparing the slip angle of the affected hip with the contralateral side or to a standard reference. In Sweden, three different methods are commonly used: the calcar femorale method (5); the Billing method (6); and the Head-shaft angle described by Southwick (7). The Southwick method can, in turn, be used both in the anteroposterior (AP) and lateral planes. An adequate lateral radiograph of the hip is the most sensitive projection to diagnose SCFE, especially in mild slips (8). However, the child's pain sometimes only allows for an AP image in unstable slips.
Identifying SCFE as early as possible is essential as early treatment is associated with better clinical outcomes. Hence, children with smaller slip angles score better in patient-reported outcome measures (PROM) (9). Conversely, a delay in diagnosis is associated with increased severity of the slip (4).
Since 2015, all cases of SCFE in Sweden must be reported to a national registry, the Swedish Pediatric Orthopedic Quality Register (SPOQ) (10). The slip angle is one crucial parameter in that register. A previous study has shown good inter- and intra-observer reliability for assessing the slip angle in 77 hip radiographs (11). However, these measurements were made by observers who were specifically trained to analyze the slip angle. Since only 50–60 cases of SCFE occur annually in Sweden, most reporting surgeons have limited experience in measuring the slip angle (2).
The aim of the present study was to evaluate whether any methods to analyze the slip angle were more reproducible than the others. We hypothesized that the reproducibility would differ between the three methods. In addition, the secondary aim was to evaluate the quality of the slip angles reported to the national registry by comparing data with an expert consensus.
Material and Methods
The SPOQ database was used to identify 208 patients registered with SCFE between 2015 and 2020. As the register does not contain the radiographs themselves, all clinics in Sweden treating children with SCFE were asked to send preoperative radiographs to a secured server for validation. Two orthopaedists, observers A and B, were defined as experienced as they work in hospitals regularly dealing with SCFE. These observers independently measured the slip angle twice in random order for the intra-observer analysis. Furthermore, the two experienced observers were blinded to the measurements made by the other observer, radiographic reports, measurement values by the clinicians, information from medical records, and their previous measurements. The values of the second measurement were used for the inter-observer analysis. Finally, a consensus measurement between the two observers was established, and this angle was compared to the angle originally reported by the clinician to the quality register. The measurements were performed according to instructions on the quality register’s website and are shown in Figs. 1–4.
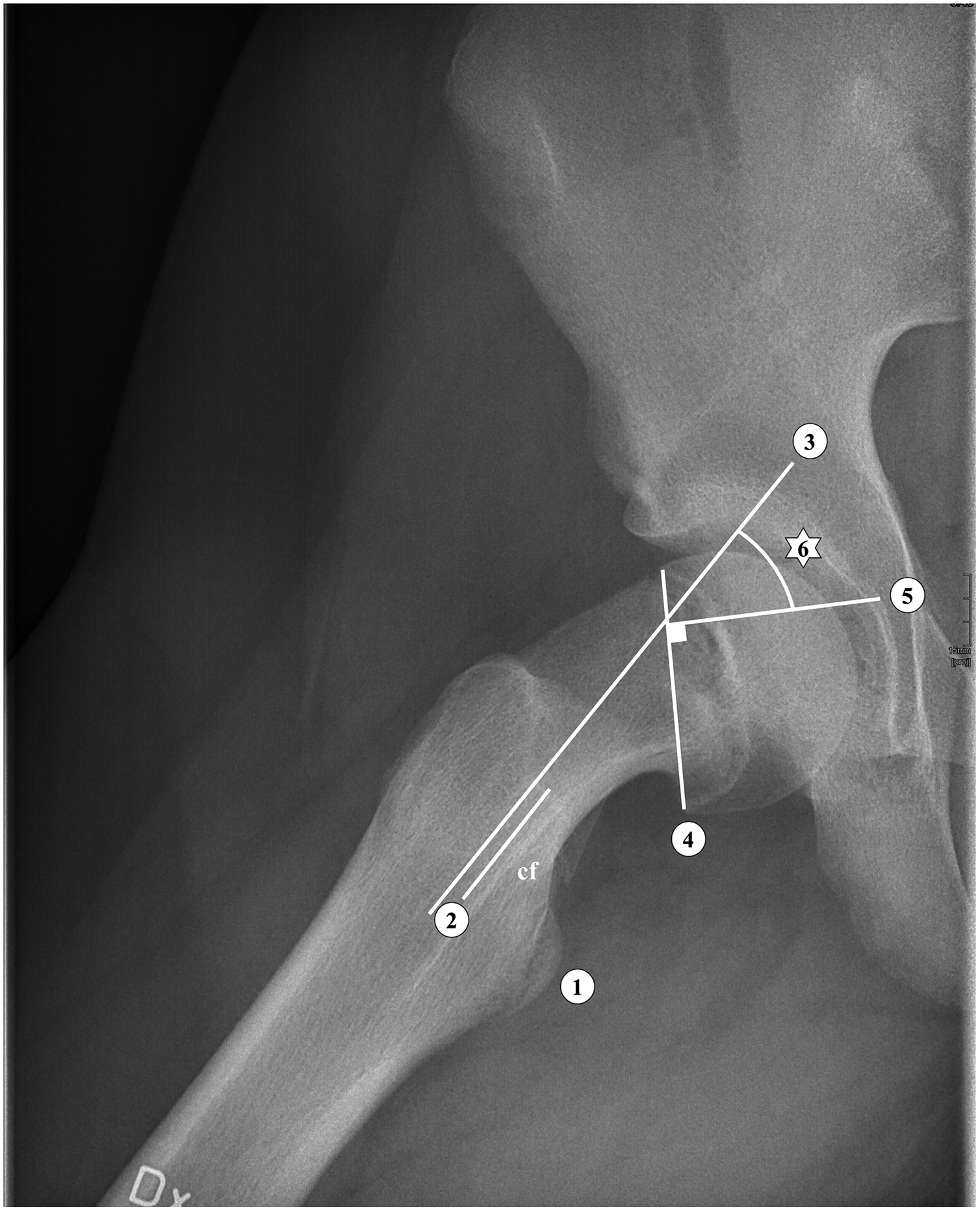
The calcar femorale method. 1: Lesser trochanter. 2: Calcar femorale (cf) line, 3 cm proxmal to 1. 3: Line parallel to 2. 4: Line through the physis. 5: Line perpendicular to 4. 6: Slip angle.
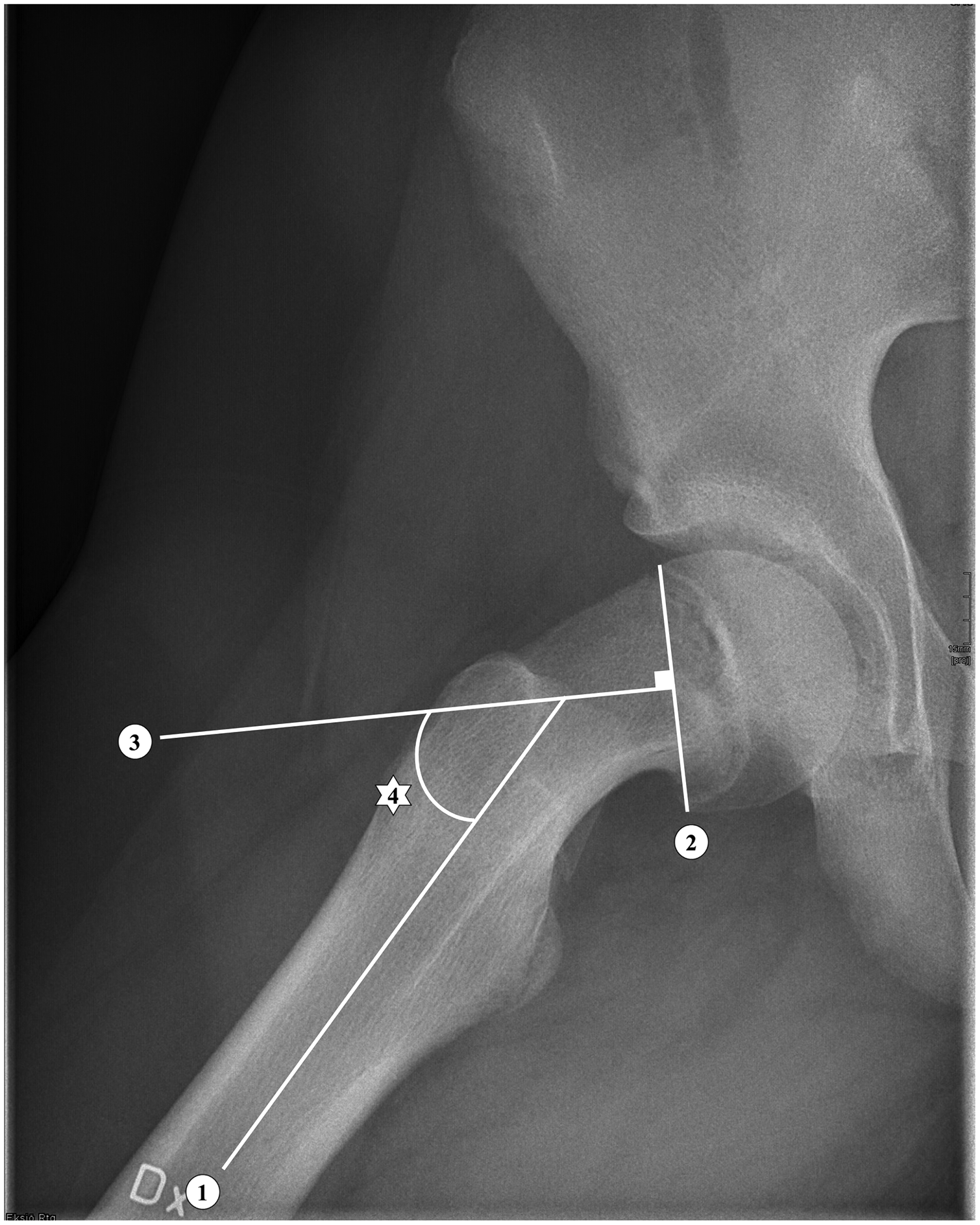
The Southwick lateral method. 1: Line parallel to the diaphysis. 2: Line through the physis. 3: Line perpendicular to 2. 4: Slip angle.
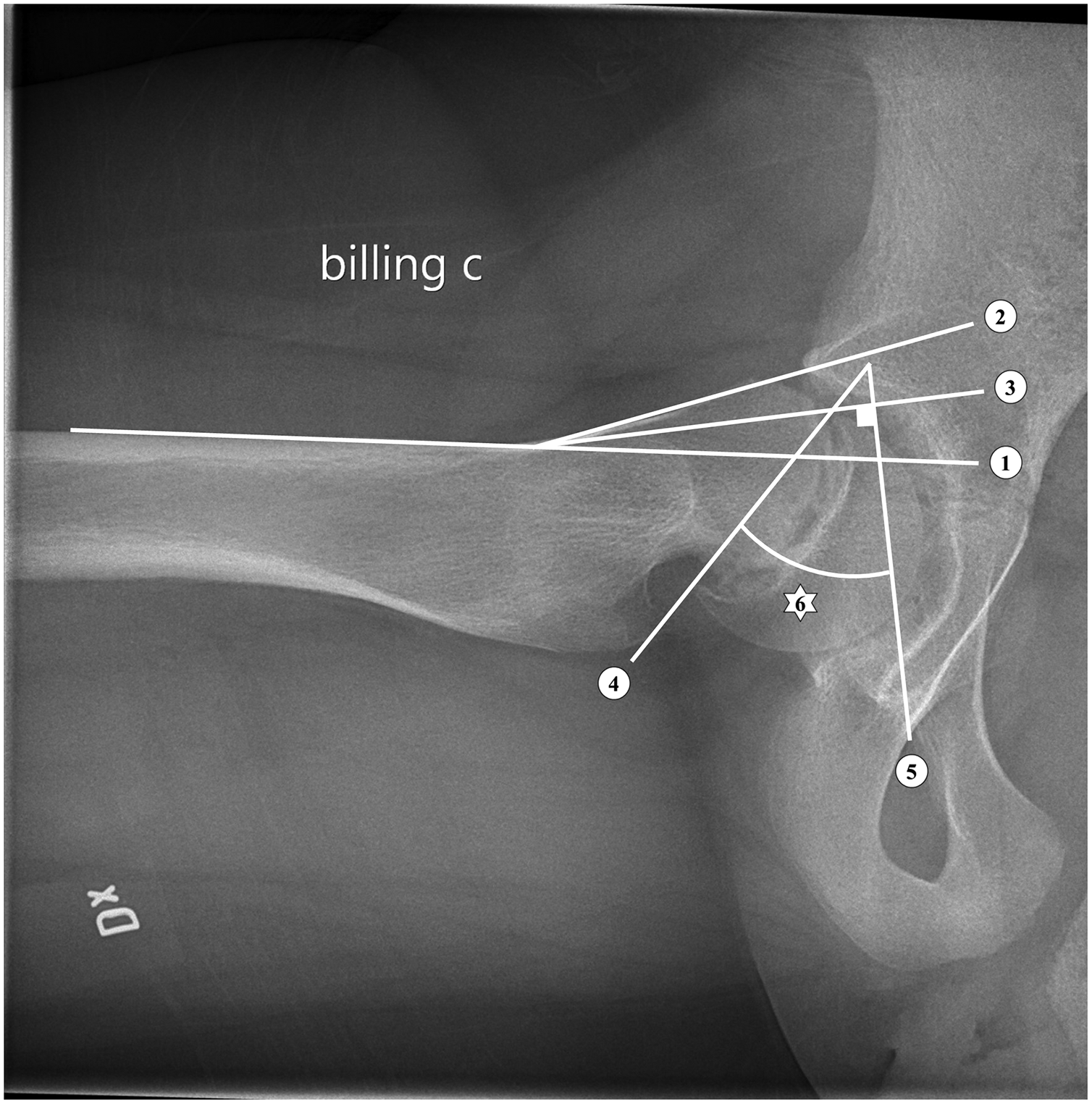
The Billing method. 1: Line parallel to the anterior cortex of femur. 2: Line parallel to the anterior femoral neck. 3: Bisector of 1 and 2. 4: Line through the physis. 5: Line perpendicular to 3. 6: Slip angle.
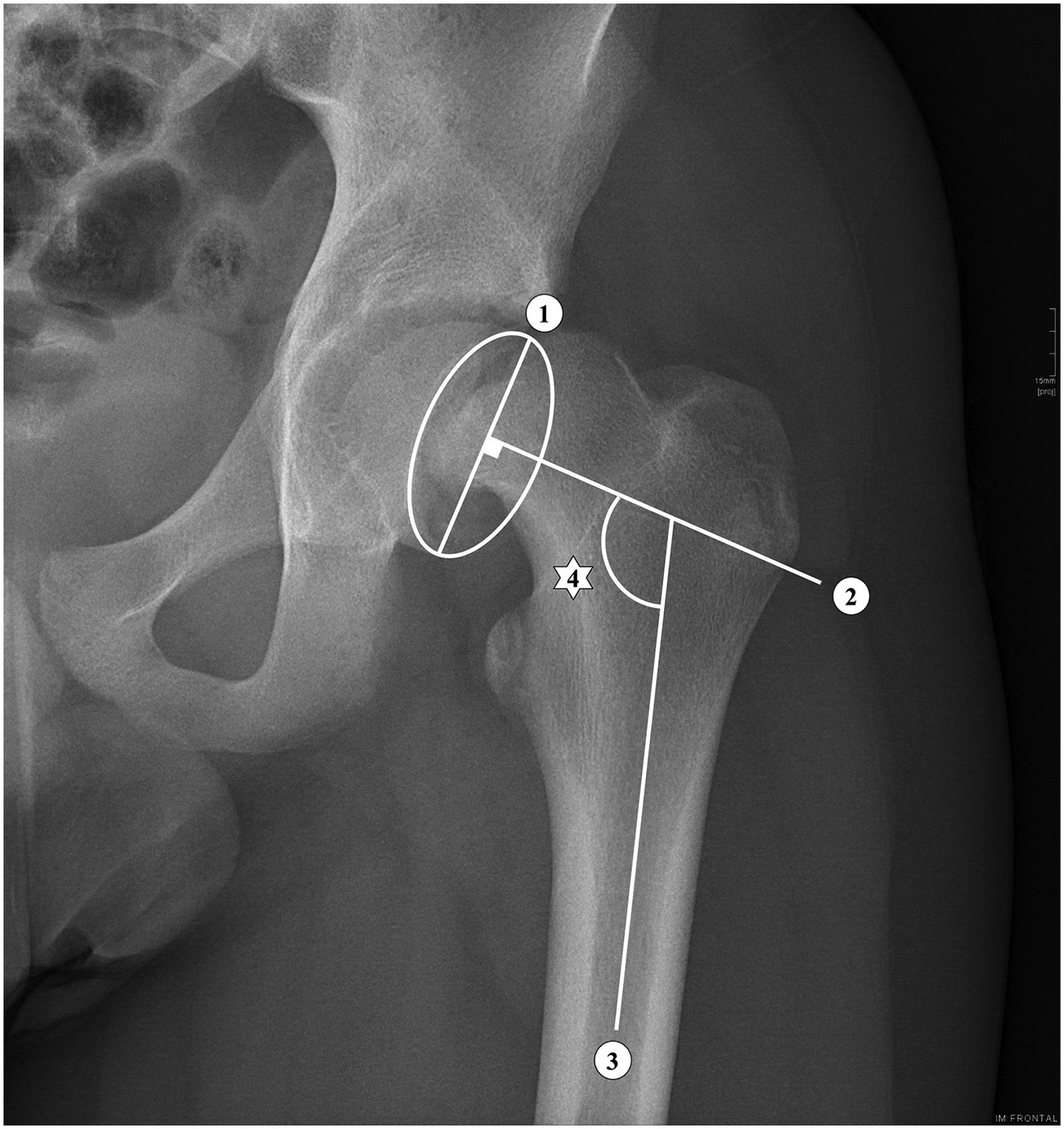
The Southwick AP method. 1: Line through the physis seen as an ellipse. 2: Line perpendicular to 1. 3: Line parallel to the diaphysis. 4: Slip angle.
Statistics
We assumed a normal distribution of data. For the intra- and inter-observer analysis, the intraclass correlation coefficient (ICC) and descriptive statistics were used. In addition, a 95% confidence interval (CI) with a two-way model and absolute agreement for single measures was used. SPSS Statistics for Windows version 27 (IBM Corp., Armonk, NY, USA) was used for all statistical analyses. According to the power analysis (90% power, P = 0.01), we needed 30 radiographs to show a difference of at least 6° between observers.
Ethics
Ethical approval was obtained from the Swedish Ethical Review Authority with diary number 2019-05824.
Results
In total, 208 patients were included (416 hips). There were 182 hips unaffected by SCFE (84 unilateral with prophylactic fixation and 98 unilateral without prophylactic fixation). However, 120 radiographs were not correctly transferred to the server and were excluded from the study. In 16 cases, the registered measurement method did not match the X-ray method of the transmitted radiograph. In five cases, the surgeon did not specify the measurement method. For two children, the slip angle was not reported at all. Thus, there were 91 hip radiographs available for validation (Fig. 5). For the intra- and inter-observer measurements, 125 images could be used as this measurement was not dependent on reported values but merely on transmitted radiographs.
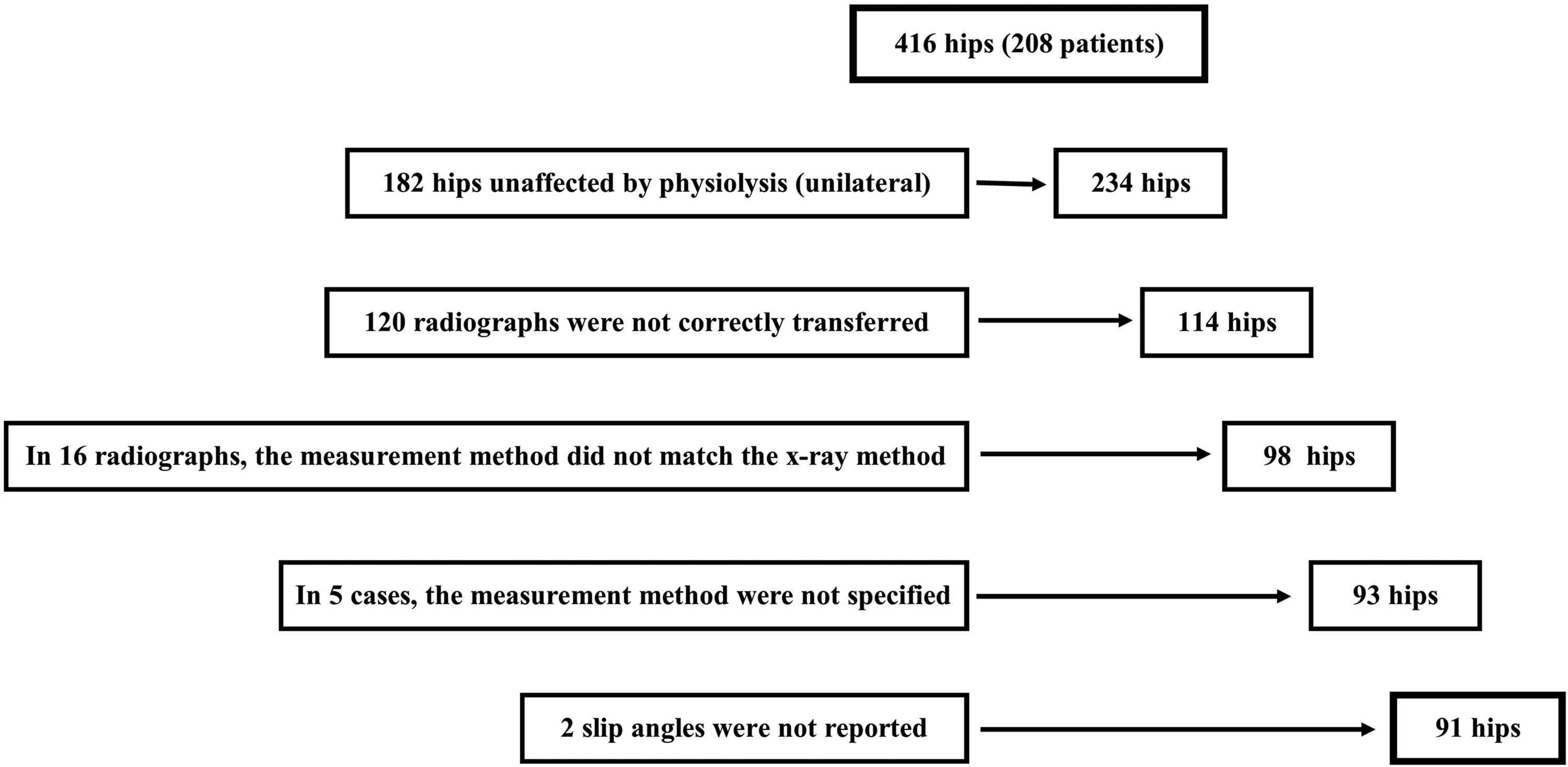
Included radiographs. Excluded hips are shown on the left.
When deciding the consensus angle, the difference between the two experienced observers was 3° in 10 cases and ≤2° in all the other cases. In total, when comparing the reported angle by the clinician with the consensus angle, the correlation according to ICC for the absolute agreement was 0.921 (95% CI = 0.883–0.947). The correlation for each specific method is shown in Table 1. Only one Southwick AP radiograph was validated and therefore excluded in Table 1.
ICC with 95% CI between the two experienced observers and the reporting clinicians for each method.
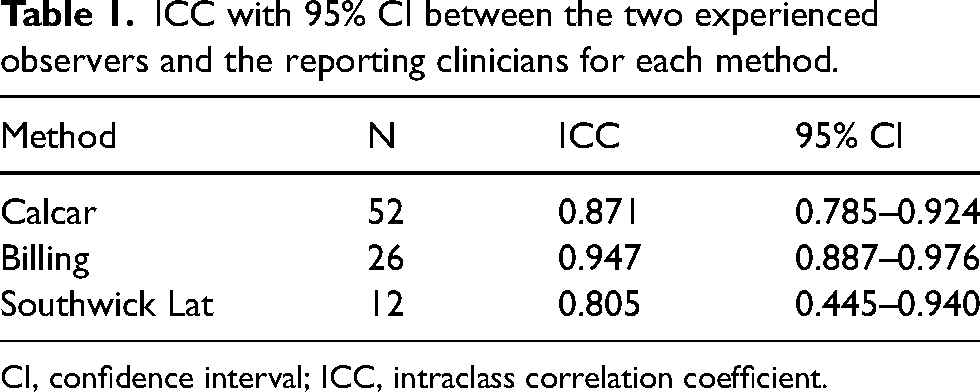
CI, confidence interval; ICC, intraclass correlation coefficient.
The variation between the observers and the initially reported value for each radiograph are shown in Fig. 6. The mean difference was 6° (P < 0.001) and the median value was 3° when comparing the observers’ value with the reported value. In 37% of cases, the difference was more than 5°. The difference exceeded 10° in 16% of the cases.
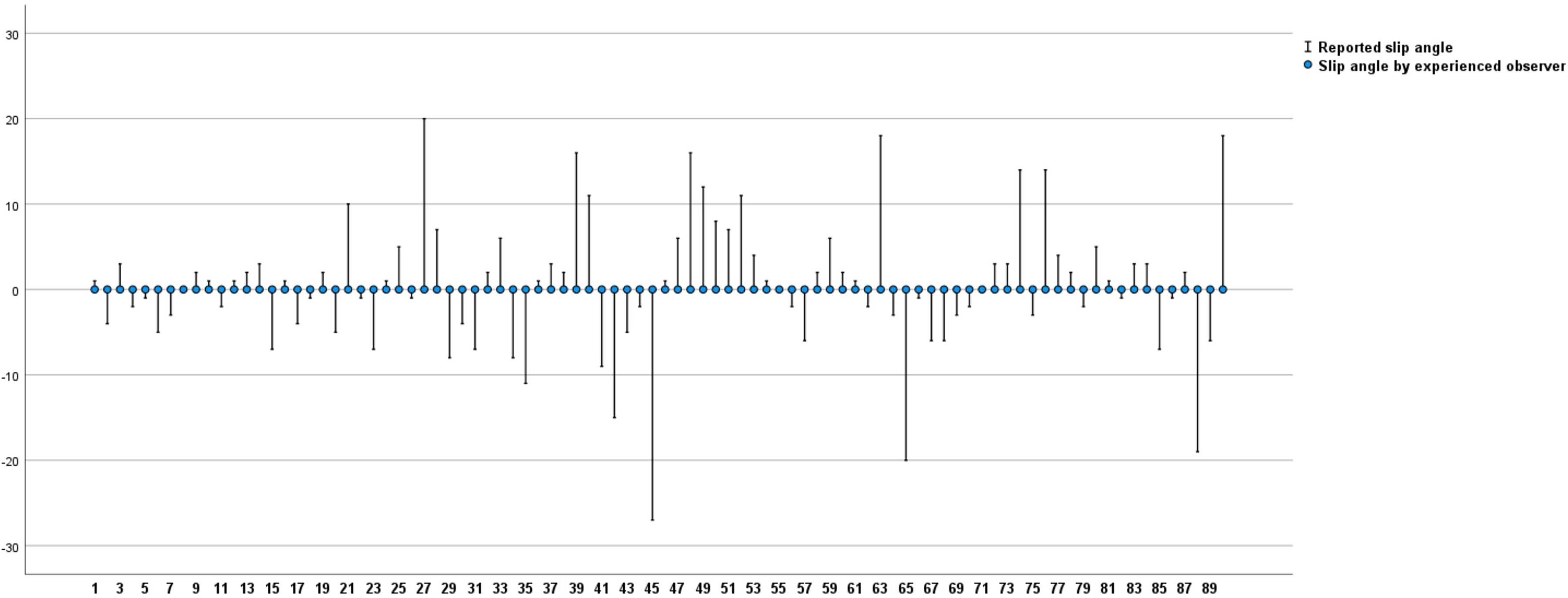
A total of 91 slip angles measured by experienced observers (dots) compared to reported angles (dashes) by clinicians. Variation in degrees in y-axis and radiographs in x-axis.
The intra- and inter-observer variability was very low, as shown in Tables 2 and 3. For example, the difference between the two experienced observers was less than 5° in 97% of the assessments.
ICC with 95% CI between observers A and B in the four different methods of measuring the slip angle.
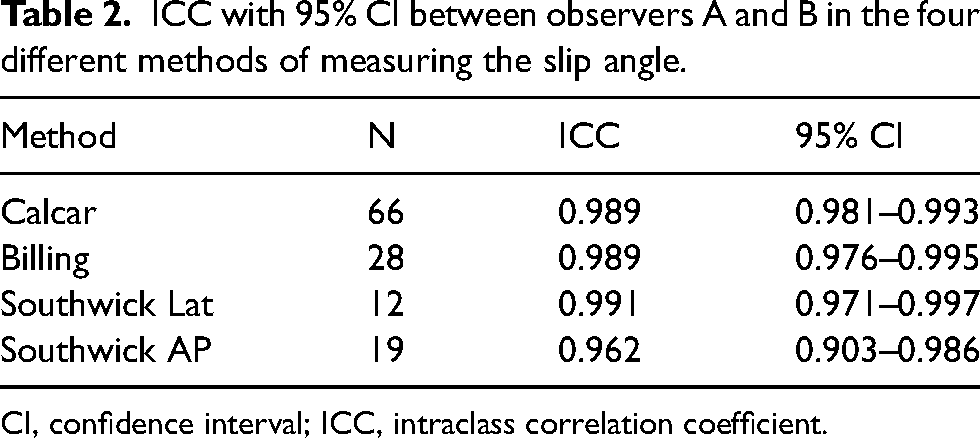
CI, confidence interval; ICC, intraclass correlation coefficient.
Results of the intra-observer analysis for observers A and B.
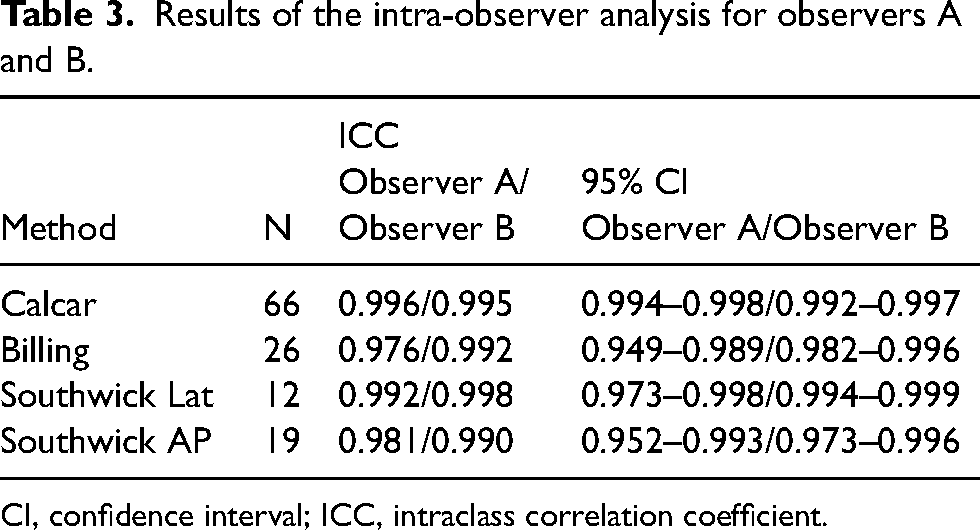
CI, confidence interval; ICC, intraclass correlation coefficient.
Discussion
Slipped capital femoral epiphysis is classified as a rare disorder by ORPHANET (www.orpha.net). Therefore, most orthopaedic surgeons and radiologists are unaccustomed to identifying SCFE radiographically. Moreover, a reliable and reproducible measurement requires practice. However, previous results indicate that inexperienced orthopaedists can achieve good reliability when measuring the slip angle using detailed instructions (11). It is a reasonable requirement that differences of more than 5° should be identified (11).
This is supported in the present study, where both experts demonstrate excellent intra-observer correlation (Table 3). In addition, both experts reported similar slip angles, as illustrated by the good inter-observer correlation (Table 2). Notably, the Southwick AP method should not be used as routine as it is less sensitive than the lateral view to detect minor posterior slips (12). The Southwick AP method should be limited to the rare cases of unstable slips where the child’s pain makes it difficult to use other methods. In stable slips, a frog leg lateral view (Lauenstein) or cross-table lateral must be included.
In all cases, the reported values from orthopaedic surgeons around Sweden did not correlate well with the experts’ measurements, as illustrated in Fig. 6. This is probably related to the fact that most orthopaedic surgeons report few cases to the register. However, we do not think the results reflect a lack of information since clear instructions for each method are provided on the quality register’s website (Figs. 1–4).
A measurement difference of 10° or more (seen in 16% of our cases) could potentially affect the treatment, especially in the mildest and the most severe cases of SCFE. In mild cases, it could influence whether the child is correctly diagnosed with SCFE or not. In severe slips, it could affect the decision to perform capital realignment surgery instead of in-situ fixation. In the current Swedish national treatment guidelines, corrective osteotomy is considered in hips with a slip angle of >50°.
The method of choice did not influence the quality of the reported values since the confidence intervals overlapped between the three major measurement methods (Table 1).
Our results indicate a need to revise the slip angles reported to the national registry. However, since only 50–60 cases are diagnosed in Sweden each year, such analysis should be feasible, perhaps even annually.
From a research and quality point of view, it would be appealing to agree on one method. It could be argued that a CT scan (or magnetic resonance imaging) would be beneficial to assess the degree of slippage in children with SCFE (13). In Sweden, where plain X-ray is the primary imaging modality used to examine children with hip and groin pain, we do not have the data for such analysis. In the future, an increasing use of low-dose CT may facilitate the analysis of the slip angle as well as the deformity in 3D. Several diagnoses may be suspected when a child seeks medical attention for groin, hip, or thigh symptoms. The frog leg lateral view is often used to identify various conditions in a child’s hip. This fact favors the use of the Southwick lateral and the calcar femorale method, which can be applied to the frog leg lateral view.
One study with a femur model in preselected positions showed that the most accurate representation of an SCFE is seen on either cross-table lateral or frog leg lateral view when the external rotation of the femur does not exceed 30°.
On the other hand, the Billing view seemed to exaggerate the degree of slippage (14). The Billing method requires a specific projection that is not routine at most Swedish hospitals. Therefore, despite similar ICC values as the calcar femorale and Southwick AP methods, we cannot recommend the Billing method for universal use. Based on the study results, we instead recommend the calcar femorale method, which can be applied on the commonly used frog leg lateral view. An advantage with the calcar femorale method is that accurate analysis of the slip angle can be done also in images where only the proximal part of the femur is seen on the radiograph. In contrast, the Southwick method requires a larger part of the proximal femur for accurate analysis of the slip angle.
The present study has some limitations. In this study, reported data from all clinics in Sweden treating SCFE have been analyzed. As a result, the degree of coverage and completeness of the Swedish Pediatric Orthopedic Quality register was high. Unfortunately, many radiographs could not be transferred to the secured server and had to be excluded from this analysis. However, according to the performed power calculation, the study dropout did not affect the statistical possibility to draw the conclusions presented in this study. Sharing radiographs between hospitals in Sweden often has to be done in several steps as a plausible explanation for the difficulties we experienced.
In conclusion, the observers' experience is more important than the method of choice when measuring the slip angle in SCFE. However, all methods have good inter- and intra-observer reliability. We recommend the calcar femorale method due to its feasibility on the versatile and commonly used frog leg lateral view. An experienced observer must reanalyze the slip angles reported to the national registry to achieve more accurate data.
Footnotes
Acknowledgments
We thank Bo Rolander, statistician at Futurum – Academy for Health and Care, Jönköping County Council, Sweden; and Futurum – Academy for Health and Care, Jönköping County, Sweden.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Futurum – Academy for Health and Care, Jönköping County Council, Sweden and Erik och Angelica Sparres Forskningsstiftelse.