
Abstract
Objective
To verify whether three different framing effects (risky choice, attribute and goal) exist in simulated medical situations and to analyse any differences.
Methods
Medical decision-making problems were established, relating to medical skill evaluation, patient compliance and a selection of treatment options. All problems were described in positive and negative frame conditions.
Results
Significantly more positive evaluations were made if the doctor’s medical records were described as ‘of 100 patients, 70 patients became better’ compared with those described as ‘of 100 patients, 30 patients didn’t become better’. Doctor’s advice described in a negative frame resulted in significantly more decisions to comply, compared with advice described in a positive frame. Treatment options described in terms of survival rates resulted in significantly more adventurous choices compared with options described in terms of mortality rates. Decision-making reversal appeared in the risky choice and attribute frames, but not the goal frame.
Conclusions
Framing effects were shown to exist in simulated medical situations, but there were significant differences among the three kinds of such effects.
Introduction
Framing effects refer to important changes in decision making (including reversal of decision) regarding the same problem when it is presented in different ways (or frames). 1 The Asian disease problem is an example where participants were told to imagine that a government was preparing for an outbreak of an Asian disease that was expected to result in 600 deaths. Two sets of rescue plans were proposed: plan A that could save 200 people (400 deaths), and plan B that had a one-third probability that all 600 people would be saved (no deaths) and two thirds probability that no one would be saved (all dead). When the question was framed in terms of ‘lives saved’, 72% chose option A; when the problem was framed in terms of ‘deaths’, 78% chose option B. 1 Further studies have shown that regardless of whether people are faced with economic, life-saving, resource allocation, or management decisions, framing effects are consistently found.2–7 Studies have also found different effects between different frames. 2 The following three kinds of frames have been distinguished in decision making: attribute frame; goal frame; risky choice frame.8,9 ‘Attribute frame’ refers to the positive or negative description of the object characteristics, for example, whether a pound of beef is described as 80% lean or 20% fat, may significantly influence a person’s evaluation of it. ‘Goal frame’ refers to the descriptions of the benefit brought from actions or the consequence of no action in significantly influencing people’s motivation and execution. ‘Risky choice’ frame refers to how describing prospects of a programme in a positive or negative way will result in a change in the willingness to take risk, the most relevant example being the Asian disease problem.1,9
There have been many studies into framing effects in medical situations,5–6,10 but these have generally included only one kind of frame. A preliminary study explored the attribute, goal and risky choice frames in a simulated medical situation. 11 The current study explored the impact of information presentation on medical decision-making problems, focusing on differences between the attribute, goal and risky choice framing effects.
Subjects and methods
Study population
This study was conducted using a battalion of an infantry regiment in Xi’an, China, on 15 September 2011. Male soldiers, with education levels that were higher than junior middle school, were recruited into the study and provided with a notebook as a reward for participating. Subjects were sequentially numbered according to the time that applications to participate in the study were submitted. The study protocol was approved by the Ethics Review Committee of the Fourth Military Medical University, Xi’an, China. All study participants provided written informed consent.
Questionnaire design and scoring system
Questions on medical decision-making problems relating to attribute, goal and risky choice frames presented in positive and negative framing conditions, used in the present study.

A between-subject design was used. Subjects were randomly divided into six groups using a computer-generated randomization schedule based on their study number. Subjects within each group were required to answer a total of two decision-making problems, each from a different frame category (attribute, goal or risky choice frame), described in different frame conditions (positive or negative). To reduce the impact of the first decision-making task influencing the second decision-making task, problems were presented in a balanced order between the groups. Questions provided to each of the groups were divided as follows: group 1, A1B2; group 2, B2A1; group 3, B1C2; group 4, C2B1; group 5, C1A2; group 6, A2C1. Subjects completed the questionnaire in the auditorium of the infantry regiment in Xi’an, China. They were informed that there was no right or wrong answer for each question, no time limit, and that the questionnaires were anonymous.
Conservative choices were assigned a value of −1, and risky choices assigned a value of 1. A new variable was computed, equal to the product of the choice option codes and the decision-making confidence codes, according to a previously described method.
12
Thus, a variable could be obtained that represented participants’ decision-making ranging from −5 (strongly tend to choose conservative choice) to 5 (strongly tend to choose risky choice)
Statistical analyses
Data analyses were performed using the SPSS® statistical software package, version 20.0 (SPSS Inc., Chicago, IL, USA) for Windows®. Between-group differences were assessed using χ2-test and a P-value <0.05 was considered statistically significant.
Results
A total of 300 male subjects were selected, with education levels ranging from junior middle school to university. The oldest participant was 26 years and the youngest was 17 years. Of the 300 questionnaires distributed, 300 were returned, but 10 questionnaires were incomplete; the second decision-making question printed on the second page of the questionnaire was blank. Data from these 10 incomplete questionnaires were excluded from the study.
Subject choices relating to three different kinds of frames (attribute, goal and risky choice) presented in positive or negative framing conditions: Results compiled from 290 respondents.
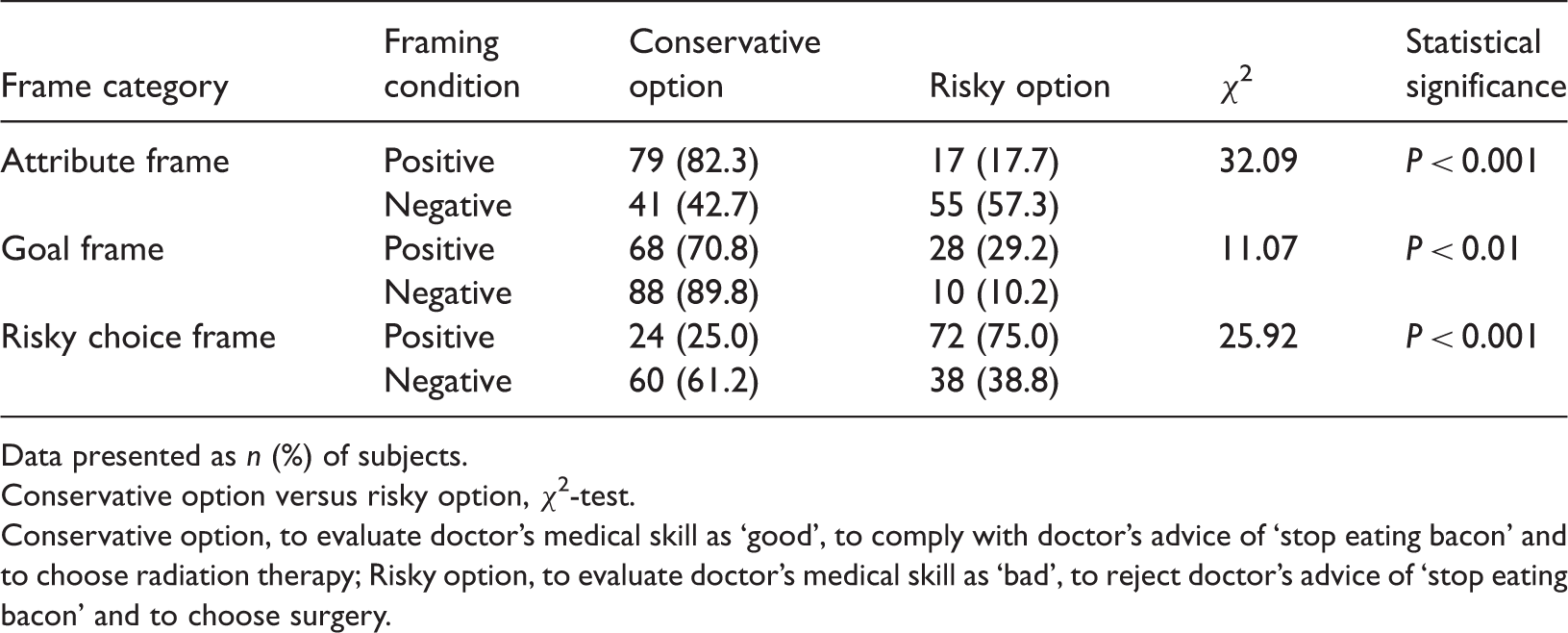
Data presented as n (%) of subjects.
Conservative option versus risky option, χ2-test.
Conservative option, to evaluate doctor’s medical skill as ‘good’, to comply with doctor’s advice of ‘stop eating bacon’ and to choose radiation therapy; Risky option, to evaluate doctor’s medical skill as ‘bad’, to reject doctor’s advice of ‘stop eating bacon’ and to choose surgery.
Analysis of the subjects’ decision-making tendencies showed that decision-making reversal occurred in the attribute frame and risky choice frame, but not in the goal frame (Figure 1).
Decision-making tendencies of 290 subjects regarding medical decision-making problems in three kinds of framing effects (attribute, goal and risky choice), presented in positive and negative frame conditions. Data presented as mean ± SE.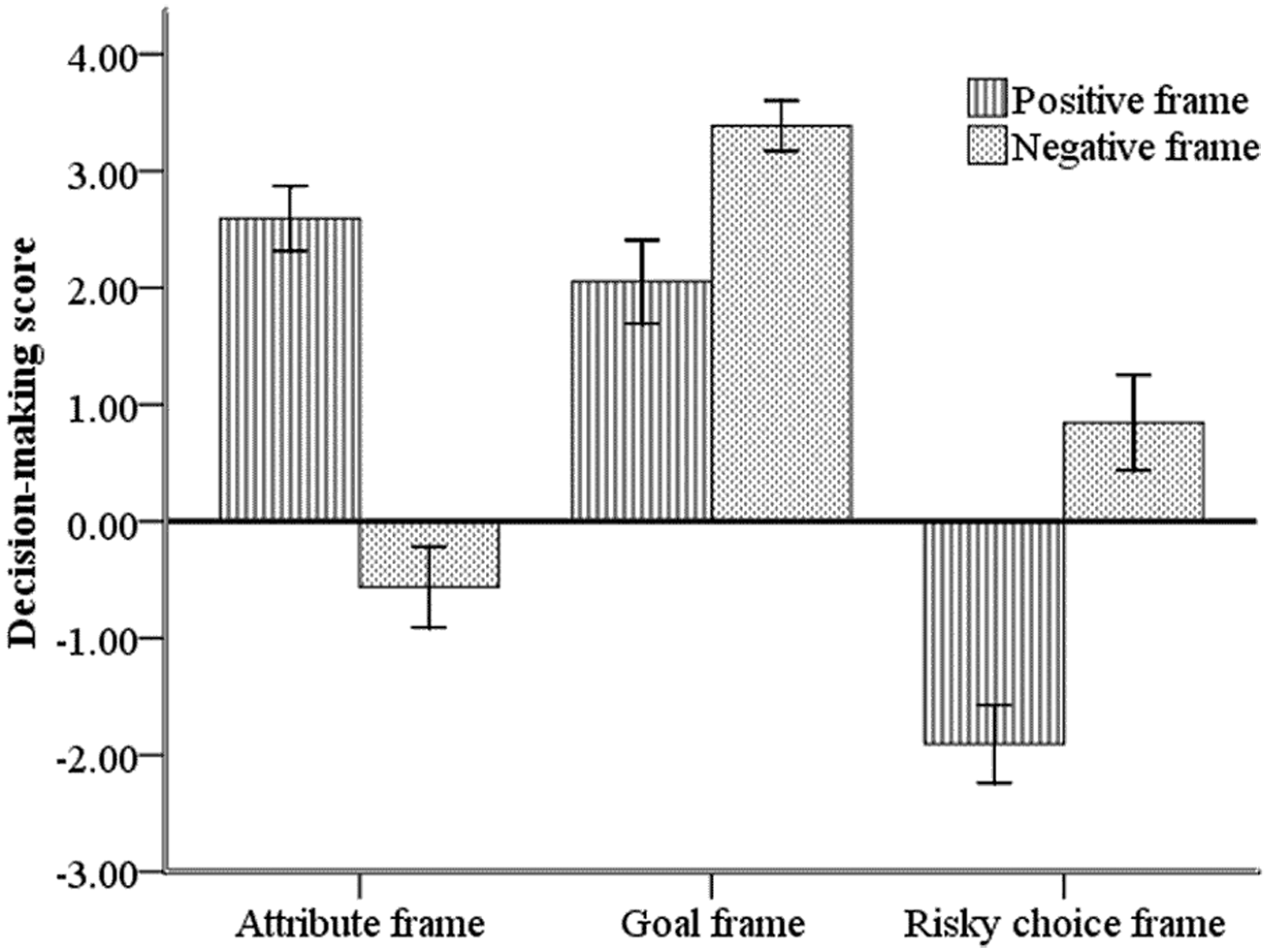
Discussion
The current study demonstrated that all three framing effect categories (attribute, goal and risky choice) existed in the simulated medical situations. In the attribute frame, when medical skill was described in a loss frame condition, evaluations were significantly negative, compared with medical skill described in a gain frame condition; this is consistent with other research. 9
It has been reported that the goal-framing effect is not significant; 8 however, this effect was found to be significant in the present study, which simulated a medical situation. Significantly more subjects chose to comply with the doctor’s advice when it was presented in the negative frame condition (consequence of noncompliance) than in the positive frame (benefit gained from compliance). According to the prospect theory, people are more sensitive to losses than to gains,13,14 where an increase in the probability of catching a disease can be regarded as a loss, and a decrease in the probability of catching a disease can be regarded as a gain. In the present study, subjects chose to comply with the doctor’s advice more readily when the advice was presented as the loss outcome of noncompliance.
Subjects were more inclined to choose radiation therapy treatment with a short-term benefit and long-term loss when they were informed of the survival probability of treatment prospects, than when informed of the probability of mortality. This was possibly because participants provided with information in terms of survival rate regarded the treatment option as an opportunity rather than a threat, but participants provided with information in terms of mortality, regarded the treatment option as a threat rather than an opportunity. Numerous studies have indicated that when decision makers perceive more opportunities than threats, they are more inclined to take risks. In contrast, when they perceive more threats than opportunities, they make more conservative choices.15–16
Two types of framing effect have been distinguished: a bidirectional framing effect, when framing descriptions result in the reversal of decision making; a unidirectional framing effect, which only leads to confirmation bias or preference shift, but not preference reverse. 17 In the present study, we concluded that the attribute and risky choice framing effects were bidirectional, while the goal framing effect was unidirectional.
The present study was limited by the fact that it was conducted under simulated medical conditions, and neither the doctors nor the patients were real. To obtain a better understanding of framing effects regarding medical decision-making problems, the study should be repeated under real medical conditions. Results of the current study could, to some extent, be transferred to medical practice. For example, patients informed of the clinical efficacy rates relating to medicines or to doctors’ performance, may feel more confident and trusting. If medical advice emphasized the potential dangers relating to the consequences of noncompliance, patients may be more co-operative with treatment regimens. If treatment options are described with emphasis on the positive outcomes, patients may be more tolerant to the treatment risk.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.