
Abstract
Highlights
The impact of non-clinical factors (e.g., resident and family preferences) on prescribing is well-established. There is a gap in the literature regarding the mechanisms through which these preferences are experienced as pressure by prescribers within the unique context of residential aged-care facilities (RACFs).
A significant relationship was found between nurses’ anxiety, clinical tolerance of uncertainty, and the perceived need for antibiotics and assessment.
As such, there is a need to expand stewardship beyond education alone to include interventions that help nurses manage uncertainty and anxiety and include other stakeholders (e.g., family members) when making clinical decisions in the RACF setting.
Keywords
Antibiotic resistance continues to be a problem of growing global concern, with approximately 50% of antibiotic prescribing considered to be inappropriate in residential aged-care facilities (RACFs). 1 Multiple sources of uncertainty have been identified in complex health care environments, such as RACFs: 1) scientific uncertainty (pertaining to diagnosis, prognosis, causal explanations, and treatment recommendations), 2) practical uncertainty (issues of structures and processes of care and systems), and 3) personal uncertainty (psycho-social, existential, and ethical issues).2–5 Infections in the older population often present atypically, with comorbidities and higher risk of complications or adverse reactions and challenges in communication due to cognitive impairments (e.g., difficulties in articulating medical history or pain levels), all of which increase scientific uncertainty.6,7 High workloads, poor staff ratios, and rotating prescribers likely contribute to fragmentation of information and breakdown in continuity of care, to increase practical uncertainties.8–13 Prescribers also report experiencing pressure to empirically prescribe antibiotics from nurses and family members in these contexts. 7 As such, high uncertainty, perceptions of risk, and pressure to prescribe empirically in the context of time constraints appear to contribute to the use of antibiotics as a safety net; however, the mechanisms through which this occurs in RACFs remain unclear. 14
In Australia, the responsibility for prescribing antibiotics usually rests with visiting general practitioners (GPs), and phone prescribing remains common practice. 15 In some local health districts, specialized nurse practitioners with prescribing authority can be called in an emergency, but GPs have the primary responsibility for the medical needs of residents under their care. 16 The staff of RACFs usually includes a nurse facility manager, registered nurses (RNs), enrolled nurses (ENs), and personal care assistants. Although nurses do not prescribe antibiotics, off-site prescribers report relying heavily on RNs and ENs to provide diagnostic histories (particularly in the context of cognitive decline), monitoring changes in residents’ clinical status (particularly in the context of atypical presentations and absence of having face to face data regarding the resident), initiating diagnostic testing, and communicating with family members.17,18 As such, RNs play a key and immediate role in not only managing the day-to-day resident needs but also as a key carrier of clinical information between all stakeholders. Research points toward nurses experiencing additional sources of personal uncertainty in providing care, such as differing goals of care for prescribers compared with family members, interprofessional tensions in managing relationships with prescribers, and ethical dilemmas regarding palliative care.19–22 They report feeling anxiety in managing residents with subtle or subclinical infections and pressure from family members to prescribe antibiotics empirically. 23 As such, risk perceptions in the RACF environment appear to be shaped by a complex interplay of high uncertainty, resource constraints, and pressure from family members on RACF staff that have not been addressed by educational stewardship. 24
In RACFs, RNs and ENs are required to manage residents with complex presentations in conditions of high uncertainty and resource constraints and make decisions based on guidelines on whether to escalate risk to a prescriber. However, there is a paucity of data regarding how RNs manage uncertainty and make decisions based on knowledge, risk, and probability in RACFs. Qualitative studies indicate that uncertainty is framed as inherently aversive within the nursing literature. 21 Nurses report experiencing difficulties in recognizing or expressing uncertainties 23 and associate uncertainty in clinical practice with feelings of frustration, anger, agitation, and anxiety, regardless of years of experience. 21 During uncertainty, nurses feel responsible for client deterioration, experience guilt and remorse, 25 and feel scared of consequences of nursing interventions. 26 Reviews of the nursing literature highlight uncertainty in nursing to be experienced as either a lack of knowledge or lack of authority to practice independently despite having knowledge of procedures. 27 Nurses struggle to manage uncertainty and use strategies such as reliance on heuristics and attempting to anticipate resident care needs by being “one step head” or deferring to peers in attempts to reduce uncertainty.28,29
The cognitive-behavioral model of anxiety offers an explanation to understand the mechanisms by which uncertainty might trigger these aversive responses. It postulates that cognitions, emotions, and behaviors are causally related. 30 A stimulus is first appraised by identifying it as negative, positive, or neutral based on comparisons of the stimuli to information in memory. Attention is then redirected based on personal relevance. However, uncertainty reduces an individual’s ability to use past experiences to predict desired outcomes and may contribute to anxiety and influence perceptions of risk of future negative events.31–33 Contemporary models of medical decision making, such as the dual processing model, explain the role of anxiety in influencing medical decision making using 2 distinct but interrelated systems. 34 Type 1 or system 1 processes are described as intuitive, automatic, fast, and affect based, whereas type 2 or system 2 processes are defined as analytical, slow, verbal, and deliberative, supporting a logical and probabilistic analysis. 35 The dual processing model defines 4 major categories that influence the valence of system 1: 1) affect, 2) evolutionary hard-wired processes (responsible for automatic responses to potential danger), 3) overlearned processes from system 2 that have been relegated to system 1 (such as the use of heuristics), and 4) the effects of tacit learning/implicit learning. 36 Therefore, the ability of nurses to be able to perceive and tolerate a level of uncertainty and anxiety is of particular importance in understanding the mechanisms underlying clinical decisions in RACFs.
While uncertainty is described as being generally uncomfortable, the perceived intensity of discomfort ranges from immobilizing fear to a more covered-over, acceptable doubt. 37 “Uncertainty tolerance” (UT) refers to a person’s cognitive, emotional, and behavioral reactions to situations perceived as uncertain and is considered distinct from fear and anxiety.38,39 Emotion regulation theories posit that individuals usually enact cognitive and behavioral strategies (e.g., avoidance) to modulate their emotional responses, enhancing the intentional desire for control or escape from undesirable internal states.31,40 Individuals with low UT have been shown to find uncertainty threatening, perceive themselves as unable to cope with uncertainty,41,42,43 and experience emotional distress, particularly when uncertainty is explicit.27,43 In addition, individuals with lower UT appear to be less confident about high-risk decisions but also less likely to change their decisions despite receiving new information. 44 Although UT has traditionally been conceptualized as a stable personality trait, contemporary findings indicate that an individual’s specific situation and context play a significant role in influencing their UT.45,46 Therefore, the ability of nurses to be able to perceive and tolerate a level of uncertainty and anxiety is of particular importance in understanding the mechanisms underlying clinical decisions in RACFs.
In sum, RACF staff experience high levels of scientific, practical, and personal uncertainty and fear negative consequences (e.g., death of a resident, worsening of symptoms, aversive responses from prescriber and/or family members’ response, de-registration) when making decisions regarding escalating care (e.g., testing for urinary tract infections). Although aged-care staff are not directly responsible for prescribing antibiotics, it is likely that this anxiety influences risk perceptions when communicating with prescribers. GPs report pressure from staff and family members to prescribe; however, the mechanisms by which this happens are unclear and warrant further investigation.15,19 Therefore, the current study aims to examine whether nurses’ anxiety and clinical tolerance of uncertainty contributes to nursing behaviors that favor initiation of antibiotics (e.g., calling the GP to initiate antibiotics earlier) or immediate assessment of the resident. It is hypothesized that the relationship between uncertainty and decisions favoring antibiotic initiation are mediated by the experience of situational anxiety. As discussed above, stewardship in RACFs has traditionally targeted aged-care staff through educational interventions. 1 While these interventions appear to be useful in addressing scientific uncertainty (e.g., remediating knowledge gaps in differentiating and interpreting different signs and symptoms), these interventions alone do not address the high levels of practical and personal uncertainty that staff experience in these settings. 24 It is expected that understanding the relationship between nursing behaviors adjacent to prescribing might inform interventions that address some of the inappropriate prescribing that occurs in RACFs.
Method
Participants
Participants were recruited to an online survey using Qualtrics software through snowballing via e-mailing repeated invitations to participate in the survey using Ageing and Dementia Health Education and Research (ADHERe) Centre at the University of Wollongong from August 2021 to August 2022. ADHERe has a membership of 1,400 gerontological specialist nurses and allied health care practitioners working in clinical practice, education, research, and policy areas. The survey was also posted through nursing organizations (e.g., the New South Wales Nursing and Midwives Association; NSWNMA) and social media. Lastly, participants were also recruited through Farron Research, a third-party market research company. Participants recruited from social media and the community were eligible to enter a draw to win 1 of 5 $200 gift cards, while those recruited from Farron Research were remunerated $50 through the company that was paid by the Australian Centre for Health Engagement, Evidence and Values (ACHEEV) at the University of Wollongong. Two hundred thirty-seven participants initiated the survey; 80 respondents were excluded because of incomplete responses. A total of 157 participants completed the survey, with a 66% completion rate.
Design and Procedure
This was a cross-sectional, vignette-based study. A case-vignette approach was adopted in line with previous literature looking at uncertainty with clinicians.47,48 Although this approach has not been validated specifically with nurses, it has been used with emergency doctors and prescribers in veterans care units. Participants were asked to complete 9 demographic questions (e.g., age, sex, education, etc.) followed by the adapted version of Physicians Reactions to Uncertainty Scale for Nurses (PRUS-N), followed by a typical presentation of an upper respiratory tract infection in RACFs with a hypothetical resident named “Navneet.” The Immediate Assessment and Antibiotics (IAA) scale describes situations in which there is significant uncertainty (and therefore no clear-cut answer) where the pressure from a staff member adds another layer of information without a change in clinical data available to the participant that might trigger antibiotic prescribing. In the development of the vignettes, we consulted with senior nursing academics in an effort to make the vignettes relevant and ecologically valid. The situations described were designed to have some element of ambiguity (as in clinical practice) with the participant being asked if they would specifically urge the GP to prescribe earlier than what the GP has deemed appropriate after visiting the resident or by escalating the resident to emergency care and calling an ambulance. Participants were asked to rate the likelihood that they would take the step described in each option (1 = definitely not to 6 = definitely would) as the vignette progressed. Participants were also asked to rate their anxiety using the following item: “Navneet’s situation makes me anxious,” rated on a Likert-style scale in which responses ranged from 1 to 6 (1 = strongly disagree to 6 = strongly agree).
Measures
IAA scale
The IAA measure provides a vignette of a typical presentation of an upper respiratory tract infection in a resident in a RACF. Participants were then asked to rate the likelihood that they would take the step described in each option (1 = definitely not to 6 = definitely would) as the vignette details were elaborated across 3 blocks of information (see example below). The full scale comprised 16 items, and factor analysis indicated that there were 3 subscales (described elsewhere). The present study used the 4-item IAA scale. The measure demonstrated satisfactory internal consistency (Cronbach’s α = 0.75). The IAA measures nursing behaviors regarding the perceived need for antibiotics and assessment. All 4 items have been given below:
“You suggest to your supervisor that you need to contact the GP to start the antibiotics earlier.”
“Given Navneet’s presentation, you urge the GP to start antibiotics over the phone.”
“You ask your manager whether you should call an ambulance and get him assessed at casualty/emergency to assess him quicker.”
“You ask your manager whether you should call an ambulance to get Navneet assessed at casualty/emergency.”
Example block of information and item: The next day you are told by other carers that Navneet seems to be losing his appetite—and has not eaten more than half of his last 3 meals. Even though he has a persistent mild fever and his cough is more noticeable, his blood pressure, pulse rate, and oxygen saturation are normal—Navneet seems to be managing okay. Near the end of your shift on a Wednesday one of the nursing assistants involved in his care tells you he is worried that Navneet might be developing a lower respiratory tract infection and urges you to do something about it.
Given Navneet’s presentation, you urge the GP to start antibiotics over the phone.
You ask your manager whether you should call an ambulance to get Navneet assessed at casualty/emergency.
Situational anxiety
Participants were asked to rate their anxiety by agreement with the statement, “Navneet’s situation makes me anxious,” completed after each of the 3 blocks of information presented. Participants rated their agreement on this item on a Likert-style scale in which responses ranged from 1 to 6 (1 = strongly disagree to 6 = strongly agree). Cronbach’s alpha for the 3 items indicated good internal consistency (α = 0.89).
Tolerance of uncertainty
The tolerance of uncertainty in the clinical context was measured using an adapted version of the Physicians Reaction to Uncertainty Scale (PRUS). 49 The PRUS is a widely used scale to measure uncertainty and has been identified as an exemplary measure of uncertainty tolerance with healthcare samples. 45 The PRUS contains 22 items rated on a six-point Likert-type scale ranging where responses ranged from 1 to 6 from strongly disagree to strongly agree. There are two subscales: stress from uncertainty and reluctance to disclose uncertainty. The stress from uncertainty subscale (13 items) measures negative affective responses to uncertainty (e.g. “I find the uncertainty involved in patient care disconcerting”). The reluctance to disclose uncertainty subscale (nine items) measures fear of disclosing uncertainty to others (e.g. “The hardest thing to say to patients or families is ‘I don’t know’”). Scores are obtained by summing all items, with higher scores suggesting lower tolerance of uncertainty (i.e., higher intolerance of uncertainty). The PRUS was modified in consultation with P.D. and A.M. in the following ways:
The referent “physician” was replaced with “nurses” and “patient” was replaced with “client.”
The following 4 items were added: I worry about malpractice when I do not know how to perform a procedure (e.g., complex dressing, setting up intravenous therapy [IVT]); If I can’t answer the doctor’s questions, I worry they will lose confidence in me; I am frustrated when I do not know how to perform a procedure (e.g., complex dressing, setting up IVT); I usually feel anxious when I am not sure of a client’s procedure (e.g., complex dressing, setting up IVT).
Existing items were modified to the following: I almost never tell other nurses if I am unsure about how to undertake a procedure (e.g., complex dressing, setting up IVT); If I don’t have clear information for the doctor to make a diagnosis, I worry they will lose confidence in me; When I am unsure of how to perform a procedure, I imagine all sorts of bad scenarios (e.g., client dies, patient sues, etc.).
The modified version of PRUS for nurses (PRUS-N) demonstrated excellent internal consistency (α = 0.91) in the current sample. The subscales of the PRUS are highly correlated and represent related dimensions within a global concept 49 ; therefore, a total score was used in line with previous studies.47,50
Analysis
Statistical analyses were conducted using IBM Statistical Package for Social Sciences (SPSS v.28). An a priori power analysis was conducted using G*Power version 3.1.9.7 51 to determine an estimate of the minimum sample size required to test the study hypothesis. Results indicated the required sample size to achieve 95% power for detecting a small effect size (0.1), at a significant criterion of α = 0.05, was N = 132. The data were screened for missing values, normality, and univariate and multivariate outliers, and descriptive analysis was conducted. All tests were 2-tailed, and the alpha was set at 0.05. The PROCESS macro was used to test whether the relationship between clinical tolerance of uncertainty and antibiotic initiation was mediated by situational anxiety.52,53 Regression diagnostics indicated that all assumptions except the normality and homoscedasticity assumptions were met. This approach allows for nonnormality and asymmetry and balances power and validity concerns. 54 The bias-corrected bootstrap confidence intervals for each of the indirect effects were based on 5,000 bootstrap samples, using 95% confidence intervals. A heteroskedasticity–consistent standard error estimator—HC3—was used to reduce the effects of heteroscedasticity. 55 Sensitivity analysis was run using the 2 items pertaining to antibiotics and 2 items pertaining to assessment separately to confirm whether the findings would hold when each of these items was used as the dependent variable.
Ethical Considerations
The study was approved by the University of Wollongong and Illawarra and Shoalhaven Local Health District Health and Medical Human Research Ethics Committee (HREC: 2021/015). The authors have checked to make sure that our submission conforms as applicable to the journal’s statistical guidelines.
Results
Sample Characteristics
One hundred fifty-seven nurses took part in the survey. The total sample consisted of 111 female participants with an average age of 43 y (s = 14.5 y) and 46 male participants with an average age of 41 y (s = 10.8 y). Most participants worked in New South Wales (NSW; 46.5%), followed by Queensland (17.8%), Victoria (16.6%), Western Australia (7.6%), Australian Capital Territory (6.4%), South Australia (3.2%), and Tasmania (1.3%). One participant worked in New Zealand but had previously worked in NSW. Most participants (75.3%) had at least 3 y of experience, 16.6% of the participants had 1 to 2 y of experience, and 8.3% had less than 1 y of experience in the residential aged-care sector. Most participants worked in direct clinical care (52.9%), followed by management (16.66%), education (7%), and policy (1.3%). From the participants, 22.3% selected “other” and worked in a combination of management, education, and policy development. Of the participants, 41.4% had a bachelor’s degree, followed by 25.5% with a master’s degree, 17.2% with a graduate certificate, and 9.6% receiving hospital-based education. One participant had a PhD, 7 participants had a diploma, and 1 participant had a certificate IV.
Preliminary Analysis
The IAA scale consisted of 4 items. Two items were related to initiation of antibiotics, and 2 items were related to the immediate and urgent assessment (with the implication that antibiotics would be one of the treatment options). Items in the IAA scale ranged from 0 to 5. The average item score across the 4 IAA items was 2.81, which falls between “somewhat unlikely” (2) and “somewhat likely” (3). The mean for the 2 items that specifically mention antibiotic initiation was 5.96 and for immediate assessment items was 5.28. On average, RNs agreed that it was “somewhat likely” that they would urge the GP to start antibiotics either earlier or over the phone. Similarly, most RNs also agreed that it was “somewhat likely” that the resident needed to be assessed at emergency/casualty or through calling an ambulance.
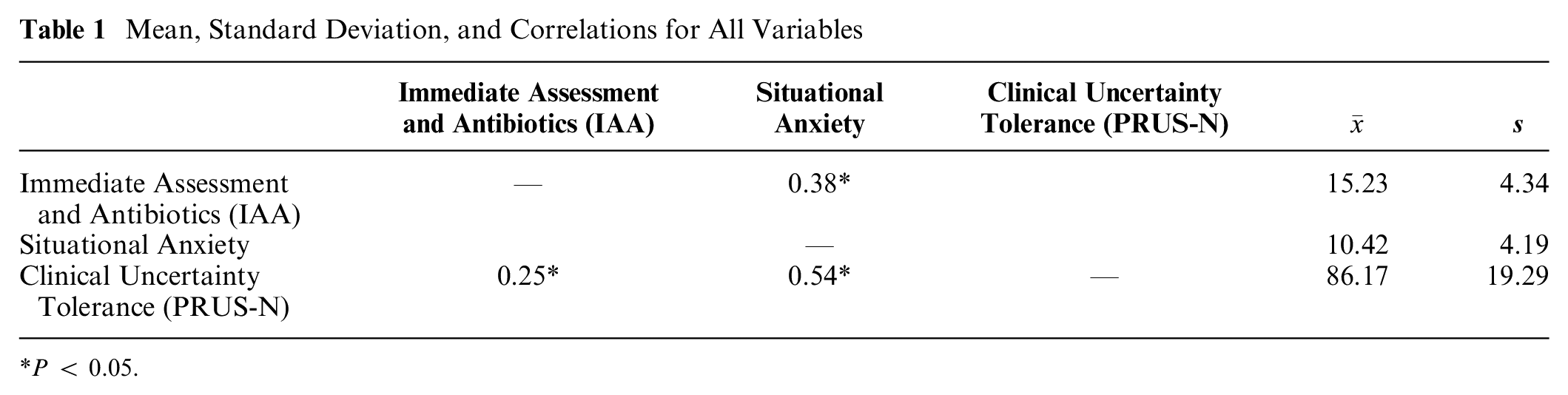
Table 1 shows the scale total means, standard deviations, and correlations for the 3 variables used in the mediation analysis. Based on Cohen’s criteria, 56 a moderate to strong positive relationship between situational anxiety and clinical tolerance of uncertainty (r = 0.54), moderate positive relationship between situational anxiety and immediate assessment and antibiotics scale (r = 0.38), and a small positive relationship between immediate assessment and antibiotics and clinical tolerance of uncertainty (r = 0.25) was evident.
Mean, Standard Deviation, and Correlations for All Variables
P < 0.05.
Mediation Analysis
A simple mediation analysis was conducted using PROCESS to assess if situational anxiety mediated the relationship between clinical tolerance of uncertainty and perceived need for antibiotics and assessment. The outcome variable for analysis was the IAA scores. The predictor variable for the analysis was the clinical tolerance of uncertainty using the PRUS-N scores (see Figure 1). The mediator variable evaluated for analysis was situational anxiety. Anxiety fully mediated nurses’ tolerance of uncertainty, explaining 6% of variance in the perceived need for immediate assessment and initiation of antibiotics for residents (see Table 2).
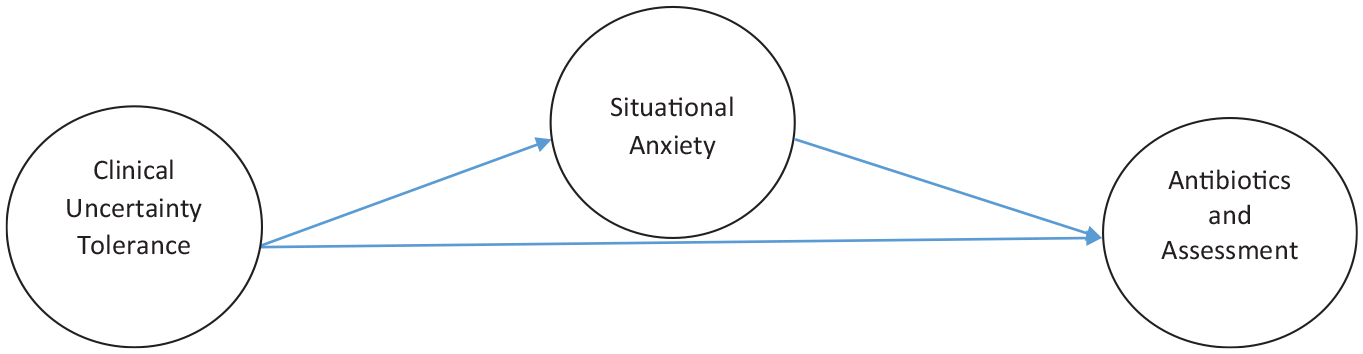
Mediation of clinical tolerance of uncertainty (X) to antibiotics and assessment (Y) by situational anxiety (M).
Mediation of Clinical Tolerance of Uncertainty (X) to Antibiotics and Assessment (Y) by Situational Anxiety (M)
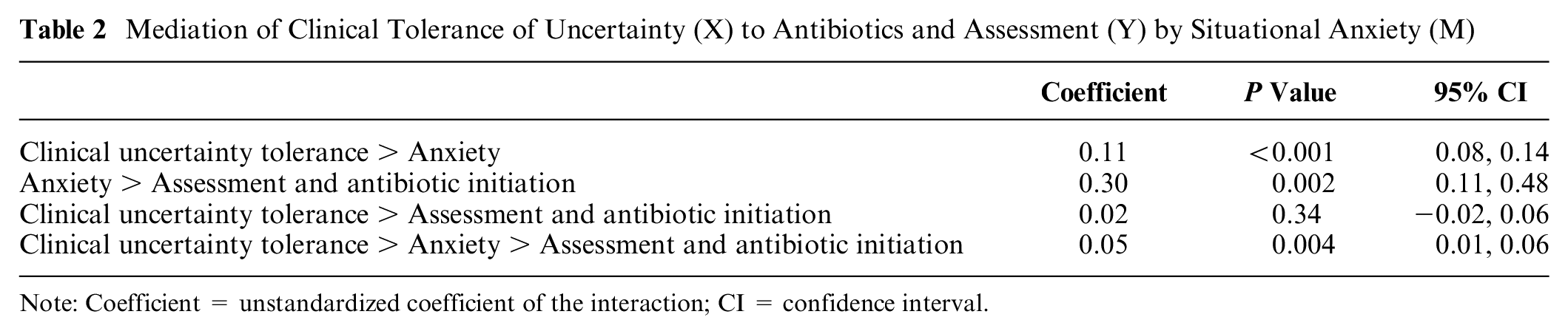
Note: Coefficient = unstandardized coefficient of the interaction; CI = confidence interval.
Post Hoc Sensitivity Analysis
Because the IAA is a new measure and 2 items specifically refer to initiation of antibiotics while the other 2 refer to immediate assessment, a sensitivity analysis was conducted by separating these item pairs. When only the 2 antibiotic initiation items were used, the mediation was not significant. When only the 2 immediate assessment items were used, the mediation remained significant. This suggests that lower tolerance of uncertainty is associated with greater anxiety in making decisions regarding resident deterioration, particularly regarding preferences for immediate assessment.
Discussion
The problem of overprescribing in RACFs is multifaceted, and a number of barriers have been identified, including high uncertainty, risk perceptions of staff, time constraints, and resident/patient and family preferences for antibiotics.14,19 A number of studies have reported that GPs experience pressure to prescribe antibiotics empirically and that antibiotics are used as a mechanism to ameliorate anxiety. 23 However, there is a gap in our understanding of how RACF staff might influence the initiation of antibiotics. Given that nurses play a key role in escalating care and relaying information between stakeholders, this study focused on their preferences regarding the need for initiation of antibiotics and need for immediate assessment by a medical professional in conditions of uncertainty and patient complexity. Findings provided support for the hypothesized model that predicted that situational anxiety mediates the relationship between clinical uncertainty tolerance and initiation of antibiotics and immediate assessment of residents. This study provides a first step toward exploring one of the potential mechanisms by which antibiotics might continue to be perceived as a means to mitigate risk in RACFs.
Most stewardship efforts in RACFs for nurses have focused on educational strategies, use of guidelines (e.g., use of McGeer criteria or local guidelines), introduction of care pathways, and use of infectious diseases teams to address overprescribing. 1 These interventions assume that inappropriate prescribing of antibiotics is driven by a lack of knowledge in individuals and that increasing awareness of antimicrobial resistance and knowledge about appropriate prescribing will to lead to behavior change. However, systematic reviews of antibiotic use and stewardship in RACFs suggest that staff report being aware of antimicrobial resistance as a problem, endorse guidelines and algorithms as diagnostic tools, and report high levels of confidence in their ability to determine changes in a resident’s clinical status due to an infection. 24 These findings suggest that factors other than a lack of education and awareness may drive some of the inappropriate antibiotic initiation in RACFs. Large variations in practices and the availability of resources across RACFs, a lack of engagement of nurses, and perceived pressure from family members further challenge the uptake and sustainability of educational interventions as a means of managing these tensions. 14
Findings from the current study validate previous literature regarding nurses’ experiences of anxiety, frustration, and agitation in the context of uncertainty.20,21,25,26 The experience of anxiety might be particularly salient in the affect-rich context of working within time constraints, increased workloads, reduced availability of prescribers and senior staff, and managing expectations from multiple stakeholders (e.g., family members) in RACFs. Nurses struggle to manage uncertainty and use strategies such as reliance on heuristics and attempting to anticipate resident care needs by being “one step ahead” or deferring to peers in attempts to reduce uncertainty.28,29 The cognitive behavioral model of anxiety explains the mechanisms by which individuals with lower UT might attempt to reduce uncertainty and manage their distress by deferring to colleagues or GPs and calling an ambulance. 35 For example, deferral to a GP or hospital in the absence of a multidisciplinary team in RACFs, particularly in the context of family pressure, is likely to produce a more immediate reduction in anxiety compared with more time-intensive strategies such as using databases to find evidence-based guidelines and research papers.15,19 Future studies might further begin to untangle what elements (e.g., family pressure) influence the relationship between anxiety, uncertainty, and prescribing intentions.
This study provides empirical support for the role of psychosocial factors beyond knowledge gaps to play a role in the immediate assessment and initiation of antibiotics in RACFs. However, there are several limitations that qualify its findings. First, the results from the sensitivity analysis suggest that the mediation is significant for the emergency department assessment items in the IAA scale but not those that explicitly recommend antibiotic initiation. Although our study relied on feedback from senior nursing academics regarding the suitability of nursing interventions, we did not compare decisions to algorithms or criteria (e.g., McGeer criteria) to test whether these interventions were concordant with guidelines. In addition, the lack of a control vignette in which the clinical situation is described without the colleagues’ input limits our ability to delineate whether variability in antibiotic initiation was driven by the clinical situation or input from colleagues. Finally, the IAA decision-making measure gets participants to endorse the extent to which they agree or disagree with a particular action. Thus, it cues participants toward particular decisions, and it is possible that there were other unique decisions that were not captured by the measure.
The current model predicts only 6% of variation, and there is a need to explore other factors. Contemporary models of decision making stipulate the role of emotions, such as regret in influencing reliance on affect-based system 1 processes.31–36 Nurses report experiencing feelings of anger and frustration during uncertainty 25 and find it difficult to manage prescribers’ and family members’ expectations. 15 It might be useful to explore how their past experiences with residents (e.g., deterioration or death), their families (e.g., attitudes toward nurses; attitudes toward death), and prescribers (e.g., anger, dismissal of concerns) might further influence decisions that have not been explored in this study. Lastly, the current study did not link antibiotic initiation with prescribing behaviors. Future studies could achieve this by administering the measure and then looking at some of the specific behaviors over the past week/month (i.e., timeline follow-back method) as a means to both link the prescribing and initiation and further validate the vignette used. Given that most of the participants in this study were experienced nurses with more than 3 y of work experience in RACF and that several studies 45 report conflicting findings of clinician experience on behaviors and tolerance of uncertainty, it might be useful to explore how nurses’ experience influences these decisions.
Despite these limitations, the current study has a number of implications to inform future stewardship in RACFs, mainly supporting the need for a multipronged approach to stewardship. The tolerance of uncertainty is understood as a multidimensional, partially mutable state that can be targeted through specific interventions.3,50 The inclusion of strategies that might be “response or relationship” focused (e.g., recognizing uncertainty through case vignettes, verbalizing and managing own reactions to uncertainty, discussions with team members and/or debriefings) is aimed at ameliorating aversive effects30–33 of uncertainty rather than curing uncertainty by deferral to GP/hospitalization. Furthermore, there is a need to engage cognitive and meta-cognitive (i.e., thinking about thinking/feeling) strategies for managing uncertainty. 35 The use of adaptive emotional regulation strategies, such as mindfulness, acceptance, and cognitive reappraisal, has been shown to be effective in targeting uncertainty tolerance in individuals. 40 In addition, given that nurses report experiencing stress and pressure to act driven by family members, 15 specific training in recognizing and differentiating own uncertainty from that communicated by family members and managing difficult conversations with residents and their family members might also be useful as part of future interventions. Stewardship interventions targeting uncertainty tolerance could be further strengthened by including other stakeholders (e.g., residents’ families and personal care assistants) and considering the inclusion of allied health (e.g., social workers, psychologists) within the care teams to help facilitate difficult conversations regarding managing care toward the end of life.
Conclusion
Our findings highlight a relationship between anxiety, clinical tolerance of uncertainty, and preferences for antibiotics and immediate assessment in RACFs. Thus, it may be that providing strategies for the management of anxiety related to uncertainty could nullify some processes contributing to inappropriate prescribing in aged-care settings. However, the implementation of these strategies requires effortful control of instinctive, more automatic reactions and engaging in more logical and deliberative ways of thinking. Given the time constraints in RACFs, it is unlikely that these stewardship strategies will be successful without a multipronged, systemic response that recognizes the impact of uncertainty on nurses and the need for investment in these skills over and above educational interventions alone.
Footnotes
Acknowledgements
The authors would like to acknowledge the New South Wales Nursing and Midwives Association (NSWNMA) in helping with the data collection that has made this study possible as well as the nurses who took time to participate, particularly during the COVID-19 pandemic.
Correction (April 2024):
Article updated to remove the Supplemental Material section.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by a PhD scholarship by the Australian Centre for Health Engagement, Evidence and Values (ACHEEV) at the University of Wollongong.
Ethics
The study was approved by The University of Wollongong and Illawarra and Shoalhaven Local Health District Health and Medical Human Research Ethics Committee (HREC: 2021/015). The authors have checked to make sure that our submission conforms as applicable to the journal’s statistical guidelines.