
Abstract
Background
Positron emission tomography (PET) using fluor-18-deoxyglucose (18F-FDG) with or without computed tomography (CT) is generally accepted as the most sensitive imaging modality for diagnosing recurrent differentiated thyroid cancer (DTC) in patients with negative whole body scintigraphy with iodine-131 (I-131).
Purpose
To assess the potential incremental value of ultrasound (US) over 18F-FDG-PET-CT.
Material and Methods
Fifty-one consecutive patients with suspected recurrent DTC were prospectively evaluated using the following multimodal imaging protocol: (i) US before PET (pre-US) with or without fine needle biopsy (FNB) of suspicious lesions; (ii) single photon emission computed tomography (≥3 GBq I-131) with co-registered CT (SPECT-CT); (iii) 18F-FDG-PET with co-registered contrast-enhanced CT of the neck; (iv) US in correlation with the other imaging modalities (post-US). Postoperative histology, FNB, and long-term follow-up (median, 2.8 years) were taken as composite gold standard.
Results
Fifty-eight malignant lesions were identified in 34 patients. Forty lesions were located in the neck or upper mediastinum. On receiver operating characteristics (ROC) analysis, 18F-FDG-PET had a limited lesion-based specificity of 59% at a set sensitivity of 90%. Pre-US had poor sensitivity and specificity of 52% and 53%, respectively, increasing to 85% and 94% on post-US, with knowledge of the PET/CT findings (P < 0.05 vs. PET and pre-US). Multimodal imaging changed therapy in 15 out of 51 patients (30%).
Conclusion
In patients with suspected recurrent DTC, supplemental targeted US in addition to 18F-FDG-PET-CT increases specificity while maintainin sensitivity, as non-malignant FDG uptake in cervical lesions can be confirmed.
Introduction
Differentiated thyroid cancer (DTC), the most common malignant endocrine tumor, generally has a favorable prognosis (1). Some patients, however, experience adverse outcomes despite improvements in preoperative imaging and surgical techniques (2,3).
In most patients with recurrent disease after previous total thyroidectomy with or without subsequent ablative radioiodine therapy (RIT), serum human thyroglobulin (hTg) will be detectable as a tumor marker. Conventional imaging including cervical ultrasound (US) and computed tomography (CT) is negative in many cases. Additional tumor lesions may be detected by iodine-131 (I-131) scintigraphy, particularly after application of a therapeutic activity of I-131 (4). In selected patients, I-131 therapy may be curative (5). In many patients, however, tumor lesions cease to take up relevant amounts of iodine. In a seminal paper in 1996, Feine showed that positron emission tomography (PET) with fluor-18-deoxy-glucose (FDG) demonstrated thyroid cancer lesions undetectable by I-131-scintigraphy (6). Highly differentiated thyroid cancer cells exhibit iodine uptake due to the expression of sodium-iodide symporter (NIS) but most often no significant glucose uptake, while less differentiated cells that ceased to express NIS upregulate glucose and FDG uptake (7–9). 18F-FDG-PET has therefore become a mainstay in the diagnosis of recurrent thyroid cancer, in particular in patients with elevated serum hTg and negative I-131 scintigraphy (10–14).
While US is the undisputed first choice in the routine evaluation and follow-up of thyroid cancer patients (10–12,15,16), its role relative to 18F-FDG-PET is less well established. We set out to determine the incremental diagnostic value of targeted cervical US performed after hybrid radionuclide imaging (FDG-PET-CT and I-131 single photon emission computed tomography + CT = SPECT-CT) (17) in a prospective cohort of 50 consecutive patients against composite gold standard based on histology, cytology, imaging, and clinical follow-up.
Material and Methods
Patient cohort
Between June 2009 and January 2012, 51 consecutive patients with suspected recurrent or progressive DTC after previous ablative therapy including total thyroidectomy (TT) and radioiodine ablation were prospectively included. Indications for multimodal imaging were (one indication per patient): suspicious US lesion(s) in 16 patients (31%) (including five already confirmed by US-guided fine needle biopsy [FNB] 10%); increasing/unexplained hTg in 20 patients (39%); restaging of known metastatic disease in five patients (10%); positive TgAB in two patients (4%); and other indications in eight patients (16%).
Imaging protocol
Imaging protocol.
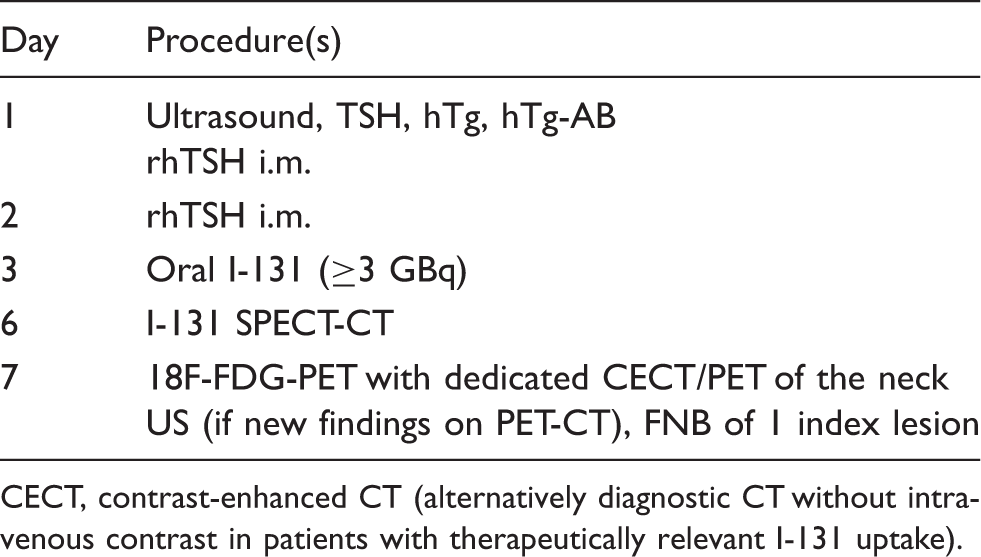
CECT, contrast-enhanced CT (alternatively diagnostic CT without intravenous contrast in patients with therapeutically relevant I-131 uptake).
I-131-SPECT-CT was performed on a Siemens Symbia T6 (Siemens Healthcare, Erlangen, Germany) with high-energy collimators. After a whole body planar scan, SPECT of the neck and upper mediastinum was taken (2 × 32 projections @ 20 s) with a co-registered low-dose CT (130 kV, effective tube current 15 mAs).
18F-FDG-PET was performed on a Siemens Biograph 40 (Siemens Healthcare) after an overnight fast. Approximately 60 min after injection of approximately 370 MBq 18F-FDG, a whole-body PET was acquired from the skull to the thighs at 3 min per bed position after an initial low-dose CT (120 kV, 50 mAs) (20). A dedicated PET-CT of the neck and upper mediastinum was then performed with the arms down at 6 min per bed with a co-registered contrast-enhanced CT (CECT; 120 mV, 240 mAs; 2 mm slices, field of view 240 mm) acquired 50 s after intravenous injection of 100 mL iomeprol (350 mg iodine/mL; Bracco Imaging Scandinavia, AB, Gothenburg, Sweden).
For stimulation with thyroid stimulating hormone (TSH), patients either received intramuscular injections of 0.9 mg recombinant human TSH (rhTSH, Thyrogen®; Genzyme Corp., Cambridge, MA, USA) on two successive days, or thyroid hormone was withdrawn for 4 weeks.
Image processing and analysis
All image data including US were digitally archived in the department's Picture Archiving and Communication System (PACS) (Agfa Impax 6, Agfa Healthcare BV, Antwerp, Belgium). USlesions were classified according to current consensuscriteria (21). CTs were read on PACS workstations using calibrated screens. Nuclear medicine data were processed with Segami Oasis (v. 1.9.3; Segami Corporation, Columbia, MD, USA). Maximum SUV(SUVmax) in PET images was determined by placing spherical volumes of interest (VOI) around each focus, preferentially in the dedicated cervical acquisition. In case of neighboring hot lesions, custom VOIswere drawn. Lesions were classified as FDG-positive when the SUV was ≥2.5 or when a focus wasclearly discernible against the background (22,23). I-131 uptake was assessed using a 5-point qualitative scale (less than background, background, faint, warm, hot).
Clinical chemistry
Serum thyroglobulin (hTg) and anti-thyroglobulin antibodies (TgAB) were analyzed by immunometric assays (Immulite 2000) from Siemens Healthcare Diagnostics (Llanberis, UK), urinary iodide based on the Sandell-Kolthoff reaction.
Surgery
Compartment-oriented microdissection with systematic removal of lymphatic and fatty tissue was performed under general anesthesia (24,25). When the compartment had already been extensively dissected, recurrent tumor was resected without systematic compartment dissection. Neural monitoring was undertaken for all relevant nerves including the recurrent laryngeal, vagus, accessory, phrenic, and hypoglossal nerves (26,27).
Histopathology
Tissues were fixed in 10% neutral buffered formalin for 2–3 days. Lymph nodes were bisected along the hilar plane. Five µm sections of samples embedded in paraffin were stained by Hematoxylin and Eosin (HE), supplemented by immunohistochemical staining for thyroglobulin in selected cases.
Follow-up
All patients were followed with the imaging modalities that had been positive on the original multimodal imaging protocol. A composite gold standard was based on the best available evidence (histology, cytology, repeat imaging, and/or clinical follow-up in descending order). Individual findings (“lesions”) were classified as true/false positive/negative as reported at the time of the original study in relation to the composite gold standard (22). On the patient level, multimodal imaging was scored as true positive (TP) if at least one TP lesion was detected, as false positive (FP)/false negative (FN) in case of at least one FP/FN lesion in the absence of TP lesions, and otherwise as true negative (TN). All original image studies were re-read to detect FN findings overlooked at the time of the original report.
Ethics
The project was conducted as a quality surveillance study in full accordance with the guidelines issued by the institutional review board (IRB) and current Norwegian legislation, and the IRB exempted the study from review on 28 February 2014.
Data management, analysis, and statistics
All observations were registered in MDcake, a client-server database application developed by our group for the present study (28,29). Multiple lesions in parenchymatous organs such as lung or liver were encoded as a single lesions to avoid biasing lesion-based analysis. Data were re-aggregated into two SQL views, one for analyzing patients/studies and one for lesions. These provide the basis for all subsequent analyses. These were conducted with the statistics program “R” (30). For group comparisons, Wilcoxon rank sum test and Fisher's exact test were applied at a significance level of 5% (two-sided).
To evaluate the performance of diagnostic modalities with a continuous (FDG SUV) or ordinal predictor (I-131 uptake), receiver operating characteristics (ROC) analysis was performed with R package pROC. The likelihood of a correct diagnosis of a tumor lesion (sensitivity) is plotted against the likelihood of an incorrectly diagnosed benign lesion (1 – specificity) for all possible values of the predictor. For an ideal method, the ROC curve will approach the upper left corner of the plot while the curve will be close to the diagonal for a method with low predictive power. Ninety-five-percent confidence intervals (CI) for sensitivity and area under the curve (AUC) were calculated by bootstrapping (2000 iterations) (31).
Results
Patient-based analysis
Patients summary.
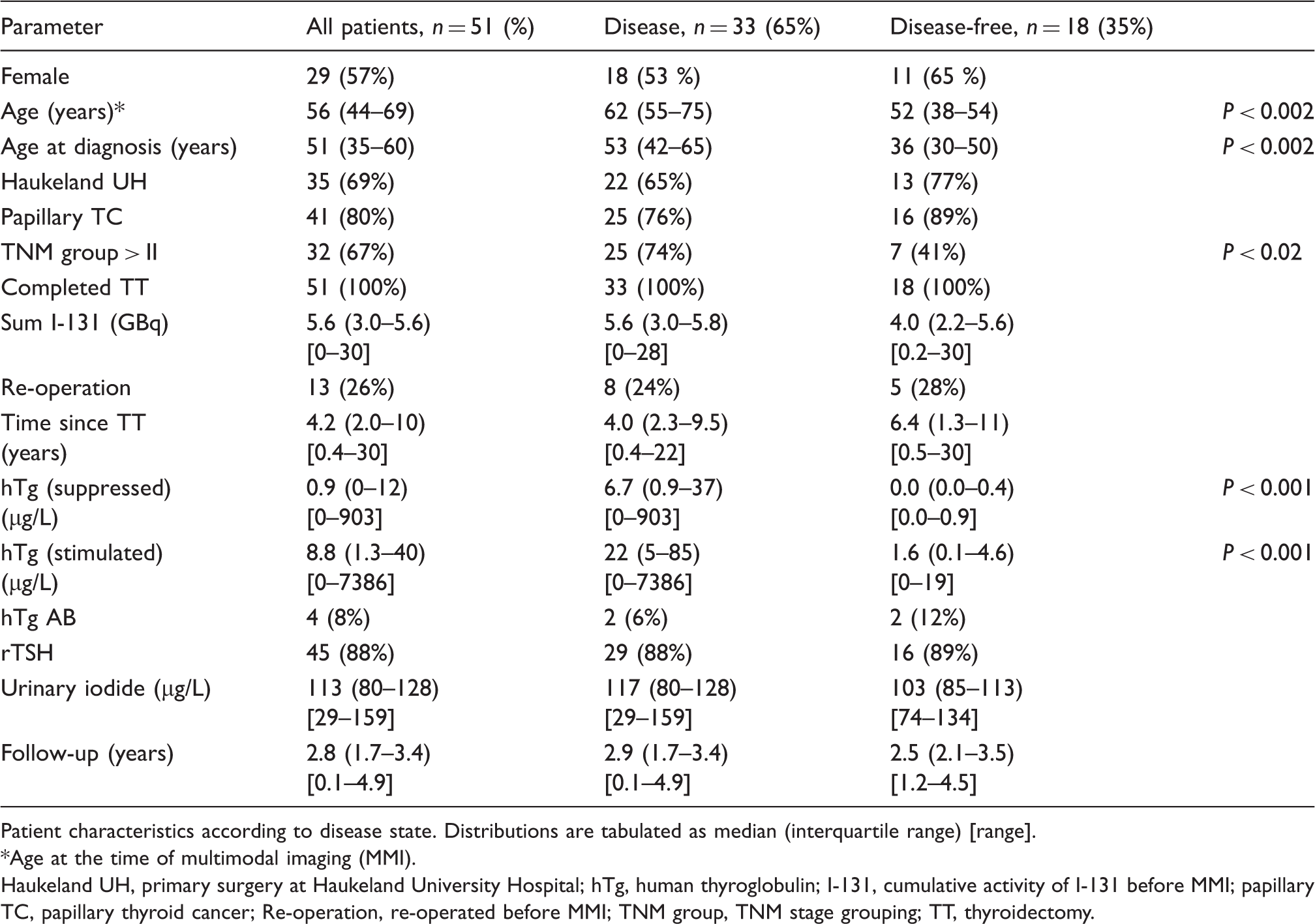
Patient characteristics according to disease state. Distributions are tabulated as median (interquartile range) [range].
Age at the time of multimodal imaging (MMI).
Haukeland UH, primary surgery at Haukeland University Hospital; hTg, human thyroglobulin; I-131, cumulative activity of I-131 before MMI; papillary TC, papillary thyroid cancer; Re-operation, re-operated before MMI; TNM group, TNM stage grouping; TT, thyroidectomy.
Lesion-based analysis
Lesions summary.
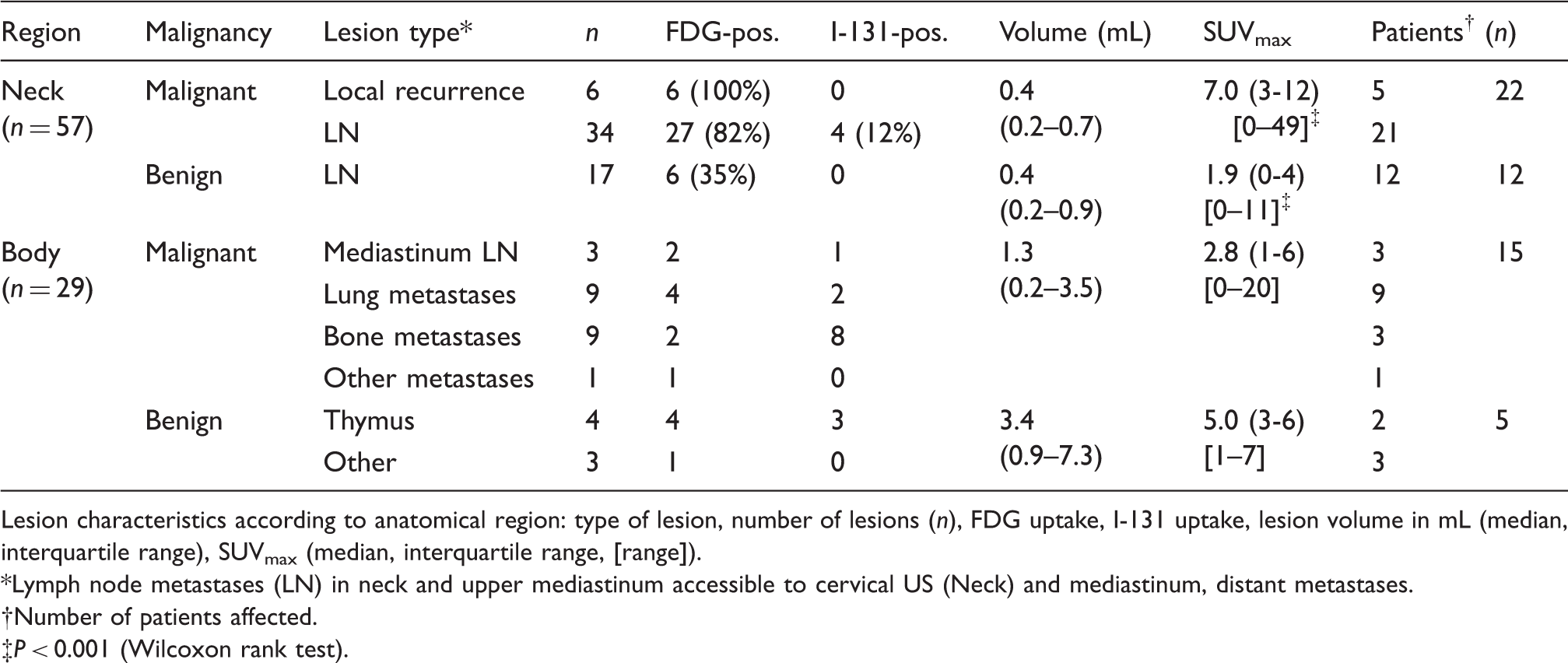
Lesion characteristics according to anatomical region: type of lesion, number of lesions (n), FDG uptake, I-131 uptake, lesion volume in mL (median, interquartile range), SUVmax (median, interquartile range, [range]).
Lymph node metastases (LN) in neck and upper mediastinum accessible to cervical US (Neck) and mediastinum, distant metastases.
Number of patients affected.
P < 0.001 (Wilcoxon rank test).
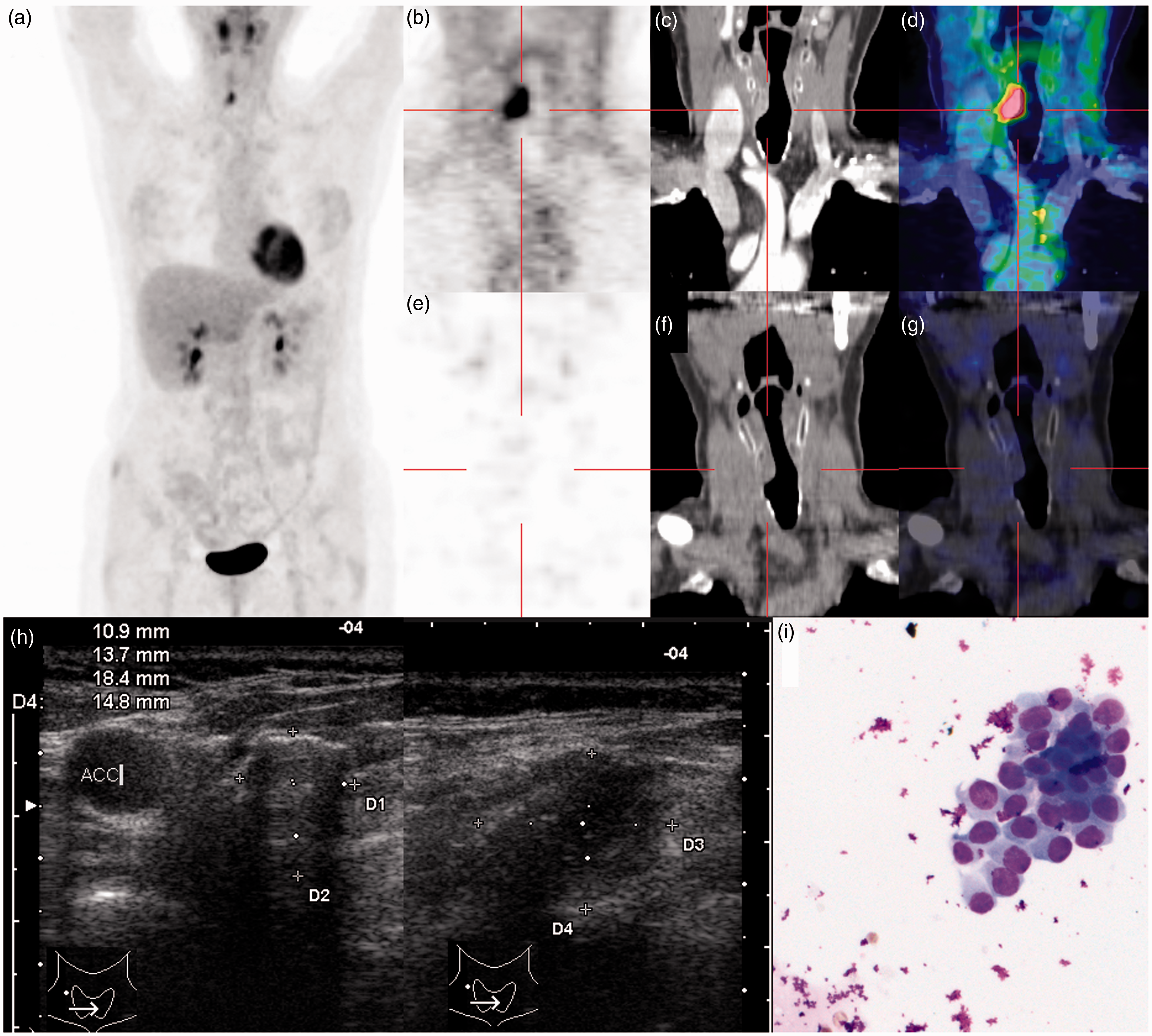
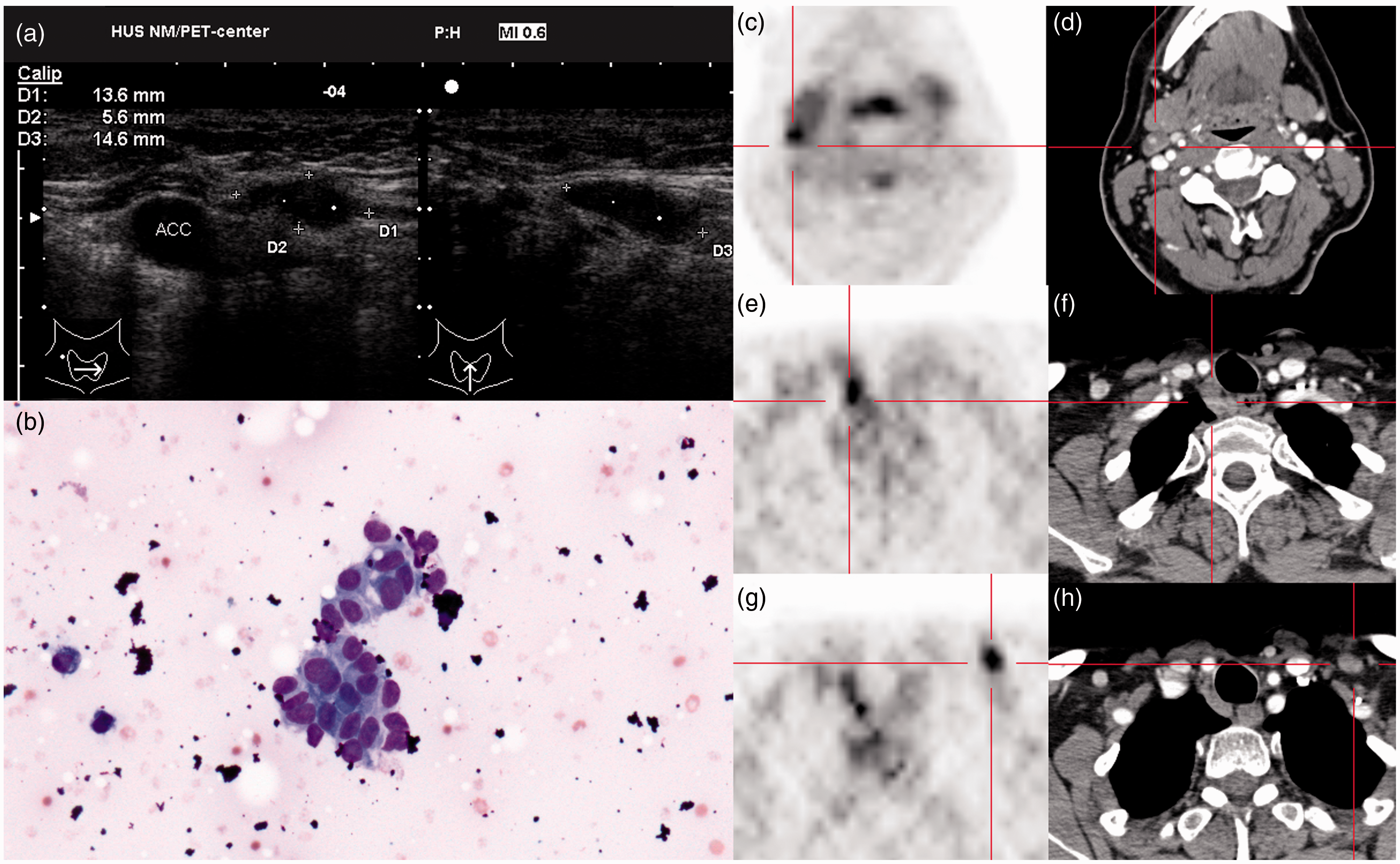
Fifty-seven lesions located in the neck or upper mediastinum accessible to US (in short: “neck lesions”) were analyzed in detail. On ROC analysis, I-131-imaging lacked predictive power with an AUC of 0.51 (95% CI 0.44 – 0.58) for neck lesions and 0.55 (0.46–0.64) for all lesions (Fig. 1). FDG-PET had high discriminative power with an AUC of 0.80 (0.67 – 0.93) for neck lesions and 0.68 (0.56 – 0.80) for all lesions. However, at high sensitivities FDG-PET showed poor specificity. The inclusion of CECT in the workup achieved a high sensitivity of 90 % (76–97) with improved specificity of 71 % (44 – 90) compared with 58 % (9 – 88) of FDG-PET alone at the same level of sensitivity, but without reaching statistical significance. US before PET including optional FNB (preUS) had limited accuracy of 53 % with a sensitivity of 53 % (36 – 69 %) and a specificity of 53 % (28 – 77 %) (Figs 2 and 3 for examples). US in the detailed knowledge of the findings on PET-CT and SPECT-CT (postUS) outperformed PET alone and preUS with a specificity of 94 % (71 – 99) while maintaining sensitivity at 85 % (70 – 94) (p < 0.05 for all comparisons).
ROC analysis. For 18F-FDG-PET (FDG) and I-131 scintigraphy (I-131) in neck lesions (neck) or the entire body (all) sensitivity is plotted against specificity for all possible values of the predictor (standardized uptake value or intensity of I-131 uptake). The performance of US before PET (Pre-PET) and after PET (Post-PET) as well as the performance of PET-CT are plotted as discrete data points. Error bars and the gray area around the curve for FDG-PET in the neck indicate 95% confidence intervals. A 59-year-old patient with unclear rise of hTg. Previous imaging including repeated ultrasound of the neck was negative. 18F-FDG-PET-CT revealed a paralaryngeal recurrence: Whole-body PET (a), coronal PET slice (b), contrast-enhanced CT (c), and fusion image (d). I-131-SPECT-CT showed no corresponding uptake (e–g). US after PET revealed an hypoechoic soft tissue lesion (h). US-guided FNB showed abnormal epithelial cells (i). The patient was treated by endotracheal laser ablation. A 54-year-old patient with cytologically confirmed index lesion. Routine US September 2009 revealed a hypoechoic lymph node behind the left clavicle (a). Cytology showed abnormal epithelium – papillary thyroid cancer (b). As expected, PET-CT showed FDG uptake (SUVmax 6.4) in the index lesion (panels g, h). In addition it revealed a right-sided paratracheal recurrence (SUVmax 7.0) that was not visible on US (e, f) and a cystic lymph node metastasis behind the right angle of the jaw (SUV 5.0) that had been overlooked on initial US. The patient was re-operated with a revision of the cranial right lateral neck (K2/II), the right-sided central compartment (K1b/IV), and the caudal left lateral neck (K3/V) with preservation of recurrent laryngeal nerve function. All lesions were histologically confirmed.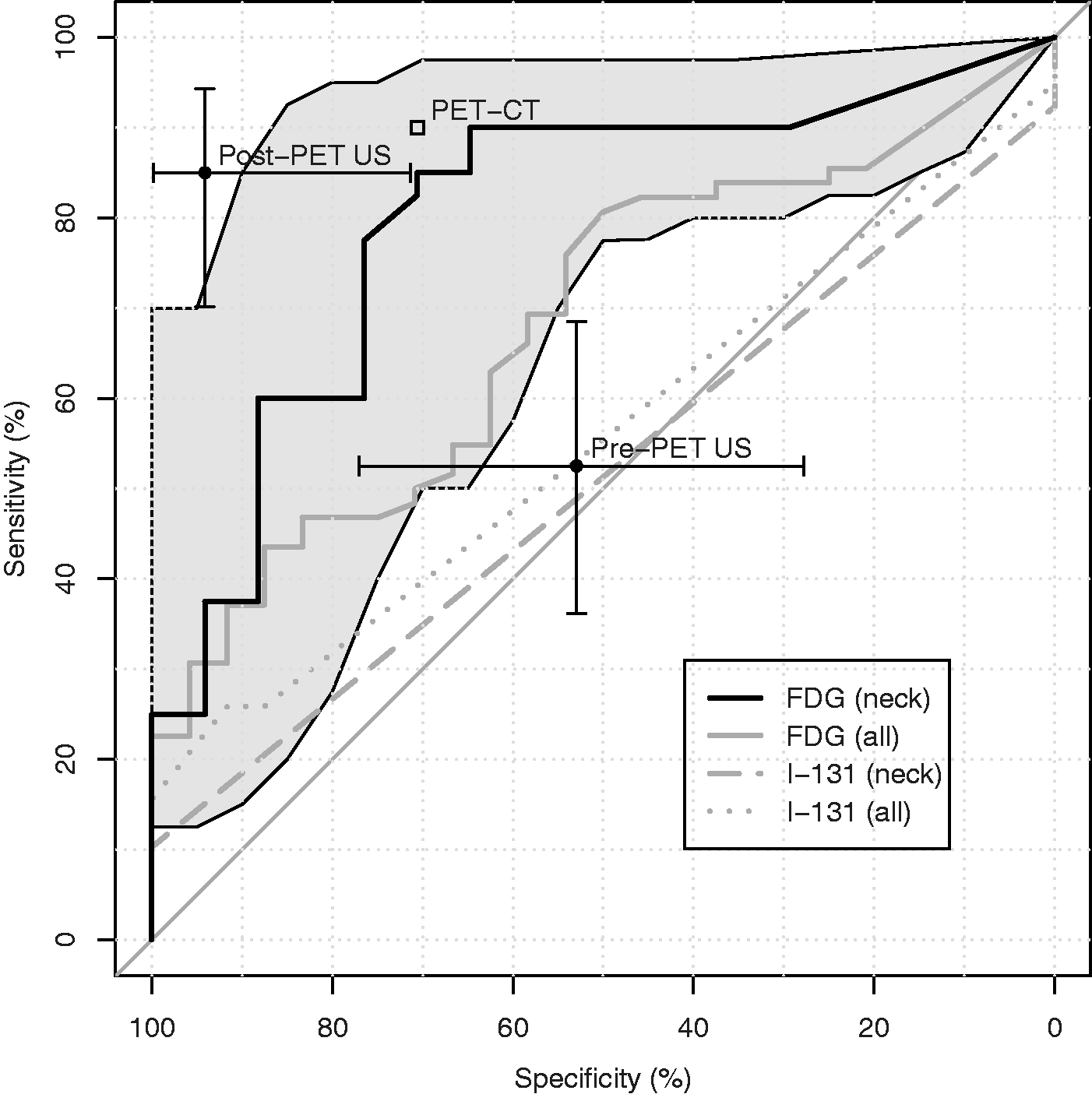
To estimate the relative contribution of US with and without FNB to overall diagnostic performance, we simulated an imaging workflow as outlined in Table 1 with FNB being performed only as the last step of the protocol. Of the 40 malignant neck lesions, pre-US without FNB would have correctly diagnosed 18 lesions (45%), and pre-US plus radionuclide imaging another 18 (45%). Post-US and FNB did not increase the diagnostic yield over the combination of pre-US and PET-CT, while four malignant lesions remained undetected. Of the 17 benign neck lesions, nine (50%) were TN on pre-US and PET-CT while eight (44%) were FDG-positive. Three (17%) required post-US and another three (17%) FNB to establish the correct diagnosis (sparing three patients for unnecessary compartment resections for benign disease) while two remained FP, one of them with a FP FNB.
Outcomes
Therapeutic consequence of multimodal imaging.
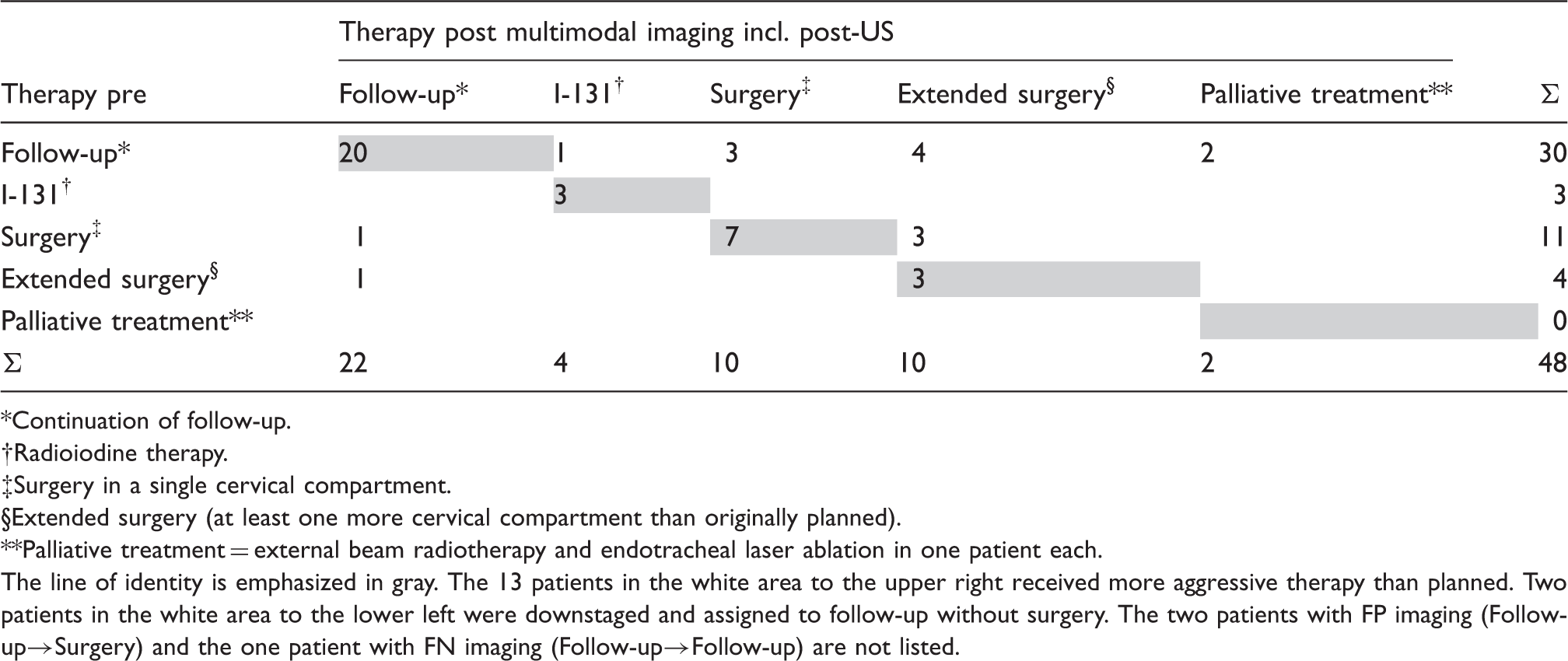
Continuation of follow-up.
Radioiodine therapy.
Surgery in a single cervical compartment.
Extended surgery (at least one more cervical compartment than originally planned).
Palliative treatment = external beam radiotherapy and endotracheal laser ablation in one patient each.
The line of identity is emphasized in gray. The 13 patients in the white area to the upper right received more aggressive therapy than planned. Two patients in the white area to the lower left were downstaged and assigned to follow-up without surgery. The two patients with FP imaging (Follow-up→Surgery) and the one patient with FN imaging (Follow-up→Follow-up) are not listed.
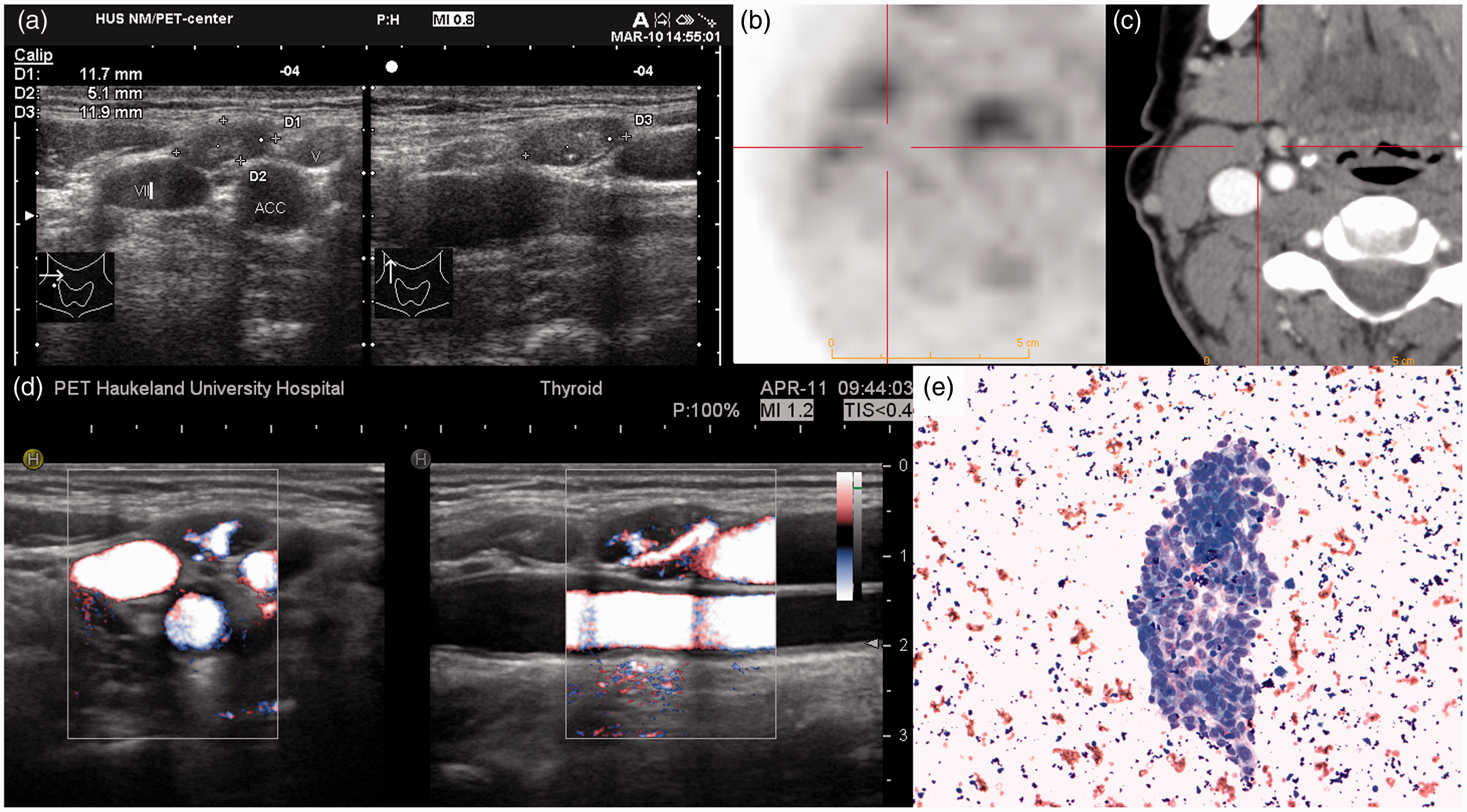
FN multimodal imaging in a 49-year-old patient. Routine US had detected a suspicious lymph node behind the right angle of the jaw with microcalcifications (a). 18F-FDG-PET (b, c) and I-131-SPECT-CT (not shown) showed no tracer uptake. US-guided FNB was FN. On repeat imaging with new US machine (d), the lymph node showed focal hyperperfusion not observed in the surrounding nodes. New cytology was positive (e) with a human thyroglobulin in the washout from the needle of 855 ng/L. FDG-PET was still negative (not shown). Re-operation revealed one metastasis in 21 lymph nodes.
Discussion
High-resolution US is the mainstay of the assessment of thyroid cancer both for initial evaluation and for follow-up (10–12,15,16). US may help avoid repeat surgery in up to 40% of patients when compared with physical examination alone (32,33).
The incremental value of US over other imaging modalities is more difficult to ascertain. To our knowledge, our series is the first to systematically evaluate the performance of US before and after multimodal sectional imaging – I-131 SPECT-CT and 18F-FDG PET-CT – by the same observer in the same cohort of patients with known or suspected recurrent DTC. In our prospective analysis of 51 consecutive patients, US with optional FNB before radionuclide imaging identified only 53% of all cancer lesions in the neck, while US after multimodal imaging had a significantly higher lesion based sensitivity of 85% (P < 0.05). US after multimodal imaging had the highest specificity of 94% versus 53% for US alone and 80% for 18F-FDG-PET alone (P < 0.05). High specificity is necessary to avoid futile surgery based on FP findings. In a simulated workflow assuming FNB as the last step in the diagnostic algorithm, pre-US and radionuclide imaging together would have identified 90% of all malignant neck lesions with no further increase in sensitivity by post-US and FNB. Post-US and FNB were, however, vital for the correct diagnosis of benign lesions with non-malignant reactive or inflammatory FDG uptake, increasing specificity from 50% for PET-CT alone to 90% for PET-CT + post-US + FNB. We therefore strongly recommend post-US with optional FNB for the evaluation of all FDG-positive neck lesions in patients with thyroid cancer, at least when surgery is considered. For the evaluation of clinically suspicious neck lesions and for routine follow-up, US supplanted by FNB up front is the most efficient first-line imaging modality: FNB of an index lesion will quickly establish or refute the indication for further imaging or therapeutic intervention, while it will also establish the correct diagnosis of malignancy in lesions that would be missed by PET-CT alone.
The main imaging modality chosen for the evaluation of US was 18F-FDG-PET as it is the most sensitive imaging method for the evaluation of recurrent DTC. In a systematic meta-analysis performed by Dong et al. in 2009, FDG-PET had a pooled lesion-based sensitivity of 91.6% and a patient-based sensitivity of 88.5% in patients with elevated hTg and negative I-131 scintigraphy (14). Specificity of FDG-PET was, however, limited to 77.5% (lesion-based) and 84.7% (patient-based), which compares well with our own results.
We were disappointed by the performance of cervical US when performed alone (pre-US). The most detailed head-to-head comparison of US and FDG-PET was performed by Seo et al. (34). In 20 thyroid cancer patients (19 PTC, 1 MTC) with cytologically proven recurrence, US, CECT, and PET-CT were compared with histology in each of 110 nodal levels that were surgically explored. Sensitivity and specificity for US was 69.2% and 89.7% for CECT 63.5% and 94.8%, and for PET-CT 53.8% and 79.3%. These findings based on histology as the sole gold standard are largely in agreement with ours. The sensitivity of US is likely overestimated, since only patients with positive FNB of at least one cervical lesion were included.
Only a few studies allow estimates of the sensitivity of US when performed independently of 18F-FDG-PET. In a series with 49 patients with DTC and positive serum hTg, only one out of six local recurrences was found on pre-PET US while five were seen on CECT and PET. All were confirmed by hTg in US-guided FNB after PET (35). In a recent multicenter series with 327 patients, per-patient sensitivity and specificity was 37% and 94% for US, and 92% and 95% for PET/CT (36). In a single-center study in 423 patients, 16 out of 90 recurrent lesions were missed on US, but diagnosed with FDG-PET-CT (23).
Our observation that cervical US misses cancerous lesions is further confirmed by studies that only included patients with negative conventional imaging including US. In a series of 34 patients with 30 tumor lesions in the neck, new US detected 18 (including three that were FDG-negative), CECT 14, and FDG-PET 27 (37). In another recent prospective series, FDG-PET/CT had a per-patient sensitivity of 87%, and a specificity of only 77% implying that the majority of the lesions had been overlooked at baseline US (38). Similar observations were made by Pomerri et al. (39) and Freudenberg et al. (40).
There are limitations connected to our study. Ideally, the standard for evaluating a diagnostic method should be completely independent of the method under study (41). A correct estimate of the specificity of a diagnostic method and its positive predictive value requires also a sufficient number of negative observations (42). If histological specimens were taken as sole gold standard, the last condition can only be met if prophylactic lymph node dissection is performed even in the absence of disease demonstrable by imaging. In a series of 560 patients by Ito, US had a per patient sensitivity of 27.2% and a specificity of 96.5% compared with histological specimens (43). Preliminary results from our own series and a smaller recent study (44) confirm that imaging underestimates the number of malignant lesions compared with histological preparations. Results from Ito's series (43,45) imply that micrometastases in cervical lymph nodes do not have the same prognostic relevance as macrometastases that are detected clinically or by cervical US. Thus measuring the performance of cervical US against histology may not lead to appropriate conclusions for the clinical management of patients with DTC.
Misdiagnoses in two patients in our series could have probably been avoided, if we had analyzed hTg from the washout of the US-guided FNB as we did from February 2011. The thymic lesions were unfortunately inaccessible to percutaneous biopsy.
The proportion of patients with iodine-avid lesions in our cohort was lower than in a recent German series, in which 78 out of 327 patients (24 %) had TP findings on I-131 scintigraphy (37). In two recent series from France and Italy, only one out of 34 hTg-positive patients had therapeutically relevant I-131 uptake (37), and only one of 22 patients had therapeutically relevant uptake in a pulmonary metastasis (46). Measurements of urinary iodine excretion in our patients exclude iodine contamination as a cause for our observation. As a consequence of this study, we have altered our protocol from combined imaging/therapy with ≥ 3 GBq I-131 to imaging with I-123, a pure gamma emitter, in order to reduce radiation exposure particularly to the salivary glands (47).
In conclusion, in patients evaluated for recurrent DTC after previous ablative therapy US performed independent of other imaging modalities misses about half of cancer lesions in the neck while 18F-FDG-PET is sensitive but lacks specificity. US performed in correlation with 18F-FDG-PET-CT maintained the sensitivity of FDG-PET, but increased specificity by eliminating false positive diagnoses due non-malignant FDG uptake in cervical lesions.
Supplementary material
Supplementary material is available online at acr.sagepub.com/supplemental.
Footnotes
Acknowledgments
We thank Bodil Næss, Bergen PET Center, Department of Radiology, for invaluable technical help in implementing the PET-CT protocols; Njål Brekke, PhD, Department of Oncology and Medical Physics, for technical advice regarding PET quantification; Prof. Gunnar Mellgren, Hormone Laboratory and Department of Clinical Medicine, Dr. Øystein Fluge, Department of Oncology, Prof. Karen Rosendahl and Dr. Lars Reisæter, both Department of Radiology and Department for Clinical Medicine, Haukeland University Hospital/University of Bergen for valuable advice in writing this manuscript.
Conflict of interest
None declared.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.