
Abstract
Background
Computed tomography angiography (CTA) is a reliable, non-invasive screening method for diagnosing panvascular disease. By using low contrast agent volume, CTA imaging enables one-stop multi-organ scanning, thereby minimizing the potential risk of contrast-induced nephropathy in patients with impaired renal function.
Purpose
To evaluate the feasibility of one-stop CTA following a heart rate (HR)-based protocol using a low volume of contrast medium (CM) for examination of the coronary, carotid and cerebrovascular arteries.
Material and Methods
Sixty patients undergoing coronary carotid, and cerebrovascular CTA after a single injection of CM were recruited and randomly divided into two groups. Group A (n = 30) underwent CTA following a traditional protocol. The timing of the scans in Group B (n = 30) was determined according to the patient's HR.
Results
The CT values for the thoracic aorta (432.2 ± 104.28 HU), anterior cerebral artery (303.96 ± 99.29 HU), and right coronary artery (366.70 ± 85.10 HU) in Group A did not differ significantly from those in Group B (445.80 ± 106.13, 293.73 ± 75.25 and 344.13 ± 111.04 HU, respectively). The qualities of most of the scanned images for both groups were scored as 3 or 4 (on a five-point scale). The radiation dose and the volume of CM were significantly higher in Group A (303.05 ± 110.95 mGy) (100 mL) than in Group B (239.46 ± 101.12 mGy) (50 mL).
Conclusion
The radiation dose and volume of CM were significantly reduced in CTA following the HR-based protocol. The personalized administration of CM also simplified the scanning process.
Keywords
Introduction
With continued economic development and improvement of living standards, the incidence of vascular diseases in China has increased in recent decades. Cardio-cerebral vascular diseases, including cerebrovascular disease, carotid disease and cardiovascular diseases, are the leading causes of death nationwide. The coexistence of these diseases has been observed using different imaging modalities (1–3), including multi-detector computed tomography angiography (CTA), Doppler ultrasonography and digital subtraction angiography (3–7). Multi-detector CTA is superior to conventional digital subtraction angiography for the diagnosis of vascular diseases, as a result of the following advantages: non-invasiveness, short acquisition time, multiple viewing methods and directions, low cost, and lower radiation dose (7). CTA has become as a reliable tool for the diagnosis of atherosclerotic disease and the characterization of carotid artery plaques, showing high concordance with histological results (8,9). CTA has also been considered an ideal imaging examination for the detection of coronary artery stenosis (10–15) and the significance of CTA in the detection of ischemic cerebrovascular diseases has been highlighted (16,17).
However, the benefits of CTA must be weighed against the potential risks associated with contrast media and radiation exposure. In the retrospective electrocardiogram-gated spiral acquisition mode, a radiation dose of 12 mSv in coronary CTA (CCTA) has been reported (18). Patients who are suspected of having panvascular disease require combined imaging of multiple vessels, such as coronary, carotid/cerebral or coronary arteries, and thoracic and abdominal aorta. A higher cumulative radiation dose is expected when patients undergo CTA for coronary, carotid and cerebrovascular arteries, all following this protocol. Additionally, the use of iodinated contrast media in CTA may cause renal impairment (19). The reported incidence of acute kidney injury after intravenous contrast media has been reported to range between 2% and 35% (20). The 16-cm wide-detector Revolution CT scanner (GE Healthcare, Chicago, IL, USA) enables the performance of one-stop imaging of an entire organ (e.g. heart, brain, parenchymal viscera and cavity viscera) (21).
The present study aimed to evaluate the feasibility of using low-dose contrast media in one-stop CTA of coronary, carotid and cerebrovascular arteries. In a control group (Group A), the test bolus technique was used to determine the delay between the initiation of coronary CTA and carotid-cerebrovascular CTA, whereas, in Group B, the delay between the initiation of coronary CTA and carotid-cerebrovascular CTA was determined according to the heart rate (HR) of the patient. The CT values for the thoracic aorta, anterior cerebral artery and right coronary artery, as well as the radiation dose and volume of contrast agent, were compared between the two groups.
Material and Methods
Study participants
In total, 60 patients who were suspected of having cardio-cerebral vascular diseases and for whom coronary and carotid-cerebrovascular CTA with a single injection of contrast agent was planned were recruited. They were randomly divided into two groups (Group A and Group B, n = 30 patients per group) and underwent CTA following different protocols. This study was approved by the Ethics Committee of Liaocheng People's Hospital (approval number: 2018063), all methods were performed in accordance with the relevant guidelines and regulations. All participants provided their written informed consent prior to enrollment.
CT examination
The American GE256 row 512-slice spiral CT scanner (GE Healthcare) was used for CT examination. The scan parameters were: X-ray tube rotation speed: 0.28 s/r; tube voltage: 120 kV, baseline voltage: 100 kV; tube current: 150–650 mA; NI: 20; 50% ASiR-V. The detector covered 12–14 cm. The thickness of the section was 0.62 mm. The window width and window location were 800 HU and 180 HU, respectively. Images were then transmitted to the workstation (AW461) via a PACS (i.e. picture archiving and communication system).
CT scanning protocols
Patients in Group A (n = 30) underwent CTA following a traditional protocol. The test bolus technique was used to determine the delay between the initiation of coronary CTA and carotid-cerebrovascular CTA (ΔT) by an injection of 20 mL of contrast agent. First, a small dose (20 mL) of contrast agent was injected to determine the peak time of the carotid, cerebrovascular and coronary arteries in each patient. The delay between the initiation of carotid-cerebrovascular CTA and coronary CTA was determined by setting the ascending aortic threshold as 120 HU, with an injection of 80 mL of contrast agent at a rate of 5 mL/s.
Patients in group B (n = 30) received an injection of 50 mL of contrast agent at a rate of 5 mL/s and underwent CTA without a test bolus. The timing of the scans was determined according to the HR of the patient: (1) HR >80 beats/min: CCTA started 9–12 s after the injection of contrast agent and the delay between the initiation of carotid-cerebrovascular CTA and coronary CTA was 4 s; (2) HR = 60–80 beats/min, CCTA started 13–16 s after the injection of contrast agent and the delay between the initiation of carotid-cerebrovascular CTA and coronary CTA was 6–8 s; (3) HR <60 beats/min , CCTA started 18–21 s after the injection of contrast agent and the delay between the initiation of carotid-cerebrovascular CTA and coronary CTA was 11 s. A total of 50 mL of contrast medium was used for each patient in this group. Carotid-cerebrovascular CTA was performed following a helical scan protocol, whereas coronary CTA was performed following an axial protocol.
The scanning and reconstruction parameters of the two groups were the same. Drugs with the potential to alter heart rate, such as beta blockers and nitrate, were not used in the study.
Image evaluation
The radiologists who evaluated the image quality were blinded to the study design. The CT values (HU) for the thoracic aorta, anterior cerebral artery and right coronary artery were measured and compared between the two patient groups (Table 1). Two experienced radiologists evaluated the quality of each image using a five-point scale (Fig. 1 and Table 2): 1, did not meet the requirement for diagnosis; 2, poor quality; 3, basically met the requirement for diagnosis; 4, good quality; and 5, high quality. The radiation dose and the volume of contrast agent were recorded.
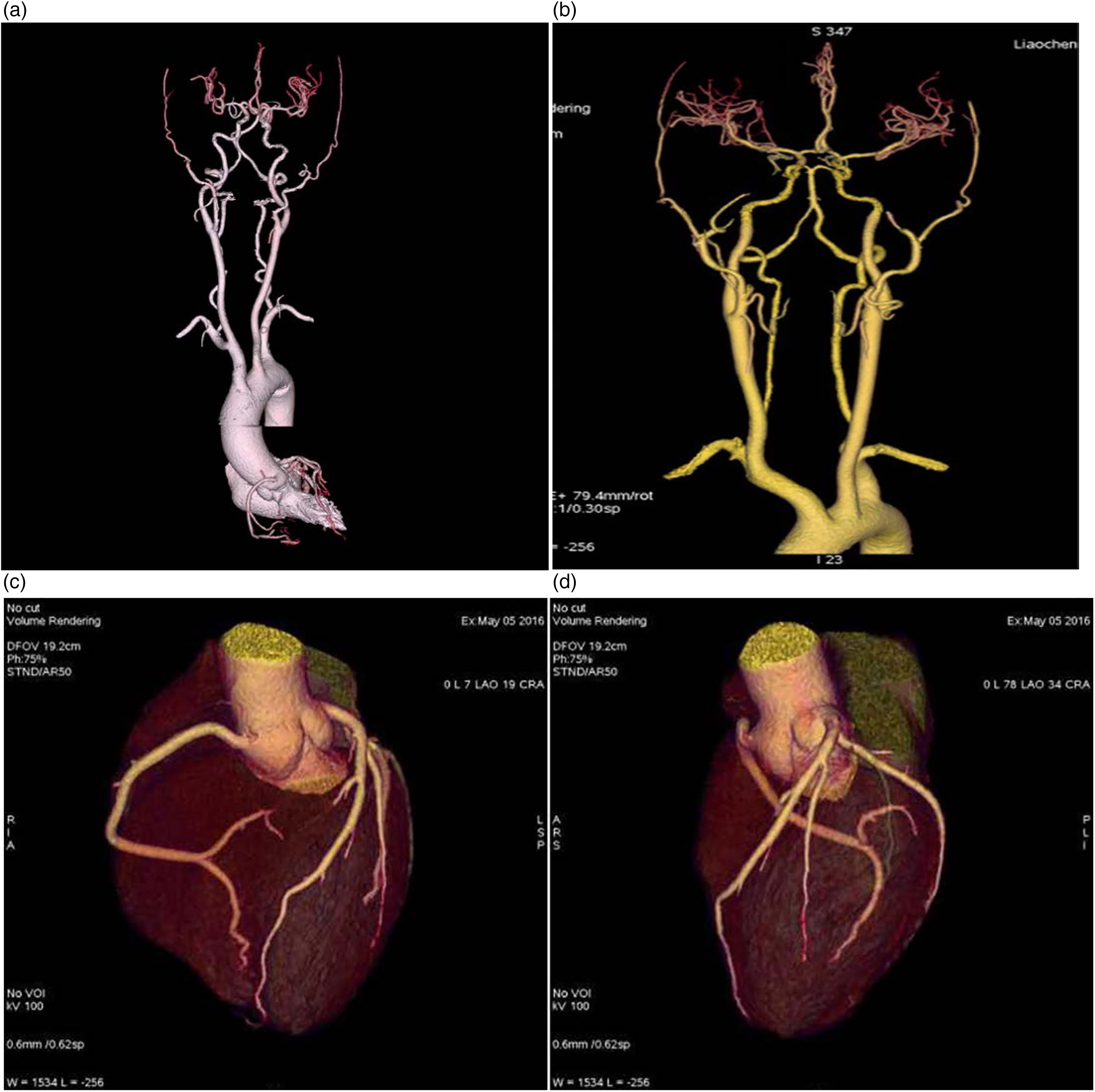
Imaging of carotid, cerebrovascular, and coronary arteries of one patient using one-stop computed tomography angiography (CTA) following the heart rate (HR)-based protocol. (a) Anterior view of coronary, cerebral and carotid arteries. (b) Anterior view of cerebral and carotid arteries. (c) Anterior view of coronary arteries. (d) Left lateral view of coronary arteries. The delay between the initiation of carotid-cerebrovascular CTA and coronary CTA was determined according to the HR of this patient.
Demographic and clinical data of the two groups at baseline.
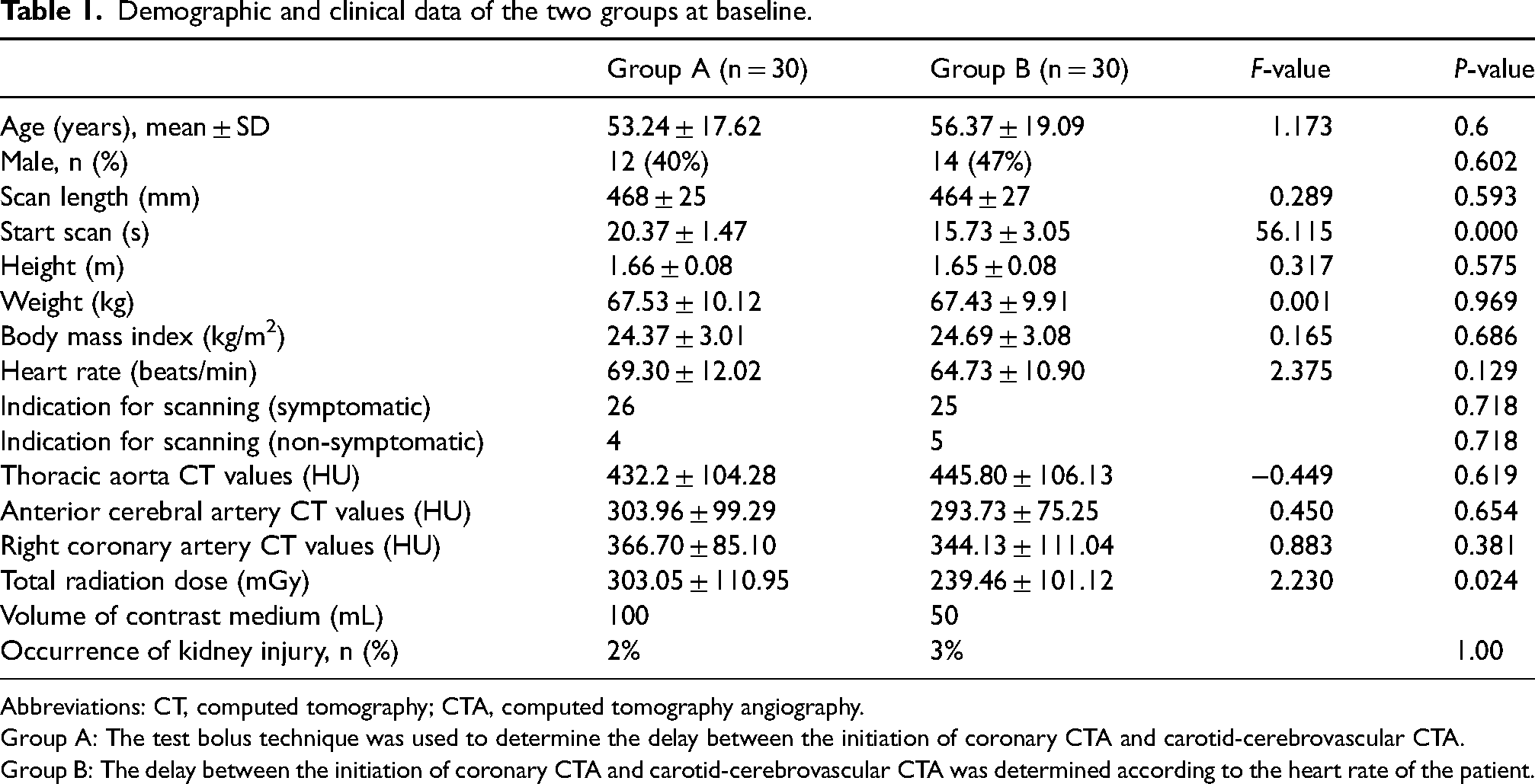
Abbreviations: CT, computed tomography; CTA, computed tomography angiography.
Group A: The test bolus technique was used to determine the delay between the initiation of coronary CTA and carotid-cerebrovascular CTA.
Group B: The delay between the initiation of coronary CTA and carotid-cerebrovascular CTA was determined according to the heart rate of the patient.
Image quality in the two groups.
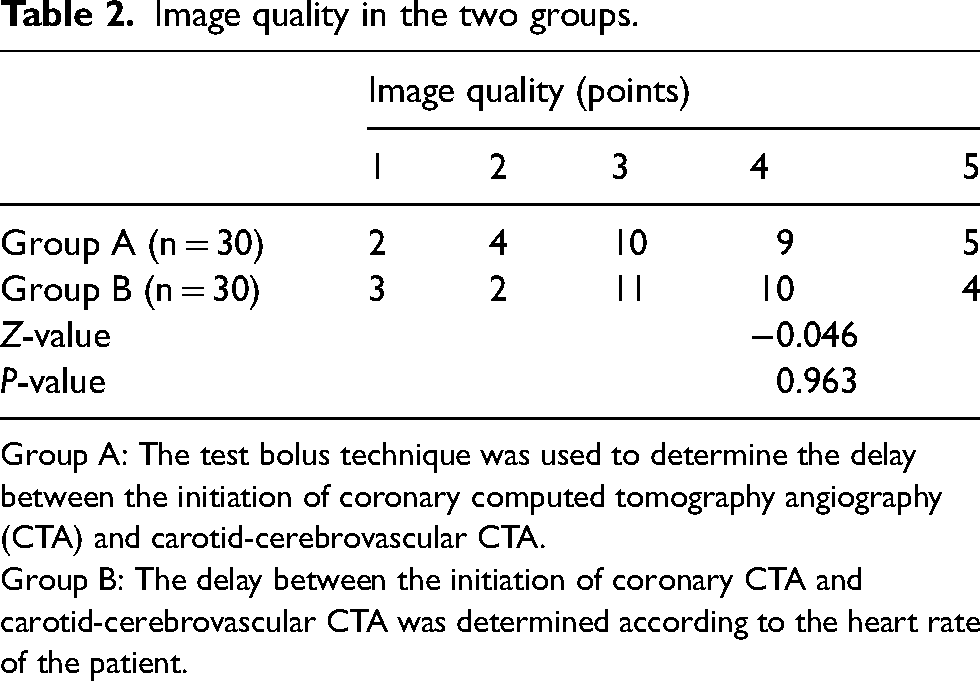
Group A: The test bolus technique was used to determine the delay between the initiation of coronary computed tomography angiography (CTA) and carotid-cerebrovascular CTA.
Group B: The delay between the initiation of coronary CTA and carotid-cerebrovascular CTA was determined according to the heart rate of the patient.
Statistical analysis
Statistical analysis was performed using SPSS, version 15.0 (SPSS Inc., Chicago, IL, USA). The Kolmogorov–Smirnov normality test was used to assess the normality of quantitative variables. All quantitative variables were normally distributed and therefore expressed as mean ± SD. Student's t-test was used to identify differences between groups. Qualitative variables were described as n (%) and the chi-squared test was used for group comparison. The rank-sum test was used to compare the scores for image quality between the two groups. P < 0.05 was considered statistically significant.
Results
Demographic and clinical characteristics of the patients
Group A included 12 males and 18 females, with a mean ± SD age of 53.24 ± 17.62 years (range 16–84 years). Group B consisted of 14 males and 16 females, with a mean ± SD age of 56.37 ± 19.09 years (range 15–84 years). The numbers of symptomatic patients with clinical indications for CT scanning were 26 and 25 in Group A and Group B, respectively.
There were no significant differences in the scan length, height, weight, body mass index and HR of patients between Group A and Group B. The time of the start scan in Group A (15.73 ± 3.05 s) was less than that in Group B (20.37 ± 1.47 s) (Table 1).
CT values of arteries following different scanning protocols
All scans were performed using the same parameters. The thoracic aorta, anterior cerebral artery and right coronary artery of 60 patients (n = 30 per group) were used as standards. In Group A, the thoracic aorta showed the highest average CT value (432.2 HU), whereas the anterior descending artery showed the lowest value (303.96 HU). In Group B, the thoracic aorta had the highest average CT value (445.8 HU), whereas the anterior cerebral artery had the lowest value (293.7 HU), suggesting that the images obtained in Group B also were of sufficient quality for clinical diagnosis. There were no significant differences in the CT values for the thoracic aorta, anterior cerebral artery or right coronary artery between the two groups (P > 0.05) (Table 1).
Radiation dose, volume of contrast medium and complication
The radiation dose in Group A (303.05 ± 110.95) was significantly higher than that in group B (239.46 ± 101.12; P = 0.024) (Table 1). The volume of contrast medium was also higher in Group A (100 mL) than in Group B (50 mL). The incidence rate of kidney injury was 2% in Group A and 3% in Group B (P > 0.05).
Image quality achieved with different scanning protocols
A five-point scale was used to evaluate the quality of CT images. The majority of the images in both groups were scored as 3 and 4, suggesting that they were of sufficient quality for clinical diagnosis. The quality scores for the scanning images did not differ significantly between the two groups (P > 0.05) (Table 2).
Discussion
In total, 50–100 mL of CM is used for one organ in traditional CTA. CTA for patients with panvascular disease requires combined scanning for vascular imaging of multiple organs. In the present study, a total of 30–70 mL of CM in a single injection was used for each patient for combined scanning of multiple vessels, including the combined scanning of coronary, coronary and pulmonary arteries, coronary and carotid/cerebral arteries, coronary and carotid/cerebral, thoracic, abdominal aorta, coronary and carotid/cerebral, thoracic, abdominal, and lower extremity arteries.
The corresponding CM volumes for these combined scans were 18 mL (9), 30 mL (22), 50 mL, 60 mL and 70 mL, respectively. Compared with the traditional CTA, the HR-based protocol significantly reduced the amount of CM used, which might decrease the risk of contrast-induced acute kidney injury in patients with impaired renal function (9,22).
The combined scanning of coronary and carotid/cerebral arteries is a part of the combined scanning for panvascular disease. In this study, patients who underwent combined CTA imaging were divided into three groups according to HR: > 90 beats/min, 60–90 beats/min, and <60 beats/min. Personalized scanning protocols were then applied to patients with different HRs. The HR-dependent CM injection protocol significantly reduced the amount of CM used and simplified the work-flow (9,22). In the traditional scanning protocol, a high-pressure injector was used to continuously inject the CM, and the dose of CM was kept at a high level during the scanning period. The overuse of CM not only increases the metabolic burden of the kidney, but also may induces kidney damage.
In the study by Bjerrum et al. (23), more than half of the middle-aged, apparently healthy individuals had subclinical atherosclerosis located in the coronary, carotid or cerebrovascular arteries. Coronary and carotid-cerebrovascular CTA greatly facilitates the diagnosis of atherosclerosis. The visualization of atherosclerotic plaques in the coronary, carotid and cerebrovascular arteries using CTA may refine the risk-stratification of this population (24). The one-step CTA with a single injection of contrast agent could be used for comprehensive assessment of the coronary, carotid and cerebrovascular arteries (25). It may detect atherosclerosis in different vessels in one scanning process, which is beneficial for high-risk populations, such as patients with familial hypercholesterolemia (26). The delay between the initiation of the coronary CTA and carotid-cerebrovascular CTA was determined according to the HR of each individual, which reduced the radiation dose and the volume of contrast agent without compromising the quality of the scanning images.
Patients of different ages and with differing body mass index values may have different HRs. The HR of elderly patients with arrhythmia or other diseases may vary significantly. The HR also varies in patients with congenital heart disease (22). Some previous studies have reported that the HR-based scanning protocol was superior to the test bolus technique (9,22). CTA has become a reliable diagnostic tool for atherosclerotic disease and exhibits high concordance with the results of histological examination for carotid artery plaques (9). Therefore, combined head, neck and coronary CTA is essential for the early diagnosis and timely treatment of patients with cardio-cerebral diseases.
In the present study, combined CTA for carotid, cerebrovascular and coronary arteries was performed using 50 mL of contrast agent, which was significantly lower than the doses of 90 mL used by Furtado et al. (27) and 60 mL used by Sun et al. (28), but slightly higher than the dose of 40 mL used by Zhao et al. (29). The quality of the scanning images was not compromised. The CT values for the thoracic aorta, anterior cerebral artery and right coronary artery obtained in this study were consistent with those published previously (30,31).
Moreover, all coronary arteries were examined by prospective electrocardiogram-trigger CCTA, which significantly decreased the radiation dose (256.3 mGy N cm) compared to that required for the combined scans reported as 360 mGy N cm by Tognolini et al. (32) and as 484.23 mGy N cm by Zhang et al. (33). Notably, the radiation dose was significantly higher in Group A than in Group B (303.05 ± 110.95 vs. 239.46 ± 101.12; P = 0.024) (Table 1), which may be attributed to the inclusion of a small bolus test, involving an additional scan step, in Group A. One limitation of the present study is that the degree of renal toxicity was not compared between the two groups.
In conclusion, personalized, HR-based administration of contrast agent for CTA allowed the use of a reduced radiation dose and lower contrast medium volume without compromising the quality of the scanning images and also simplified the scanning process.
Footnotes
Author contributions
Peiji Song, Hairong Yu and Tiangang Song were responsible for study concepts and design. Hao Song and Xiaonan Sun were responsible for the literature research. Jie Zhao, Taiyang Zuo and Lihua Jing were responsible for clinical studies. Hairong Yu and Hao Song were responsible for experimental studies/data analysis. Hairong Yu, Hao Song, Jianghua Xu, Ruiying Qin, Anming Xie and Peiji Song were responsible for the statistical analysis. Hairong Yu and Hao Song were responsible for manuscript preparation. Peiji Song, Hairong Yu, Hao Song, Zengkun Wang, Huijing Chai, Xiaomei Luan and Yuanzhen Zhao were responsible for manuscript editing. Peiji Song is the guarantor of integrity of the entire study.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics approval
This study was approved by the Ethics Committee of the Liaocheng People's Hospital (approval number: 2018063, date of the approval: July in 2018), all methods were performed in accordance with the relevant guidelines and regulations.
Consent to participate
Informed consent was obtained from all patients.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received the following financial support for the research, authorship, and/or publication of this article: This research was supported by four institutions: the Jinan Clinical Medical Science and Technology Innovation Program Project (202019133), the Jinan Central Hospital's 2020 First-batch Research Fund for Introducing Talents (YJRC2020005), the Jinan Government 5150 Project for innovative Talents, and Medical and Health Science and Technology Development Plan Project of Shandong Province (202209010494).