
Abstract
Background
How health workers frame their communication about vaccines’ probability of adverse side effects could play an important role in people’s intentions to be vaccinated (e.g., positive frame: side effects are unlikely v. negative frame: there is a chance of side effects). Based on the pragmatic account of framing as implicit advice, we expected that participants would report greater vaccination intentions when a trustworthy physician framed the risks positively (v. negatively), but we expected this effect would be reduced or reversed when the physician was untrustworthy.
Design
In 4 online experiments (n = 191, snowball sampling and n = 453, 451, and 464 UK residents via Prolific; Mage≈ 34 y, 70% women, 84% White British), we manipulated the trustworthiness of a physician and how they framed the risk of adverse side effects in a scenario (i.e., a chance v. unlikely adverse side effects). Participants reported their vaccination intention, their level of distrust in health care systems, and COVID-19 conspiracy beliefs.
Results
Physicians who were trustworthy (v. untrustworthy) consistently led to an increase in vaccination intention, but the way they described adverse side effects mattered too. A positive framing of the risks given by a trustworthy physician consistently led to increased vaccination intention relative to a negative framing, but framing had no effect or the opposite effect when given by an untrustworthy physician. The exception to this trend occurred in unvaccinated individuals in experiment 3, following serious concerns about one of the COVID vaccines. In that study, unvaccinated participants responded more favorably to the negative framing of the trustworthy physician.
Conclusions
Trusted sources should use positive framing to foster vaccination acceptance. However, in a situation of heightened fears, a negative framing—attracting more attention to the risks—might be more effective.
Highlights
How health workers frame their communication about a vaccine’s probability of adverse side effects plays an important role in people’s intentions to be vaccinated.
In 4 experiments, we manipulated the trustworthiness of a physician and how the physician framed the risk of adverse side effects of a COVID vaccine.
Positive framing given by a trustworthy physician promoted vaccination intention but had null effect or did backfire when given by an untrustworthy physician.
The effect occurred over and above participants’ attitude toward the health care system, risk perceptions, and beliefs in COVID misinformation.
Vaccinations have been crucial in improving global health. In particular, the COVID-19 vaccines currently represent the best long-term solution to reduce the heavy toll of the COVID-19 pandemic. However, vaccines often invite controversy and false information, 1 which might make people fearful of adverse side effects, undermine trust, and reduce intentions to be vaccinated. 2 For example, the COVID vaccine was deemed to be a tool to control the masses and a plot to reduce women’s fertility. 3 Honest communication about side effects is necessary to foster trust and support informed decision making, which together lead to positive health outcomes. 4 However, how to do this is not straightforward, especially given the ambient distrust surrounding vaccines. How can we adapt the communication about the risk of adverse side effects to ensure a good uptake without appearing manipulative? In this article, we study how trust in the information provider moderates the effect of framing of adverse side effect risks on vaccination intention.
The way information is presented, or “framed,” affects people’s perceptions and their health decisions.5–11 Past research has typically focused on framing preventative health messages in terms of goals (i.e., “gain v. loss” framing; e.g., the benefits one receives v. the losses one avoids by getting vaccinated 12 ), finding that the effects type of people’s decision making can vary and are context specific.13,14 In this article, we focus on yet a different type of framing research, in which the exact same piece of information framed either positively or negatively (i.e., “equivalence framing” i ) changes people’s decisions (see Krishnamurthy et al. 5 and Levin et al. 15 for more details on framing taxonomy). For example, people reported higher intentions to get a flu vaccine when told it was effective in 70% to 90% of cases compared to when told it was not effective in 10% to 30% of cases 6 and where the risk of adverse side effects was described as not occurring in 79,999 in every 80,0000 cases versus as occurring in 1 of every 80,000 cases. 11 Participants also judged positively framed statements about vaccine risks more plausible, they were more willing to share those and had a more positive attitude toward vaccines than participants who read negatively framed statements. 16 Equivalence framing can use percentages and complementary outcomes as above or be more subtle by focusing on the same outcome but using positive or negative verbal probabilities (e.g., “a chance” v. “unlikely”). Verbal probability framing is especially interesting because health professionals use words more often than numbers to communicate risks to their patients.17,18 This preference is reinforced by regulations by the European Commission, which advises drug manufacturers to use verbal labels in their leaflets along with numerical ones. 19 Although subtle, the verbal framing effect is quite influential. For example, most of the participants who read that a treatment had “a possibility” of being effective endorsed the treatment, whereas only a minority did so when they read an equivalent but negatively framed statement describing the treatment as “not certain” to be effective. 20
Trust in health practitioners is well known to increase patients’ adherence to their doctor’s advice 21 and promote vaccination intention.22,23 Yet, its role within the framing effect is not clear. The 2 main theoretical accounts of the framing effects have different expectation about the role of trust in the effect. Based on the “valence as bias” account, which explains the effect as merely valence induced,9,24,25 we could expect trust not to affect the framing effect. According to this account, the valence of a sentence varies on a positive-negative continuum that automatically triggers an emotion in recipients, which in turn shapes their preference. The valence of a positively framed statement induces automatically a positive emotion that colors participants’ perception of that option positively, whereas the valence of negatively framed statements would automatically elicit a negative emotion that would negatively distort their perception of that option. 9 As a result, people should be more willing to accept a vaccine if the side effects are “unlikely” (positive framing) than if there is “a small possibility” of them occurring (negative framing), whoever the speaker is. In contrast, according to a pragmatic account, the trustworthiness of the speaker should moderate the framing effect. According to this account, the framing effect occurs through a more reflective route, in which the frames implicitly convey an advice to the recipient.8,26,27 Statements have different layers of meaning: a semantic meaning (of what is explicitly said) and a pragmatic meaning (of what is implied but not explicitly said). The pragmatic meaning of a statement often has a perlocutionary function (to follow the Speech Acts terminology of Austin 28 ), which means that it intends to shape the recipients’ behavior. The pragmatic message of a speaker using a positive framing is to advise the recipient to select that option, whereas the pragmatic message of a speaker using a negative framing is more of a warning against that option. 20 Whether a recipient will take this advice relies on the assumption that linguistic exchanges follow a wider social contract: communication partners are direct, honest, and cooperative. 29 It is well recognized in the advice-taking literature: If one does not trust their advisor, they are less likely to follow their advice.30,31 Hence, according to the pragmatic approach, trust will moderate the framing effect, since framing given by untrustworthy sources is expected to be less potent. A study testing both the effect of valence and perceived advice based on different framing (e.g., 20% of your calories intake v. 20% of your energy intake) found supporting evidence for both the framing as bias and the framing as advice accounts, suggesting that valence and implicit advice might work in tandem. 27 However, the role of the trustworthiness of the source may disentangle which aspect of framing is most instrumental in decision making. For the “framing as bias” account, trust is not an essential ingredient for the effect, whereas for the “framing as advice” pragmatic account, trust is necessary.
Evidence converges to support that trust might indeed moderate the framing effect. For example, while a credible source denying that vaccine risks exist (e.g., “there are absolutely no risks”) led to lower risk perceptions than a statement acknowledging some risks (e.g., “the risks are very low”), the effect backfired when the source was not credible. 4 Evidence also shows that trust influenced how participants perceived 2 mathematically equivalent pieces of information. When 2 individuals described a product they sold using different—but equivalent—numerical frames (e.g., 70% lean v. 30% fat), participants preferred to buy the product described with a positive frame than the one described with a negative frame; however, this was less the case when the individuals describing their product were not trustworthy. 8 In line with a pragmatic account, the framing effect was weaker when speakers were untrustworthy than when they were trustworthy, but supporting the framing as bias, the framing effect still occurred nevertheless.
The possibility that trust moderates the framing effect is especially plausible in a medical context, where trust is potent in patients’ decisions because of their lack of knowledge.21,32,33 While, on average, in the United Kingdom, people tend to trust their family physician and the health care system in general, 34 people’s levels of trust vary to a great extent, 21 creating the possibility that the effects of real-life health messages would vary as well. And, indeed, framing information regarding vaccines has not always had the expected effect.35,36
Overview
In 4 experiments, we manipulated risk framing and the trustworthiness of the source to test how trust might moderate the framing effect on vaccination intention. Our first experiment took place at the onset of the vaccination program in the United Kingdom (December 21–January 22) and the last one when about half of the UK residents were vaccinated (May 2021; see Figure 1). We expected that a trustworthy family physician, framing positively the risk of adverse side effects would increase vaccination intention compared with the same physician framing the risk negatively. However, we expected that the positive framing might backfire or have no effect when given by an untrustworthy family physician. Across studies, we controlled for participants’ initial levels of distrust toward the health care system and beliefs in common COVID-19 misinformation.
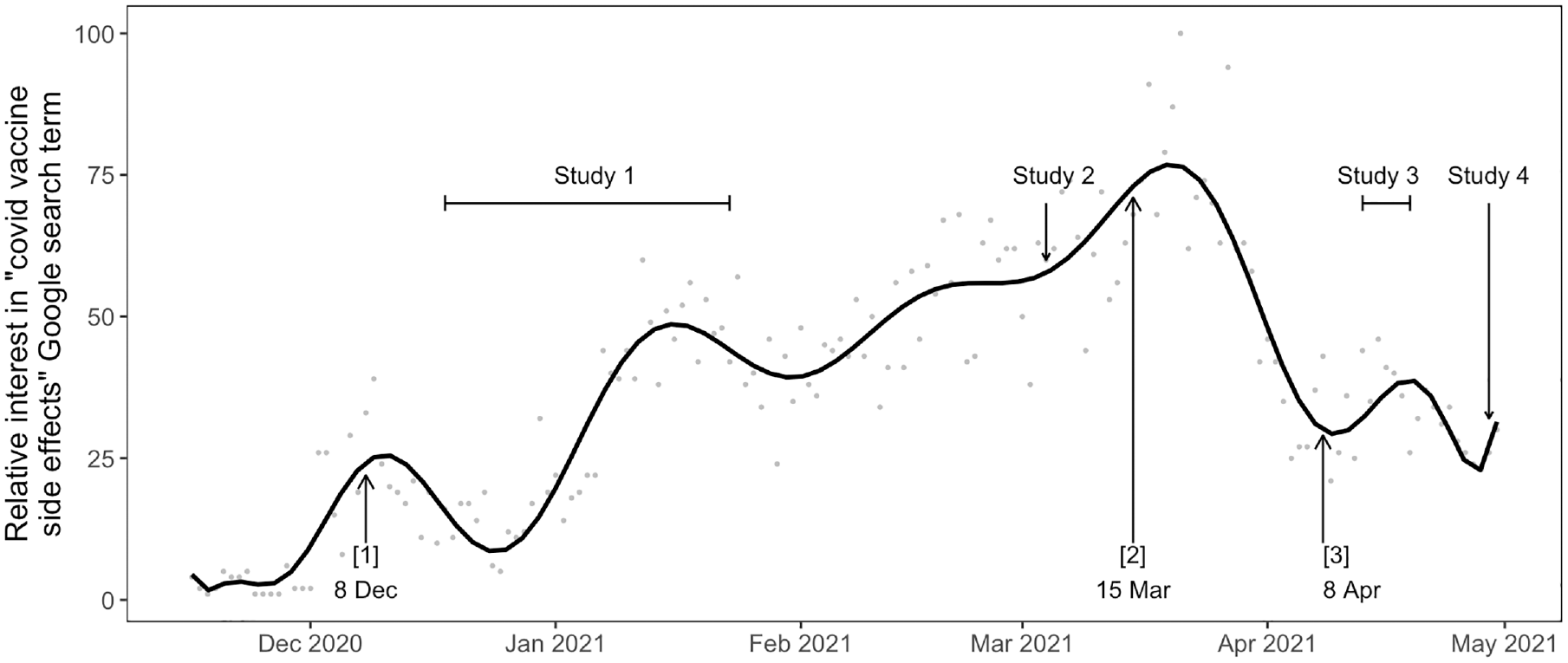
Evolution of the concerns about “COVID-19 vaccine side effects” in the United Kingdom based on the frequency of Google search for the words “COVID-19 vaccine side effects” and timeline of the 4 experiments presented here.
Experiment 1
Method
Open science statement
The data and materials for all the experiments are available on the Open Science Framework (OSF): https://bit.ly/3lGHyNU. 38 For experiments 2 to 4, the preregistrations are also available.
Participants
Participants completed the study in December 2020 and January 2021, at the onset of the UK vaccination program, after the vaccinations had started and were being rolled out to all the over-80s and some health care workers. For this study, we aimed to gather data from at least 200 participants within a 36-d period through snowball sampling and via the university psychology student pool (in exchange for course credits). We recruited 231 participants, of whom 199 fully completed all of the experimental part. We excluded 8 cases in which the completion time was less than 2.5 min, resulting in an analytical sample of 191 participants. According to a sensitivity analysis, this gave 95% statistical power to detect a medium-size effect of f = 0.26 (η2p = 0.06) in a variance analysis including main and interaction effects (α = 5%). The characteristics of the sample are shown in Table 1.
Characteristics of the Participants in Experiments 1 to 4 a
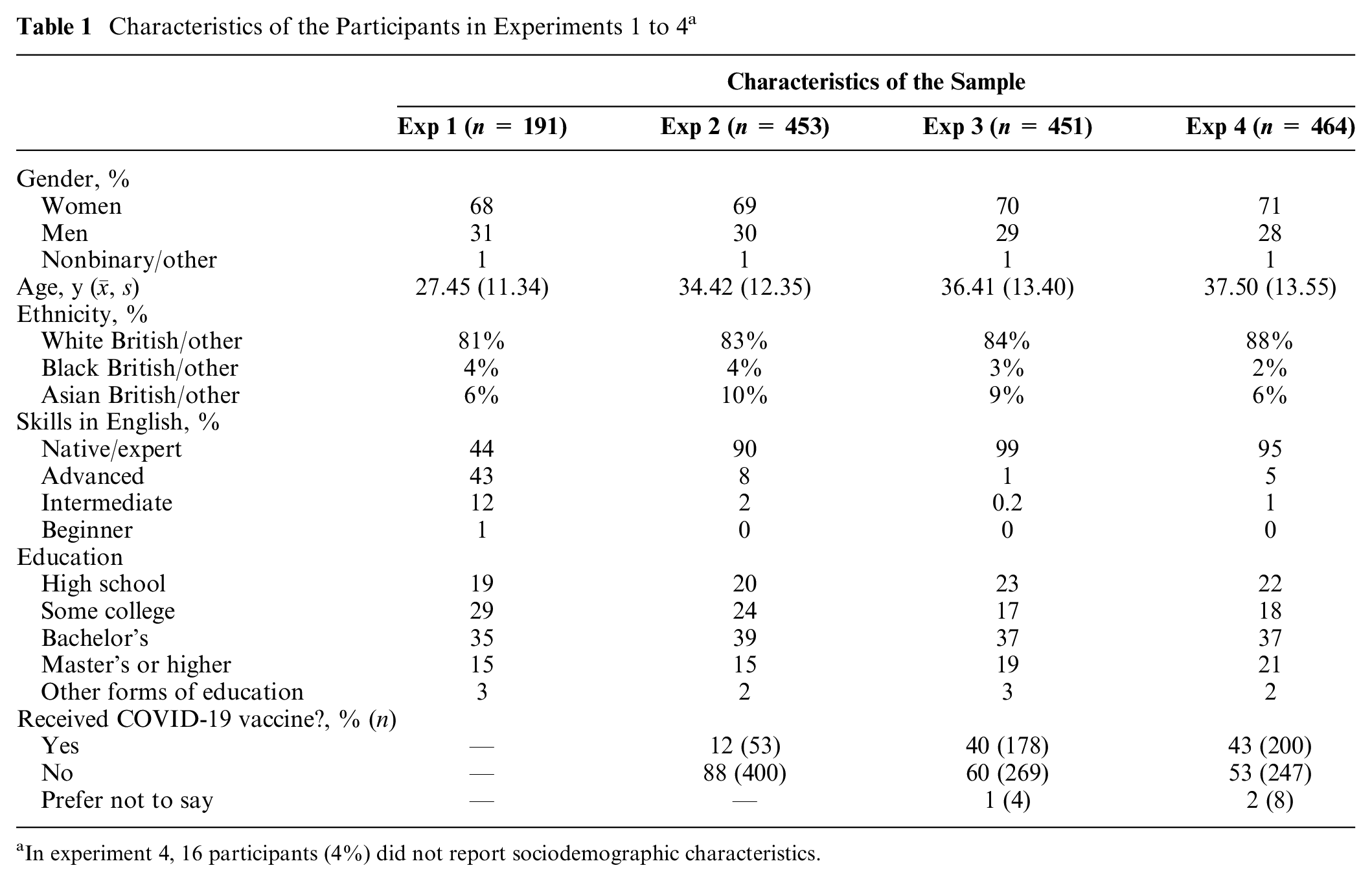
In experiment 4, 16 participants (4%) did not report sociodemographic characteristics.
Design, Materials, and Procedure
Participants completed the study online. Participants first answered questions that measured their trust in the health care system and the government along with their beliefs and feelings about the COVID-19 pandemic. We used the 9-item Distrust in the Healthcare System scale 39 (e.g., “The healthcare system covers up its mistakes”; Cronbach’s α = 0.80) and 1 question about trust in the government to manage the pandemic (i.e., “I believe that the government is handling the pandemic well”). We also included 5 questions about health-related conspiracy theory beliefs (e.g., “The spread of the virus is a deliberate attempt to reduce the size of the global population”; Cronbach’s α = 0.80) and 3 questions measuring how worried participants were about the pandemic (e.g., “When it comes to the new coronavirus, I believe that we are all in danger”; Cronbach’s α = 0.59). For all of these questions, participants responded on a 1 to 5 Likert-type scale ranging from 1 = strongly disagree to 5 = strongly agree, with 3 = neither agree nor disagree. The different constructs were measured on separate pages and presented in a randomized order.
Participants were then randomly allocated to read 1 of 4 vaccination scenarios resulting from the crossing of 2 independent variables with 2 conditions each (Qualtrics double-blind randomization): framing (positive [n = 95] v. negative [n = 96]) and trustworthiness of the family physician (trustworthy [n = 93] v. untrustworthy [n = 98]). Participants imagined that they were attending a regular checkup with their family physician and that their family physician offered them a COVID-19 vaccine. In the scenario, the family physician described the possibility of experiencing adverse side effects from the vaccine as being “a small probability” in the negative framing condition or as being “unlikely” in the positive framing condition. The verbal probability “a small probability” attracts attention toward the outcome occurrence (having adverse side effects) and is hence considered negative, whereas “unlikely” attracts attention toward the complementary outcome (not having adverse side effects40,41) and was hence considered positive.
The trustworthiness of the family physician was manipulated through their social warmth and competence in the consultation, based on the dual account of trust. 42 We used an existing trust manipulation that was found to be successful in the United Kingdom, where the trustworthy family physician was warm (e.g., making frequent eye contact) and competent (e.g., conducting the examination well), whereas the untrustworthy family physician was cold (e.g., making limited eye contact) and incompetent (e.g., making mistakes in the examination). 21 In the scenario, we also included a photo of the family physician that showed a White man from the Chicago Face database. 43 The photo was either that of the most or least trusted White men in the database.
At the end of the scenario, participants reported their intention to be vaccinated on a 5-point Likert-type scale ranging from 1 = No, I definitely do not want the vaccine to 5 = Yes, I would definitely like the vaccine, with 3 = I am not sure. The responses to this question were fairly distributed, with 44% responding that they would prefer not to have the vaccine (answers 1 or 2) and 39% responding that they wanted it (answers 4 or 5) and 17% not being sure.
After the vaccine scenario, participants reported on a separate page the extent to which they trusted the family physician, as a manipulation check. Participants rated their trust in the family physician from the scenario on a 1 to 5 Likert-type scale (not at all, a little, a moderate amount, a lot, and completely). Then, participants evaluated the chance that a vaccine would cause adverse side effects given that these were described as “unlikely” (the positive framing condition) or as having “a small probability” (the negative framing condition). Participants reported their judgment on a 0% to 100% slider scale. They then answered some sociodemographic questions. The trust manipulation was effective, and participants rated that the 2 verbal probability statement conveyed a similar probability (see Supplementary Materials on the OSF).
Analyses
The effect of the framing and trust manipulation on vaccination intention were tested in a variance analysis using framing and trust as between-subjects independent variables and vaccination as a dependent variable. We test the robustness of the effects by repeating this analysis together with relevant covariates for each study (e.g., COVID conspiracy beliefs).
Results
As shown in Figure 2, when the family physician was trustworthy, participants reported greater intentions to have the COVID-19 vaccine in the positive framing condition compared with the negative framing condition (green v. red), but the trend was the opposite when the family physician was not trustworthy: participants reported stronger intentions to have the vaccine when the framing was negative compared with when it was positive. This pattern is supported by the interaction effect between framing and trust that we found in a variance analysis, F(1, 190) = 11.35, P = 0.001, η2p = 0.06, while the main effect of framing and trustworthiness was not statistically significant, F(1, 190) = 0.15, P = 0.90, η2p < 0.01, and F(1, 190) = 1.60, P = 0.21, η2p = 0.01. When we repeated this analysis with distrust in health care systems, beliefs in health conspiracy theories, trust in government, and worry about COVID-19 as covariates, we still found that the interaction effect between framing and trust, and the effect of trust, became statistically significant as well, F(1, 190) = 5.06, P = 0.026, η2p = .03, and F(1, 190) = 9.80, P = 0.002, η2p = 0.05. In addition, both distrust in the health care system and beliefs in health conspiracy theories predicted lower intentions to be vaccinated, F(1, 190) = 6.02, P = 0.015, η2p = 0.03, and F(1, 190) = 60.63, P < 0.001, η2p = 0.25.
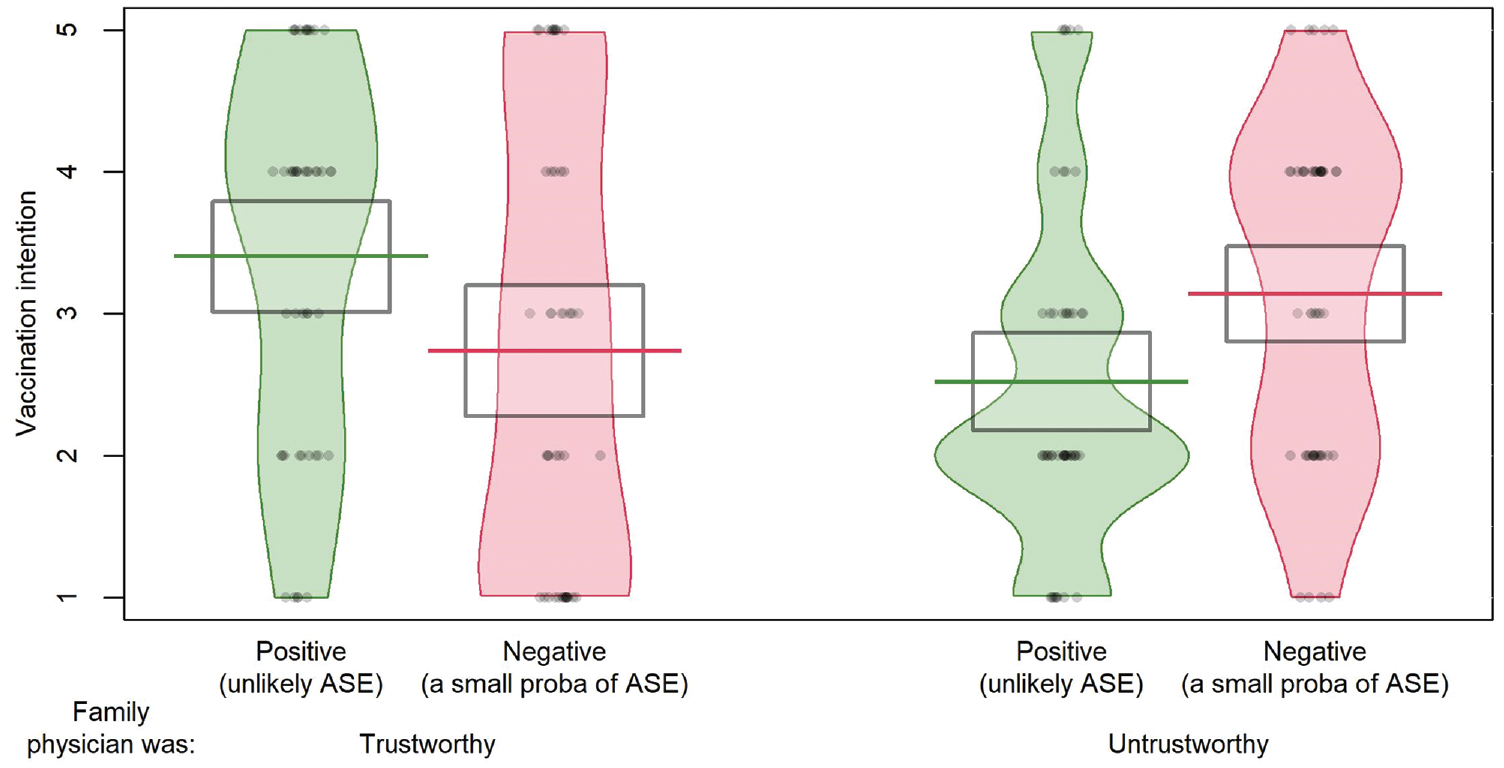
COVID-19 vaccination intentions depended on the way the risk of adverse effects was framed and the trustworthiness of the speaker in experiment 1 (n = 191).
Experiment 2
Experiment 2 was a preregistered replication of experiment 1, conducted on a larger sample of UK residents. The study materials were the same, except that we counterbalanced the order of presentation of the individual difference measures (before or after the vaccination scenario) and included only the measure of individual differences that predicted vaccination intention in experiment 1 (distrust in the health care system and COVID conspiracy beliefs).
Method
Participants
We invited 450 UK residents to complete the study on the Prolific platform, but 453 completed the study fully. Prolific is a platform managing a large pool of participants that delivers quality data. 44 Participants were paid £0.71 for a study with a median completion time of 8 min (£0.60 fee and £0.11 bonus). None of the participants completed the study in less than 2.5 min. Participants’ characteristics are shown in Table 1. This gave us a 99.96% power to identify an interaction effect, framing × trust, of a similar size to study 1 (ηp2 = 0.06, f = 0.25).
Design, materials, and procedure
Participants completed the study on March 4, 2021, when adults older than 60 y were invited to be vaccinated. Participants were randomly allocated to 1 of 4 conditions from the 2 (framing: positive [n = 226] v. negative [n = 227]) × 2 (trust: trustworthy [n = 227] v. untrustworthy [n = 226]) design. The experiment was the same as experiment 1 except for 2 changes. The study included the Distrust in the Healthcare System and the COVID conspiracy beliefs scales but not the measures of trust in the government and COVID-19 worry because those did not predict vaccination intentions. We also amended the measure for vaccination intention by adding a response option I have already been vaccinated to the vaccination intention scale that ranged from 1 = No, I definitely do not want the vaccine to 5 = Yes I would definitely like the vaccine. Of the 453 participants, 12% answered that they had already been vaccinated (n = 53). Among unvaccinated participants, the reported vaccination intentions were fairly high, showcasing the positive trend in support for the vaccine while the rollout occurred. 45 Only 18% of participants reported not wanting the vaccine (answers 1 or 2), whereas 77% reported that they wanted it (answers 4 or 5) and 6% reported that they were not sure. The trust manipulation was effective, but participants rated that the positively framed risk statement conveyed a higher probability than the negative one, so we included subjective probability perception as covariate in the analyses (see Supplementary Materials on the OSF).
Results
When the family physician was trustworthy, participants reported a slightly greater intention to be vaccinated in the positive framing compared with the negative framing condition, and the opposite occurred when the physician was untrustworthy (see Figure 3). Despite the similarity to experiment 1, the interaction effect was not statistically significant (see Table 2, model 1). Framing did not affect vaccination intentions either, but trust did (see Table 2, model 1). Participants were more likely to agree to have the vaccine when the family physician was trustworthy than untrustworthy.
Vaccination intentions as a function of framing and trustworthiness of the family physician in experiment 2 (n = 453).
Effect of Framing and Trust on COVID-19 Vaccination Intentions (Model 1) Together with Covariates: Probability Perception of Side Effects (Model 2) and Personal Attitudes and Beliefs regarding Health Care (Model 3)
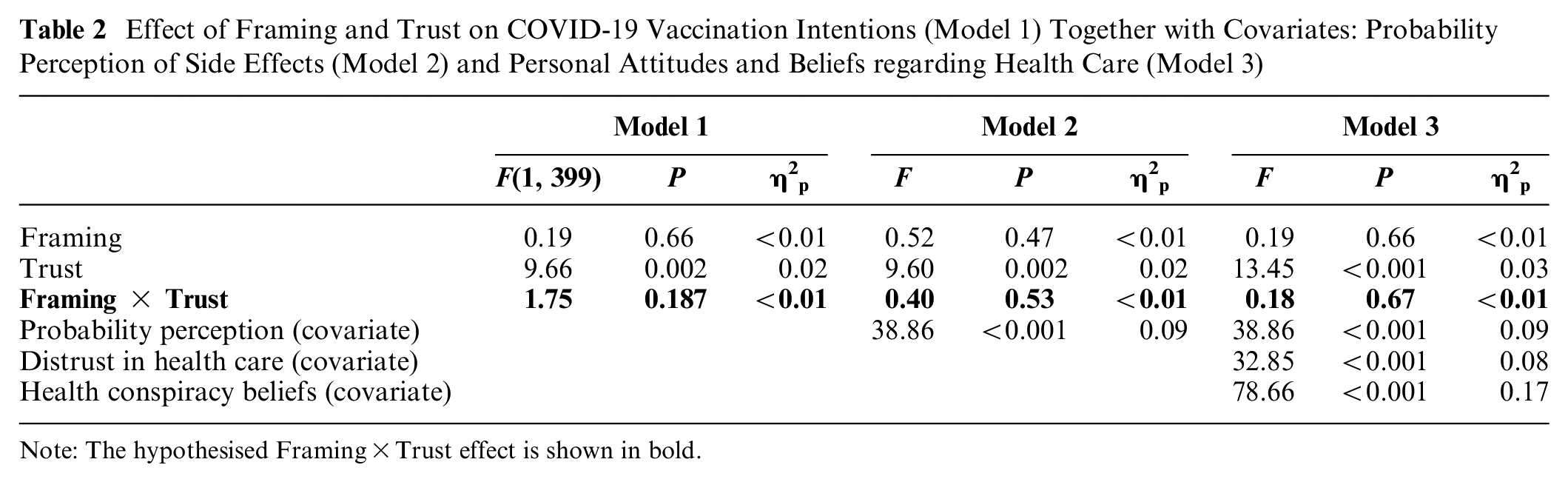
Note: The hypothesised Framing×Trust effect is shown in bold.
Furthermore, we reran the model while including participants’ probability perceptions as a covariate, since participants felt they were more at risk from the vaccine in the positive framing condition (model 2). This analysis produced the same conclusion, with an additional relationship between probability perception and vaccination intentions (see model 2). Finally, in a third model, we included participants’ levels of distrust in the health care system and beliefs in health conspiracy theories. This third model yielded the same pattern of findings (see model 3).
Experiment 3
This preregistered experiment aimed to replicate experiment 2 but with more variability in vaccination intention to avoid a ceiling effect.
Method
Participants
A sample of 454 participants recruited via Prolific completed the study and were paid £0.55 (median time: 6 min). Three cases in which the completion time was less than 2.5 min were excluded. The remaining sample of 451 is described in Table 1. This sample gave us 75% power to detect an effect size that was 50% smaller than the one observed in experiment 1, which represented the average effect size between experiments 1 and 2 (ηp2 = .03, f = 0.125).
Design, materials, and procedure
Participants completed the study in mid-April 2021, when the vaccination program was progressing toward younger age groups, with people aged 45+ y being invited. Participants were randomly allocated to 1 of 4 conditions from the 2 (framing: positive [n = 226] v. negative [n = 225]) × 2 (trust: trustworthy [n = 221] v. untrustworthy [n = 226]) design. The study replicated experiment 2, except for slight variations in the vaccine scenario to ensure a better distribution of answers. Importantly, we changed the vaccination intention question and focused on whether participants wanted the vaccine now or if they preferred to wait (and possibly have a different vaccine later). This took into account the rising concerns surrounding the potential adverse side effects of the Oxford/AstraZeneca vaccine. These concerns manifested in a surge in Google searches for “COVID-19 vaccine side effects” (Figure 1) and reports of individuals willing to be vaccinated yet refusing to have the Oxford/AstraZeneca vaccine. 46 The change in the measure was effective in providing a less skewed distribution of answers. Of the 451 participants, 32% reported that they would rather wait (answers 1 or 2), 59% reported that they wanted the vaccine now (answers 4 or 5), and 10% reported being unsure.
We also included a separate question about vaccination status at the onset of the study, and participants who had already had at least their first injection were instructed to imagine that they had not done so yet. In the sample, 59.6% had not yet been vaccinated (n = 269), 39.5% had already been (n = 178), and 0.9% preferred not to disclose this information (n = 4). The trust manipulation was effective but also interacted with framing and vaccination status to determine subjective trust (see SM on OSF), so we included vaccination status in our analyses. Furthermore, participants rated that the positively framed risk statement conveyed a higher probability than the negative one, so we included subjective probability perception as covariate in the analyses (see OSF).
Results
We assessed the effect of framing and trust on vaccination intention and found a main effect of trust and an interaction effect between framing and trust. However, on inspection of the data, it was clear that this effect was qualified by an interaction with the participant’s vaccination status. To best account for the data, we explored the expected effect of framing and trust as a function of vaccination status, and we report in SM the confirmatory analyses of the hypothesized effect, focusing only on framing, trust, and their interaction.
On average, trustworthiness and positive framing led to greater vaccination intention, but the 2 also interacted, and the nature of this interaction depended on vaccination status. As shown in Figure 4, for participants who were already vaccinated (top panel), the trustworthiness of the physician also mattered, but the effect of framing did not depend on it: vaccinated individuals reported greater intentions to vaccinate when the framing was positive than when it was negative. In contrast, in participants who were not yet vaccinated (right panel), the framing effect was the opposite in the trustworthy and untrustworthy conditions. In unvaccinated individuals, the positive framing voiced by a trustworthy physician backfired: unvaccinated participants reported greater intentions to be vaccinated based on the negative framing than based on the positive framing when the physician was trustworthy. Conversely, the positive framing voiced by an untrustworthy physician lead to greater vaccination intention than the negative framing for unvaccinated individuals. They were more convinced by the positive framing of the untrustworthy physician than by their negative framing.
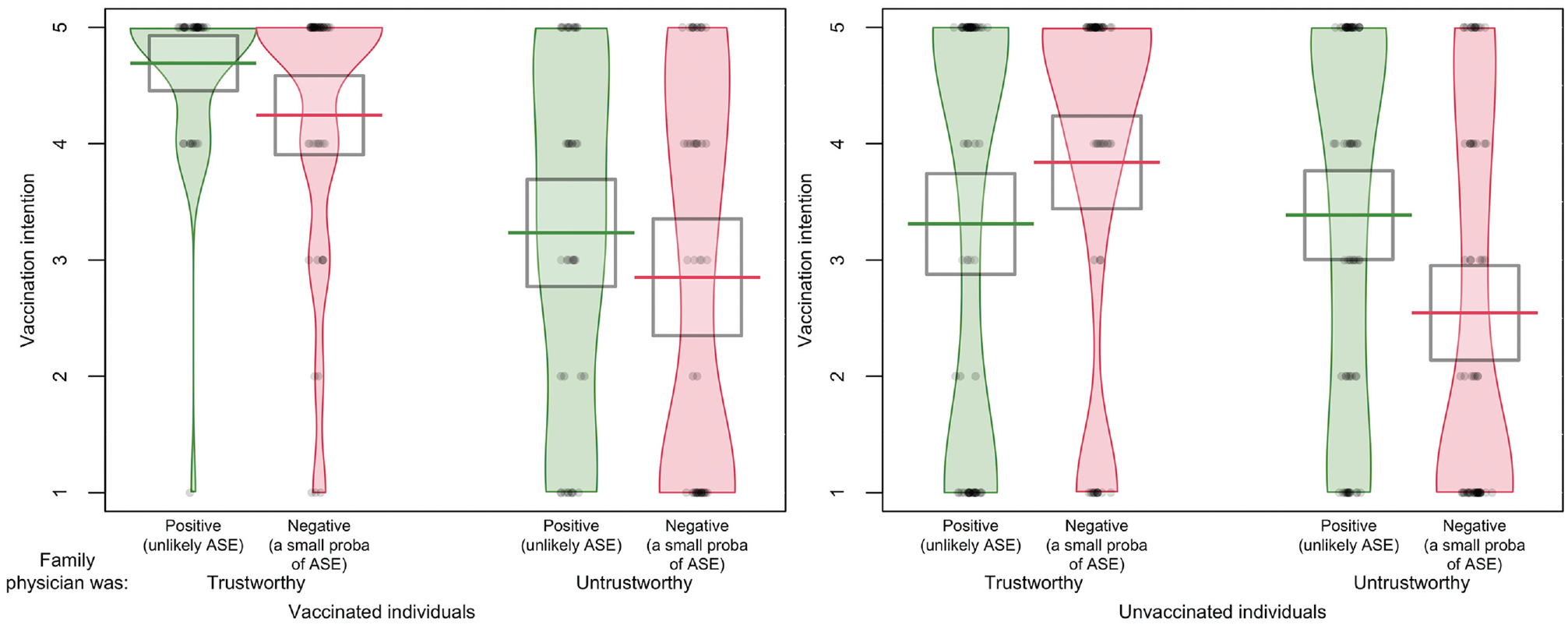
The effect of framing and trustworthiness on vaccination intention differed between participants who were vaccinated and those who were not (experiment 3, n = 451).
In other words, for unvaccinated individuals, a trustworthy family physician stressing the risk of adverse side effects using negative framing led to an increase in vaccination intention (v. positive framing), whereas an untrustworthy family physician using negative framing (v. positive) led to a decrease in vaccination intention. This difference in the effect of framing and trust as a function of vaccination status was supported by a statistically significant 3-way interaction effect (see Table 3, model 1). Clearly, our participants who were yet to be vaccinated (and who could possibly suffer from adverse side effects) were more skeptical about the good intentions of the warm and competent family physician (as seen in their trust perception), especially when the physician stressed that adverse side effects were “unlikely” (v. “a small probability”).
Effect of Framing, Trust, and Vaccination Status on COVID Vaccination Intention (Model 1), Together with Probability Perception of Side Effects and Personal Attitudes and Beliefs regarding Health Care as Covariates (Model 2)
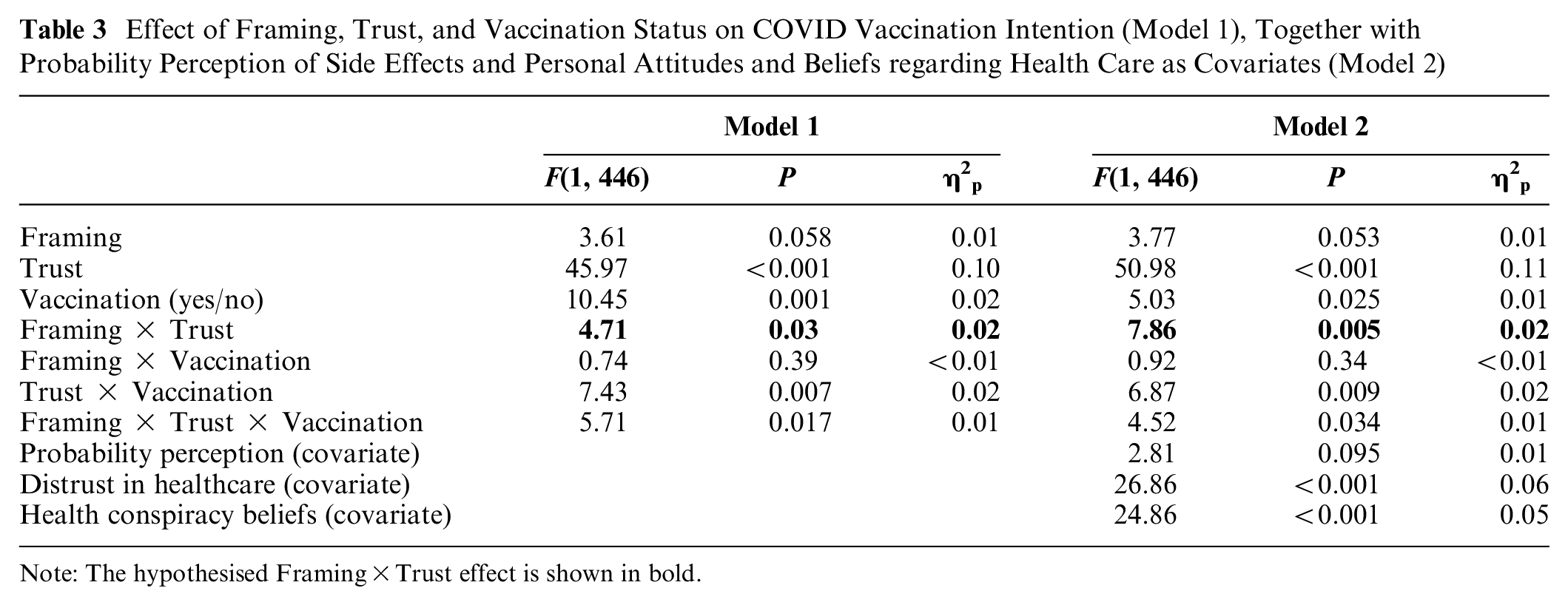
Note: The hypothesised Framing×Trust effect is shown in bold.
The results also show a main effect of trust (more trust = greater vaccination intention) and a main effect of vaccination status (vaccinated = greater vaccination intention), whereas the effect of framing on its own was not statistically significant. The same analysis including participants’ probability perceptions, levels of distrust in the health care system, and beliefs in health conspiracy theories as covariates showed a consistent picture. The effects were the same, with an additional effect of distrust in health care and health conspiracy beliefs (Table 3, model 2).
Experiment 4
Results of Experiments 1 to 3 show that the interaction pattern between framing and trust evolved based on respondents’ vaccination experience. To examine the effect of framing and trust, while minimizing the role of experience, we replicated our study in a new hypothetical context.
Method
Participants
We invited 470 participants from the United Kingdom to complete the study on Prolific, and 471 participants started the study; of those, 7 did not complete the main part fully and were excluded, providing a sample of 464 participants. Participants were paid £0.50 for completing the 5-min study. The sample is described in Table 1. Participants who preferred not to report their COVID-19 vaccination status (n = 8) or those who did not answer that question (n = 9) were not included in the analyses where vaccination status was controlled for (n = 447 for those). A sample size of 464 gave us 77% power to detect an effect size that was 50% smaller than the one observed in experiment 1 (ηp2 = 0.03, f = 0.125).
Design, materials, and procedure
Participants completed the study at the end of April 2021. The study replicated experiment 3 but focused on a new antibiotic-resistant bacteria instead of COVID-19. Participants were randomly allocated to 1 of 4 conditions from the 2 (framing: positive [n = 233] v. negative [n = 231]) × 2 (trust: trustworthy [n = 232] v. untrustworthy [n = 232]) design. The scenario was hypothetical yet realistic, with the rise of antibiotic-resistant bacteria and the search for vaccines against bacterial infections. 47 The family physician appointment scenario was exactly the same, except that at the end, the patient was offered a vaccine against a hypothetical antibiotic-resistant “Zora” bacteria. Responses were well distributed: 35% of the participants reported that they would rather wait (answers 1 or 2) and 44% said that they wanted the vaccine now (answers 4 or 5), while 21% reported being unsure. The trust manipulation was effective to determine subjective trust, and participants rated that the positively framed risk statement conveyed a higher probability than the negative one (see OSF), so we included subjective probability perception as covariate in the analyses.
Results
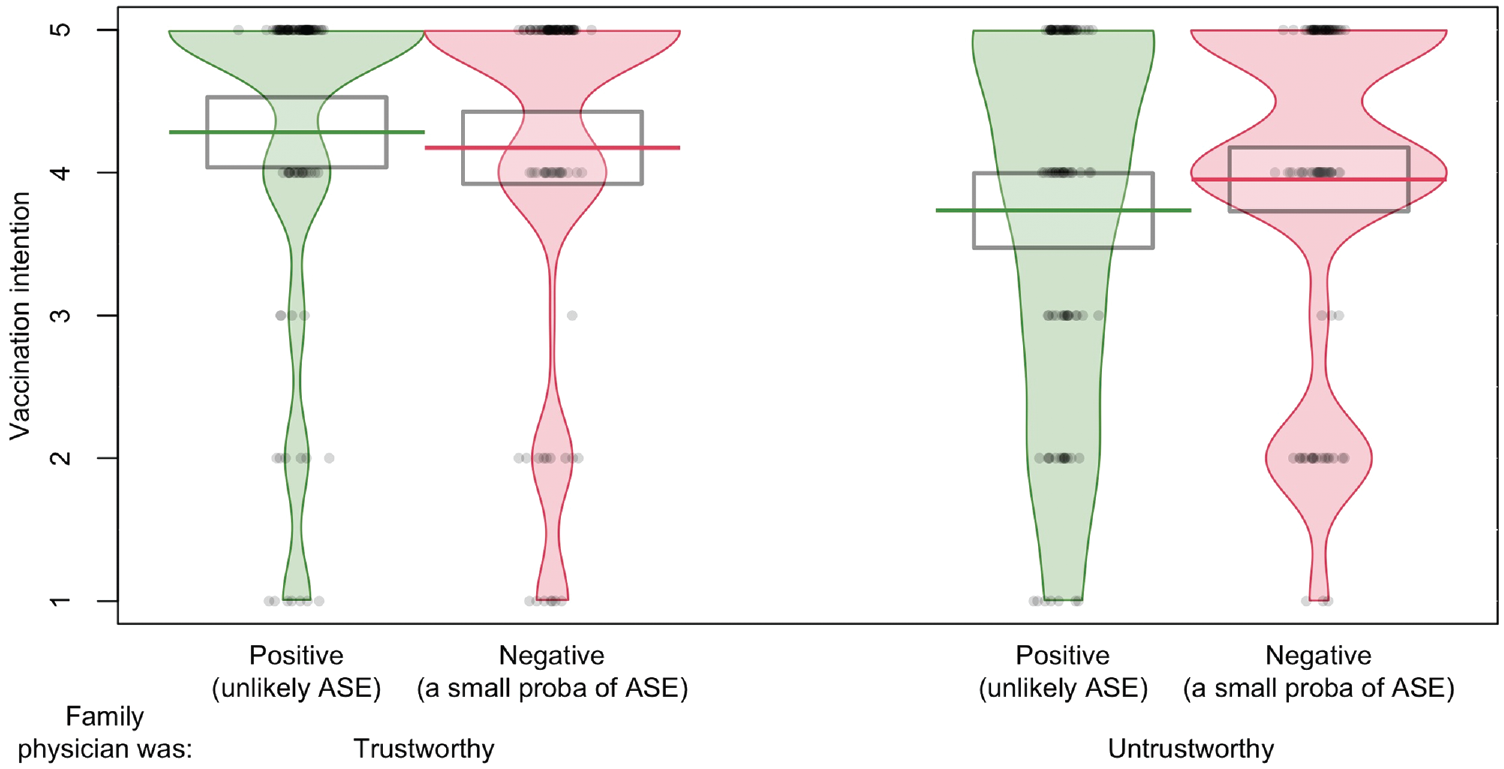
As shown in Figure 5, an interaction pattern between framing and trust is visible: when the family physician was trustworthy, participants reported greater intentions to have the vaccine in the positive framing condition than in the negative framing condition (green v. red), but when the family physician was untrustworthy, the difference between the framing conditions was close to nil. This trend was supported by a statistically significant interaction effect between framing and trust after introducing the covariates probability perception and vaccination status (see Table 4, model 2). The model also showed a main effect of framing and trust. Participants also reported greater intentions to be vaccinated when the family physician was trustworthy (v. untrustworthy) and when the risk of adverse side effects was positively framed (v. negatively framed).
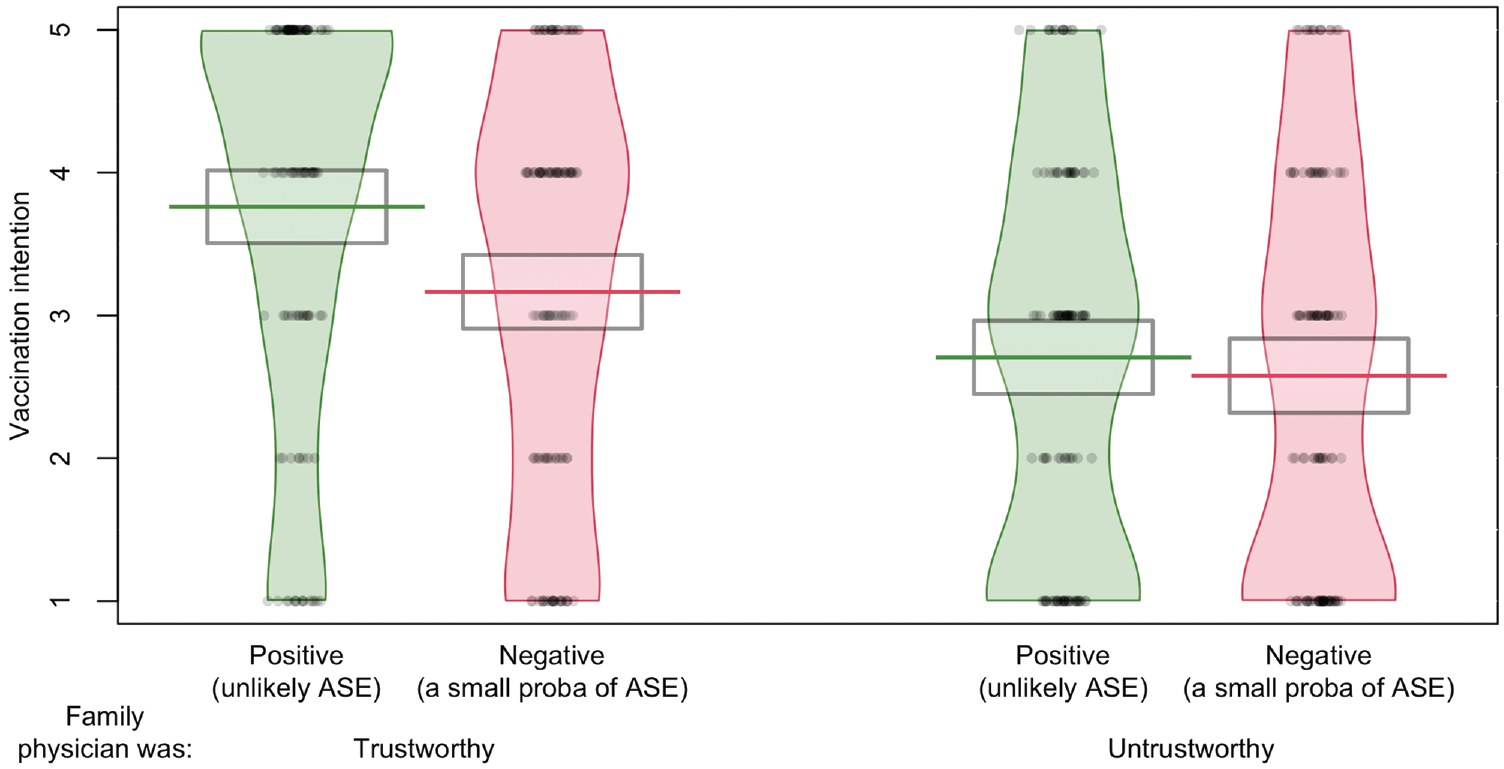
Vaccination intention for a hypothetical bacterial illness as a function of framing and trustworthiness of the family physician in experiment 4 (n = 464).
Framing and Trust Interacted to Affect Vaccination Intention for a Hypothetical New Illness in Line with a Pragmatic Account of the Framing Effect (Experiment 4, n = 464)
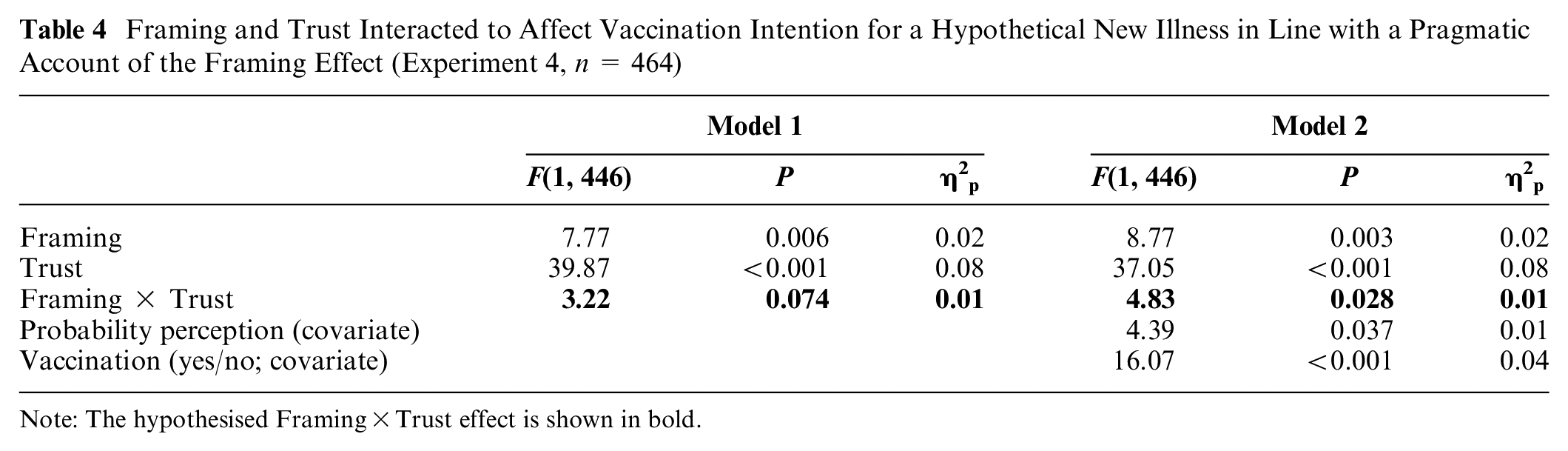
Note: The hypothesised Framing×Trust effect is shown in bold.
Meta-analyzing Results from Experiment 1 to 4
In experiment 1 and 4, we found the expected Framing × Trust interaction effect on vaccination intention. In experiment 2, the effect was not statistically significant, whereas in experiment 3, the effect was better explained by a 3-way interaction. To assess the moderating role of trust in the framing effect, we pooled the data of the 4 studies together and conducted a meta-analysis of the framing effect with trust as a moderator. The analysis including all of the studies show high residual heterogeneity and no moderating effect. In experiment 3, the trend was opposite to that of experiments 1, 2, and 4, because unvaccinated participants responded more positively to the negative framing of risks (the statement that attracted attention to the risks), in a context of heightened fears about the Astra-Zeneca vaccine. The inclusion of all of the studies, except the unvaccinated participants of experiment 3, showed a lower and acceptable level of residual heterogeneity and a moderating effect of trustworthiness on the framing effect. Based on that meta-regression, the moderating effect of trustworthiness on the framing effect was Cohen’s d = 0.42, 95% CI [0.09, 0.75]; more specifically, when the physician was trustworthy, the framing effect was Cohen’s d = 0.34, CI [0.09, 0.75], and when the physician was untrustworthy, the framing effect was Cohen’s d = −0.07, CI [−0.31, 0.16]).
General Discussion
A rapid and massive uptake of vaccinations is necessary to control and possibly eradicate epidemics. With the perceived risk of adverse side effects being a key driver of vaccination intention, 48 it is critical to ensure the effective communication of those risks. In 4 experiments, we evaluated the effect of framing the risk of adverse side effects positively or negatively as a function of the trustworthiness of the person communicating the risk. We expected and globally found that, when communicated by a trustworthy physician, positive framing led to a greater vaccination intention than negative framing, whereas the effect was smaller or even reversed when the physician was untrustworthy.
We evaluated whether people were more likely to agree to be vaccinated when the risks of adverse side effects from the vaccine were positively framed (“they are unlikely,” focusing attention away from their possible occurrence) compared with negatively framed (“there is a small probability they will occur,” focusing attention toward their possible occurrence). Consistent with the “implicit advice” pragmatic account of the framing effect,8,20,26,27 we found that the effect of framing depends on the trustworthiness of the speaker, but the patterns were more complex than that. The interaction pattern found on the COVID vaccination intention in experiments 1 and 2 conducted before most people could get vaccinated, and experiment 4, conducted on a hypothetical vaccine, showed the classic and expected framing effect in the trustworthy condition (i.e., positive framing increased vaccination intention) and a null or opposite tendency when the family physician was clearly incompetent and socially detached. However, this pattern evolved and seemed to wear off, with smaller differences in experiment 2, when a large majority of people eagerly waited for the COVID vaccine. The results of experiment 3 also supported the importance of the role of experience, showing that the interaction pattern between trust and framing depended on whether participants had received the COVID vaccine or not. Specifically, unvaccinated individuals reported greater vaccination intentions when the risk of adverse effects was acknowledged using negative framing (i.e., “there is a small probability of adverse side effects”) than when they were positively framed (i.e., “adverse side effects are unlikely”). In that particular group and context (unvaccinated individuals with a heightened perception of risks), emphasizing that adverse side effects were “unlikely” actually backfired compared with acknowledging that they had a “small probability” of occurring. In contrast, people who had already been vaccinated showed the expected pattern, being more likely to prefer vaccination based on the positive frame than the negative one. This is consistent with past work showing the negative effect of noncredible sources strongly denying the existence of vaccine risks 4 and the positive effect of disclosing negative information on trust. 49 This finding adds to other “backfiring” interventions, such as those in which debunking false information led to an increase in belief in that misinformation. 50 The pattern of experiment 3 might be due to the heightened climate of concerns about the Oxford/AstraZeneca vaccine at the time. 46 The disclosure in the media that the Oxford/AstraZeneca vaccine had worse adverse side effects than expected may have increased participants’ vaccine risk perception, fed conspiratorial beliefs that powerful institutions hide the truth about vaccines, and eroded trust in health practitioners promoting the COVID vaccine. Indeed, vaccine risk perception is linked with conspiratorial beliefs and low trust in health professionals,23,51 although it is not clear if conspiracy beliefs cause decrement in vaccination intention or the other way around. 52
Overall, our findings support that verbal framing effects do not simply occur as an automatic emotional bias in reaction to a frame9,24,25 but instead rely on a more reflective and socially rooted pragmatic inference.20,26,40,53 Framing acts as an implicit advice, and therefore, theories of framing have to further integrate people’s preferences and experiences to account for the complex dynamics of the advice taking beyond the logic of conversation: advice given does not necessarily translate into advice taken. Theories of framing could rely further on the advice-taking literature. 30 The advice-taking literature acknowledges the importance of the trustworthiness of the advisor to account for variation in advice taking but also clearly outlines the importance of people’s perception of the option presented to them. 30 Advice is more likely to be discounted when it is given by someone untrustworthy 31 or when it is further away from one’s preference. 54 Accordingly, the effect of framing was weakened when participants were uncertain and the source was untrustworthy (experiments 1, 2, and 4) or when participants had a strong preexisting preference (experiment 2, when most people wanted the vaccine), whereas the effect was even reversed when the outcome was undesirable (for people who remained unvaccinated at a time when vaccination was widely available in experiment 3). The classic framing effect seems to reflect a situation in which people trust the source, experience high uncertainty, and have no clear preference.
Across experiments, the simple effect of verbal framing on vaccination intention (without interaction) occurred only in the hypothetical context of experiment 4, again highlighting the role of knowledge and personal preference and hinting that artificial tasks (where participants have no relevant knowledge) may magnify the role of framing in decisions. Possibly, verbal risk framing is less potent than attribute risk framing (which uses numbers with opposite outcomes, e.g., 1 in 10 people suffer from adverse side effects v. 9 in 10 do not), but numerical attribute framing has also yielded mixed results, with in some cases positive framing having a positive effect5,6,11 and sometimes not.35,36 Furthermore, our results hint at an explanation of the mixed findings, since the effect of framing depends on the perceived trustworthiness of the source and the perceived value of the vaccine. Null results might have been found in cases where the information provider was deemed untrustworthy (or trust perception was split) or where attitudes were negative, whereas past work demonstrating “classic” framing effects could occur where the information provider was assumed to be trustworthy and the option appeared appealing to some extent.
Overall, our work highlights the importance of building trust in encouraging vaccination uptake consistently with past work on trust in the health care system, 55 health care professionals, 56 and family physicians. 33 Importantly, the effect of trust in our studies relies on a strong manipulation of trustworthiness, in which a competent and caring doctor is compared with a more distant and incompetent doctor, but other factors may also play a role in trust perception, like the belief that a doctor is hiding their true nature. We successfully manipulated trust through cues such as making eye contact (v. gazing toward their computer), but this kind of manipulation is culturally sensitive and might need to be adapted for cultures in which eye contact may seem disrespectful. 57
In addition, we can recommend positively framing the risk of adverse side effects of vaccines when the source is trusted and in a context without heightened fears. When the speaker is trustworthy, framing the risk of side effects in a positive way may help to reassure people about the vaccine, but only if this is perceived as genuine. In a context with heightened fears, this may backfire. When sources are not trusted, negative framing may be a better bet; it may not matter or have a positive effect. This form of upfront communication may be perceived as balanced and autonomy supportive, which was shown to increase vaccination intention. 58
Limitations
An important caveat when considering our data is that we focused on hypothetical situations. The situations were quite realistic (people were invited to be vaccinated at the time), but still, it is unclear whether people’s intention to be vaccinated would translate into actual behaviors. Furthermore, the trustworthiness of the personal physician was manipulated via their competence and warmth, but it is not clear which of these 2 dimensions was most relevant in the interaction with framing. Are people more likely to rely on someone’ advice because they are competent or caring?
Overall, our findings show the major role of the social context on (medical) decision making and the importance of tailoring risk communication as a function of that social context. Positively framing the risk of adverse side effects increased vaccination intentions when it came from a trusted source, but this effect was reduced or even reversed in situations in which the source was not trustworthy and when people experienced heightened worries about risk.
Supplemental Material
sj-docx-1-mdm-10.1177_0272989X231197646 – Supplemental material for How Should Doctors Frame the Risk of a Vaccine’s Adverse Side Effects? It Depends on How Trustworthy They Are
Supplemental material, sj-docx-1-mdm-10.1177_0272989X231197646 for How Should Doctors Frame the Risk of a Vaccine’s Adverse Side Effects? It Depends on How Trustworthy They Are by Marie Juanchich, Miroslav Sirota and Dawn Liu Holford in Medical Decision Making
Footnotes
Acknowledgements
We are grateful to Maria Kyriakou and Margarita Christou for helping with the data collection of experiment 1.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors received no financial support for the research, authorship, and/or publication of this article.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.