
Abstract
Background
Medical uncertainty is a pervasive and important problem, but the strategies physicians use to manage it have not been systematically described.
Objectives
To explore the uncertainty management strategies employed by physicians practicing in acute-care hospital settings and to organize these strategies within a conceptual taxonomy that can guide further efforts to understand and improve physicians’ tolerance of medical uncertainty.
Design
Qualitative study using individual in-depth interviews.
Participants
Convenience sample of 22 physicians and trainees (11 attending physicians, 7 residents [postgraduate years 1–3), 4 fourth-year medical students), working within 3 medical specialties (emergency medicine, internal medicine, internal medicine–pediatrics), at a single large US teaching hospital.
Measurements
Semistructured interviews explored participants’ strategies for managing medical uncertainty and temporal changes in their uncertainty tolerance. Inductive qualitative analysis of audio-recorded interview transcripts was conducted to identify and categorize key themes and to develop a coherent conceptual taxonomy of uncertainty management strategies.
Results
Participants identified various uncertainty management strategies that differed in their primary focus: 1) ignorance-focused, 2) uncertainty-focused, 3) response-focused, and 4) relationship-focused. Ignorance- and uncertainty-focused strategies were primarily curative (aimed at reducing uncertainty), while response- and relationship-focused strategies were primarily palliative (aimed at ameliorating aversive effects of uncertainty). Several participants described a temporal evolution in their tolerance of uncertainty, which coincided with the development of greater epistemic maturity, humility, flexibility, and openness.
Conclusions
Physicians and physician-trainees employ a variety of uncertainty management strategies focused on different goals, and their tolerance of uncertainty evolves with the development of several key capacities. More work is needed to understand and improve the management of medical uncertainty by physicians, and a conceptual taxonomy can provide a useful organizing framework for this work.
Uncertainty—the conscious, metacognitive awareness of ignorance—is a pervasive and important experience in medicine. 1 It arises in a wide variety of circumstances, affects both providers and recipients of health care, and has numerous, primarily aversive psychological effects, including thoughts and feelings of vulnerability and a propensity toward indecision and inaction.2–4 Physicians and other health care providers manage these effects and their experience of uncertainty itself through various strategies, but principal among these is the effort to seek information to reduce uncertainty.5–7 Nearly every major clinical activity that physicians undertake—diagnostic, prognostic, and therapeutic—is part of this overarching effort.
However, information seeking ultimately has limited effectiveness as a strategy for managing medical uncertainty. From a practical standpoint, this effort takes time; physicians and patients alike must always endure at least some period of waiting—for the patient’s course of illness to unfold, for the diagnostic workup to be completed, for the effects of treatment to become manifest—before medical uncertainty is reduced by added information. In the meantime, they must somehow deal with its aversive effects. From a theoretical standpoint, furthermore, many medical uncertainties are simply not reducible by information. No amount of empirical evidence, for example, can definitively answer the question of what the “right” treatment is for any individual patient. Not only is this ultimately a moral question that depends on the values and preferences of individuals, but scientific knowledge of all medical outcomes is confined to probability estimates that are inherently imprecise and incompletely applicable to individuals.3,8,9
The important task of managing medical uncertainty thus requires more than information seeking; however, there is surprisingly little empirical evidence on broader uncertainty management strategies used by physicians, other health care providers, or patients. In her seminal ethnographic studies of medical school training in the 1950s, sociologist Renée Fox documented how medical students employ various strategies to “manage their emotional reactions” to uncertainty, including “counterphobic, ironic, medical humor, laced through with impiety and self-mockery,” 10 and the adoption of a posture of “detached concern” toward patients.11,12 In the early 1980s, physician and legal scholar Jay Katz famously characterized physicians’ predominant management strategy as a “disregard of uncertainty”—a tendency to avoid acknowledging and disclosing uncertainty to patients. 13 The limited empirical research that has since been conducted, however, has focused almost exclusively on information-seeking strategies for managing medical uncertainty.14–22 With the exception of a recent study by Ilgen and colleagues,23,24 to our knowledge there have been no other attempts to systematically account for the broader range of strategies that physicians use.
This is an important research gap for several reasons. It limits our theoretical understanding of how uncertainty affects both physicians and patients, what uncertainty management strategies are more or less effective, and why. More importantly, it limits our practical ability to help physicians cope with the negative effects of uncertainty on their own well-being and the care they provide to patients. Further empirical research to identify and coherently classify the variety of physicians’ uncertainty management strategies is an important first step in overcoming these limitations.
To begin to address this need, we conducted a qualitative study to explore the views of a diverse sample of physicians and physician-trainees representing varying levels of professional experience and practicing in acute-care, high-stakes clinical settings (emergency medicine, inpatient general internal medicine) that generate a high degree of uncertainty about a wide range of issues. The overarching objective of our study was to provide a preliminary description of the strategies that physicians and physician-trainees use to manage the uncertainties they experience in their daily work and the ways in which their tolerance of these uncertainties evolves over time. The study’s ultimate goal was to begin to develop a coherent conceptual taxonomy of strategies for managing medical uncertainty, which might serve as a provisional foundation for future research.
Methods
Study Design, Participants, and Recruitment
The study employed in-depth individual qualitative interviews and was led by an experienced behavioral scientist and internal medicine/palliative medicine physician who has conducted conceptual and empirical research on medical uncertainty.1–3,8,9,25,26 The study team included other experienced behavioral scientists, clinician-researchers, and clinician-educators representing internal medicine, emergency medicine, nursing, and a range of professional interests including clinical reasoning and medical education. Most team members and study participants worked at the same institution, a large urban 637-bed teaching hospital. Participants consisted of a convenience sample of 1) attending physicians and postgraduate residents (postgraduate year [PGY] 1–3), representing 3 specialties that deal with a broad array of problems (emergency medicine, internal medicine, medicine-pediatrics) in inpatient settings (emergency department, hospital medicine service) and 2) fourth-year undergraduate medical students in their final 6 mo of medical school training. Recruitment was purposive and conducted by email invitation, in-person presentations at department meetings, and snowball sampling and aimed at achieving a mix of more senior and junior attending physicians (both greater and less than 10 y of practice experience), residents, and students. Participants were informed of the study’s topical focus on medical uncertainty. Recruitment aimed at data saturation but was ultimately driven by available resources and the overall goal of establishing an initial foundation for further research. The study was approved by the medical center Institutional Review Board.
Data Collection and Interview Content
From July 2018–April 2019, 22 individual interviews, lasting approximately 30 to 45 min, were conducted by telephone by 1 of 3 experienced qualitative researchers with no professional relationships with participants. Field notes were kept to track notable findings and the data collection process, and interviews were audio-recorded and transcribed verbatim by a professional transcription service. Interviews were semistructured and followed a moderator guide (Supplementary Appendix), developed by the entire multidisciplinary research team and consisting of open-ended questions and close-ended probes designed to elicit participants’ perceptions of 1) the extent and types of uncertainties they experience in clinical practice; 2) their psychological responses to these uncertainties, and any temporal changes in these responses; and 3) the strategies they use to manage medical uncertainties. During the course of the study, minor revisions were made in the interview guide to clarify and explore emergent themes in greater depth.
Data Analysis
Line-by-line software-assisted coding and in-depth qualitative analysis of anonymized interview transcripts were conducted using the program MaxQDA. The analysis used an inductive, constant comparative, grounded theory approach aimed at minimizing preconceptions, allowing key themes to emerge, and generating new theoretical understandings.27,28 Two researchers—the lead investigator and an experienced qualitative data analyst and doctoral-level medical anthropologist—first developed a working codebook by reading 10 transcripts, inductively identifying themes in participants’ verbatim statements (open coding), and then categorizing emergent themes according to their content (axial coding).27,29,30 The investigators met after coding each transcript to compare coding decisions, resolve areas of disagreement, and refine the codebook. The lead investigator and a second experienced master’s-level qualitative data analyst then applied the working codebook to analyze all remaining transcripts, comparing new data, concepts, and themes to those previously identified, highlighting potential interpretive biases, and achieving consensus by triangulating investigators’ differing perspectives. The investigators met regularly to compare, harmonize, and validate interpretations and coding decisions. Finally, the lead investigator conducted a secondary analysis of final codes and coded text to organize primary themes into higher-order conceptual categories according to logical relationships between them, triangulating these categories with theoretical constructs from the broader psychological literature to create an overall conceptual taxonomy that the entire research team reviewed and refined. Participant feedback on study findings was obtained from 5 extensively quoted members (23%) of the study sample.
Results
The study sample (Table 1) consisted of 22 participants: 11 attending physicians (practice experience 1–41 y), 7 resident physicians (PGY 1–3), and 4 medical students (MS-4). Participants described multiple uncertainties in their daily clinical work, which were primarily related to the diagnosis, prognosis, and treatment of their patients, and various primarily negative psychological responses to these uncertainties, including feelings of insecurity, fear, and anxiety. Participants described various strategies for managing these uncertainties, which we classified within 1 of 4 conceptual categories corresponding to their primary focus or target: 1) ignorance-focused, 2) uncertainty-focused, 3) response-focused, and 4) relationship-focused. This classification does not preclude multiple focus areas for any given uncertainty management strategy but simply assigns a logically primary focus to each. Several participants also described a temporal evolution in their management of uncertainty, which they attributed to the development of several key capacities: epistemic maturity, humility, flexibility, and openness.
Participant Characteristics a
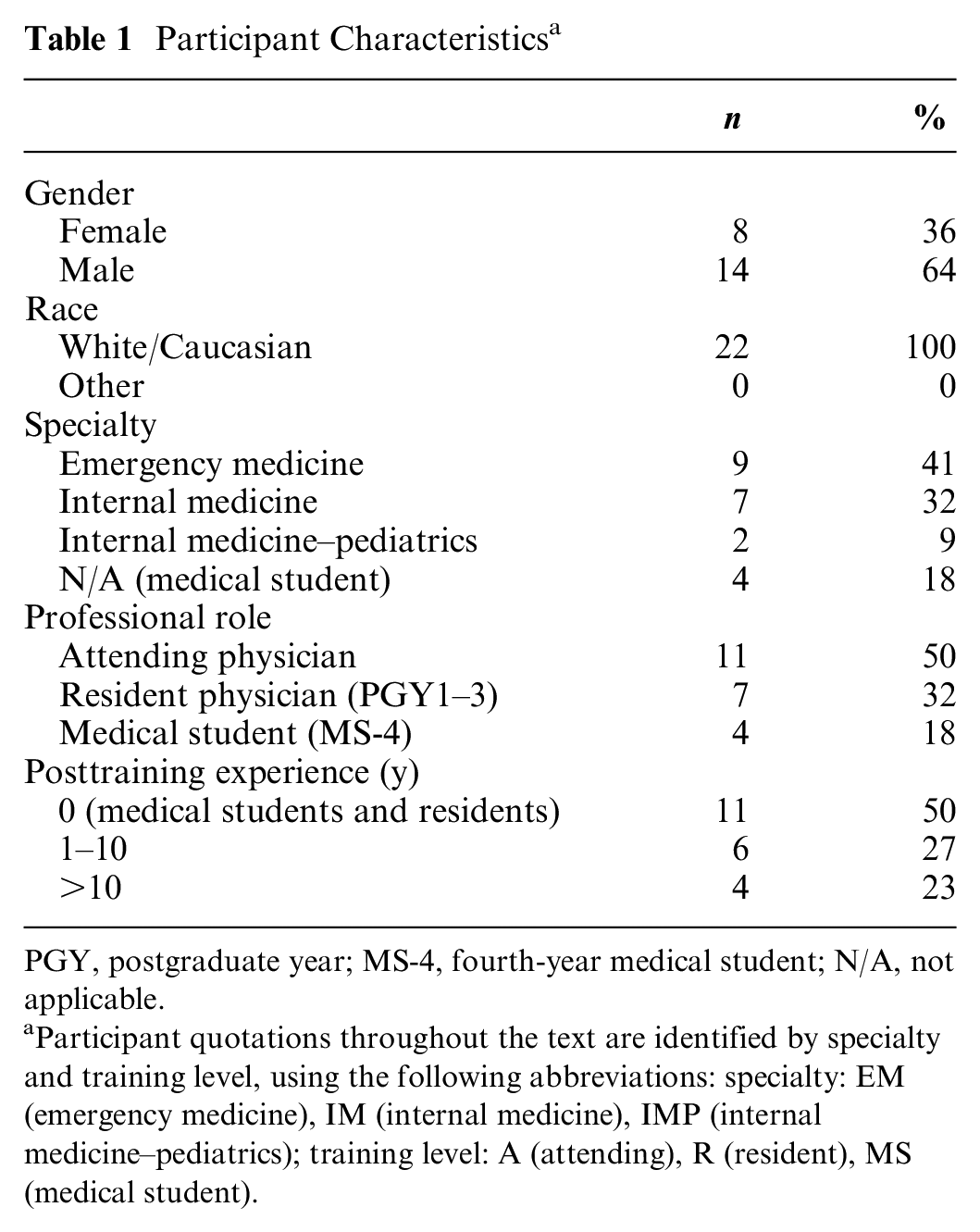
PGY, postgraduate year; MS-4, fourth-year medical student; N/A, not applicable.
Participant quotations throughout the text are identified by specialty and training level, using the following abbreviations: specialty: EM (emergency medicine), IM (internal medicine), IMP (internal medicine–pediatrics); training level: A (attending), R (resident), MS (medical student).
Ignorance-Focused Strategies
A major category of uncertainty management strategies is ignorance-focused, that is, directed at reducing or “curing” medical uncertainty by decreasing the ignorance that constitutes its object or root cause as a metacognitive state. These commonly cited strategies form the foundation of routine clinical care and encompass initiating diagnostic evaluation, instituting therapeutic trials, consulting with colleagues, and searching the medical literature. Illustrative quotes are presented in Table 2, and a conceptual taxonomy of strategies is presented in Figure 1.
Uncertainty Management Strategies a

Participant quotations identified by specialty and training level, using the following abbreviations: specialty: EM (emergency medicine), IM (internal medicine), IMP (internal medicine–pediatrics); training level: A (attending), R (resident), MS (medical student).
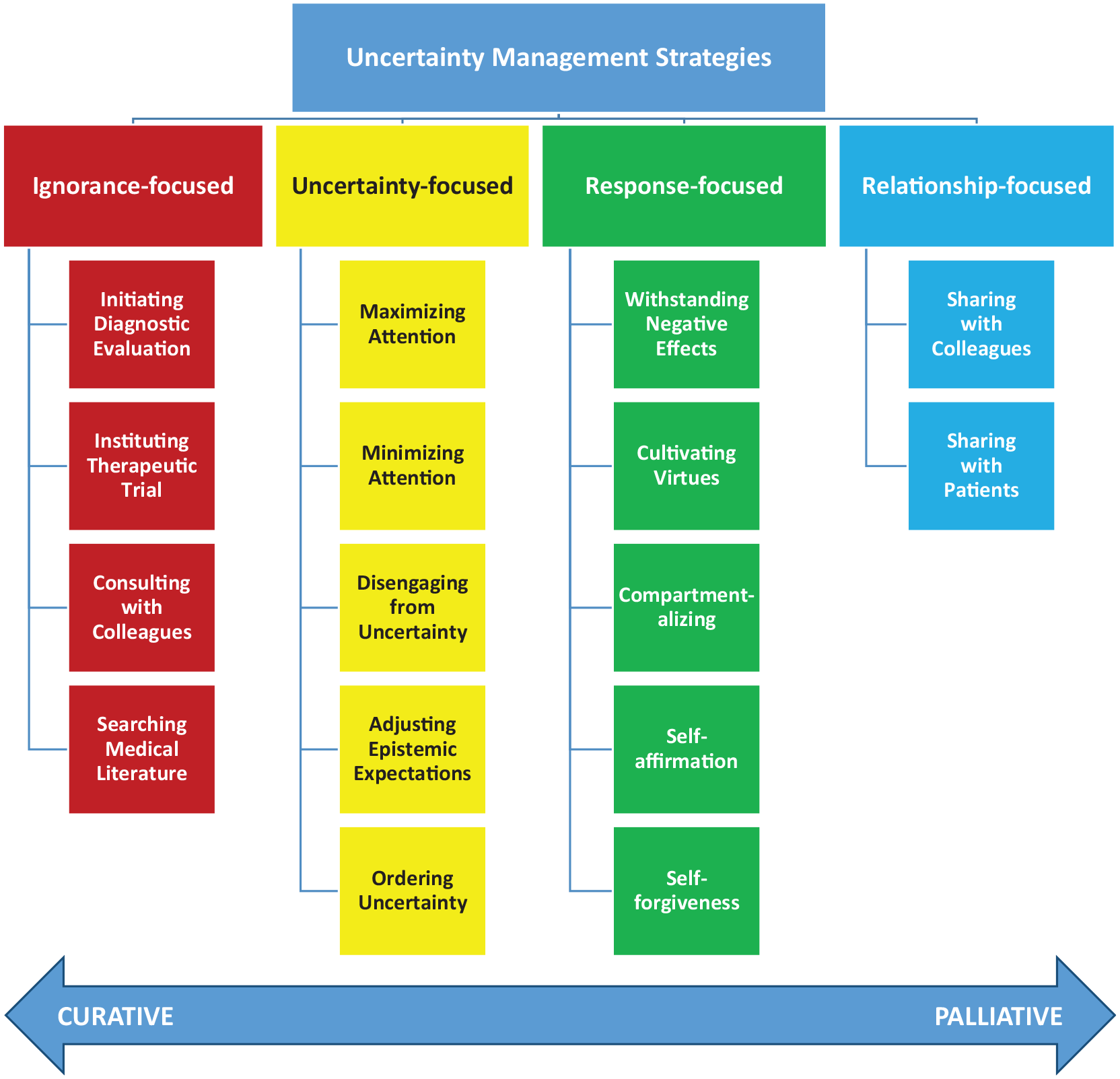
Physicians’ uncertainty management strategies: conceptual taxonomy.
Uncertainty-Focused Strategies
A second major category of uncertainty management strategies is uncertainty-focused, that is, directed not at the ignorance that represents the object of one’s uncertainty but at the higher-order, conscious awareness of this ignorance that is necessary for uncertainty to exist as a metacognitive state. 1
One commonly cited strategy, reinforced by the prevailing culture of medical practice and education, consisted of maximizing attention to one’s ignorance (e.g., by “double-checking” or maintaining a “high index of suspicion”), thereby maintaining one’s uncertainty. Participants noted, however, that this strategy promoted emotional distress and needed to be counterbalanced by efforts aimed at minimizing attention to one’s ignorance: ignoring one’s ignorance or restricting the scope of one’s awareness of it—thereby reducing or curing one’s uncertainty. A related strategy was disengaging from uncertainty: psychologically letting go by either emotionally distancing oneself from uncertainty or transferring the responsibility of dealing with it to others. Another important strategy was adjusting epistemic expectations: acknowledging the impossibility of perfect medical knowledge and thereby relinquishing the quest for certainty. A final uncertainty-focused strategy was ordering uncertainty: imposing some logical structure or process to make it more manageable. Examples included adopting a rational risk-benefit analytic framework or having an order of operations or clinical pathway to follow.
Response-Focused Strategies
A third major category of uncertainty management strategies is response-focused, that is, directed neither at ignorance nor one’s consciousness of it but at one’s own psychological responses to uncertainty. These differ from ignorance- and uncertainty-focused strategies in attempting not to reduce or “cure” uncertainty but to mitigate or palliate its aversive psychological effects.
A primary response-focused strategy identified by several participants consisted of withstanding negative effects: somehow resisting or stoically enduring the “feeling of angst,” as one EM attending physician described it, incited by uncertainty (EM-A-18). Another frequently cited response-focused strategy was cultivating virtues: enacting moral values such as industriousness, thoroughness, or due diligence in patient care as guiding ideals or surrogate goals that could be achieved despite the incurability of uncertainty. Compartmentalizing psychological responses—uncoupling and sequestering cognitive, emotional, or behavioral responses to uncertainty order to limit their deleterious effects—was another frequently cited coping strategy. Another important strategy was self-affirmation: an acknowledgment of one’s own core strengths or positively valued attributes that transcend one’s limitations. Self-forgiveness was a final related strategy that involved not only absolving oneself from guilt and blame but caring less about the negative evaluation of other people—both clinicians and patients.
Relationship-Focused Strategies
A fourth major category of uncertainty management strategies is relationship-focused, that is, directed not at ignorance, uncertainty, or psychological responses to uncertainty but at social relationships between physicians, other health professionals, and patients. These differ from ignorance-focused information-seeking strategies in relating with other persons not as a means of curing uncertainty but of palliating its aversive psychological effects.
Sharing with colleagues was the most commonly cited relationship-focused strategy, which helped physicians and trainees to cope with uncertainty by fostering mutual feelings of trust, support, and self-worth and preventing feelings of isolation. As one IM resident put it, “You don’t want to just be like an island and by yourself” (IM-R-14). Sharing with patients—giving them “a little bit of investment in the decision-making process,” as one EM attending physician put it (EM-A-13)—was another strategy that multiple participants valued as a means of lightening the emotional burden of uncertainty.31,32
Evolution of Uncertainty Tolerance
An important cross-cutting theme that emerged throughout all interviews was a temporal change in physicians’ responses to medical uncertainty. Participants at all levels of experience described how their own set of negative and positive psychological responses—that is, their “uncertainty tolerance”2,26—evolved over time and how this process involved the acquisition of various key capacities (Table 3).
Key Capacities in the Evolution of Physicians’ Uncertainty Tolerance a
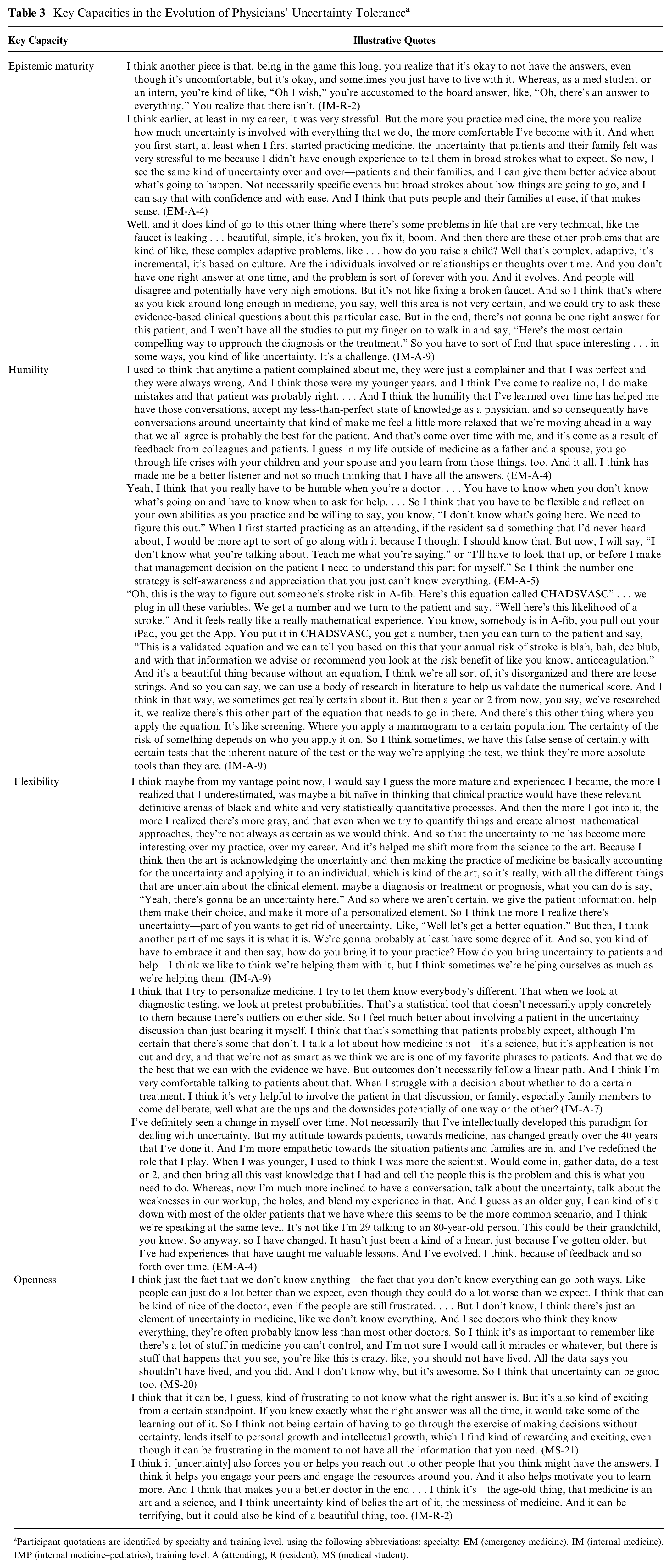
Participant quotations are identified by specialty and training level, using the following abbreviations: specialty: EM (emergency medicine), IM (internal medicine), IMP (internal medicine–pediatrics); training level: A (attending), R (resident), MS (medical student).
The first consisted of what educational psychologists have called epistemic maturity: a developmental state characterized by beliefs about knowledge that affirm its fundamentally limited nature and the need for caution and flexibility in evaluating truth claims.33–39 Epistemic maturity develops over time with learning and experience and involves a shift—reported in other studies of medical trainees 40 —from a naïve view of knowledge as dualistic (right v. wrong), absolute, and definitive to a more mature view of knowledge as pluralistic, relative, and provisional.34,36,41–43
Humility was a second key capacity in the evolution of the physicians’ uncertainty tolerance. The most experienced physicians related that clinical experience paradoxically made them both more confident and more humble about the limits of medical knowledge and open to the unknown. This humility, in turn, was tied to other changes, including greater willingness to seek help and to communicate openly with colleagues and patients, skepticism about medical truth claims, and emotional tolerance of uncertainty.
Flexibility was a third key capacity in the evolution of physicians’ uncertainty tolerance. Physicians also affirmed how uncertainty permitted them to approach their work in a more adaptive, creative manner aimed at understanding the uniqueness of individual patients and personalizing medical care without any definitive answers on how to do so. Physicians saw the adoption of this approach as freeing them up to “shift more from the science to the art” of medicine—from its technical to its humanistic aspects (IM-A-9)—and entailing greater empathy “towards the situation patient and families are in” (EM-A-4).
A final key capacity in the evolution of uncertainty tolerance was openness toward medical uncertainty, what Fox characterized as an “affirmative attitude” toward uncertainty, 10 which enabled physicians to acknowledge not only its negative but also its positive aspects and to view uncertainty not only as a threat but an opportunity. One manifestation of this capacity was an affirmation of the possibility of positive outcomes, for example, an ability to acknowledge that “people can just do a lot better than we expect” (MS-20), and to see uncertainty as an opportunity for both “personal growth and intellectual growth” (MS-21) and meaningful engagements with colleagues and patients.
Discussion
This qualitative study explored the uncertainty management strategies of physicians caring for general medical patients in acute-care hospital settings. To our knowledge, this is the first study to attempt to systematically describe these strategies among a diverse, multispecialty sample of physicians with varying levels of training and experience. Ilgen et al. recently conducted a qualitative study of 12 emergency medicine faculty physicians, which identified several activities and processes they use to judge and manage their comfort and discomfort with uncertainty.23,24 The current study extends that work by identifying additional previously undescribed strategies, classifying these strategies according to their psychological targets, organizing them within a conceptual taxonomy, and identifying key individual capacities that appear to be associated with the evolution of uncertainty tolerance. We believe the current study thus provides useful data to guide future efforts to understand and improve the management of medical uncertainty by physicians.
The study’s main finding was the wide variety of uncertainty management strategies that physicians and physician-trainees employ in their daily work. Importantly, these strategies focus on much more than medical ignorance and its reduction through information seeking, the overriding focus of medical practice and education. They center on various other phenomena, including uncertainty itself, psychological responses to uncertainty, and social relationships, that together constitute the experience of medical uncertainty and also on different goals. Both ignorance- and uncertainty-focused strategies focus primarily on “curing” (i.e., rejecting or eliminating) uncertainty, by reducing either medical ignorance or one’s conscious awareness of it. Response- and relationship-focused strategies focus primarily on “palliating” (i.e., accepting and ameliorating) uncertainty, either by altering one’s psychological responses to it or sharing the experience of uncertainty with others. Uncertainty management strategies, in other words, are not all created equal, and the taxonomy clarifies how they differ in their substance, functions, and ultimate goals.
This new taxonomy further reveals how managing uncertainty in medicine requires engaging in multiple, often conflicting strategies at the same time. Although the default strategy of medicine is to strive to cure uncertainty, both the practical and theoretical limits to medical knowledge and the cognitive burden and deleterious psychological effects of uncertainty require physicians to balance efforts to cure uncertainty with equal efforts to palliate it. Every physician must achieve some adaptive equilibrium between resisting and engaging with one’s uncertainty and accepting and disengaging from it, between pursuing knowledge and abandoning the pursuit, between eliminating the problem and mitigating its sequelae. The taxonomy catalogues the range of strategies that serve these essential functions and promotes an understanding of uncertainty management as a dynamic metacognitive process of self-regulation, by which individuals exert control over themselves and their environment by monitoring and adaptively changing their own responses or inner states.25,44 The importance of such an adaptive process has also been highlighted by “situativity” theories, which locate human knowledge, thinking, and learning in the continuous, dynamic interactions of individuals with their physical, cultural, and social environments. These theories emphasize how these interactions not only give rise to mental states such as uncertainty but also provide ways for individuals to regulate these states.45,46
The taxonomy can thus assist efforts to understand and improve the management of medical uncertainty. It can help researchers to more systematically measure the effects of different uncertainty management strategies and to develop new theoretical understandings of uncertainty management as a broader psychological process. The taxonomy’s categories are simply heuristic abstractions that may apply to multiple strategies; however, they enable these strategies to be disentangled and better understood. Many of the strategies identified in the taxonomy map onto discrete, well-described constructs in the broader psychological literature (e.g., coping, 47 categorization, 48 resilience,49,50 self-affirmation 51 ). The taxonomy can enable researchers to bridge these insights to develop a richer, more integrative, evidence-based understanding of uncertainty management, with broader applicability beyond medicine and physicians. It could also guide research on the effects of different uncertainty management strategies on not only patient-centered but also physician-centered outcomes, including well-being and burnout.26,52–54 At the same time, the taxonomy might also enable clinicians and educators to manage uncertainty in a more intentional, systematic, and rational manner. Applied as a tool for clinical practice or training, it could help physicians take inventory of alternative management strategies and select the most appropriate strategy based on various factors, for example, the particular diagnosis (i.e., source and issue) of the uncertainty at hand as well as its prognosis (i.e., reducibility). 1 It could help make the process of uncertainty management more active, intentional, and deliberative rather than passive, organic, and driven primarily by the “hidden curriculum” of medical care and training.
Yet the taxonomy is purely descriptive; it offers no definitive answers to the normative question of how physicians ought to manage different uncertainties. Our study, however, offers preliminary insights on this question. In reflecting on the evolution of their own uncertainty tolerance, participants identified epistemic maturity, humility, flexibility, and openness as acquired capacities that helped them to tolerate uncertainty—that is, to palliate its negative effects and realize its positive ones. These capacities may thus represent key components of uncertainty tolerance and instrumental goals in managing medical uncertainty (Figure 2); however, more research is needed to determine whether they can be intentionally cultivated52,55 and to identify other important normative goals.
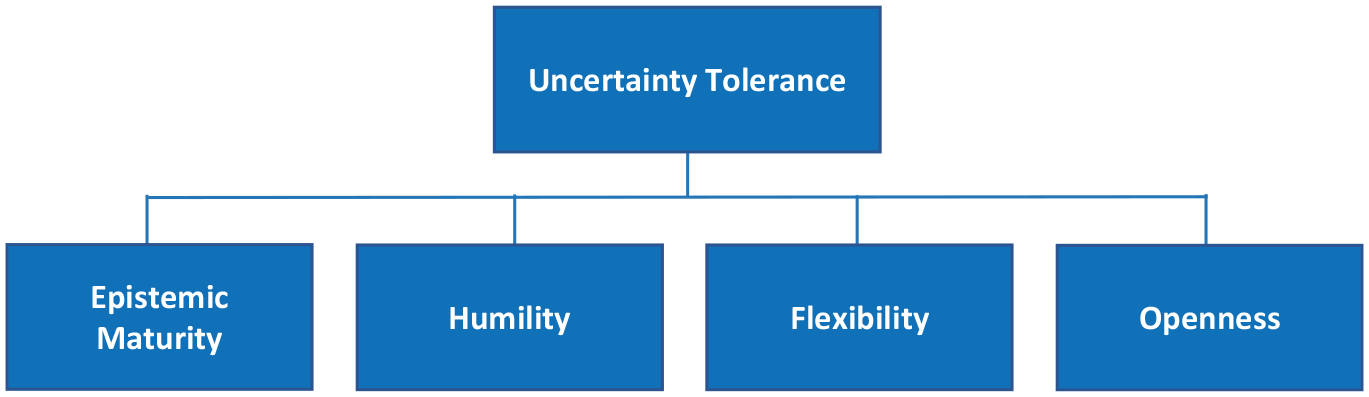
Normative goals of uncertainty management: key capacities.
This study had several limitations that qualify its findings. It used a relatively small convenience sample of racially homogeneous physicians practicing in general medical specialties and acute-care settings at a single hospital. These factors may have privileged some types of uncertainties (e.g., diagnostic, therapeutic) or management strategies over others and may have favored the selection of participants who were more tolerant of uncertainty or otherwise willing to talk about it. Furthermore, although the frequent recurrence of particular themes across the interviews suggested a high degree of thematic saturation, recruitment was ultimately limited by study resources; important uncertainty management strategies thus could have been missed. Multiple factors including physician specialty, practice setting, or uncertainty tolerance may produce variation in their uncertainty management strategies2,26; larger studies of more diverse physician samples are needed to fully capture this variation and confirm the transferability of our findings. Finally, qualitative interviews allow physicians themselves to describe the uncertainty management strategies they use but preclude the assessment of unconscious strategies; a more complete assessment requires direct observation of their actual behaviors.
For all of these reasons, our study simply provides an orienting framework for further research; however, this is also its greatest value. To begin to understand how physicians undertake the critical, consequential task of managing medical uncertainty, we need some way of imposing useful order on the problem. Our conceptual taxonomy and the prototypical uncertainty management strategies it identifies provide a provisional starting point. It remains for future research to identify additional strategies, to build on and refine the taxonomy, and to demonstrate its usefulness in efforts to understand and improve the management of medical uncertainty.
Supplemental Material
sj-docx-1-mdm-10.1177_0272989X21992340 – Supplemental material for How Physicians Manage Medical Uncertainty: A Qualitative Study and Conceptual Taxonomy
Supplemental material, sj-docx-1-mdm-10.1177_0272989X21992340 for How Physicians Manage Medical Uncertainty: A Qualitative Study and Conceptual Taxonomy by Paul K. J. Han, Tania D. Strout, Caitlin Gutheil, Carl Germann, Brian King, Eirik Ofstad, Pål Gulbrandsen and Robert Trowbridge in Medical Decision Making
Footnotes
Acknowledgements
We thank the physicians and trainees who generously donated their time and insights to participate in this study and Michael Kohut, PhD, and Hayley Mandeville, MPH, for assistance in the interviews and initial qualitative analysis. Portions of this study were presented at the 2019 International Conference on Communication in Healthcare, San Diego, California.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided by institutional research funds from Maine Medical Center. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report. The following authors are employed by the sponsor: Han, Strout, Gutheil, Germann, King, Trowbridge.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.