
Abstract
Background
The Australian National Bowel Cancer Screening Program (NBCSP), which provides 2-yearly screening to people aged 50 to 74 y, had a phased rollout from 2006 and was fully implemented in 2020. To measure the effectiveness of the NBCSP accounting for age-specific trends, we aimed to develop a novel integrative method to project colorectal cancer (CRC) incidence rates from 2006 to 2045 in the absence of the NBCSP (referred to as “no-NBCSP projections”) while addressing the challenge of complex age-specific trends in CRC incidence.
Methods
We constructed a new dataset by replacing the observed data for NBCSP-eligible individuals aged 50 to 74 y with intermediate projections based on pre-NBCSP data from 1982 to 2005. We compared the no-NBCSP CRC incidence projected using a standard age-period-cohort (APC) model, age-stratified APC models, and the integrative modeling approach.
Results
The integrative modeling approach captured complex age-specific trends better than the standard and age-stratified APC models did. Without the NBCSP, the overall CRC incidence rates would be expected to decline from 2005 to 2025, followed by increases from 2026 to 2045. The incidence rates for those aged <50 y would be projected to continue increasing to 2045, and an increase in incidence rates for older age groups would be projected to occur from 2020 for ages 50 to 54 y, from 2030 for ages 65 to 74 y, and from 2035 for ages 75 y and older.
Conclusions
These no-NBCSP projections provide a counterfactual benchmark against which to measure the impact of the NBCSP on CRC incidence in Australia, and they have been used as new calibration targets for a simulation model of CRC and screening in Australia. The methods developed here could be used to generate comparators to assess the impact of other public health interventions.
Highlights
We constructed counterfactual projections of colorectal cancer (CRC) incidence rates in the absence of the National Bowel Cancer Screening Program (no-NBCSP projections).
To do this, we developed a new integrative modeling approach to capture complex age-specific colorectal cancer incidence trends.
These no-NBCSP projections provide a counterfactual benchmark against which to measure the impact of the NBCSP on CRC incidence in Australia.
These projections stress the need for ongoing assessment of the starting age for the NBCSP, to tackle the increasing incidence for people younger than 50 y.
This is a visual representation of the abstract.
Keywords
Introduction
Estimates of cancer incidence and mortality in 2024 show colorectal cancer (CRC) to be the fourth most commonly diagnosed cancer (excluding nonmelanoma skin cancers) and the second most common cause of cancer death in Australia. 1 Fortunately, there has been a decrease in CRC incidence rates for Australians older than 50 y of age, initially occurring in the 1990s for those aged 50 to 54 y, followed by a gradual decline for older age groups (e.g., for those aged 65 to 74 y beginning in the early 2010s). Opportunistic screening (fecal occult blood test or colonoscopy), which can prevent CRC by detecting and removing precancerous polyps, has been available since the mid-1990s2,3 and is likely to have contributed to the decline in CRC incidence rates for people older than 50 y. 4 The Australian National Bowel Cancer Screening Program (NBCSP) is an organized population screening program that provides 2-yearly immunochemical fecal occult blood tests (iFOBTs) to individuals aged 50 to 74 y. The NBCSP, introduced in 2006 in a phased rollout, was fully implemented by the end of 2020. 5 However, in contrast to the decreases in incidence rates observed for older Australians, a recent study has shown that CRC incidence rates for Australians younger than 50 y have increased over the past 2 decades, 6 a trend also seen in other countries. 7 It is important to account for these conflicting incidence trends, especially when evaluating the effectiveness of the NBCSP now and in the future.
Counterfactual projections of the cancer burden can provide essential estimates of the CRC incidence rates and numbers of new cases that would have occurred if the NBCSP had not been implemented. Such projections are critical as a benchmark against which to assess the effectiveness of the NBCSP and for optimizing the program further. Age-period-cohort (APC) models are a flexible statistical projection method that can effectively capture various factors contributing to cancer incidence. 8 However, a standard statistical APC modeling approach assumes common period effects across different birth cohorts. Thus, the standard approach may not be able to capture the conflicting trends in the observed CRC incidence rates across younger and older age groups. For example, a standard APC model estimated a decrease in the incidence rate for younger age groups, rather than the observed increasing trend; this is likely due to the model fitting being dominated by the decreasing CRC incidence since the 1990s for people aged 50+ y (who represent the overwhelming majority of CRC cases). Therefore, a more sophisticated modeling approach is needed.
In this study, we aimed to develop a novel integrative modeling approach to construct counterfactual projections of CRC incidence rates from 2006 to 2045 in the absence of the NBCSP (hereafter referred to as “no-NBCSP projections”). This approach is designed to capture changes in trends, especially for younger age groups, and to account for the effect of opportunistic screening, while excluding the effects of the NBCSP in Australia. This method can be used broadly to generate counterfactual projections that exclude the influence of any newly introduced age-specific interventions, such as a screening program.
Methods
Data Sources
Appendix Figure A1 summarizes the data sources used in this study. We obtained national tabulated data on the numbers of new cases for CRC (ICD-10 codes C18 for colon cancer and C19-C20 for rectal cancer) in Australia by sex, 5-y age group, and calendar year from 1982 to 2018 from the Australian Institute of Health and Welfare (AIHW). 9 The numbers of new cases by single calendar year were smoothed using a 3-y moving average. The reporting of incident invasive cancer is mandatory in all Australian states and territories, with data sent to the AIHW for national reporting. 9 All registries conform to the International Agency for Research on Cancer’s criteria for population-based cancer registration, are “A” quality rated, and have their data published in the “Cancer Incidence in Five Continents” series. 10 Australian population data by sex, 5-y age group, and calendar year from 1982 to 2045 were obtained from the Australian Historical Population Statistics and Population Projections (Series B, based on medium population growth) produced by the Australian Bureau of Statistics (ABS).11,12 As projection model validation is critical,13,14 the New South Wales Cancer Registry (NSWCR) data on colon and rectal cancer incidence by sex and 5-y age group from 1972 to 1995 were used to evaluate the integrative modeling approach developed in this study.
To understand the impact of opportunistic screening over time, we analyzed Services Australia’s Medicare Benefits Schedule (MBS) data for colonoscopies over the period January 1994 to December 2021. 2 The MBS records include health services subsidized by the Australian Government. MBS item codes for colonoscopy are listed in Appendix Table A1. Appendix Figure A2 shows the rates of colonoscopy by sex and age group during 1994 to 2021 in Australia, illustrating increasing trends across all age groups from 2005 to 2018. It is important to note that not all colonoscopies are conducted for opportunistic screening. Since 2006, approximately 10% to 15% of colonoscopies have been performed as part of the NBCSP, either as follow-up to positive iFOBT results or for surveillance of individuals with a history of colorectal polyps that were identified through the NBCSP and then removed. 15
Projection Methods
The modeling process for the counterfactual no-NBCSP projections involves 2 related analytical steps (Figure 1), with APC models used as the basic projection method, as detailed below.
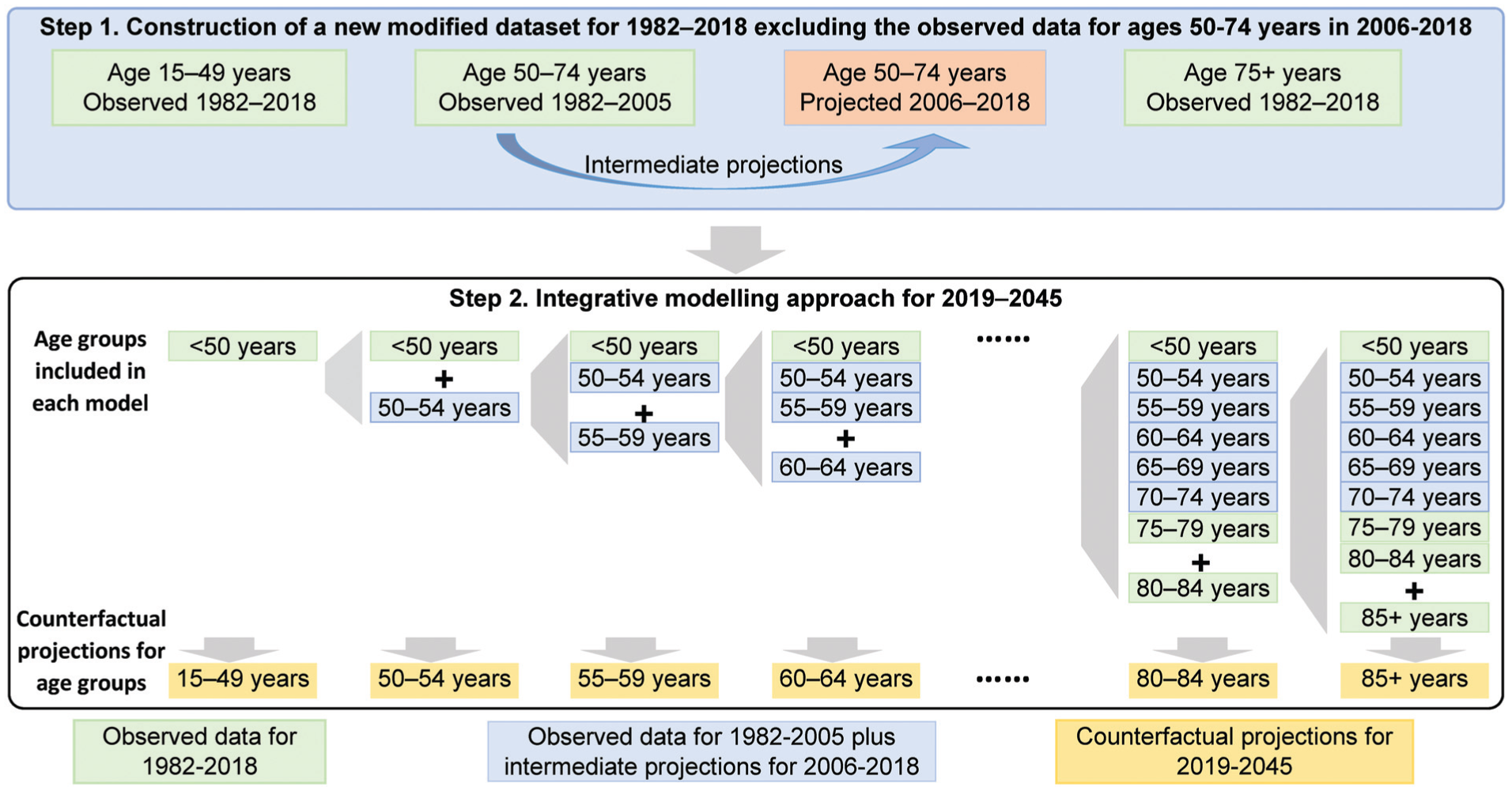
Conceptual model for the new integrative modeling approach.
Basic projection model: Standard APC model
Detailed methods for standard APC models can be found in the published literature 16 and are summarized in Appendix 3. Standard APC models were fitted by the apcspline command in Stata 17 with natural cubic splines for smoothing. 16 APC models may effectively capture some of the factors that contribute to cancer incidence, as age, period, and cohort effects can be considered to be surrogates for exposure to a range of risk factors and other cancer diagnostic factors. 8 For example, period effects can reflect diagnostic factors that lead to changes in disease incidence across all age groups, 8 while the cohort effect may represent risk factors or cancer screening participation that changes from generation to generation.8,17,18 Details on the model assumptions are provided in Appendix Table A2.
Counterfactual no-NBCSP projection method
Step 1. Create modified datasets excluding the effect of the NBCSP
We created modified datasets by combining the following data subsets:
Observed data from 1982 to 2018 for age groups <50 y and age groups 75+ y, who were not eligible for the NBCSP during this period.
Observed data for age groups 50 to 74 y for the pre-NBCSP period from 1982 to 2005.
Intermediate projections for age groups 50 to 74 y from 2006 to 2018, obtained by fitting a standard APC model to the data subset (2) from 1982 to 2005. We calculated the uncertainty interval (UI) as the confidence interval of the intermediate projections based on the variances of the parameters in the APC model.
Three modified datasets were created comprising: (a) these 3 data subsets, (b) the first 2 subsets and the lower bounds of the 95% UIs of the intermediate projections, and (c) the first 2 subsets and the upper bounds of the 95% UIs of the intermediate projections (Appendix Figure A3).
Step 2. New integrative modeling approach
Using the modified datasets created in the first step, we developed a new integrative modeling approach (Figure 1). This approach is designed to capture complex trends in age-specific incidence rates (e.g., increase in younger age groups and decrease in older age groups) while excluding the effects of the NBCSP in Australia.
The integrative modeling approach was implemented through an iterative process. First, a standard APC model was used to project the number of new CRC cases for individuals younger than 50 y from 2019 to 2045, using data for age groups younger than 50 y from 1982 to 2018. Then, projections for older age groups (50+ years) were constructed through a stepwise addition of successive age groups (Figure 1). For example, the projection for the 60- to 64-y age group was generated from an APC model fitted to the data including ages up to 64 y, with data for age groups <60 y included in the model fitting to inform period and cohort effects. This stepwise approach aimed to propagate the increasing trends observed in younger age groups to older age groups. Through this stepwise addition of older age groups into the model that included data for younger age groups, the period and cohort effects can better capture the patterns emerging in the younger age groups. In addition to the model assumptions for standard APC models, when propagating the increasing trends from younger to older age groups, there is an implicit assumption that there will be no future changes in underlying factors, such as changing exposures or the implementation of new cancer control initiatives during the projection period (Appendix Table A2).
Reflecting different sources of uncertainty in final counterfactual no-NBCSP projections
The UI of the final no-NBCSP projections reflects multiple sources of uncertainty, as shown in Appendix Figure A3. The main estimates for the final no-NBCSP projected numbers of cases were constructed using the modified dataset (a) from step 1 and the medium series of population projections. The upper uncertainty bounds for the final no-NBCSP projections were based on the upper bounds of the 95% UI for the intermediate projections in step 1 (3), the upper bounds in the subsequent integrative modeling in step 2, and the high series of population projections. The lower bounds of the 95% UI for the final no-NBCSP projections were constructed analogously using the lower bounds of the 95% UIs in steps 1 (3) and 2 and the low series of population projections. For simplicity, in this study, we estimated the UI based on the variance of the parameters in the model in each step without resampling the data. As such, these UIs capture only some aspects of the uncertainty and should not be interpreted probabilistically.
Model Selection of the Integrative Modeling Approach
In general, the most appropriate projection method is selected based on the model fit statistics (i.e., lowest Bayesian information criterion), validated using observed data by withholding the most recent data from the model fitting, and then comparing the projected rates for those years with the actual rates. However, there are no observed data available to inform the CRC incidence trends and projections for ages 50 to 74 y in the absence of the NBCSP. Therefore, the counterfactual no-NBCSP CRC projections cannot be directly validated, as the scenario is hypothetical.
Thus, instead, selection of the final model was based on the performance of the no-NBCSP CRC incidence projections when used in the recalibration of Policy1-Bowel, a well-established microsimulation model for the natural history of CRC in the Australian population. 4 The full details of Policy1-Bowel have been reported elsewhere.4,19 In brief, Policy1-Bowel is a well-established microsimulation model that simulates the natural disease history of CRC including precancerous lesions, incidence, survival, and mortality. Policy1-Bowel simulates 20 million individuals with natural history parameters relating to the initiation, growth, and progression of precancerous lesions to CRC, and these were well calibrated to clinical trials. 4 It has been used to evaluate the effects of the NBCSP in Australia by simulating screening participation rates.4,19,20 Therefore, in this study, Policy1-Bowel was used to evaluate the no-NBCSP CRC incidence projections as a backward evaluation process.
The model selection process is illustrated in Appendix 6 Figure A4, and the detailed recalibration process has been described elsewhere. 19 In brief, we generated a number of no-NBCSP incidence projections with different numbers of knots for the age, period, and cohort in each APC model component. A set of no-NBCSP incidence projections was initially selected based on the model fit statistics (i.e., lowest Bayesian information criterion). Policy1-Bowel was recalibrated to these no-NBCSP CRC incidence projections. We then used this recalibrated Policy1-Bowel to simulate an overall ∼40% NBCSP participation rate (the reported NBCSP participation rate in 2006–2018) 21 and generated CRC incidence projections from 2006 to 2018 in the presence of the NBCSP. The resulting CRC incidence projections were then compared with the observed CRC incidence data, which included the effect of the NBCSP from 2006 to 2018. 19 If the patterns were inconsistent, we adjusted the integrative model settings to obtain updated no-NBCSP incidence projections and repeated the process until the differences between the Policy1-Bowel projections for the CRC incidence rates in the presence of the NBCSP and the observed incidence rates from 2006 to 2018 were minimized. 19
Model Validation of the Integrative Modeling Approach
As discussed above, it was not possible to directly validate the no-NBCSP CRC projections as the scenario is hypothetical. For validation of the integrative modeling approach in this study, we evaluated the performance of the method in capturing complex age-specific trends that do not include the sharp change due to the impact of opportunistic or organized screening activities. This validation is possible only with data up to 1995, before any opportunistic or organized screening was introduced in Australia. As national incidence data are available only from 1982, we used the NSW incidence data from the NSWCR from 1972 to 1995 to assess the performance of the projections from the integrative modeling approach. All states and territories (including NSW) have legislation that makes cancer notifiable to state-specific cancer registries, and each registry supplies the data to the AIHW to be compiled into the national data. 1 NSW is the most populous state in Australia with almost one-third of the total population (8.6 million in 2025), 22 and the NSWCR is the largest state-based population-wide registry in Australia. In addition, NSW colon and rectal cancer incidence rates are in good agreement with the national rates (median differences: 1.0 to 2.2 per 100 000) (Appendix Figure A5). 23 Previously, NSW data have been used for evaluating CRC mortality rates in the Australian context. 24 We applied the integrative modeling approach using NSWCR data from 1972 to 1980 (the data for model fitting do not overlap with the national data from 1982) to project rates from 1981 to 1995 and then compared the projected rates with the corresponding actual observed NSWCR rates from 1981 to 1995.
Comparison of projection approaches
To evaluate the performance of the integrative modeling approach in capturing complex age-specific trends compared with different approaches, we also fitted a standard APC model and separate age-stratified APC models for ages <50 y and 50+ y using the same modified datasets. The no-NBCSP projections were compared with the observed CRC incidence rates for younger age groups <50 y and the cohort-specific rates to understand the propagation of trends in younger age groups to older age groups.
All models were developed separately for males and females and by cancer subtypes. All analyses were performed using Stata (version 17.1, Stata Corporation, College Station, TX, USA). Unless stated otherwise, all age-standardized rates presented in the main results of this article were standardized to the 2001 Australian standard population.
Results
For both males and females, the observed incidence rates of colon cancer were higher than those of rectal cancer, with variations by sex and age groups (Figure 2a and Appendix Figure A6). From 1982 to 2018, opposing and fluctuating trends in CRC incidence rates were observed across different age groups. For instance, the colon cancer incidence rate among individuals younger than 40 y began to rise in the mid-1990s. In contrast, the rate for the 50- to 54-y age group decreased from the early 1990s (Figure 2a).
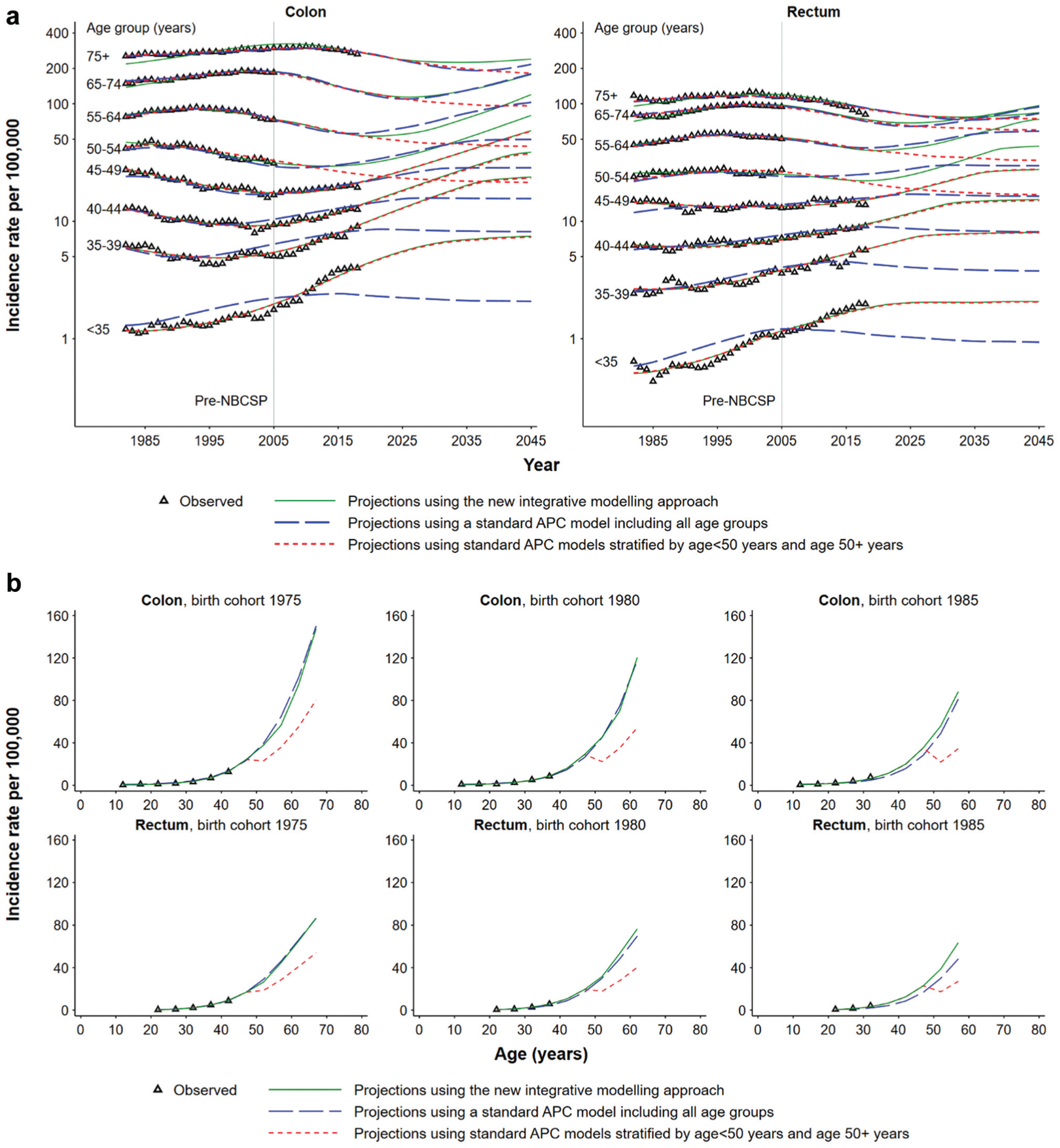
Comparison of incidence trends for colon and rectal cancers in Australia captured by different projection approaches: (a) age-specific rates and (b) cohort-specific rates.
Comparison of Model Performance in Capturing Complex Trends in Age-Specific Incidence Rates
The standard APC model including all ages could not accurately capture the opposing trends in cancer incidence rates for younger and older age groups. For younger age groups, the model fit was poor and estimated a decreasing rather than increasing trend for ages <50 y, even during the period for which observed data were available (Figure 2a). Fitting separate APC models for ages <50 y and ages 50+ y captured the increasing trends in incidence rates for younger age groups, but these trends were not propagated to the older age groups, resulting in an illogical pattern in cohort-specific rates across ages (Figure 2b). By contrast, the newly developed integrative modeling approach appeared to capture recent trends from the younger age groups (Figure 2a) and propagate them to older age groups with consistent cohort-specific rates (Figure 2b). Therefore, this approach was used as the final method for obtaining the counterfactual no-NBCSP projections.
Counterfactual No-NBCSP Projections Using the Integrative Modeling Approach
The observed and projected overall age-standardized and age-specific CRC incidence rates for a no-NBCSP counterfactual scenario in Australia are presented in Figure 3 and Appendix Table A3. In this counterfactual no-NBCSP scenario, the overall age-standardized incidence rates for CRC for both males and females would be projected to continuously decline over the period 2005 to the mid-2020s and then increase from 2025 to 2045 (Figure 3). If the NBCSP had not been implemented in Australia, the age-standardized incidence rates for colon cancer would be projected to decline from 43.5 per 100,000 in 2005 to 35.0 per 100,000 in 2025 and then increase to 53.7 per 100,000 in 2045. Similar patterns would be projected for rectal cancer, with incidence rates for rectal cancer projected to decline from 22.2 per 100,000 in 2005 to 17.9 per 100,000 in 2020, then increase to 25.5 per 100,000 in 2045 (Appendix Table A3).
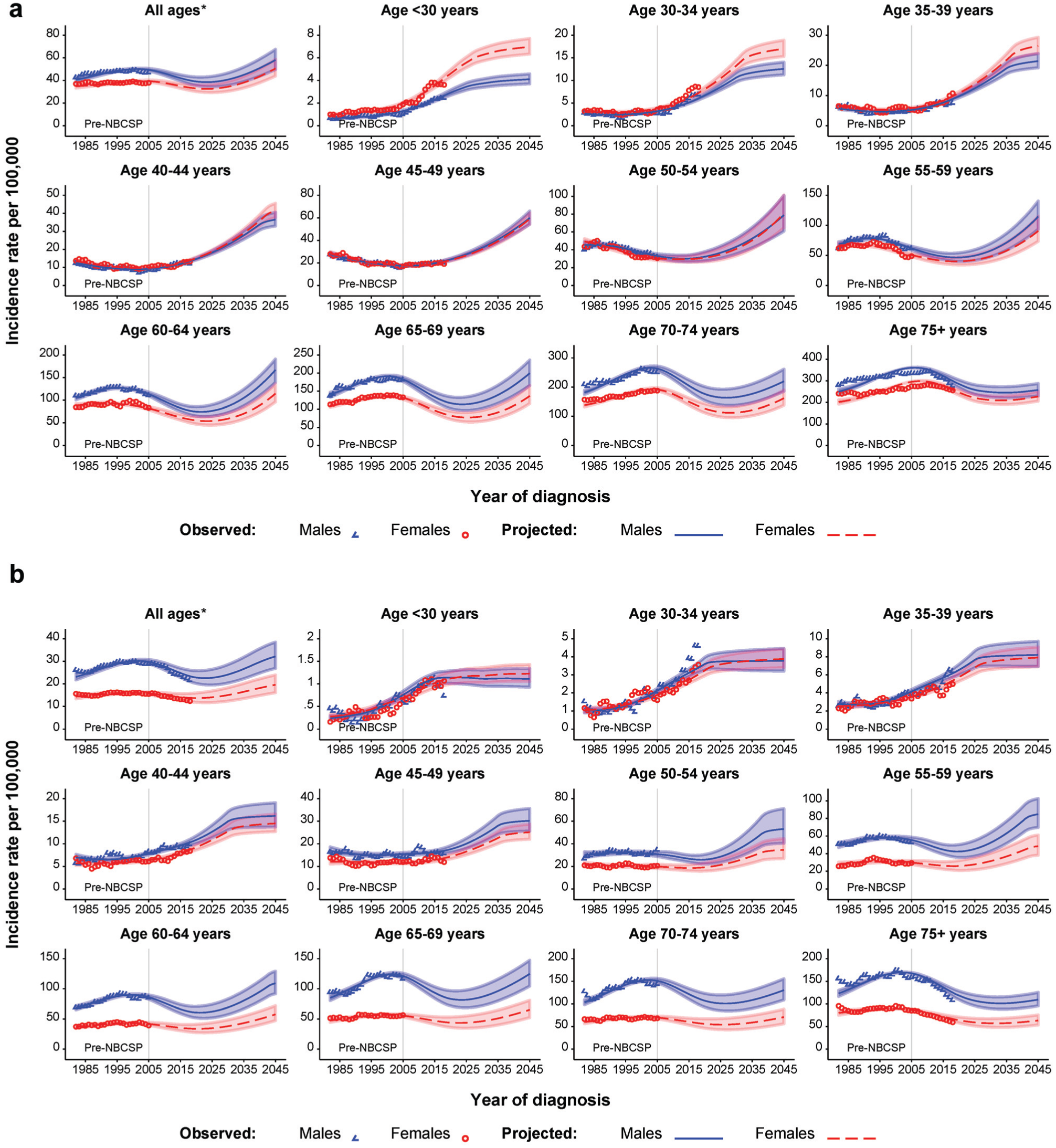
Observed and projected age-specific incidence rates for colon and rectal cancer in the absence of the National Bowel Cancer Screening Program (NBCSP) in Australia, using the new integrative modeling approach: (a) colon cancer and (b) rectal cancer.
For both males and females, our projections suggest that increasing colon cancer incidence rates for males and females aged <50 y would continue to 2045 in the no-NBCSP scenario and for rectal cancers would be expected to level off from the 2030s (Figure 3). The age-standardized incidence rates for colon cancer aged <50 y would be projected to more than triple over 2005 to 2045, increasing from 4.3 per 100,000 in 2005 to 16.2 per 100,000 in 2045. The incidence rates for rectal cancer in people aged <50 y would be projected to double over this period, increasing from 2.8 per 100,000 in 2005 to 5.8 per 100,000 in 2045 (Appendix Table A3).
In the absence of the NBCSP, the incidence rates for males and females aged 50 to 54 y would be projected to decline steadily from the 1990s to the late-2010s but increase from 2020 to 2045. A similar pattern would be projected to occur 5 to 20 y later for each of the older age groups after propagating the increasing trend in younger to older age groups. For rectal cancer, the decline in rates from the 1990s to 2010s would be projected to occur at a slower pace than for colon cancer (Figure 3). If the NBCSP had not been implemented in Australia, the age-standardized incidence rates for colon cancer for ages 50 to 74 y would be projected to decrease from 96.2 per 100,000 in 2005 to 66.8 per 100,000 in 2025 and then increase to 124.7 per 100,000 in 2045. Similar patterns would be projected for rectal cancer, with incidence rates for rectal cancer in people aged 50 to 74 y projected to decline from 57.9 per 100,000 in 2005 to 44.1 per 100,000 in 2020, then increase to 71.5 per 100,000 in 2045 (Appendix Table A3).
Assessing the New Integrative Modeling Approach
Figure 4 shows the comparison of the NSW 15-y projected and observed age-standardized incidence rates for colon and rectal cancer from 1981 to 1995. During the overall period from 1972 to 1995, decreases in CRC incidence rates among individuals aged <45 y were observed, whereas the rate for the age groups 45 to 49 and 50 to 54 y increased from 1972 and decreased around the 1990s (Figure 4). The patterns of projected rates from 1981 to 1995 for both colon and rectal cancer and for males and females are generally close to the observed patterns, suggesting that the integrative modeling approach can capture the opposing trends in incidence rates for younger and older age groups.
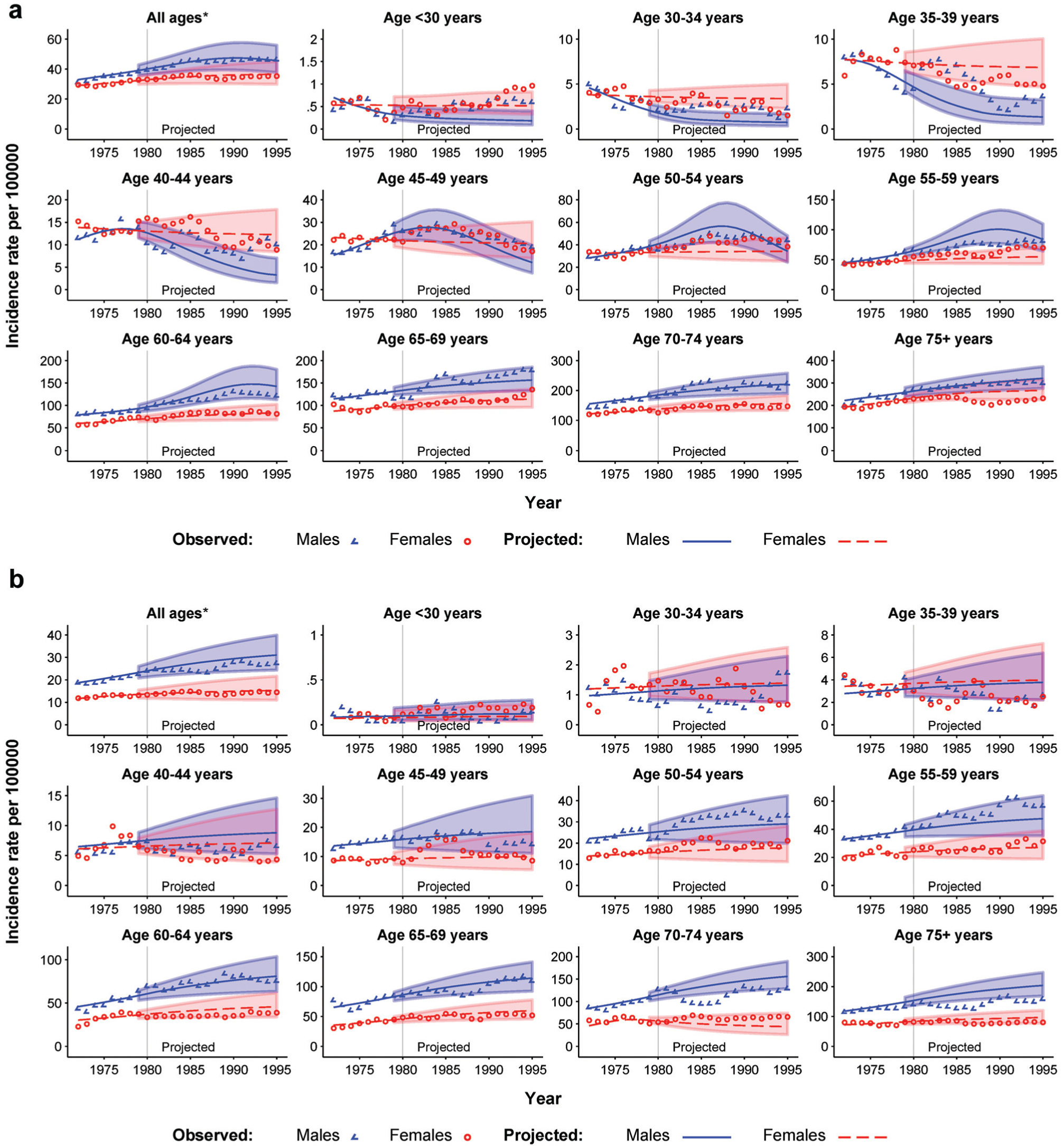
Validation of 15-y projections for colon and rectal cancer age-specific incidence rates in NSW using the integrative modeling approach: (a) colon cancer and (b) rectal cancer.
Discussion
We developed a new integrative modeling approach to generate counterfactual benchmarking projections of CRC incidence rates in Australia in the absence of the NBCSP. In this no-NBCSP scenario, our projections suggest that increasing colon cancer incidence rates for males and females younger than 50 y of age would continue to 2045, and rectal cancer rates would be expected to level off from the 2030s. Propagating these increasing trends in younger age groups to older age groups in the absence of the NBCSP, our projections suggest that CRC incidence rates for older age groups would have increased after the mid-2020s. These projections stress the need for ongoing assessment of the starting age for the organized screening program, to tackle the increasing incidence for people younger than 50 y. 6
The new integrative modeling approach that we developed can be more generally useful as a method to generate counterfactual estimates that can be used as comparators to assess the impact of public health or other interventions, particularly those for asymptomatic populations. Assessing such interventions for populations that are experiencing complex age-specific trends in underlying disease incidence, such as CRC, requires a thorough understanding of how those trends would continue in the absence of the intervention. The methods described here provide a way to generate such estimates.
These no-NBCSP projections aim to capture the effects of background factors other than the NBCSP in Australia, such as trends in risk factors, and have been used as calibration targets for the Policy1-Bowel model. 19 Policy1-Bowel is a microsimulation model that is used to evaluate the long-term impact of the NBCSP on CRC outcomes and costs in Australia.4,25 Previous versions of Policy1-Bowel assumed that the underlying age-specific risk of CRC and other factors remain constant, excluding cohort and period effects. 4 By including the updated counterfactual no-NBCSP projections generated in this study, the newly recalibrated Policy1-Bowel is able to capture detailed trends in CRC incidence for younger age groups, including the effect on their lifetime cancer risk and how this impacts the effectiveness of screening. The recalibrated Policy1-Bowel was used to inform Australian National Health and Medical Research Council–endorsed clinical practice guidelines, including providing evidence to support new recommendations to lower the eligible starting age for the NBCSP from 50 to 45 y.19,26 This would not have been possible without the benchmarking projections from this study. This change in screening recommendations has since been implemented, with the NBCSP including people 45 to 49 y old in an opt-in basis. 26
The main advantage of our integrative modeling approach for counterfactual no-NBCSP CRC incidence projections is that it propagates the increasing trend in younger age groups 6 to older age groups over time, which is critical for informing planning for the NBCSP.19,26 Except for the slight increase in the use of colonoscopy in this younger age group (Appendix Figure A2), it is likely that changes in risk factor exposures could be the key drivers behind the increasing CRC incidence rates for younger age groups. 27 The prevalence of overweight and obesity in children, adolescents,28,29 and adults has been increasing over recent years and is projected to continuously increase to 2025.30,31 Lack of physical activity, 32 diets low in fiber, and high consumption of red or processed meats are also likely to have contributed to this increased incidence pattern. 6 A recent evidence update has also highlighted the consumption of sugary drinks as a risk factor for CRC 33 ; in Australia, 9.1% of adults and 7.1% of children consume them daily, 34 which may also contribute to changes in CRC incidence.
Another advantage of our integrative modeling approach for counterfactual no-NBCSP projections is the ability to capture the effect of opportunistic screening, which has been occurring since the mid-1990s. When excluding the observed data for ages 50 to 74 y from 2006 onward from the model fitting, we found that the projected age-standardized incidence rates for colon and rectal cancers from 2006 to 2018 were close to the observed rates including the early years of the NBCSP roll out. There are several possible explanations for the similar incidence rates in the absence of the NBCSP. First, limited eligibility for, and uptake of, the NBCSP in those early years limited the impact of the screening program on national incidence rates. 19 Second, opportunistic screening likely contributed to the decline in the observed incidence rates of colon and rectal cancer from the early 2000s to the late 2020s, with early detection and removal of precancerous lesions leading to a decrease in the cancer incidence. 35
This study has some limitations. As with all modeled projections, the main limitation is that the projections are dependent on the assumptions made (detailed model assumptions are summarized in Appendix 3), and there is always uncertainty when extrapolating current trends into the future. The models assumed that the relative risk due to the age effects will remain unchanged over time. For older age groups (50–74 y) from 2006 to 2018, we assumed that period and cohort effects in the intermediate projections are the same as the period and cohort effects for 2005 in the absence of the NBCSP. It is also assumed that future cohort and period effects are equal to cohort and period effects in the most recent fitted data. 16 In addition, when propagating the increasing trends from younger age groups to older age groups from 2019 to 2045, these projections do not take into account any future changes in underlying factors, such as changing exposures or the implementation of new cancer control initiatives. By design, counterfactual projections cannot be fully validated. We could not explicitly capture the lead-time effects of screening in our projections; however, these effects are captured in the Policy1 model as it simulates full NBCSP screening, including changes in time of diagnosis and the impact on survival times. Moreover, the population denominators were projected by the ABS, 12 and this adds further uncertainty to our projections. In addition, the UIs reported in this study were derived from the variances of the model parameters rather than using a resampling approach and therefore capture only some aspects of the uncertainty. Future research should explore an approach that assigns probability distributions to uncertain quantities and propagates uncertainty to the outputs (e.g., using bootstrapping and/or Monte Carlo simulations) to obtain conservative, probabilistically interpretable UIs for integrated projections.
Despite these limitations, this study and its methods have many strengths. First, the long-term observed incidence data used in this study are known to be of high quality and have high population coverage. 36 Second, this study used APC models as the basic modeling approach during the integration steps to project incidence rates, which can successfully implicitly capture the factors that contribute to CRC incidence at a population level. 8 Third, this new integrative modeling approach for counterfactual no-NBCSP projections accounted for the no-NBCSP factors that contributed to the CRC incidence trends, including opposing trends for younger and older age groups. This integrative modeling approach may be applicable elsewhere: it is broadly generalizable to other diseases, providing counterfactual benchmark incidence rates in the absence of screening or other specified interventions for comparison with incidence rates with the intervention. Furthermore, this integrative modeling approach was able to successfully and accurately propagate the increasing trends in younger age groups to older ages. This was demonstrated in the validation exercise, which showed that this modeling approach could capture opposing trends in age-specific incidence rates and provide accurate and meaningful projections. Also, this approach could be generalized for projections related to other diseases, in which complex patterns in incidence or mortality rates across age groups need to be captured.
This study provides previously unavailable information on counterfactual projections of CRC incidence in the absence of the NBCSP in Australia to 2045. Assuming no NBCSP in Australia, our projections from our newly developed integrative modeling approach suggested that incidence rates for CRC would decrease from 2000 to the mid-2020s, followed by increases in the rates from 2025 onward. This means that continued efforts to optimize the organized cancer screening program and control risk factors, including smoking prevalence, obesity, physical inactivity, and alcohol use, will remain significant public health priorities. The estimates generated by this study will be key to evaluating the impact of these cancer control activities. In particular, as the eligible screening age for the NBCSP has recently been lowered, so that individuals from age 45 y are now eligible for the NBCSP, these projections provide the counterfactual benchmark against which to evaluate the impact of the lowered screening age in the future.
Supplemental Material
sj-pdf-1-mdm-10.1177_0272989X251393257 – Supplemental material for A New Integrative Modeling Approach for Generating Counterfactual Projections of Colorectal Cancer Incidence Rates in the Absence of Organized Screening in Australia
Supplemental material, sj-pdf-1-mdm-10.1177_0272989X251393257 for A New Integrative Modeling Approach for Generating Counterfactual Projections of Colorectal Cancer Incidence Rates in the Absence of Organized Screening in Australia by Qingwei Luo, Jie-Bin Lew, Joachim Worthington, Clare Kahn, Han Ge, Emily He, Michael Caruana, Michael David, Dianne L O’Connell, Karen Canfell, Julia Steinberg and Eleonora Feletto in Medical Decision Making
Footnotes
Acknowledgements
This research was completed using data from the Cancer Data Linkage (Candles) Initiative. The CanDLe Initiative is led by the Cancer Institute NSW and supported by the NSW Ministry of Health. This work was undertaken to support the 2023 review and update of the Population Screening chapter of the Clinical Practice Guidelines for the Prevention, Early Detection and Management of Colorectal Cancer, which were auspiced by Cancer Council Australia and the Australian Government’s Department of Health and Aged Care. This work is a component of the Cancer-Patient Population Projections project funded by a Medical Research Future Fund (MRFF) Preventive and Public Health Research Initiative: 2019 Target Health System and Community Organisation Research Grant Opportunity (MRF1200535). KC and JBL report grant funding from the National Health and Medical Research Council of Australia (APP1194679 and APP1194784, respectively). JS is a recipient of a Cancer Institute NSW Career Development Fellowship (2022/CDF1154).
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KC is co-principal investigator of an investigator-initiated trial of cervical screening, Compass, run by the Australian Centre for Prevention of Cervical Cancer (ACPCC), which is a government-funded not-for-profit charity; the ACPCC has received equipment and a funding contribution from Roche Molecular Diagnostics and operational support from the Australian Government. KC is also co-principal investigator on a major investigator-initiated implementation program Elimination of Cervical Cancer in the Western Pacific, which will receive support from the Minderoo Foundation, the Frazer Family Foundation, and equipment donations from Cepheid. Neither KC nor her institution on her behalf receives direct funding from industry for any project. MC is an investigator on an investigator-initiated trial of cytology and primary HPV screening in Australia (‘‘Compass’’) (ACTRN12613001207707 and NCT02328872), which is conducted and funded by the Australian Centre for the Prevention of Cervical Cancer, a government-funded health promotion charity. The ACPCC has received equipment and a funding contribution for the Compass trial from Roche Molecular Systems and operational support from the Australian Government. However, neither MC nor his institution on his behalf receive direct or indirect funding from industry for Compass Australia. These disclosures do not constitute a conflict of interest for the present study, and so the authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was undertaken to support the 2023 review and update of the Population Screening chapter of the Clinical Practice Guidelines for the Prevention, Early Detection and Management of CRC, which were auspiced by Cancer Council Australia and the Australian Government’s Department of Health and Aged Care. This work is a component of the Cancer-Patient Population Projections project funded by a Medical Research Future Fund (MRFF) Preventive and Public Health Research Initiative: 2019 Target Health System and Community Organisation Research Grant Opportunity (MRF1200535). KC and JBL report grant funding from the National Health and Medical Research Council of Australia (APP1194679 and APP1194784, respectively). JS is a recipient of a Cancer Institute NSW Career Development Fellowship (2022/CDF1154).
Authors’ Contributions
EF and KC: conceived the study. QL and JBL: designed the study, conducted the statistical analysis, interpreted the results, and drafted the manuscript. JS, JBL, KC, and EF: contributed to the design and methods used. All authors contributed to drafting the manuscript, made a substantial contribution to the interpretation of the results, critically revised the manuscript, approved the final manuscript, and agreed to be accountable for all aspects of the article. KC, EF, and JS: secured funding for the study.
Ethical Considerations
This study used existing tabulated national data for colorectal cancer incidence released by the Australian Institute of Health and Welfare. Ethics approval and patient consent were not required to use these aggregated data. The validation analysis using the tabulated data for colorectal cancer incidence from the New South Wales (NSW) Cancer Registry and received ethics approval from the NSW Population and Health Services Research Ethics Committee (2019/ETH12584) for the Cancer Institute NSW’s Enduring Cancer Data Linkage (CanDLe).
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
ORCID iDs
Data Availability
The tabulated data on national colorectal cancer incidence are available at https://www.aihw.gov.au/reports/cancer/cancer-data-in-australia/contents/summary. The Medicare Benefits Schedule data are available at ![]() . The NSW CanDLe data were stored in the Secure Unified Research Environment facility and we, as authorized researchers, were given encrypted access with strong authentication.
. The NSW CanDLe data were stored in the Secure Unified Research Environment facility and we, as authorized researchers, were given encrypted access with strong authentication.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.