
Abstract
Dysfunction in mental imagery may contribute to the development of mental disorders. We studied the vividness and controllability of mental imagery in a sample of 42 individuals with recent-onset psychosis, using a cross sectional design. Contrary to earlier studies, the claim that mental imagery is enhanced and the controllability weak in psychotic disorder was not supported. Especially the negative and affective symptoms associated with low vividness, and the stronger the symptoms the patients had, the less vivid was their imagery. Anxiety and self-neglect were the best predictors of low vividness. Only an elevated mood associated with higher vividness. The cognitive performance of the participants did not associate significantly with imagery. Surprisingly, organic modality was reported to be the most vivid modality, whereas visual imagery was the least vivid. Understanding the role of mental imagery in early psychosis may help us to understand and treat these disorders better.
There has been a long tradition of studying the relationship between mental imagery and mental disorders, such as psychotic disorders, anxiety and mood disorders, and post-traumatic stress disorder (PTSD) (Brewin et al., 1996; Bywaters et al., 2004; Galton, 1880; 1883; Hirsch & Holmes, 2007; Holmes & Mathews, 2010; Horowitz, 1995; Morina et al., 2011; Oertel et al., 2009; Sack et al., 2005), but the link has still remained controversial. ‘Mental imagery’ refers to perceptual experiences in the absence of any sensory stimulation, being internally generated from memory (Richardson, 1994). Mental images are characterized by their subjective resemblance to sensory impressions, as seeing with the “mind’s eye” (Kosslyn et al., 1999) or hearing with the “mind’s ear” (Kosslyn et al., 2001). Imagery can involve multiple sensory modalities, including bodily sensations and feelings, and can be aroused voluntarily or spontaneously. Imagining a familiar face or object, the smell of roses or the sound of an ambulance siren all depend on our mental imagery ability. According to the preference order of sensory modalities, visual and auditory images are usually experienced as being the most vivid, whereas olfactory and gustatory images are experienced as being the least vivid (Schifferstein, 2009).
As mental imagery is important in all cognitive processes (Kosslyn et al., 1995; Pearson et al., 2015), it is also important in psychopathology because of its powerful impact on emotion (Holmes et al., 2008; 2009; Holmes & Mathews, 2010). It has been found that mental images elicit stronger emotions compared to the representations in verbal form (Pearson et al., 2015). One possible explanation why imagery enhances emotion is due to responding as if events or stimuli were “real” (Holmes & Mathews, 2010; Kosslyn et al., 2001). Emotional imagery (f. ex. fearful and distressing images) will likely lead to more vivid imagery compared to neutral images (Bywaters et al., 2004; Lang, 1977, 1979). The assessment of individual differences in mental imagery (ability) across mental disorders can help in treatment planning as well as in diagnostic decision-making (Ji et al., 2019). The examination of imagery in early psychosis may be especially valuable as this phase is associated with later outcomes (Laing et al., 2016).
Traditionally, imagery ability has been assessed according to two fundamental characteristics, vividness and controllability (Pearson et al., 2013; Richardson, 1994). The vividness refers to the clarity and liveliness of the image simulating an actual perception (Marks, 1972; 1989; McKelvie, 1995). The controllability refers to the ability to intentionally transform or manipulate mental images in one’s mind (Gordon, 1949; Kosslyn, 1994; Richardson, 1994). This means that persons have a capacity to shift their mental view of an object and they can view it from different positions. According to Gordon (1972), an adaptive mental imagery depends on it being controlled and voluntary.
Usually vivid and controlled imagery is the expected imagery type in healthy people (Richardson, 1972). Mental imagery ability can differ in its vividness and controllability according to personality types and mental disorders (Ji et al., 2019; Richardson, 1994). Costello (1957), who was the first to empirically link the characteristics of vividness and controllability of imagery with personality factors and psychopathology, suggested that the type of imagery indicates the type of disorder to which an individual might be prone. In psychotic disorders and severe mood disorders, such as schizophrenia spectrum disorders and bipolar disorder, the vivid and uncontrolled imagery type has been found (Aleman et al., 2000; Benson & Park, 2013; Crespi et al., 2016; Ivins et al., 2014; Oertel et al., 2009; Pearson et al., 2013; Rasmussen & Parnas, 2015; Sack et al., 2005). In that case mental images are “especially vivid” and are characterized by intrusive and distressing (repetive) emotional images (Brewin et al., 2010; Holmes & Hackmann, 2004; Holmes & Mathews, 2010; Jones & Steel, 2012; Morina et al., 2011; Morrison et al., 2002; Schulze et al., 2013). Mental images can interfere with reality, so that the person is not able to differentiate internal or external experiences, true or imagined perceptions. Thus, imagery that is “too vivid” may contribute to the maintenance of psychotic symptoms, for example, hallucinations and delusions (Aynsworth et al., 2017; Morrison, 2001; Morrison et al., 2002; Winfield & Kamboj, 2010). On the other hand, Crespi et al. (2016) have demonstrated that, in an opposite effect to psychotic conditions, imagery vividness is decreased in autism spectrum conditions. Thus, both decreased and increased mental imagery may associate with psychiatric disorders. This is contrary to the previous claim by Harvey et al. (2004), conceptualizing mental imagery as a continuum, where at one end is normative processing and at the other end psychopathological processing.
In previous research, impaired mental imagery (low vividness of imagery) has been associated with depression and anxiety disorders (Bryant & Harvey, 1996; Holmes et al., 2008; Morina et al., 2011; Morrison et al., 2011; Zarrinpar et al., 2006). However, more recent studies have not found deficits in the ability to generate, manipulate, or recall images in depressive and anxiety disorders compared to matched healthy controls (Di Simplicio et al., 2016). In affective disorders, the impairment of mental imagery seems to associate with the emotional content, so imagining positive scenarios is less vivid while the vividness of negative imagery is elevated (Holmes et al., 2008; 2016; Ji et al., 2019; Morina et al., 2011; Pile & Lau, 2018; Weßlau & Steil, 2014; Wu et al., 2015). This may further maintain anxiety and depressive symptoms (Ji et al., 2019). In contrast, in bipolar disorder the high vividness appears to be associated to both negative and positive mental imagery (Holmes et al., 2008; O’Donnell et al., 2018).
The study results concerning the relationship between imagery vividness (low vs. high) and psychotic symptoms are contradictory. In the review article by Seal et al. (2004), no clear relationship between vivid auditory imagery and auditory verbal hallucinations were found in schizophrenia, except for in a few studies (for example, Böcker et al., 2000; Mintz & Alpert, 1972) that found that the patients with hallucinations showed a higher level of vividness of mental imagery, especially in the auditory modality. The opposite results of weak (not vivid) auditory imagery in hallucinating subjects (Brett & Starker, 1977; Seitz & Molholm, 1947), or no differences in imagery vividness between patients with or without hallucinations (Chandiramani & Varma, 1987; Heilbrun et al., 1983; Slade, 1976; Starker & Jolin, 1982) have also been reported. Although auditory imagery has been found as the preferred imagery modality in individuals with hallucinations with schizophrenia (Aleman et al., 2002; Böcker et al., 2000; Heilbrun et al., 1983), also olfactory images have been found to occur relatively frequently and with greater sensory detail in people scoring highly on schizotypy or experiencing hallucinations or magical thinking (Kwapil et al., 1996; Mohr et al., 2002; Winfield & Kamboj, 2010). However, the study by Stevenson et al. (2011) did not find a relationship between olfactory imagery ability and olfactory hallucinations.
The studies by Sack et al. (2005) and the replicating study by Oertel et al. (2009) found a significantly higher vividness of mental imagery in schizophrenia patients, but there were no significant correlations between vividness and hallucinations, or any other psychotic symptoms. Because of this, they claimed that mental imagery vividness is not an effect of the patient’s current psychopathological state or a predisposition towards psychopathology, but an independent symptom that might be a new trait marker of schizophrenia, maybe related to the genetic liability to develop schizophrenia. Also, the study by Ng et al. (2016) postulated that increased mental imagery susceptibility might be a trait risk factor for bipolar disorders instead of a state-like feature or an effect of the disorder. However, the latest studies have found that people who have a general ability to experience vivid mental imagery may be more vulnerable to developing psychotic-like symptoms in trauma and stress conditions compared with people with low imagery vividness (Morina et al., 2013). According to them, hallucinations depend on the level of vividness, in other words, high vividness will predispose one to psychotic symptoms like hallucinations or mood amplifications (Aynsworth et al., 2017; O’Donnell et al., 2018). To summarize, the literature is inconsistent on whether “vivid imagery” accounts for psychotic experiences.
The possible associations between imagery and cognitive abilities have also been studied (Oertel et al., 2009; Richardson, 1994). Intelligence measured by IQ-type tests has not been found to systematically associate with imagery ability, e.g. whether weak imagers are more or less intelligent than vivid imagers (Richardson, 1994).
The main purpose of the present study was to examine the mental imagery ability among individuals with recent-onset psychosis. As well as the previous studies, also our study focuses on mental imagery of non-emotional stimuli during a non-aroused state. We assessed the vividness and controllability of mental imagery as well as the preference order of sensory modalities of this group.
We hypothesized that individuals with psychosis show high imagery vividness and low imagery controllability and that auditory imagery is the most preferred modality in this group.
Our second aim was to examine possible associations between mental imagery and clinical variables such as psychotic symptoms and cognitive performance.
Methods
Participants
The participants consisted of 42 individuals with recent-onset psychosis (female: 19; male: 23) one year after their first psychiatric treatment contact for psychosis. They were diagnosed with a schizophrenia spectrum psychotic disorder (66.7%, n = 28), psychotic mood disorders (bipolar disorder and major depression) (19.0%, n = 8), psychotic disorder not otherwise specified (11.9%, n = 5), and a brief psychotic disorder (2.4%, n = 1). DSM-IV diagnostic assessment was done by a senior psychiatrist (JS) after the one-year follow-up using all available information including SCID interviews (performed by a research nurse or a psychologist) and a review of all lifetime medical records from both psychiatric and other treatment contacts (Keinänen et al., 2015). The participants were recruited from the in- and outpatients units of the Hospital District of Helsinki and Uusimaa and the City of Helsinki and participated in the Helsinki Early Psychosis Study (Keinänen et al., 2015; Lindgren et al., 2017) between the years 2010 and 2016. Participation in the study was voluntary, and a written consent was provided by all the participants. The study was conducted according to the Declaration of Helsinki with approval of the Ethics Committee of the Hospital District of Helsinki and Uusimaa, and of the institutional review boards of the Finnish Institute for Health and Welfare, Helsinki, and the University of Helsinki.
Measures
The shortened form of Betts’ Questionnaire upon Mental Imagery. The vividness of mental imagery was assessed by the shortened form of Betts’ Questionnaire upon Mental Imagery (QMI) by Sheehan (1967a), which is a revised version of a 150-item questionnaire constructed by Betts (1909). QMI measures a general ability to imagine across seven sensory modalities, i.e., visual, auditory, cutaneous (tactile), kinaesthetic (motor), gustatory (taste), olfactory (smell), and organic (bodily sensations) modalities. Sheehan’s (1967a) shortened inventory contains 35 items, five items for each of the seven sensory modalities. The respondents are asked to imagine different kinds of sensory items (e.g., “hearing an ambulance siren,” “the sensation of fatigue,” or “smelling the scent of a rose”), and to rate their imagery vividness on a seven-point scale ranging from 1 (a “perfect image,” i.e., “I perceive it perfectly clearly and vividly, as if it were an actual experience”) to 7 (“no image at all”, i.e., “I am thinking about it but I cannot imagine it”). Thus, high scores indicate less vivid imagery and low scores more vivid imagery. The total score is reached by adding up the number of points for each item. The scale is a reliable and valid method for measuring the general ability to imagine (Sheehan, 1967a; 1967b; White et al., 1977). There are no significant gender differences in any of seven sensory modalities of the Betts’ QMI (Campos, 2014a, 2014b; Campos & Pérez-Fabello, 2005; McKelvie, 1995). The scale is an internally consistent and reliable inventory in both clinical and general population groups (see e.g., Campos & Pérez-Fabello, 2005; Oertel et al., 2009; Sack et al., 2005; Vella-Brodrick & MacRae, 2004; White et al., 1977). The means and standard deviations for QMI subscales for college students (Kihlstrom et al., 1991) were the following: visual: 11.6 (4.4); auditory: 12.58 (4.64); cutaneous: 12.04 (4.6); kinesthetic: 12.1 (4.6); gustatory: 12.7 (5.13); olfactory: 14.44 (5.49); organic: 10.83 (4.27). The mean value of 3 or less on the seven-point scale refers to at least moderately clear and vivid images. Of the college students, only 1–2% of the subjects reported a mean value of 6 or more, and the distribution was positively skewed (Kihlstrom et al., 1991).
The Controllability of Visual Imagery Questionnaire. The controllability of mental imagery was assessed by the Controllability of Visual Imagery Questionnaire (CVIQ; Richardson, 1969), which is the adapted version of the Gordon’s Test of Visual Imagery Control (Gordon, 1949). The CVIQ is a self-report test that measures the ability to control and manipulate images. It consists of 12 items in which participants are asked to visualize a car in a certain scene and then asked to rate on a three-point scale whether they could imagine it in different colors, positions, and states of motion (scoring: yes = 2, I’m unsure = 1, no = 0). Total scores range from 0 to 24, and high scores indicate better image control. The mean score for college students (Kihlstrom et al., 1991) was 16.7 (SD: 4.7). The Gordon test is a well-established, empirically validated measure of controllability of mental imagery (Pearson et al., 2013; Richardson, 1994).
The Brief Psychiatric Rating Scale—Expanded. The clinical evaluation was done using the Brief Psychiatric Rating Scale—Expanded (BPRS-E; Ventura et al., 1993), which is a widely used rating scale for assessing the type, severity, and change over time of psychiatric symptoms. Ratings are based on clinical observations and subjects’ verbal report of symptoms during the interview. Each symptom is rated on a seven-point scale, ranging from 1 (not present) to 7 (extremely severe). With regard to severity, BPRS item scores of 3 or below have been defined as a mild severity (or in remission) (Andreasen et al., 2005). Symptom severity was rated based on the past seven days (current), and positive and disorganized symptoms were also rated from the worst period during the past year. Three domains (alogia, anhedonia-asociality, and avolition-apathy) of the Scale for the Assessment of Negative Symptoms (SANS) (Andreasen, 1989) were also included. The total score was reached by adding up the sum of 24 items of the BPRS. The reality distortion sum score was calculated as the mean of current hallucinations and unusual thought content item scores. The negative symptom sum score was calculated as the sum of BPRS scores for blunted affect and the three SANS items. Remission was defined according to the criteria by Andreasen et al. (2005), based on current symptom severity at the time of the one-year interview.
Neurocognitive performance, g factor. Cognitive testing was administered by a psychologist at one year, comprising tests from the Wechsler Adult Intelligence Scale, the Wechsler Memory Scale, the Trail Making Test, Verbal Fluency, the Tapping Task, and the Continuous Performance Test (Identical Pairs). A single exploratory factor model of the neurocognitive variables was formed to summarize neurocognitive performance (Lindgren et al., 2020), and the factor scores for this g factor were used to investigate the possible associations between cognitive performance and imagery.
Data Analyses
Mean, standard deviation, and range were calculated for the demographic characteristics, mental imagery (vividness and controllability), and the symptom variables. Gender and age differences were analyzed by the Mann-Whitney U test and chi-square test. The Spearman’s rho test was used to investigate the relationships between the mental imagery (vividness and controllability), and symptoms and cognitive performance.
We also repeated these analyses excluding the participants with psychotic mood disorder in order to see whether the results would be the same among those with non-affective psychosis.
Finally, a linear regression model was performed in the whole participant group to investigate which symptoms best explained the vividness of mental imagery. The symptoms with significant correlations with total mental imagery vividness were entered into a stepwise linear model that predicted vividness. All statistical analyses were calculated with SPSS Statistics for Windows, Version 25, with the significance level of .05.
Results
The means and standard deviations for the vividness and controllability of the mental imagery among the individuals with recent-onset psychosis are presented in Table 1. No significant gender and age differences were observed in imagery vividness nor in controllability of mental imagery. The total vividness score was 94.9. Most subjects reported experiencing at least moderately vivid images, corresponding to a mean value of 2.7 on the seven-point scale in most modalities. Organic and auditory imagery were the most vivid (mean: 2.4), whereas visual and olfactory imagery (mean: 3.2) were the least vivid sensory modalities. The mean score for controllability was 20.1.
Demographic Characteristics, Mental Imagery (Vividness and Controllability) and BPRS Variables in Psychosis Patients (N = 42, Female = 19, Male =23).
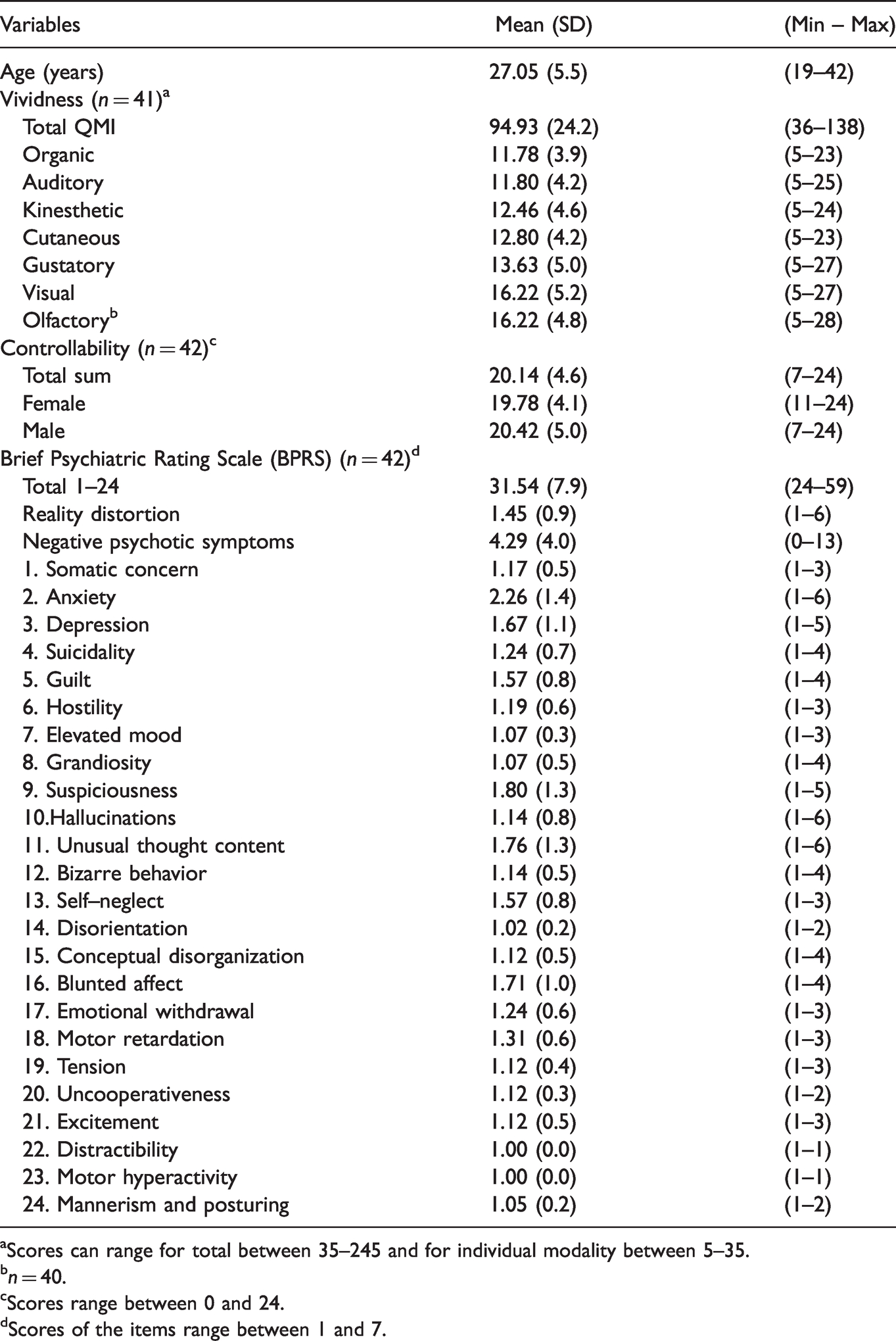
aScores can range for total between 35–245 and for individual modality between 5–35.
bn = 40.
cScores range between 0 and 24.
dScores of the items range between 1 and 7.
Correlations between the mental imagery and symptoms are provided in Table 2. Total mental imagery vividness (sum QMI) correlated significantly with current anxiety and motor retardation, and with guilty feelings and self-neglect related to the worst period during the preceding year. The correlations were positive, meaning that the more symptoms, the less vivid the imagery. The individual sensory modalities mainly correlated positively with different symptoms. The olfactory modality correlated negatively with elevated mood, meaning that the more elevated mood, the more vivid the imagery. The cutaneous (tactile) modality was the only modality with no significant correlations with symptoms.
Spearman Correlations Between the Mental Imagery Vividness and Controllability and BPRS Symptoms and Cognitive Performance.

Significant correlations (<.05) are followed with p-value.
The controllability of mental imagery correlated negatively with emotional withdrawal. This means that the higher emotional withdrawal associated with a weaker controllability.
The g factor did not correlate statistically significantly with the vividness of mental imagery but the association of higher cognitive performance with higher controllability approached significance (p = .054).
We then repeated the analyses excluding the eight individuals with a psychotic mood disorder. Among the 33 individuals with non-affective psychosis, the total vividness score was 97.0 and the controllability score was 19.8. The results concerning the preference order of the sensory modalities and the correlations between mental imagery and clinical variables were mainly identical compared to the results using the whole sample.
Finally, in a linear regression model, the symptoms with significant correlations with total mental imagery vividness (anxiety, self-neglect during the worst period, guilt during the worst period, motor retardation) were entered into a stepwise linear model that predicted the vividness of mental imagery. As gender, age, and cognitive performance were not significantly associated with vividness, we did not include these variables as covariates in the model. Anxiety and self-neglect remained the best predictors of low vividness (see Table 3).
Regression Model of Total Mental Imagery Vividness.
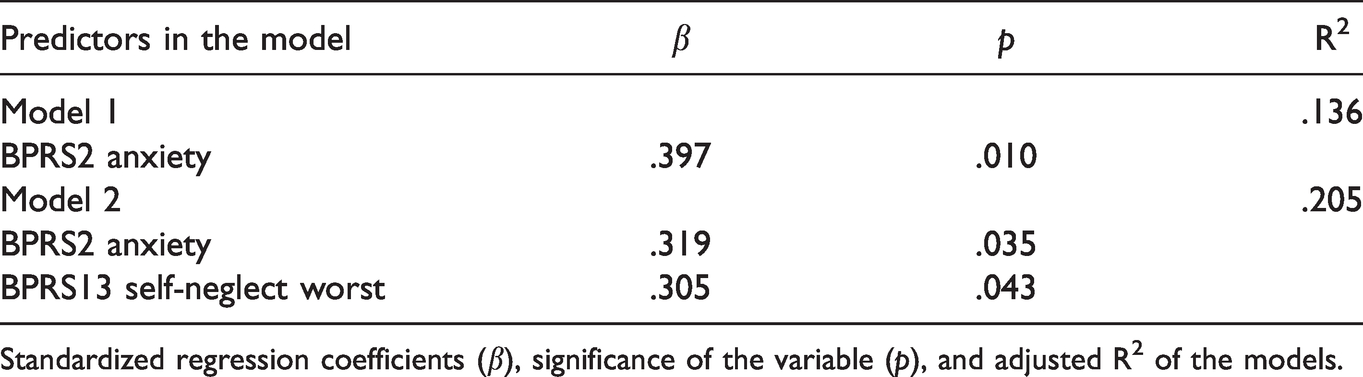
Standardized regression coefficients (β), significance of the variable (p), and adjusted R2 of the models.
Discussion
The aim of the study was to examine the mental imagery ability among individuals with recent-onset psychosis one year after entering treatment, most of them diagnosed with schizophrenia spectrum disorder and psychotic mood disorders. We hypothesized that, compared to the general population, the imagery vividness of individuals with psychosis would be high and the imagery controllability low, and that auditory imagery would be the most preferred modality. The vividness total score was 94.9, compared with 85.3 in the normative data published earlier (Campos & Pérez-Fabello, 2005). Noting that high scores indicate less vivid imagery, the vividness (according to normative data) was not high, as we had expected. Instead, it was very much like in the general population or even below. The controllability of imagery was strong: 20.1, compared with 16.7 among college students (Kihlstrom et al., 1991). Organic and auditory imagery were the most vivid modalities.
Our second aim was to examine possible associations between mental imagery and clinical symptoms. In our study, significant correlations were mainly with negative symptoms, blunted affect, motor retardation, emotional withdrawal, and self-neglect, and with depressive and anxiety symptoms including depression, anxiety, suicidality, and guilt. The stronger symptoms the patients had, the less vivid was their imagery. Only in elevated mood was the correlation reverse, meaning that a more elevated mood associated with more vivid mental imagery. According to a linear regression model, the best predictors of low vividness were anxiety and self-neglect, highlighting the significance of these clinical symptoms in the context of mental imagery.
The current study supported the previous research (f. ex., Holmes et al., 2008; Morina et al., 2011; Morrison et al., 2011) in that depression and anxiety associated with low vividness of imagery but did not support the expected relationship between the high vividness of imagery and positive psychotic symptoms. In previous research high vividness has usually been connected to positive symptoms like hallucinations (f. ex., Mintz & Alpert, 1972; Böcker et al., 2000; Morina et al., 2013), although findings on weak vividness in auditory imagery have also been published in schizophrenia populations (Brett & Starker, 1977; Seitz & Molholm, 1947). The reason for the few correlations with positive symptoms may be that 60% of the study sample was already in remission one year after entering treatment, according to the criteria suggested by Andreasen et al. (2005). In our study, negative and affective symptoms associated with low vividness, whereas an elevated mood (the manic-excitement factor) associated with higher vividness. The above-mentioned result supports the claim that individuals suffering from bipolar disorder show high spontaneous use of imagery (Holmes et al., 2011).
The controllability of mental imagery in people with psychosis was higher than in the normative data based on previous research. Adaptive mental imagery depends on it being controlled (Gordon, 1972) but not overcontrolled (Laor et al., 1999), like it seems to be in this patient group. According to Laor et al. (1999) high image control is associated with poor emotion regulation (or control). Perhaps high controllability may tell about a poor introspection ability more than good (adaptive) controllability. Poor insight has been stated to be a typical feature in schizophrenia (Erickson et al., 2011; Giugiario et al., 2012). On the other hand, our study result supports the claim that individuals with schizophrenia are able to manipulate and control mental representations in order to form mental images (Matthews et al., 2014). Thakkar and Park (2012) reported that schizophrenia patients are better than controls in a mental rotation test, which demands the manipulation of internal representations (mental images). One of the most striking findings was that organic modality was reported as the most vivid modality, whereas the visual imagery was the least vivid. The organic modality refers to imaging physical sensations such as fatigue, hunger or pain. The organic modality being experienced as the most vivid could be hypothesized to be associated with the somatic symptoms the individuals with psychosis typically experience. A study by Schifferstein (2009) found that the recency of the imagined activity would affect to the vividness of images. On the other hand, organic modality correlated significantly with the BPRS variables measuring all kinds of psychotic symptoms, as well as reality distortion and strong anxiety, possibly illustrating the severity of illness. It did not correlate with the somatic symptoms.
Visual imagery was the least vivid modality, whereas in healthy people it is usually the most preferred modality (Schifferstein, 2009). According to literature on patients experiencing hallucinations, auditory imagery has been found to be the preferred imagery modality compared with visual imagery (Aleman et al., 2000; Böcker et al., 2000). It has been noted that when the vividness of auditory imagery increases, then the vividness of visual imagery decreases. On the other hand, visual imagery in particular seems to be sensitive to anxiety and depression and their impoverishing effect, leading to alterations in mental imagery ability (Bryant & Harvey, 1996; Zago et al., 2011).
Based on previous literature, the weak vividness of imagery in the visual modality in individuals with psychotic disorder could be associated with the function of memory. Visual imagery is the most studied imagery modality and is suggested to be the most important modality for human beings in daily tasks as well as in cognitive skills (Pearson et al., 2015). Visual imagery has been considered important for the memory system, e.g., memory reliving in autobiographical memory (Brewer,1996; Rubin et al., 2003), as autobiographical memories typically take the form of visual images (Rubin, 2006; Tulving, 1984) and the more vivid the image, the stronger the memory retrieval. Thus, weak visual imagery vividness could dampen the ability to remember the past and plan the future, which has been noted to decrease in psychopathology, mostly in respect to positive memories. Usually people remember positive memories in their lives, but related to psychopathology (after trauma or in depression) intrusive and negative images may come into the mind involuntarily (Walker et al., 2003).
Working memory deficits are a core feature of schizophrenia (Forbes et al., 2009; Kang et al., 2011; Lee & Park, 2005). It has been found that individuals with stronger visual mental imagery perform better in visual working memory tasks (Keogh & Pearson, 2011). It has been investigated whether mental imagery and working memory share the same mechanism (Albers et al., 2013; Keogh & Pearson, 2011), whether or not they are “one and the same,” to use the words of Tong (2013). In every case, both of them represent and manipulate visual information. Thus, could weak visual imagery ability partially or fully explain poor working memory ability or the other way around? According to the preliminary studies by Baddeley and Andrade (2000), imagery vividness is dependent on working memory, i.e., in order to form a vivid image, one needs to maintain and manipulate visual information in the visuospatial sketchpad without disruption or interference. When the process of maintenance fails, then the vividness of images reduces. In our study, anxiety would be an explaining factor, interfering with the process of maintenance. In this study, we investigated cognitive performance on a general level using the g factor and did not study working memory separately. The g factor also included working memory tasks but was loaded most heavily on verbal learning tasks along with processing speed and executive functioning tasks (Lindgren et al., 2020). There was a trend approaching significance that controllability (not vividness) was also associated with cognitive performance, meaning that the better the neurocognitive performance, the better the ability to control imagery. In previous studies no systematic association between imagery ability and cognitive abilities has been found (Richardson, 1977; 1994). Oertel et al. (2009) also found that performance on cognitive tests is independent from the vividness of mental imagery.
Strengths and Weaknesses
We report results on mental imagery of non-emotional stimuli and the results do not tell about mental imagery regarding distressing stimuli or imagery in a distressed emotional state. The strength of our study is that both the vividness and controllability of mental imagery were assessed using well-validated methods. Broad clinical evaluation and cognitive assessment were done, and the sample included individuals with both affective and non-affective psychosis. Our results were practically the same when using the whole sample or just the non-affective subsample. Besides of this, the strength of our study was that we also took into account negative symptoms. Pearson et al. (2013) have criticized that mental imagery research of the individuals with schizophrenia has focused on the positive symptoms (f. ex., hallucinations) and the relationship with trait imagery, but not on the negative symptoms (blunted affect etc.).
The lack of a matched control group is a weakness in our study. Instead we compared our results with earlier published references to normative data, not directly comparable with our sample. Another limitation of this study is that the sample size is rather small for the number of variables and replication studies are thus needed. Symptom measures used may account for the differences in our findings compared to previous findings. Positive and negative symptom levels were only assessed using the BPRS interview and the issue of imagery among individuals with recent-onset psychosis should be further studied using also specific symptom scales. The discrepant findings from other studies were based largely on individuals with schizophrenia, whereas in our study sample, 2/3 was diagnosed with a schizophrenia spectrum psychotic disorder. This could be one reason for the different findings in our study compared to previous studies.
Also, assessing mental imagery ability using self-ratings questionnaires, there is a possibility that individuals may overestimate their imagery skills associated with social desirability (Allbutt et al., 2008; Di Vesta et al., 1971; Richardson, 1977). Therefore, other ways to measure mental imagery have been suggested (Pearson et al., 2013). For example, measuring imagery controllability, objective measures (visuospatial tasks) are recommended in addition to subjective methods like the CVIQ test (Lequerica et al., 2002). It is difficult to assess the reliability of the results on whether the subjects were really able to visualize and transform a given scenario. It has been stated that the CVIQ demands an ability for self-observation or insight (Richardson, 1972). However, the advantage of using the self-report test like CVIQ is that no gender differences have been found, contrary to the objective (the performance-based) tests (Campos, 2014b; Campos et al., 2004). In this study we did not analyze the effects of antipsychotic medication that most (83%) of the participants used. There are only a few studies on this topic. The study by Sack et al. (2005) did not find a significant influence of different antipsychotic medication on mental imagery vividness. Finally, our cross-sectional study does not inform us about whether mental imagery ability is a stable inter-individual trait that predicts the development and maintenance of mental disorders (Andrade et al., 2014; Pearson et al., 2013) or a state that depends on mental disorders. The inconsistent findings of the present study as well as the previous studies on this topic may also suggest that mental imagery is not a very relevant indicator of psychopathology of psychosis or a diagnostic marker.
Conclusion
Our findings do not support the claim (Böcker et al., 2000; Mintz & Alpert, 1972; Oertel et al., 2009; Sack et al., 2005) that mental imagery vividness is enhanced in people with psychotic disorder, nor that controllability is weak. Traditionally, vivid imagery has been found to associate with hallucinations. In this recent-onset psychosis sample, we found relationships between mental imagery and clinical symptoms that were contrary to some previous studies (Oertel et al., 2009; Sack et al., 2005). We found that stronger negative symptoms, depressive symptoms and anxiety associated with lower imagery vividness. However, an elevated mood associated with higher imagery vividness. According to Laing et al. (2016), anxiety and depression have an impoverishing effect on positive imagery influencing negatively future-oriented behavior, which is clinically important in the early course of psychosis. Decreasing anxiety and negative symptoms may increase imagery vividness, especially visual imagery vividness, which is an important modality in everyday tasks as well as in many cognitive skills, planning the future, and success in therapeutic interventions and treatment.
Footnotes
Acknowledgments
We thank Marjut Grainger, Sebastian Therman, and the whole of the Helsinki Early Psychosis Study group, as well as our participants.
Author Contributions
J. S. and T. K. are principal investigators in the Helsinki Early Psychosis Study and designed the original study protocol. L. A.-L. and M. L. participated in collecting the data, and J. S. was responsible for DSM-IV diagnoses. T. I. designed the focus of the study. L. A.-L. and M. L. undertook the statistical analysis. L. A.-L. wrote the first draft of the manuscript. All the authors contributed to and have approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the European Union’s Seventh Framework Programme for the project METSY—Neuroimaging platform for characterization of metabolic co-morbidities in psychotic disorders (#602478; J. S.), the Academy of Finland (#323035 and #278171; J. S.), the Finnish Cultural Foundation (J. S.), and the Sigrid Jusélius Foundation (J. S.). The funding organizations played no further part in the study design; in the collection, analysis, and interpretation of data; or in the writing of the paper.