
Abstract
Symptomatic calcification is an entity in which hydroxyapatite calcific deposits cause inflammation, then burst and dissolve into the surrounding structures. Although a well-known pathologic condition in the rotator cuff tendons, it can also occur in other structures of the locomotor system. Radiographs are usually taken at the initial examination but can also be useful for follow-up evaluation of the course of the calcified matter. Here, we present a case of symptomatic calcification of the lateral collateral ligament of the knee, in which movement of the calcified matter could be observed both by radiography and magnetic resonance imaging as correlated with the clinical symptoms.
Introduction
Symptomatic calcification is an entity in which hydroxyapatite calcific deposits cause inflammation, then burst and dissolve into surrounding structures. Although a well-known pathologic condition in the rotator cuff tendons, it can occur in other structures of the locomotor system as well. It should be considered when a non-traumatic, healthy adult encounters acute severe pain around the attachment of a tendon or ligament. There have been reports of symptomatic calcification in various tendons and ligaments around the knee, including anterior cruciate ligament (ACL), lateral collateral ligament (LCL), and medial collateral ligament (MCL) (1–4). Radiographs are usually taken at first examination but could also be useful for follow-up to evaluate the calcified matter. Here, we present a case of symptomatic calcification of the LCL of the knee, in which the calcified matter moved downward due to gravity into a potential space, likely an acquired bursa, then gradually dissolved. Its course could be observed both by radiography and magnetic resonance imaging (MRI) and correlated with the clinical symptoms.
Case report
A 42-year-old man complained of severe pain in the left knee, which had started several months ago. He had no preceding trauma, regular sport activity or previous relevant medical history. Knee movements were associated with severe pain. Localized swelling and numbness of the lateral aspect of the knee was observed.
The patient first consulted a local orthopedic clinic, due to pain and swelling in the knee. Loss of range of motion (ROM) was also seen due to the pain. A radiograph was taken and revealed a high attenuation area located near the lateral femoral condyle, which continued to the lateral side of the proximal tibia along the course of LCL (Fig. 1). Myositis ossificans, ruptured calcified tendinitis, infected bursitis, or extra-skeletal osteosarcoma was suspected. Three days later MRI was performed to delineate in detail the region surrounding the calcified structures to differentiate these entities. T2-weighted image showed a low signal area located mainly in the proximal portion of LCL. A part of the low signal area continued to the space adjacent to the iliotibial tract. There was edema in the surrounding tissue (Fig. 2). Considering the imaging findings and clinical condition, ruptured calcified tendinitis of the LCL was suspected.

Initial radiograph.

MRI taken after initial radiograph. Coronal T1-weighted image (left), T2*-weighted image (middle), and T2-weighted image (right).
Ten days after the MRI at the local clinic, local steroid injection was performed due to the pain that had persisted for two weeks, but no improvement was obtained, and the patient was referred to our hospital. Although calcifying tendinitis or myositis ossificans was suspected based on the initial radiograph and MRI findings, the intense pain continued unexpectedly with increasing numbness of the lateral aspect of the thigh, associated with loss of the ROM. Physical examination showed a mass at the lateral aspect of the fibular head with redness and spontaneous pain. A radiograph was taken and showed a large high attenuation area downward around the lateral side of the head of the fibula. A second radiograph was taken which showed slit-like calcification with changes in its shape and moving downward compared to the first radiograph (Fig. 3). A second MRI was performed one week after the second radiograph to confirm the diagnosis of ruptured calcifying tendinitis and evaluate where the primary lesion existed. Another aim was to rule out any co-existent conditions or infective complications. There was a low signal in the LCL area with edematous change of the surrounding soft tissue corresponding to the high attenuation area noted on the radiograph (Fig. 4). A follow-up radiograph was taken six weeks after the second MRI. By this time, the pain and loss of ROM had subsided. The high attenuation area almost vanished beside the calcified nodules at the insertion point of the lateral femoral condyle of the LCL (Fig. 5).

Second radiograph taken three weeks later.
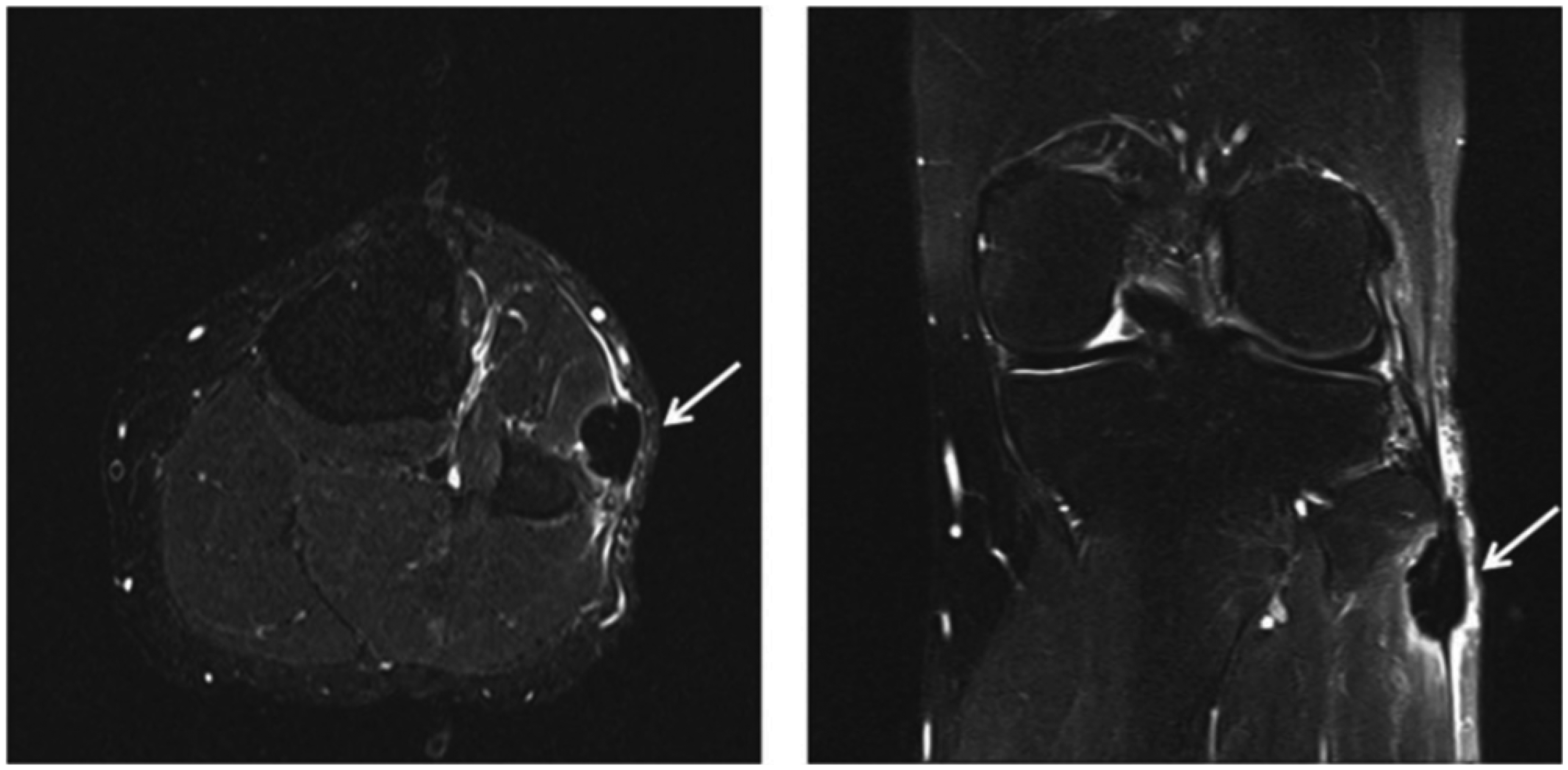
MRI taken after second radiograph. Axial and coronal STIR.

Third radiograph taken three months later.
The most probable hypothesis is that some calcified matter developed a liquid-like feature (so-called “milk of calcium”) induced by inflammation and ruptured causing severe pain. This could have happened in a bursa nearby since the LCL itself usually does not and cannot contain such a space. After rupture, the calcified matter likely moved downward due to gravity and into a potential space such as an acquired bursa, and then gradually dissolved, which is consistent with the timing of the decrease in pain. Puncture was not performed for this patient, and our hypothesis is not proved pathologically. At one-year follow-up, no recurrence was evident on MRI (not shown). The patient gained a full ROM with no pain and he was able to comfortably perform his routine activities.
Discussion
Symptomatic calcification occurs from the deposition of calcium hydroxyapatite crystals at the attachment sites of ligaments and tendons causing severe pain and disability. However, its pathogenesis is not fully understood. Codman (4) initially proposed that degeneration of tendon fibers precedes dystrophic calcification and hypothesized that the fibers of the tendon are degenerated and necrotic and then develop dystrophic calcification. Uthoff (5) also suggested that “wear and tear” due to overuse and aging results in degeneration of tendon fibers. Sherman (6) concluded that the factors causing degenerative remain elusive, because some cases did not manifest any evidence of them.
However, most of the earlier literature is based on cases with involvement of the rotator cuff, it being the most common site. Therefore, one should keep in mind that symptomatic calcification occurring in other areas may have some different features and pathogenesis. For the pathogenesis of symptomatic calcification, according to Mosley et al. (7) there are three phases: (i) silent phase; (ii) mechanical phase; and (iii) phase of adhesive periarthritis:
The silent phase occurs in which the calcium deposit is completely contained within the tendon. This phase corresponds radiographically to sharply defined, circumscribed deposits, which, if removed, would appear as inspissated granular or cheesy material. The mechanical phase is characterized by enlargement of the deposits, followed by impingement like symptoms. The deposits become liquified, leading to increased pressure and bursitis. At this stage, the radiographic appearance of the deposit is less well defined, but the deposit is still present within the tendon. Recurrent attacks of bursitis generally lead to rupture of the deposit, either subbursal of intrabursal. The evacuation of the calcium deposit may not be complete. This later stage is characterized by painful attacks. On radiographs, the calcification may show dispersion into the bursa. Disappearance of calcification is frequent and may or may not correspond to the clinical course. The phase of adhesive periarthritis is characterized by general debility, pain, and limitation of motion. Calcium deposits may evacuate with treatment.
The knee area, like other joint areas, includes many native bursas (subcutaneous, synovial, and sub-muscular) and acquire adventitious bursas too. The major native bursas in which bursitis is known to particularly occur are: suprapatellar; subcutaneous prepatellar; subcutaneous and deep infrapatellar bursa in the anterior region; subsartorial (pes anserinus) bursa in the medial region; semimembranosus bursa in the posterior region; and gastronemius and popliteus bursa in the lateral region. However, in our case, anatomical confirmation was not possible based on the MRI findings, and since no major native bursa follows the LCL, we speculated that a calcified material ruptured into a potential space such as an acquired bursa between the LCL and iliotibial tract.
In conclusion, LCL is a rare location for symptomatic calcification. We here report this case in which we could observe the dynamic changes in the distribution of calcified matter and its acute process in milk of calcium, as correlated with changes in pain, which likely occurred due to gravity and the anatomical presence of a potential space.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.