
Abstract
Introduction:
Fear of COVID-19 makes tuberculosis (TB) patients seek health care after complications of the case. This can be the reason for serious illness, increased length of infectiousness, poor treatment outcomes, and economic crisis for families and the health system. Despite this, no study has been conducted in Ethiopia and in other African countries with the factor “fear of COVID-19.” Identified preventable factor and other covariates are used to reduce the healthcare-seeking delay.
Objective:
This study assessed the association of fear of COVID-19 with healthcare-seeking delay among TB patients in Ilu Ababor Zone health facilities, south-western Ethiopia.
Methods and materials:
A health institution-based cross-sectional study was conducted among TB patients from October 15, 2020, to March 1, 2021. Using a systematic sampling method, 403 TB patients were selected for face-to-face interviews. The association of fear of getting COVID-19 with healthcare-seeking delay was assessed by a chi-square test. Variables with a p-value <0.25 in the bi-variable binary logistic regression were entered into the multivariable binary logistic regression model. The level of statistical significance in multivariable binary logistic regression was declared at a p-value <0.05.
Result:
In this study, the proportion of patient healthcare-seeking delay was 46.7%. Chi-square test of the association of fear of COVID-19 with healthcare-seeking delay among TB patients showed a significant association (p-value = 0.042). After controlling for covariates, patients living in rural area (adjusted odds ratio (AOR) = 2.437, 95% confidence interval (CI): 1.385–4.286), patients with poor knowledge (AOR = 3.300, 95% CI: 1.792–6.078), earning monthly income <200 Ethiopian birr (ETB) (AOR = 3.912 95% CI: 1.951–7.841), traveling greater than 30 min (AOR = 2.127, 95% CI: 1.301–3.476), and fear of COVID-19 pandemic (AOR = 3.124, 95% CI: 1.029–9.479) were significantly associated with patient healthcare-seeking delay.
Conclusion:
The study found that healthcare-seeking delay among TB patients was substantial. Patient healthcare-seeking delay was significantly associated with fear of COVID-19.
Introduction
Tuberculosis (TB) is a chronic contagious disease caused by Mycobacterium tuberculosis complex and other related species. 1 Early diagnosis of TB and treatment effects are the keystones of global TB control programs. 2 Despite the exhaustive strategies of the World Health Organization for controlling this disease, millions of people are still being infected annually. 3 Therefore, individuals who had a cough and/or other clinical manifestations should seek health care as early as possible.1,4,5 Strategies of TB control and prevention are to identify and treat new incident cases as early as possible, but the strategy is hard to meet because patients usually go to the health facility (HF) late. 6
Healthcare-seeking delay refers to when patients wait for a long period of days after the onset of TB symptom/s to seek healthcare facilities, 7 greater than the median time from the onset of symptom until visiting the healthcare facility (HCF) for the first time.7–10
TB remains a major public health problem in Ethiopia and this could be partly due to patient healthcare-seeking delay.11,12 A result of the first national TB prevalence survey conducted in 2011 revealed that smear-positive pulmonary TB (SPTB) prevalence was 108/100,000; of which 55% were not detected before the survey. 13 Moreover, according to a recent global report, about 32% of TB cases in Ethiopia mean that approximately 54,295 TB cases from an estimated 172,000 new cases may not have been diagnosed and properly treated and left in the population. 3
Late TB case identification results in serious illness, increased length of infectiousness, poor treatment outcomes, and economic crisis.14–24 Therefore, the crisis is very high from such preventable and treatable diseases because of delayed healthcare-seeking.3,25 Common factors contributing to patient healthcare-seeking delay include family size, occupation, income of family, stigma, knowledge about TB, and distance to a HF.14,26–30
Cognizant of this, the Government of Ethiopia has given due attention to the control of TB and included the prevention and control of TB among the priority health programs in the country’s health sectors transformation plan. 31 In Ethiopia, TB case findings were mainly relying on passive and community-based enhanced TB case finding as the main strategies.31,32
Although the problem is still a big issue in the country, no study has been conducted in Ethiopia and in other countries of Africa with the factor “fears of COVID-19.” Therefore, this study aimed to assess the association of fear of COVID-19 with healthcare-seeking delay among TB patients in Ilubabor zone HFs, south-west Ethiopia.
Methods and materials
Study design and population
The study was conducted in Ilubabor Zone HFs, south-west Ethiopia. A HF-based cross-sectional study was conducted from October 15, 2020, to March 1, 2021. All TB-diagnosed patients, both pulmonary and extrapulmonary cases, who were registered and receiving treatment in Ilubabor zone HFs, south-west Ethiopia were the source population. Diagnosed TB patients who were registered and receiving DOTS treatment at the 10 selected HFs during the study period were the study population in this study.
Inclusion criteria: All TB patients, both pulmonary and extrapulmonary cases, registered in the master registration book and those TB patients who transferred in for a continuation of treatment to the selected HFs were included.
Exclusion criteria: TB patients who were critically ill and unable to communicate were excluded from the study.
Sample population
The sample size for this study was calculated from a previous related study by using the single population proportion formula. 33 The final sample size for this study was 403. The study was carried out in Ilubabor zone HFs that provide DOTS services. Ten HFs were randomly selected among the study area HFs. A systematic sampling technique using sampling interval = 2 was used to recruit the predetermined sample size (403) (Figure 1).

Schematic representation of sampling procedure on assessments of the association of fear of COVID-19 with healthcare-seeking delay among TB patients in Ilubabor zone health facilities, south-west Ethiopia, 2020.
Dependent variables: Healthcare-seeking delay.
Independent variable: Fear of COVID-19.
Covariates
Sociodemographic: Sex, age, residence, marital status, literacy, family size, occupation, income, religion, and travel time to the HF.
Care-seeking practices: First action to illness, visited HCF, several visits to HCF, source of referral/advice to seek HCF.
Clinical factors: Type of HCF where TB is diagnosed, presenting symptoms, HIV sero-status, the severity of disease/patient functional status, types of diagnostic test used, types of TB, and history of TB contact.
Knowledge, attitude, and stigma: Knowledge of TB disease, perceived TB stigma.
Behavioral characteristics: Smoking, drinking alcohol.
Measures of healthcare-seeking delay
Healthcare-seeking delay is the time interval from the onset of symptoms of TB until the first visit to any formal HCF at a time greater than the median days as a cutoff point.3,7–10
The onset of TB symptom: The time at which the first symptom (i.e. cough and other constitutional symptoms like fever, weakness, and weight loss or chest pain) of the illness for which a patient’s healthcare-seeking began. 34
Fear of COVID-19: In this study, fear of COVID-19 indicated the fear of COVID-19 during HF care-seeking. The variable was collected using the Question “Did you fear COVID-19, for HF care-seeking when you were manifesting TB symptoms?” The options were “yes, no, I don’t know COVID-19.”
Functional status
Working: Able to perform usual work in or out of the house.
Ambulatory: Able to perform activities of daily living.
Bedridden: Not able to perform activities of daily living.
Data collection tool and data collection procedure
An adapted structured questionnaire was used to gather the data.8,14 Besides, a data abstraction checklist was prepared to draw clinical profiles of the patients from the TB register. The questionnaire was initially prepared in English and then translated to Afan Oromo language, and was translated back to English to check for any inconsistencies. Data was collected by 10 nurse professionals who can speak the Afan Oromo language and 5 supervisors. Data were collected after obtaining informed written consent from the study participants.
The collected information from the TB registry and the patients were reported to the supervisors every 2–3 days, to enable taking immediate action in case inconsistencies and problems happen with the reported data. Reports were regularly cross-checked with the main TB registry found in the respective HFs and finally, the reviewed questionnaires were returned to the investigators.
Data quality assurance
To assure the data quality, a data collection tool was prepared after reviewing relevant literature and similar studies. The training was given to both data collectors and supervisors on a briefing on the general objective of the study, and a discussion of the contents of the questionnaire by the investigators. Pretesting of the questionnaire was carried out on the 5% of sample size in one of the health centers found outside of the study facilities before actual data collection. A necessary correction was made based on the pretested result to avoid any confusion and for better completion of the questions. The overall activities of data collection were also supervised and coordinated by the investigators. The completeness of the data was checked by data collectors during data collection and immediately after data collection by the supervisors and the investigators.
Statistical analysis
The collected data was entered into Epi-data version 4.4.2.1, exported to SPSS software version 25, and checked for inconsistencies and missing values by running frequencies and other data explorations. Frequency distributions mean/median and interquartile ranges were computed.
Beyond descriptive statistics, an association between the dependent variable and the independent variable (fear of COVID-19) was assessed by the chi-square test. Bi-variable binary logistic regression analysis was performed on each variable and a respective crude odds ratio was calculated. Independent variable (fear of COVID-19) and other covariates with marginal associations (p < 0.25) in the bi-variable binary logistic regression analysis were entered into a multivariable binary logistic regression analysis to detect factors contributed to healthcare-seeking delay among TB patients in the study area. A p-value of ⩽0.05 was declared as statistically significant. Multicollinearity was checked using a collinearity matrix. The final model was fitted with Hosmer and Lemeshow (p-value = 0.55). The significant association of the independent variables and covariates with the dependent variable was reported using a 95% confidence interval and a respective adjusted odds ratio.
Ethical consideration
Ethical approval was obtained from the research and community service coordination office (RCS) of Mettu University College of Health Sciences with Ref/RCS/114/13. Following the approval, an official letter of co-operation was written to concerned bodies. Permission was also obtained from the zonal Health Bureau. Respondents were informed about the objective and purpose of the study and written informed consent was obtained from each respondent. Clear information was given to inform respondents about the purpose and procedure of the study, the importance of their participation, the right to withdraw at any time if they want, and about privacy and confidentiality of the information maintained throughout the study by maintaining anonymity, keeping their privacy by interviewing them in a separate room during the interview and locking records.
Results
Sociodemographic characteristics
In this study, 403 TB patients were involved and answered for the questionnaire making a response rate 100%. Most of the participants 207 (51.4%) were in the age category of 25–44 years. The number of male participants was 243 (60.3%). The majority of the participants were married—288 (71.5%). Among the participants, 189 (46.9%) were living in rural areas while the rest were in urban residences (Table 1).
Sociodemographic characteristics of TB patients in Ilubabor in HFs, 2020.
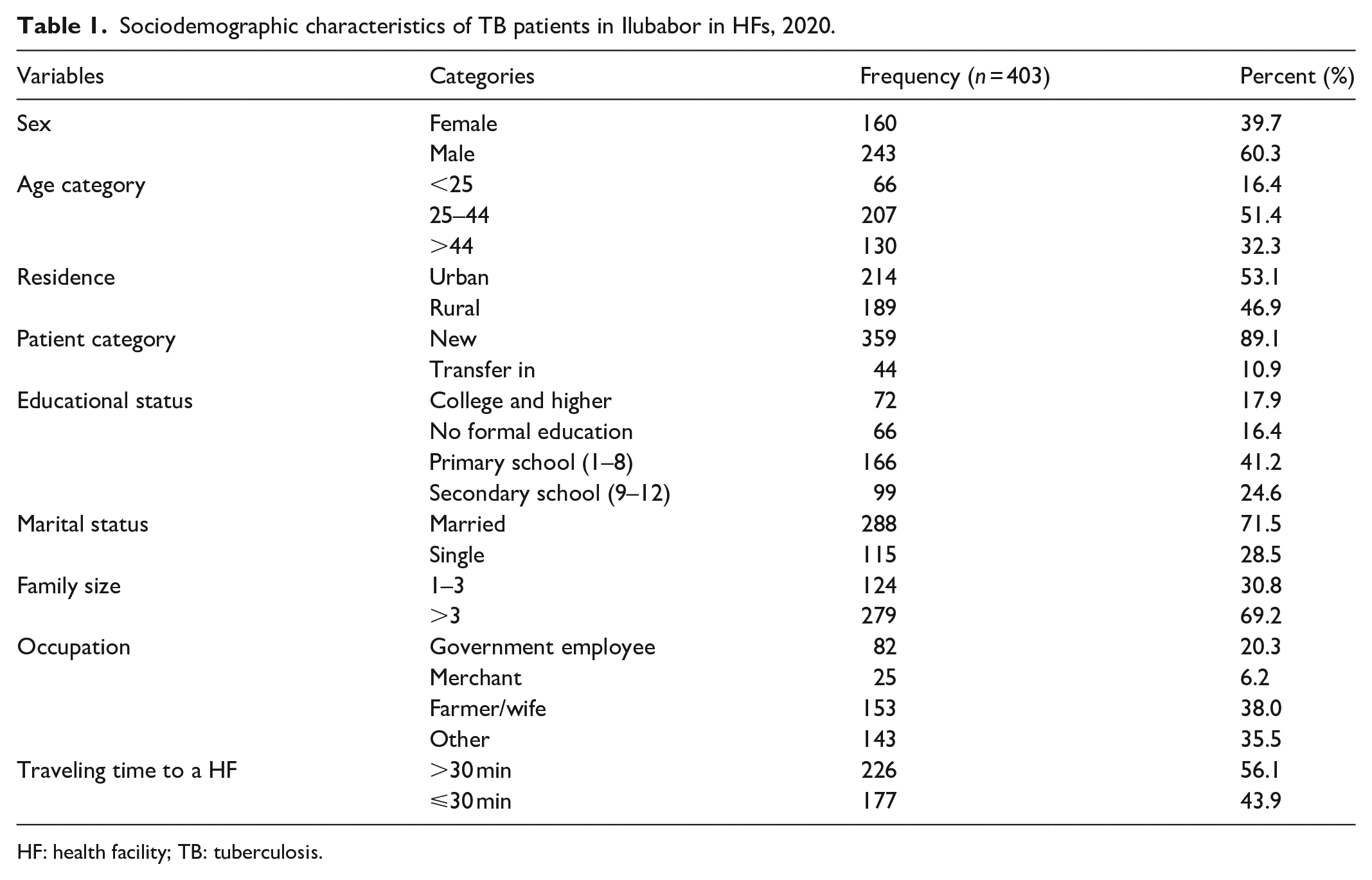
HF: health facility; TB: tuberculosis.
Healthcare-seeking practices
Among the participants, 195 (48.4%) patients consulted informal care providers for their illnesses. The majority of the participant who visited health centers for the first time for their illness were 269 (66.7%); 289 (71.7%) of the study participants had a low stigma toward TB illness (Table 2).
Healthcare-seeking practices of TB patients in Ilubabor in HFs, 2020.

HCF: health-care facility; HF: health facility; TB: tuberculosis.
Clinical characteristics
Most of the participants 292 (72.5%) were presented to HFs with coughs. The majority of the study participants 244 (60.5%) were ambulatory during a presentation to HFs. Among the patients who come to HF, 275 (68.2%) of them were SPTB (Table 3; Figures 2, 3, 4, and 5).
Clinical characteristics and substance use among TB patients in Ilubabor zone HFs, 2021.

HF: health facility; TB: tuberculosis; EPTB: extrapulmonary tuberculosis; SNPTB: sputum-negative pulmonary tuberculosis; SPPTB: sputum-positive pulmonary tuberculosis.

Knowledge status of the patient toward TB in Ilubabor zone HFs, 2021.

The attitude of TB patients in Ilubabor zone HFs, 2021.

Fear of COVID-19 status of the TB patients in Ilubabor zone HFs, 2020.
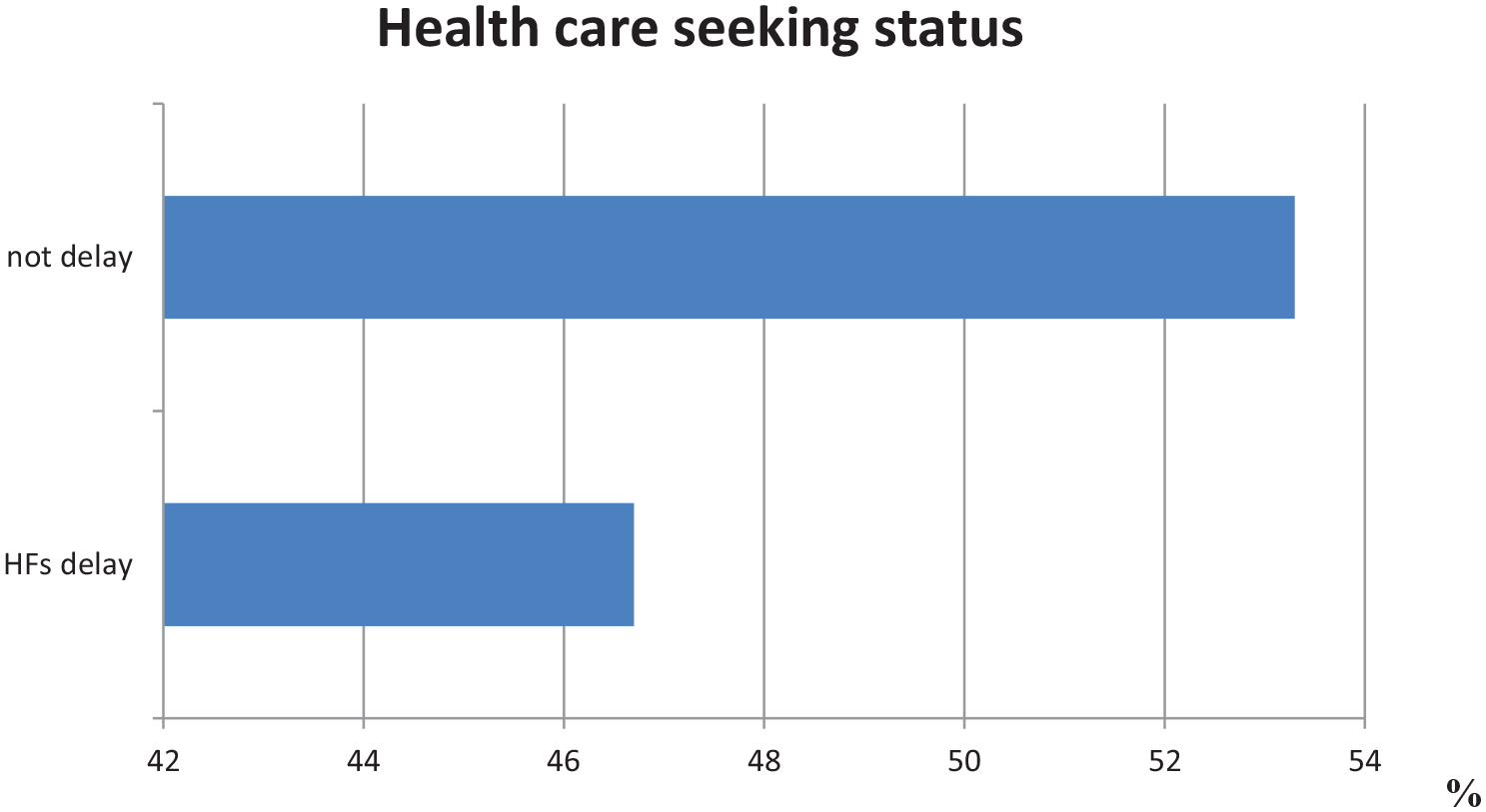
Health facility seeking status among TB patients in Ilubabor Zone, 2021.
Knowledge status of TB patients
The attitude of patients toward TB in Ilubabor zone HFs
Frequency
Fear of COVID-19 of TB patients and its association with healthcare-seeking delay
HF care-seeking status
Factors associated with healthcare-seeking delay among TB patients
Bi-variable logistic regression was conducted to identify candidate variables with a p-value < 0.25. The identified variables: sex, place of residence, educational status, suspecting illness to be TB, alcohol drinking status, manifested TB symptom, knowledge, monthly income, first action for consultation, distance from HFs, action enforced to seek HF, and fear of COVID-19 were entered to multivariable binary logistic regression to identify the possible significantly associated factors with healthcare-seeking delay among TB patients.
In multivariable logistic regression place of rural residence, poor knowledge, average monthly income <2001 Ethiopian birr (ETB), distance traveled to HF >30 min, and fear of COVID-19 were significantly associated factors with healthcare-seeking delay among TB patients in Ilubabor HFs (Table 4).
Bi-variable and multivariable binary logistic regressions to identify factors associated with healthcare-seeking delay among TB patients in Ilubabor zone HFs, 2021.

AOR: adjusted odds ratio; COR: crude odds ratio; HF: health facility; TB: tuberculosis; CI; confidence interval.
Discussion
This study was conducted to assess the association between fear of COVID-19 and healthcare-seeking delay among TB patients in Ilubabor zone HFs, south-west Ethiopia. The proportion of TB patient HF care-seeking delay with a 95% confidence interval was 46.7% (41.7–51.7%). This study was in line with the study conducted in Addis Ababa 42.1% 16 and Montenegro 49%. 35 The proportion of patient healthcare-seeking delay in this study was lower than the study conducted in Ghana 60.3% 36 and Kenya 87%. 37 This might be due to community-based awareness being delivered by Ethiopian health extension workers toward early HF seeking as it is one of the responsibilities of Ethiopian health extension workers. The finding of this study was higher than the study conducted in Australia 41.3%, 38 France 27%, 39 Dessie 41.1, 15 and Asella 36.7%. 40 This might be due to fear of COVID-19 and the lifestyle of the population toward HF-seeking behavior as well as the distance from HF, monthly income of the population, and residency area matters the habit of seeking HF.
In this study, patients who were living in rural areas were twofold times more likely to delay with healthcare-seeking. This study is in line with the study conducted in Angola and Bale. 34 The possible explanation might be the distance from the HF and the accessibility of the service. Patients who were earning <2001 ETB average monthly income were about fourfold times to delay healthcare-seeking than those who earned >4000 ETB. This study was supported by studies conducted in Addis Ababa, Hadiya, and India.16,17,41 The possible explanation regarding this might be transportation fees as well as charges for the diagnostic procedure until the case is identified. If they have the case of low average monthly income, they might be challenged to seek health care as early as needed.
Poor knowledge of TB resulted in threefold times more likely to delay HF care-seeking than knowledgeable patients. This study was consistent with the study conducted in the Affar region. 42 This might be due to low awareness about symptoms of TB and the negative impacts of TB that enforce them to seek health care to be healed from the infection as early as possible. If the patient knew about the case, they would have sought healthcare as the case is curable.
Traveling more than 30 min to a HF contributed about twofold times more likely to delay healthcare-seeking than those traveling 30 min or less. This might be related to the distance that should be traveled to access healthcare. As HFs distance from their residential area, the probability to seek health care for their problem becomes low.
Fear of COVID-19 was about threefold times more likely to delay healthcare-seeking than those not fearing COVID-19. A possible explanation might be, fear of COVID-19 challenges them to seek healthcare because of the perception going to the hospital may lead to COVID-19 exposure that may infect them. The other explanation might be due to the symptom of TB-like coughing might be considered a symptom of COVID-19 that they fear being diagnosed with COVID-19 as well as fear of isolation due to the perception of being COVID-19 patient might be the reason for healthcare-seeking delay.
Information from this study is useful in developing interventions aimed at improving the early healthcare-seeking to initiate effective chemotherapy and minimize the potential of disease transmission in the population and the burden of morbidity in the patients. In the same way, the study can help health extension workers to have adequate information to improve finding TB cases in the community, especially in the study areas.
Furthermore, findings from this study can be used by the Ilubabor Zone health department to design and develop locally an appropriate plan and implementation strategy to improve early case detection of TB patients. Finally, the study is also important in providing information for government policymakers, program planners, and nongovernmental organizations to develop a relevant intervention.
Conclusion
This study found that healthcare-seeking delay among TB patients was substantial. Factors that contributed to patient healthcare-seeking delay were fear of COVID-19, rural area residence, poor knowledge, traveling time >30 min to a HF, and average monthly income <2000 ETB. Creating awareness for the community toward TB and about early healthcare-seeking as soon as the appearance of TB symptoms with clear information about the symptoms especially, for the rural communities as the result of the study indicated that they are both poor knowledge about the infection; by encouraging them to travel more distance to be healthy from the acute and chronic outcome of the disease. They should also focus on a group of people with a fear of COVID-19 to seek healthcare as early as possible by developing a strategic intervention for the group of the society according to the police of the country to overcome a fear of COVID-19.
Strength of the study: In this study, the variable that was not considered in the previous studies “fear of COVID-19” was included.
Limitation of the study: Due to the design effect, identification of cause and effect is difficult. Comparing the situation of improvement of delay due to COVID-19 during the study period as the general of the country was difficulty due to deficit of information.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221142469 – Supplemental material for Healthcare-seeking delay during COVID-19 pandemic among tuberculosis patients in Ilubabor zone health facilities, south-west Ethiopia
Supplemental material, sj-docx-1-smo-10.1177_20503121221142469 for Healthcare-seeking delay during COVID-19 pandemic among tuberculosis patients in Ilubabor zone health facilities, south-west Ethiopia by Jira Wakoya Feyisa, Keno Melkamu Kitila, Jiregna Chalchisa Lemu, Megersa Dinku Hunde and Aboma Diriba Hunde in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to acknowledge the Ilubabor health facilities administrator, health professionals, and data collectors who contributed to this work. We would like to thank all the participants for their participation and the information they provided us. Finally, we would like to extend our gratitude to Mettu University.
Author contributions
KM, JW, JCH, MD, and AD conceived and designed the study, developed data collection instruments, and supervised data collection. KM, JW, JCH, and MD participated in the testing and finalization of the data collection instruments and coordinated the study progress. JW performed the statistical analysis and wrote all versions of the manuscript. All authors read and approved the final manuscript.
Availability of data and materials
The raw data documents are available upon request from the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval was obtained from the research and community service coordination office (RCS) of Mettu University College of Health Sciences with Ref/RCS/114/13. Following the approval, an official letter of co-operation was written to concerned bodies. Permission was also obtained from the zonal Health Bureau.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Respondents were informed about the objective and purpose of the study and written informed consent was obtained from each respondent. Clear information was given to inform respondents about the purpose and procedure of the study, the importance of their participation, the right to withdraw at any time if they want, and about privacy and confidentiality of the information maintained throughout the study by maintaining anonymity, keeping their privacy by interviewing them in a separate room during the interview and locking records; for every study participant written consent was ticked as “yes” by data collectors if the individual was voluntary to participate. Therefore whether educated or not the purpose of the study was read for them and they understood and decided.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.