
Abstract
Background
Infectious diseases such as COVID-19 and HIV/AIDS are behaviorally challenging for persons, vaccine and drug companies, and donors.
Methods
In 3 linked games in which a disease may or may not be contracted,
Results
Each person chooses risky behavior if its utility outweighs safe behavior, accounting for nature’s probability of disease contraction which depends on how many are vaccinated. Each person buys a vaccine or drug if the companies produce them and if their utilities (accounting for side effects and virus mutation) outweigh the costs, which may be subsidized by a sponsor.
Discussion
Drug purchases depend on nature’s recovery probability exceeding the probability in the absence of a drug. Each company develops and produces a vaccine or drug if nature’s probability of successful development is high, if sufficiently many persons buy the vaccine or drug at a sales price that sufficiently exceeds the production price, and if the donor sponsors.
Conclusion
Accounting for all players’ interlinked decisions allowing 14 outcomes, which is challenging without a game theoretic analysis, the donor maximizes all persons’ expected utilities at the societal level to adjust how persons’ purchases and the companies’ development and production are subsidized.
Highlights
A game theoretic approach can help explain the production decisions of vaccine and drug companies, and the decisions of persons and a donor, impacted by Nature.
In 3 linked games, N persons choose risky behavior if its utility outweighs safe behavior.
Vaccine and drug companies develop vaccines and drugs sponsored by a donor if profitable, allowing 14 outcomes.
Keywords
Introduction
Background
Infectious diseases challenge humankind, with health, social, political, and economic consequences. As of January 16, 2021, 95 million were infected with COVID-19, and 2 million had died. 1 In 2019, 38 million people lived with HIV/AIDS. 2 Such diseases pose behavioral challenges for persons regarding attitudes toward risk; challenges for vaccine and drug companies regarding development, production, and sale; and challenges for societies represented, for example, by a donor that may subsidize. If too many persons choose risky behavior, if too few are vaccinated or if vaccines are unavailable, and if drugs are ineffective or unavailable, persons may die prematurely or recover with negative health effects, with societal impact.3–5
Literature
Nongame theoretic studies
Prevention
Fitzpatrick et al. 6 recommended the creation of a congressional cost-effectiveness committee to promote societal welfare and reveal underinvestment in public health compared with other sectors. If underinvestment is documented, donors are needed with the appropriate incentives. This article shows how a donor’s choices depend on the benefits to all persons of subsidization to induce vaccine and drug purchases, minus the subsidization costs, which may be adjusted to obtain optimal public health investment. Galárraga et al. 7 argued that prevention programs are insufficiently implemented, causing more than 7000 HIV infections per day, due to unconvincing evidence of cost-effectiveness and challenges in comparing programs. i Understanding the forces driving such a high number of infections relates to nature’s probability of disease contraction modeled in this article. This probability plays a role in the persons’ and donor’s expected utilities, which affect whether persons choose risky behavior, whether they buy vaccines and drugs, and whether the donor subsidizes, all of which in turn affect whether the companies develop, produce, and sell vaccines and drugs.
Prevention and treatment
To combat HIV/AIDS, Hogan et al.
15
recommended mass media campaigns, interventions for sex workers, and treatment of sexually transmitted infections when resources are scarce, and when resources are not scarce, they recommended prevention of mother-to-child transmission, voluntary counseling and testing, and school-based education.
iv
These recommendations are of paramount importance to inform persons, analyzed in this article, to understand
Treatment
Forsythe et al. 27 documented substantially improved health achievements and economic benefits and decreased costs during 20 y of ART. DiMasi et al. 28 estimated $2.6 billion for HIV drug research and development costs for the years 2017 to 2021. West and Schneider 29 estimated revenues for HIV/AIDS treatment for the years 2017 to 2021 for some African countries. Such costs are important inputs for the vaccine and drug companies’ expected profit functions in this article, affecting whether benefits outweigh costs and whether vaccines and drugs should be developed and produced. Kremer and Snyder,30,31 Thomas, 32 and Kremer and Glennerster 33 found that incentives for developing treatment drugs are stronger than incentives for developing prevention vaccines. Hence, more citizens may become sick, causing countries with a high disease prevalence to allocate more resources to treatment than to prevention. This finding is particularly relevant for the donor’s decision making in this article. In particular, the donor may subsidize development, production, and purchases (all 3 of which are analyzed in this article) of vaccines more than drugs, thus favoring prevention more than treatment.
Game theoretic studies
Game theoretic contributions are rare for this phenomenon. Hausken and Ncube 34 considered 5 outcomes in a game between persons and 1 pharmaceutical company (i.e., safe behavior, risky behavior and no disease contraction, disease contraction without drug availability, disease contraction with drug availability but without buying the drug, and disease contraction and buying the drug). They illustrated with HIV/AIDS data how a parametric donor affects drug development and drug purchases. Mamani et al. 35 recommended a contractual mechanism to remedy the inefficient allocation of influenza vaccines within multiple countries affected by the interdependent risk of infection across borders. They demonstrate decreased global costs of infection and fewer infections, especially with high cross-border transmission rates. Hausken and Ncube36,37 assessed policy makers choosing resource allocation between disease prevention and treatment, the international community choosing disease treatment funding, and nature choosing population fractions of disease contraction, sickness/death, and recovery. They illustrated free riding and found that more resource allocation for prevention causes less disease contraction but a higher death rate given disease contraction. This article contributes to this literature by modeling more players than in the above studies do (i.e., persons, vaccine companies, drug companies, a donor, and nature), accounting for more relationships between the players and better explaining how the games relate to the vaccine and drug companies’ research and development, production, bringing their products to the market, and sale.
Contribution
Health policy decisions are not usually analyzed game theoretically. This article incorporates the relevant players game theoretically. Game theory requires at least 2 players, with at least 1 player choosing at least 2 strategies and each player receiving a payoff given the combinations of strategies chosen by all players. Enabling each player’s strategy to depend mutually on all the players’ strategies allows for a different kind of analysis compared with when each player chooses a strategy or makes a decision unilaterally considering the environment as fixed or immutable.
The research question is to determine how each player weighs which benefits against which costs when choosing between which strategies. That question is particularly relevant for this phenomenon, where life and death depend on all the players’ interlinked decisions. More specifically, each person chooses between safe behavior, which may preserve life but may be more restrictive and be less exciting than risky behavior, which may cause disease. Each person also chooses whether or not to buy 1 vaccine if the disease is not contracted and 1 drug if the disease is contracted. That choice depends on the vaccine or drug being available at acceptable prices; which depends on donor subsidies; the utility of vaccination (which may have side effects or may not handle virus mutation); the utilities of recovery, death, and risky versus safe behavior; and nature’s probabilities of disease contraction and recovery with and without a drug.
Two vaccine companies and 2 drug (pharmaceutical) companies choose whether or not to develop and produce vaccines and drugs. These choices depend on the development costs affected by sponsor subsidies and nature’s probabilities of whether the development succeeds, on the production costs and sales prices, and on how many persons buy vaccines and drugs. A donor chooses subsidization of vaccine and drug development and vaccine and drug purchases for persons. The donor’s choices depend on all persons’ benefits of subsidization to induce vaccine and drug purchases, weighed against the subsidization costs. Nature chooses the disease contraction probability given risky behavior, the disease recovery probability without drugs, the disease recovery probabilities with each of the 2 drugs, and whether vaccines and drugs are developed successfully. This conceptualization is intended to better address the challenges in designing a strategic response to a pandemic or epidemic infectious disease.
This article contributes to the prevention literature by applying game theory to model whether and how vaccine companies develop vaccines and how persons buy vaccines, sponsored by a donor, and affected by nature choosing probabilities of disease contraction, recovery and death, and whether vaccines and drugs are developed successfully. This article contributes to the treatment literature by applying game theory to model whether and how drug companies develop drugs and how persons buy drugs, sponsored by a donor, and affected by nature choosing probabilities of disease contraction, recovery and death, and whether vaccines and drugs are developed successfully.
Article Organization
The “Methods” section presents the methods, design, and model. The “Results” section provides the results. The “Discussion” section discusses the results, with limitations, future research, and literature review. The last section concludes.
Methods
Overview
The subject of study is potential disease contraction depending on persons choosing risky or safe behavior, potential vaccine and drug developments by vaccine and drug companies, potential purchases of vaccines and drugs by persons, potential subsidization by a donor, and potential recovery or death (or decreased life quality) for persons contracting the disease.
The model applies to diseases satisfying 3 criteria. First, disease contraction depends on each person choosing risky or safe behavior (e.g., not wearing a mask, washing hands, and keeping distance against COVID-19 or not using a condom or avoiding multiple partners against HIV, hence excluding genetically predisposed and behaviorally independent diseases). Second, vaccine and drug companies are assumed that may develop vaccines and drugs. If vaccines or drugs cannot be produced for the given disease, the model simplifies to the special case when vaccines or drugs are unavailable. Third, we assume diseases enabling recovery in various degrees with or without drugs.
The model is illustrated and parameters estimated with early COVID-19 data on the BioNTech/Pfizer Comirnaty vaccine and the Moderna vaccine and the experimental drugs hydroxychloroquine and ivermectin. These 2 controversial off-the-shelf drugs were chosen because they currently have available prices. The model applies equally well for drugs involving, for example, new molecular entities developed over many years if prices and development costs can be estimated.
We show how the players strike balances when making their decisions in a game theoretic cost-benefit analysis. Each person may buy 1 drug given disease contraction and 1 vaccine otherwise. The vaccine and drug companies may or may not enable such purchases. The donor may or not sponsor. Nature may choose disease contraction, recovery and death, and whether vaccines and drugs are developed successfully, in multifarious ways.
Conceptualization
Figure 1 shows vaccine company
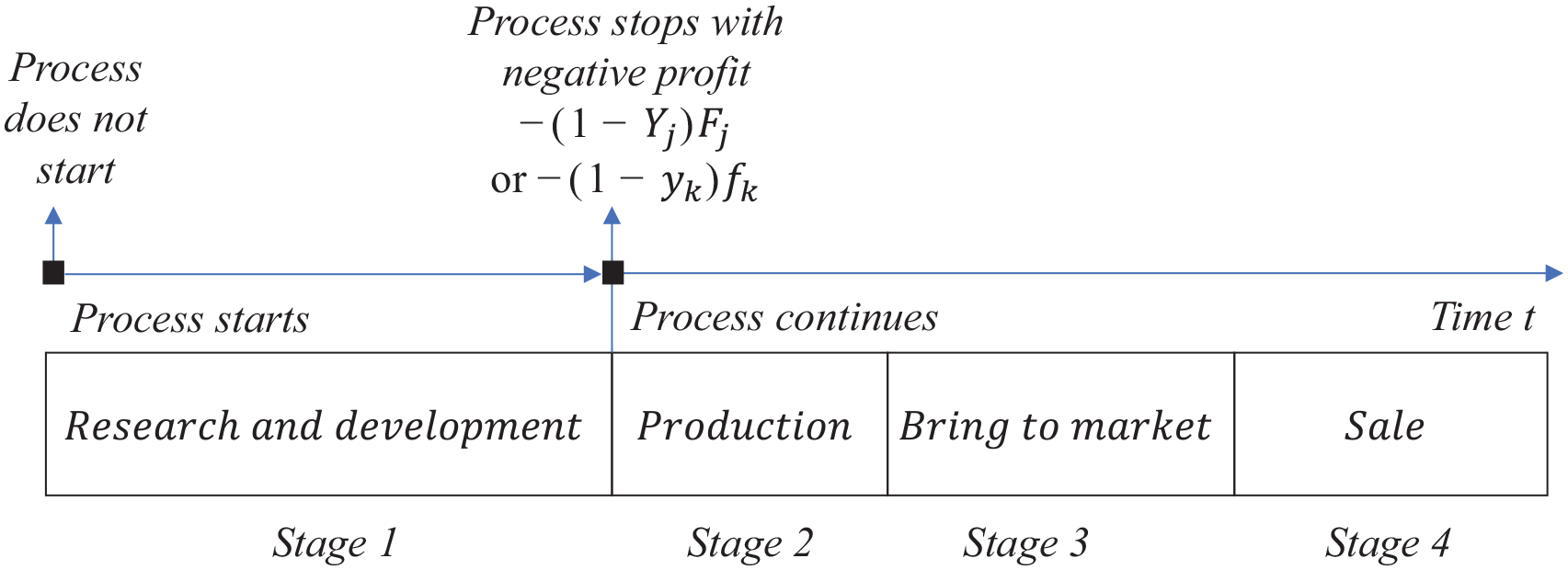
Vaccine company
The players, that is,
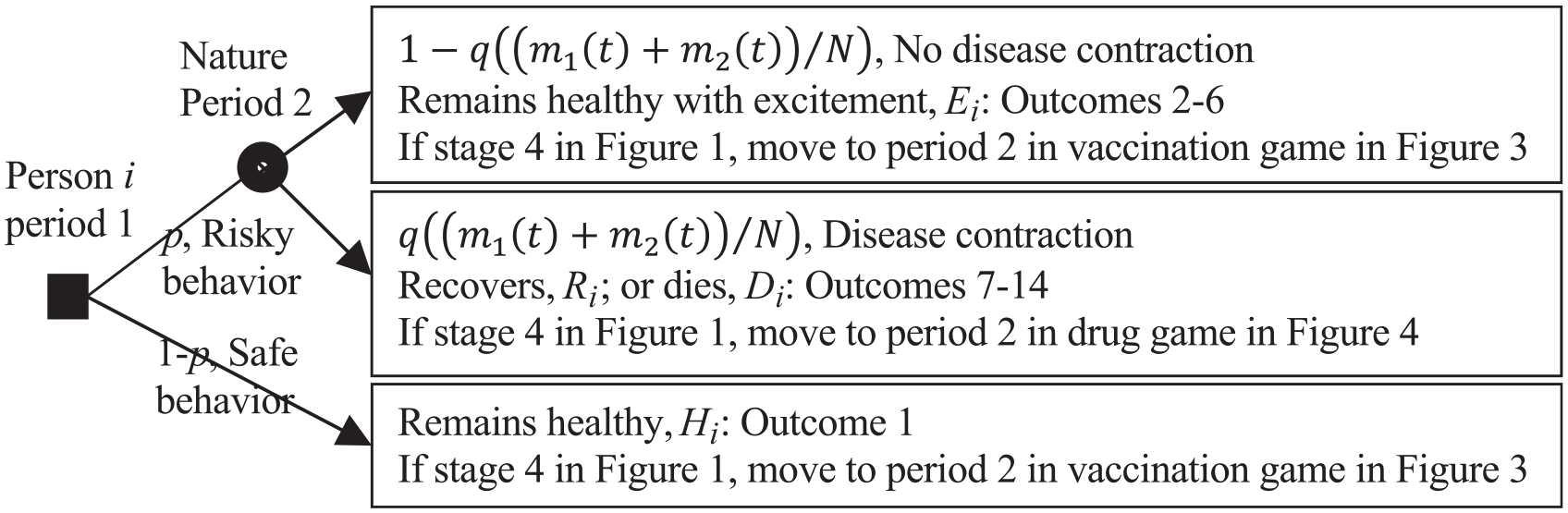
Two-period game between person i, i = 1, . . ., N, in period 1 and nature in period 2 on safe versus risky behavior and whether or not to contract the disease. The filled square decision node is for person i. The filled circle chance node is for nature.
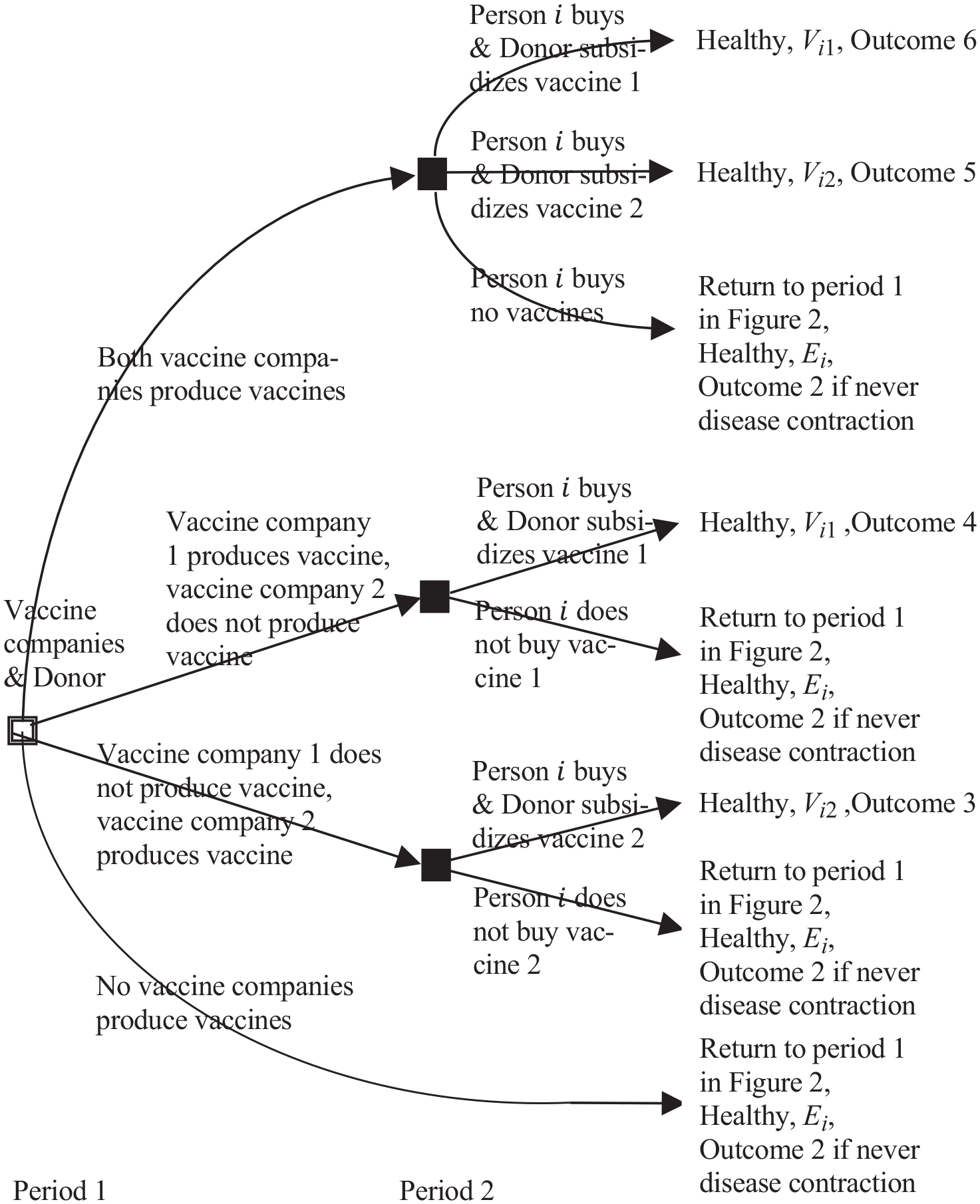
Two-period game between vaccine companies 1 and 2, the donor, and the part of N persons who have not contracted the disease. The framed square decision node (unfilled square with 2 demarcating lines along each side) is for the vaccine companies and the donor. The filled square decision nodes are for person i.
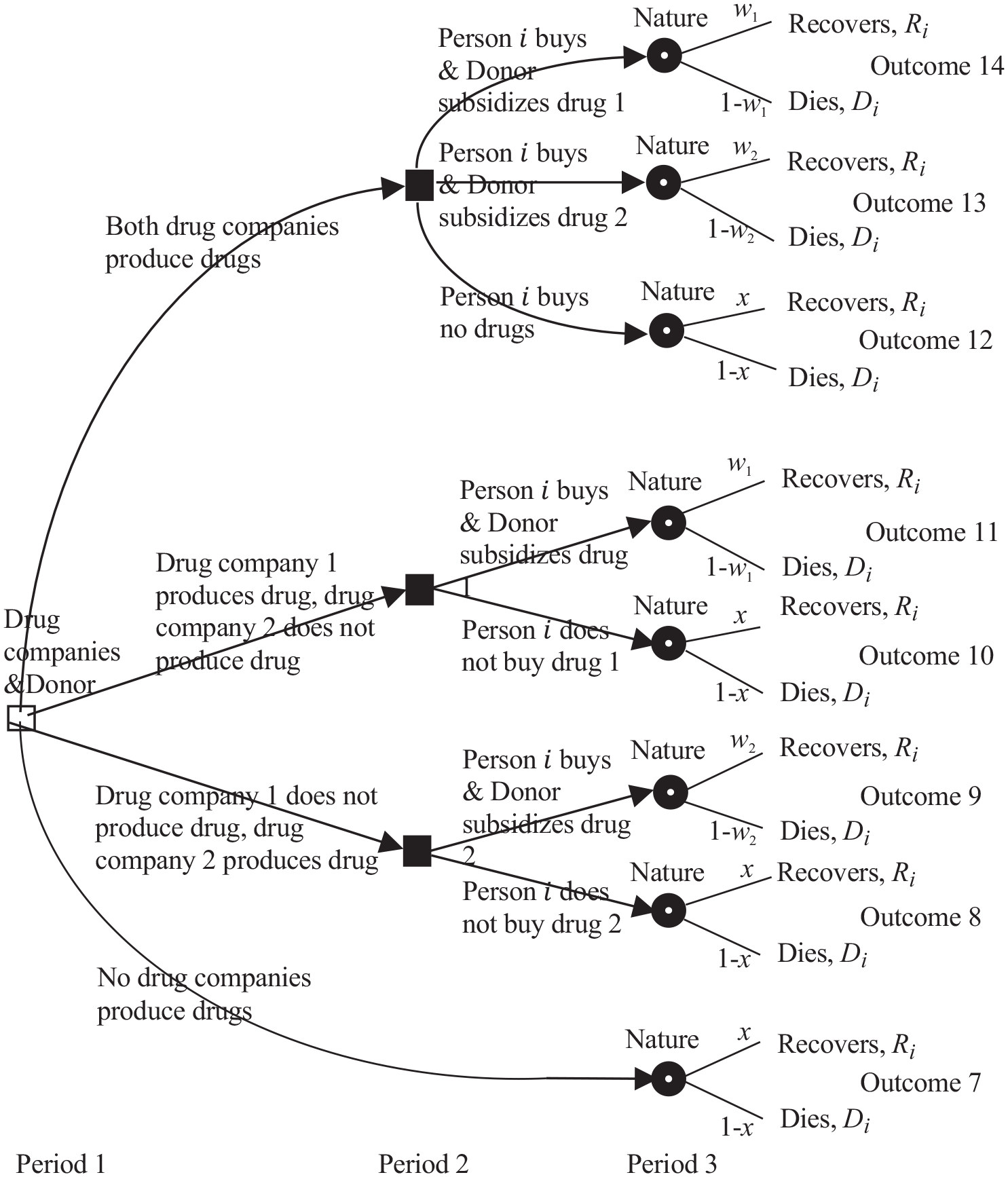
Three-period game between drug companies 1 and 2, the donor, the part of the persons N who have contracted the disease, and nature. The unfilled square decision node is for the drug companies and the donor. The filled square decision nodes are for person i. The filled circle chance i nodes are for nature.
Figure 3 shows the 2-period complete information game between vaccine companies 1 and 2, the donor,
iii
and the
Figure 4 shows the 3-period game between drug companies 1 and 2, the donor, the
Results
Overview
Person
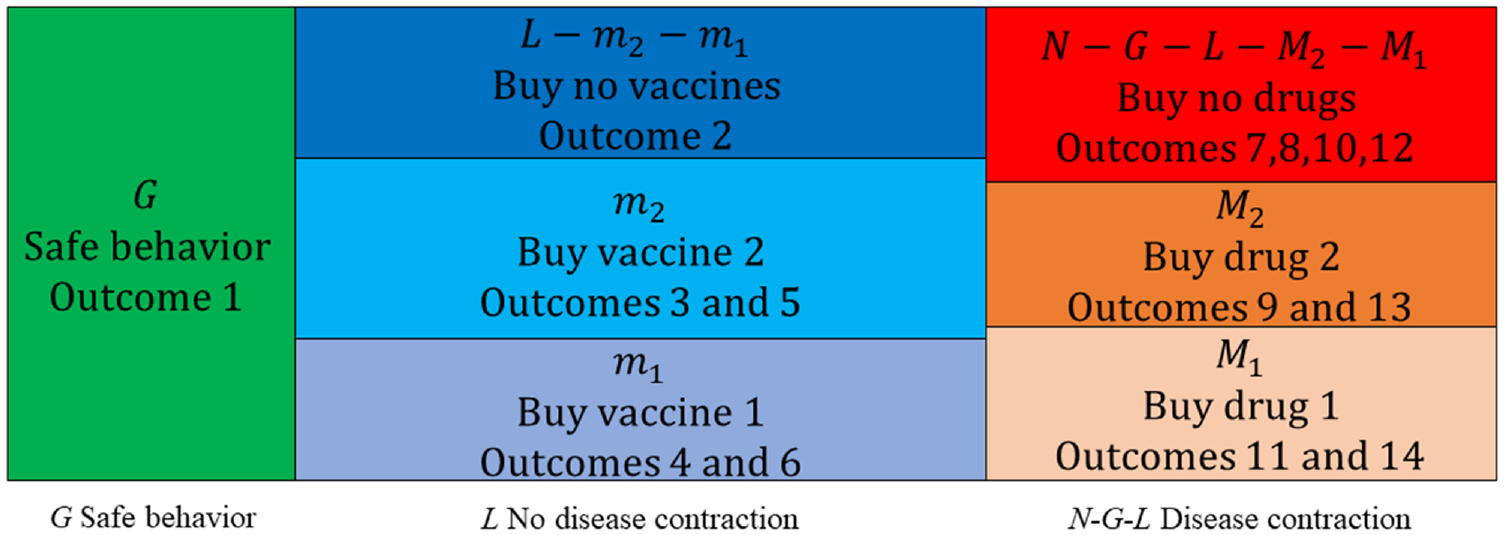
N persons dispersed across 7 groups.
Numerical Example Estimating the Parameters
Benchmark scenario with outcomes 5, 6, and 14
This section estimates the model’s parameters; the donor’s 8 strategic choices
At the time of writing, few drugs against COVID-19 exist. We thus consider the 2 experimental and controversial drugs hydroxychloroquine and ivermectin, which have been used by some, although not approved by sufficiently many authorities. Lansdowne states that design, development and drug approval can take 10–15 years, or less if the drug is believed to outcompete existing drugs or is the only available treatment.
41
One hundred tablets, each weighing 200 mg, of hydroxychloroquine cost $37.22.
42
Consuming 400 mg per week for 1 y
43
gives a drug 1 purchasing cost for 1 person of
Person
The donor’s 8 subsidy fractions are currently unknown. We estimate
To estimate nature’s 8 strategic choices, observe that 116 million people have contracted COVID-19 by March 5, 2021, 65.5 million have recovered, and 2.6 million have died,
47
out of the world’s 7.85 billion population.
48
Dividing 116 million by 7.85 billion gives the fraction 0.01478. If we hypothetically assume that 785 million will have contracted COVID-19 at some time in the future, we get the disease contraction probability
Applying the above parameter values gives the results in the 2 rightmost columns in Table 1 (Supplementary Appendix D). Using the game tree in Figures 2–4, outcome 1 is impossible and person
Inserting the parameter values into (9), person
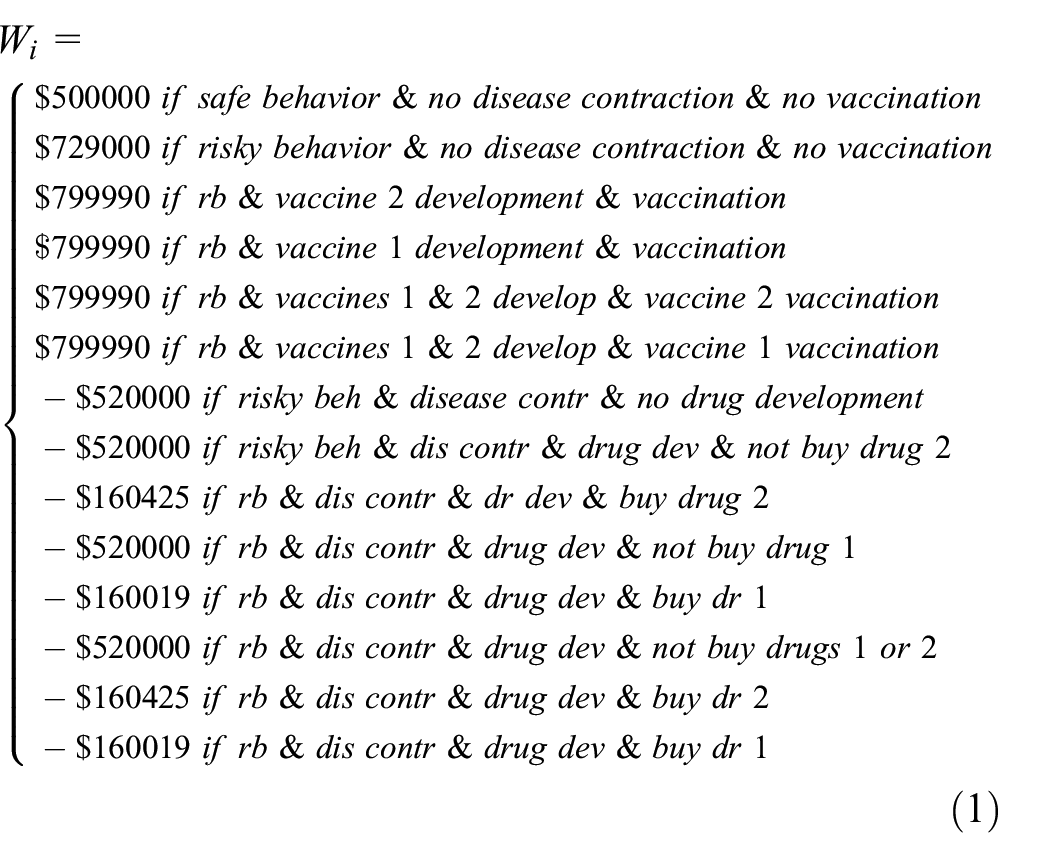
Equation (1) shows that outcome 14 (line 14) occurs if the disease is contracted, whereas outcome 5 or 6 (lines 5 or 6) occurs if the disease is not contracted, and person
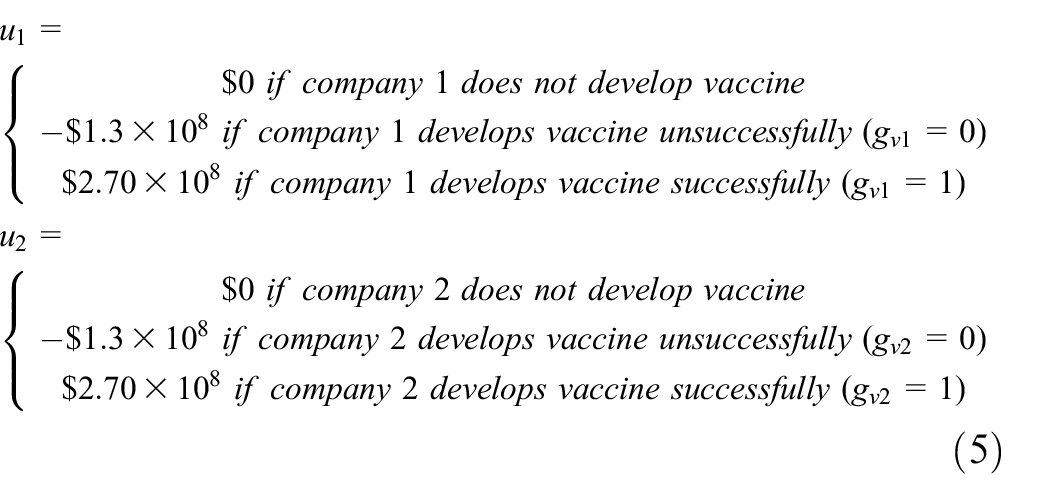
Inserting the parameter values into (7), vaccine company
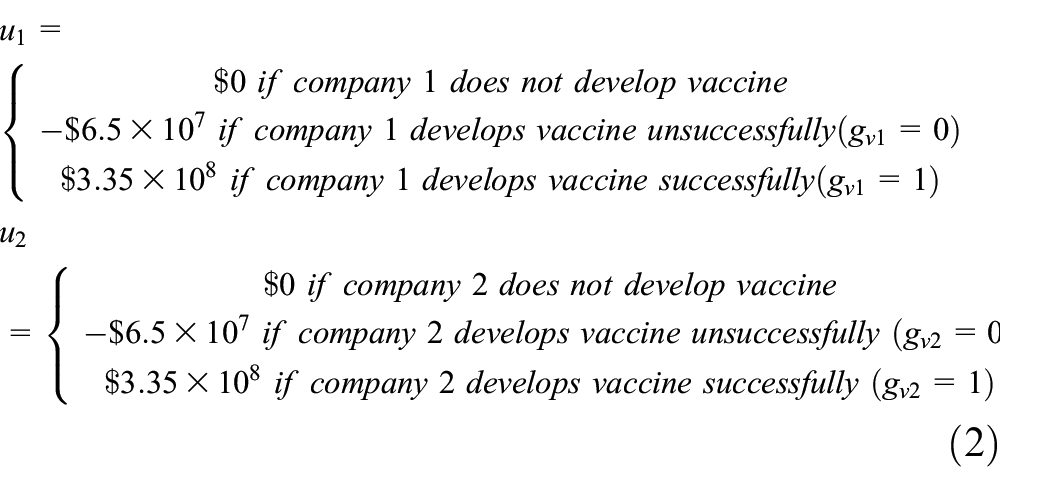
and hence both vaccine companies develop vaccines.
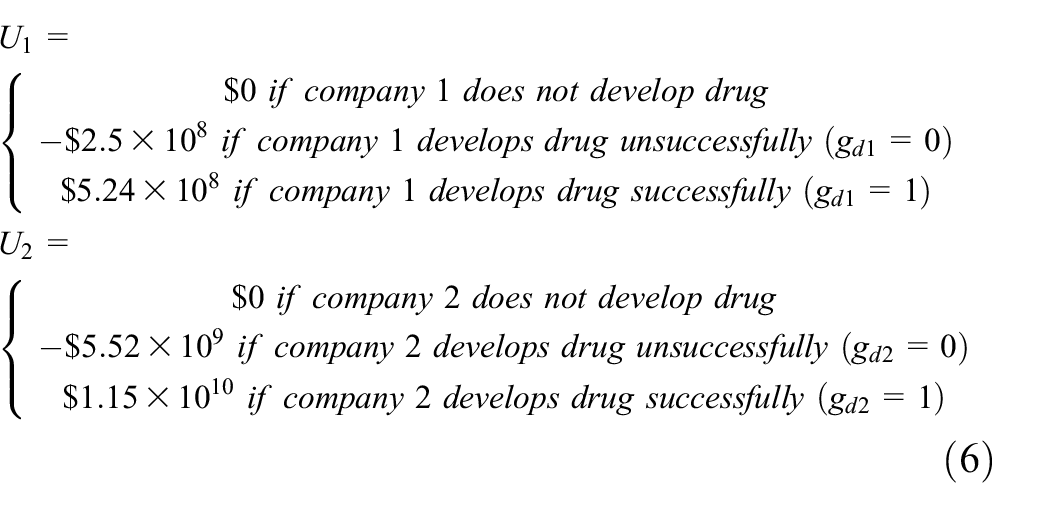
Inserting the parameter values into (8), drug company
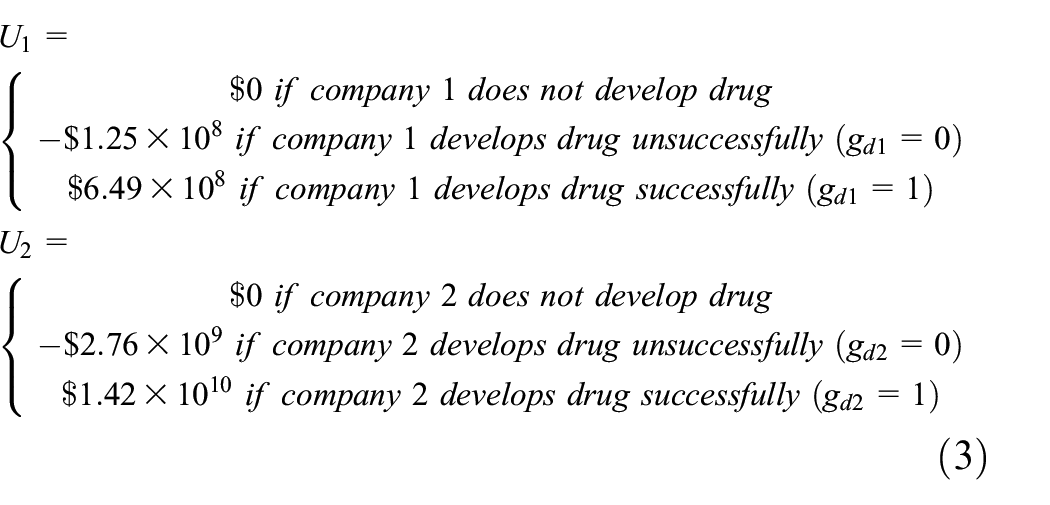
and hence both drug companies develop drugs.
The donor’s expected utility depends on a few additional parameters. We consider a country with
where we have illustrated the role of the donor’s 8 strategic choice variables
Alternative scenarios with outcomes 1–4, 7–13
Person
If person
If person
Vaccine company
.
If vaccine company
Drug company
If drug company j does not develop the vaccine successfully, that is, g dj = 0, its expected profit MjCj−(MjBj)Aj−(1−Yj) Fj in rows 2 and 3 in (8), that is, U1 = $6.49 × 108 in row 3 and U2 = $1.42 × 1010 in row 6 in (3), for our benchmark scenario does not occur. That expected profit has a positive term MjCj that decreases if the costs C1 = $38.71 and C2 = $849.74 of buying drugs 1 and 2 decreases or the number M j = 20 million persons buying j drug decreases (which depends on person i’s decision). Drug company j’s expected profit Uj also has a cost term (MjBj)Aj− (1 –Yj)Fj if gdj = 1, which increases if the drug development costs F1 = $0.25 billion and F2 = $5.52 billion increase or if the drug j production costs M1B1 = $9.68 × 20 × 106 and M2B2 = $212.44 × 20 × 106 for the Mj = 20 million persons increase. If drug 1 is free, that is, C1 = 0, drug company 1’s expected profit decreases to U1 = −$1.251014 × 107, drug 1 will not be produced. If the drug 1 development cost F1 = $0.25 billion increases to F1 = $1.548372 billion, drug company 1’s expected profit decreases to U1 = $0, causing it to be indifferent between producing and not producing the drug. If rows 3 and 6 in (3) do not occur, so that no drugs are produced, outcomes 8–14 are impossible. Person i then has no choice causing outcome 7 with expected utility Wi = (1 −x)D i +xR i = −$520,000. For person i to actively choose outcome 7, if it had a choice, its utility Ri = $0.2 million when recovering from disease and its disease recovery probability x = 0.9 without a drug would have to be high, and its utility Di = −$7 million of death would have to be less negative.
The donor
If the donor does not choose its 8 subsidy fractions
With this change, the vaccines and drugs are still produced, but the companies’ profit margins are lower and may become negative if other parameter values change adversely.
Discussion, Limitations, Future Research, and Literature Review
Discussion
The model illustrates the strategic interaction between
The parameter estimation in the section “Numerical example estimating the parameters” in the Results section illustrates how each of these 14 outcomes can be realized. The article shows how each person chooses risky or safe behavior dependent on the expected benefits and costs of the various outcomes and nature’s choice of the probability of disease contraction. That probability is of particular interest related to the finding of Galárraga et al. 7 of 7000 HIV infections per day in their study.
We illustrate a benchmark scenario in which vaccines and drugs are produced and person
The parameters and the players’ strategies change with changing markets, prices, diseases, persons’ preferences, demography, modes of interaction, technology, and so forth. In the benchmark scenario, the 4 companies produce vaccines and drugs. The companies’ choices also depend on weighing the benefits against the costs, which can be decreased as recommended by Granich et al.,
25
, Bärnighausen et al.,
26
Forsythe et al.,
27
and others, as discussed in the section “Treatment” in the Introduction. In the alternative scenarios, as quantified in the examples, vaccines and drugs are not developed and produced if the costs are too high, affected by whether the donor subsidizes, if the probability of successful development is too low, and if too few persons buy the vaccines or drugs at too low costs. As the persons’ and companies’ strategies change, the previous section also shows how the donor’s weighing of the benefits to the
Societal changes in preferences, beliefs, demography, and modes of interaction may change the persons’ expected utilities of the various outcomes. More effective and cheaper drugs, produced and distributed more effectively, may affect the outcomes. Such factors affect which of the 14 outcomes occur. Understanding the impact of changes may enable players to choose better strategies and enable policy makers and others, not modeled in this article, to make good decisions.
The prices of vaccines and drugs are affected by many factors. Large volumes generally cause price reduction. 49 COVID-19 is too recent to experience established price discovery for vaccines and drugs. Some drug manufacturers of antiretroviral drugs for HIV/AIDS, such as Merck, GlaxoSmithKline, and Bristol Myers Squibb, apply price tiers depending on the countries’ socioeconomic status. Some apply the World Bank definition of low, lower-middle, upper-middle, and high-income countries. 50 Other companies apply their own classification. 51 Prices are also influenced by procurement processes including third-party negotiations. For example, the Clinton Health Access Initiative 52 negotiates procurement prices on behalf of its member countries with mainly generic manufacturers.
The article assumes that person
No vaccine exists against HIV/AIDS, which emerged in 1983–1984, because of HIV’s high strain diversity. The HIV variability within one individual exceeds the worldwide variability in the influenza virus during one season. HIV’s high virus replication prevents recognition by antibodies.
53
Five unsuccessful phase 3 vaccine efficacy trials have been performed against HIV, each costing more than US$100 million. Game theoretically, this means that the vaccine
Limitations
Limitations of the article are related to different market conditions, technology, and preferences of the players over time. Vaccine and drug companies develop increased competence over time, while diseases change due to virus mutation. How donors sponsor and how nature chooses disease contraction, recovery, death, and whether vaccines and drugs are developed successfully also have impact. Some suggestions are made below for how future research may address such limitations.
Future Research
The article assumes rational agents and conventional expected utility theory. Future research may verify the results assuming boundedly rational agents 54 and alternatives, such as prospect theory, in which the expected utility is concave for gains, convex for losses, assigns excessive weight to low probability events, and insufficient weight to low-probability events. 55
Future research may assess how a country’s economy, productivity, economic growth, and societal indicators such as income and health are affected by the factors analyzed in this article. Research may distinguish between persons according to age, sex, occupation, ethnicity, race, and so forth and model probability distributions for types of persons according to utilities for risky behavior, safe behavior, recovery from disease, and death.
Research may model different kinds of competition between multiple vaccine and drug companies; competition between multiple donors as strategic players; regulation by multiple regulatory agencies; model more players such as doctors, hospitals, regulators, and politicians; and account for more choices by nature, which may potentially be endogenized. For example, the disease contraction probability for infectious diseases may depend on how many persons have previously contracted the disease in each person’s various networks of family, work, leisure activities, and so on. The disease recovery probability with and without various vaccines and drugs may be endogenized by modeling the biological virus evolution processes.21,56
Research may model how people choose different kinds and degrees of risky and safe behavior before, during, and after various vaccines and drugs are produced and available. Such behaviors can be expected to depend on persons’ perceptions of the qualities and prices of vaccines and drugs and how vaccines and drugs are adjusted to the changing characteristics of various diseases. Future research should collect empirical data on a variety of infectious diseases, assess empirical support of the model in this article and other models, and develop further models.
Conclusion
Three linked games for an infectious disease such as COVID-19 or HIV/AIDS are developed between
The article illustrates how the players (i.e., persons, vaccine and drug companies, the donor, and nature) strike balances in a game-theoretic cost-benefit analysis that impacts which of the 14 outcomes arise. Illustrating how such balances are struck may improve society’s ability to handle infectious diseases and has managerial implications for running vaccine and drug companies, determining how a donor should subsidize, and how persons should manage their own health. More specifically, each player has a benefit and a cost. Each person incurs a cost of buying a vaccine or drug, which may be sponsored by a donor, weighted against probabilistic utilities associated with risky or safe behavior, vaccination, recovery, and death, affecting the person’s strategy. Relative to a benchmark scenario in which a person buys a vaccine or drug, we show how changing conditions may affect the person not to buy a vaccine or drug.
Each vaccine and drug company incurs a cost of developing and producing a vaccine or drug, successfully or unsuccessfully, potentially sponsored by a donor. The production cost depends on how many persons buy the vaccine or drug, which illustrates the linkage between the players. Each vaccine and drug company’s benefit is the price of the vaccine or drug, which also depends on how many persons buy it. We show how changing conditions may induce vaccine and drug companies not to produce vaccines and drugs. The donor’s expected utility equals the sum of the persons’ benefits across the 14 outcomes minus the cost of subsidizing the development and purchase of vaccines and drugs. The donor subsidizes based on weighing the benefit against the cost.
As a pandemic evolves, nature’s probabilities of disease contraction and recovery with and without a drug changes. This affects each person’s strategies of safe versus risky behavior and whether to buy a vaccine or drug. Each vaccine and drug company faces uncertainties as to whether a vaccine or drug can be successfully developed and produced, at what cost, how many persons will buy it, at which price, and how the sponsor may subsidize. The strong linkages between the players affect their strategies. Various scenarios are presented for how the players choose strategies associated with the 14 outcomes. Policy makers may assess the players’ strategies when designing broader societal strategies, potentially inducing players to choose the preferable outcomes among the 14 outcomes.
Future research may generalize the model to include various strategies for doctors, hospitals, advisors, insurance companies, and so on that also play a role in the health and political system. The persons’ strategies may be generalized to a continuum from extremely risky to extremely safe. More than 2 vaccine companies and 2 drug companies may be considered, with various forms of competition (e.g., on price and quality) between them.
Supplemental Material
sj-docx-1-mdm-10.1177_0272989X211053563 – Supplemental material for A Game Theoretic Analysis of Competition Between Vaccine and Drug Companies during Disease Contraction and Recovery
Supplemental material, sj-docx-1-mdm-10.1177_0272989X211053563 for A Game Theoretic Analysis of Competition Between Vaccine and Drug Companies during Disease Contraction and Recovery by Kjell Hausken and Mthuli Ncube in Medical Decision Making
Supplemental Material
sj-docx-2-mdm-10.1177_0272989X211053563 – Supplemental material for A Game Theoretic Analysis of Competition Between Vaccine and Drug Companies during Disease Contraction and Recovery
Supplemental material, sj-docx-2-mdm-10.1177_0272989X211053563 for A Game Theoretic Analysis of Competition Between Vaccine and Drug Companies during Disease Contraction and Recovery by Kjell Hausken and Mthuli Ncube in Medical Decision Making
Supplemental Material
sj-docx-3-mdm-10.1177_0272989X211053563 – Supplemental material for A Game Theoretic Analysis of Competition Between Vaccine and Drug Companies during Disease Contraction and Recovery
Supplemental material, sj-docx-3-mdm-10.1177_0272989X211053563 for A Game Theoretic Analysis of Competition Between Vaccine and Drug Companies during Disease Contraction and Recovery by Kjell Hausken and Mthuli Ncube in Medical Decision Making
Supplemental Material
sj-docx-4-mdm-10.1177_0272989X211053563 – Supplemental material for A Game Theoretic Analysis of Competition Between Vaccine and Drug Companies during Disease Contraction and Recovery
Supplemental material, sj-docx-4-mdm-10.1177_0272989X211053563 for A Game Theoretic Analysis of Competition Between Vaccine and Drug Companies during Disease Contraction and Recovery by Kjell Hausken and Mthuli Ncube in Medical Decision Making
Footnotes
Acknowledgements
We thank the 3 referees of this journal, an associate editor, and the editor-in-chief for useful comments.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.
Journal of Economic Literature classification numbers: C72, D81, H51, I11, N3
Supplemental Material
Data Availability
All data generated or analyzed during this study is included in this published article.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.