
Abstract
The assessment of value along the clinical development and regulation of a new medicine is complex and involves different decision problems. It commences with manufacturers’ internal decisions regarding which disease areas to invest in as part of research and development (R&D) portfolio prioritization and progresses to choices related to clinical study design, regulatory assessment of the product’s benefit-risk profile, payer evaluation of reimbursement conditions via health technology assessment (HTA), and concludes with prescriber behavior based on clinical guidance and individual patient need. Arguably, for better decisions and improved transparency, the preferences of decision makers should more often be quantified and explicitly communicated. 1
The early HTA context, in which payer concerns relating to the expected value of new compounds are explored before the licensing stage, is becoming more important in Europe. This is reflected through the joint work plan of the European Medicines Agency (EMA) and the European Network for Health Technology Assessment (EUnetHTA),2,3 an important aspect of which is parallel consultation 4 and EUnetHTA Early Dialogue. 5 Early HTA empirical studies are becoming more frequent, and although a number of methods have been used to identify and evaluate technologies, the use of multicriteria decision analysis (MCDA) has been recommended as a tool to support decisions in product development.6,7
Decision analysis methods and, specifically, quantitative modeling approaches such as MCDA can be used to aid medical decision making, to explicitly integrate objective measurement with value judgment while managing subjectivity transparently. This is useful for drug evaluation contexts because, although the clinical evidence concerning different treatments’ performance might be objective in nature, the understanding of its value requires subjective interpretation; for example, relating to the relevance of data for the disease of interest, the meaningfulness of improvement in health benefit, and the value trade-offs with possible risks 8 .
A method of eliciting value preferences from different stakeholder groups is decision conferencing,9,10 a form of face-to-face workshops guided by a facilitator while applying decision theory with multiple objectives. 11 In medical decision making, MCDA methods in combination with decision conferencing could be used as a tool to elicit and communicate value preferences across a number of evaluation aspects with the view to ranking a set of alternative medical options based on their value. 12
Since European drug regulators called for more explicit and quantitative methodological approaches in the assessment of drug benefit-risk balance with well-defined evaluation criteria and the valuation of outcomes through numerical weights, 13 a number of MCDA studies have been conducted in the licensing context.14–16 The EMA currently adopts and recommends the use of the “effects table” for the tabulation of the most important favorable and unfavorable effects and their uncertainty, 17 a constituent step of MCDA methodologies 18 . Other similar structured frameworks are also implemented by drug regulators for increasing transparency in the communication of benefits and risks, 19 including by the US Food and Drug Administration. 20
Due to various limitations of economic evaluation methods, MCDA applications in the context of HTA have intensified in recent years.21,22 Good practice guidelines for the use of MCDA and its adaptation to HTA have been developed,23–25 and different multicriteria value frameworks have been recommended.26–29 A number of empirical studies have been conducted, often simulating different HTA settings30–33 or by involving and eliciting the preferences of real decision makers and evaluators across different settings.34–37 Still, a number of challenges relating to the appropriate use of such methods and their integration with policy-making have been raised that would be critical for MCDA implementation.38,39
Although MCDA approaches have been explored in the context of product development and treatment selection, fewer studies exist compared with the drug approval context. Relevant case studies include the use of MCDA and decision conferencing to prioritize R&D project portfolios of pharmaceutical companies and budget allocation 40 and the use of a stochastic MCDA approach for the selection of statins in primary prevention. 41
In the context of early HTA, no quantitative, cross-country MCDA studies exist. More broadly, in the context of health care evaluation, there have been no validating MCDA studies testing the consistency of their results by repeating the exercise with different groups of participants.
In this study, we investigate the use of the Advance Value Framework (AVF), a multicriteria value framework, 27 to assess the value of compounds in clinical development for the treatment of nonalcoholic steatohepatitis (NASH). A key objective is to test the consistency of the results, both between and within countries, by conducting 2 rounds of decision conferences (DCs). An early-stage HTA scope is adopted in an attempt to make the best use of available evidence at the time of the study, with the collection of views from key stakeholders across 3 countries (England, France and Germany). Given the compounds’ early clinical development stage, a set of hypothetical assumptions are imposed in some cases on their performance for the purpose of enabling their comparative assessment. The output generated aims to engage key experts and decision makers in discussions around compound value at this early stage in their development, to communicate their value prospects while aligning with increasing clinical evidence availability, rather than inform clinical or policy decisions.
Methods
Methodological Framework and Overall Process
The AVF is based on multiattribute value theory (MAVT)10,42 and comprises 5 distinct phases: a) problem structuring, b) model building, c) model assessment, d) model appraisal and e) development of action plans. 25 The AVF was operationalized using a decision support system (M-MACBETH) enabling the use of graphics to build a model of values, acting as a facilitation tool to inform both the structuring phases (“a,”“b”) and the evaluation phases (“c,”“d”) 43 ; the development of action plans phase (“e”) was not conducted because of the early development phase of the compounds.
The study consisted of 2 rounds. The first took place between November 2016 and June 2017 and included all 4 phases (a–d) with the involvement of 26 participants in 3 DCs (1 in each country); the second took place between November 2017 and June 2018, acting as a follow-up to validate the results obtained in the first round by conducting the 3 latter phases of the methodological process (b–d) and involving 25 participants, the purpose being to elicit additional preferences through 3 further DCs in the same study countries. Both rounds used an identical methodological approach in relation to value preference elicitation and construction.
Following problem structuring (phase a), as part of model building (phase b), an extensive review of the clinical literature was conducted to understand the clinical endpoints of interest and in consultation with a clinical hepatologist, co-author of the study (M.T.), a preliminary version of a NASH value tree was developed alongside the collection of the appropriate performance data, which was validated at the beginning of each DC. During model assessment (phase c) and model appraisal (phase d), DC participant value preferences were elicited and were used to inform, first, compound scoring against the evaluation criteria and, second, criteria weighting. The process was completed by analyzing the results, including sensitivity analysis.
Phase a. Problem Structuring: Clinical Practice and Scope
Nonalcoholic fatty liver disease (NAFLD) is the most common chronic liver disease worldwide, affecting as many as 30% of adults and 70% to 80% of those who are obese and have type 2 diabetes. 44 NAFLD represents a histologic spectrum of conditions, ranging from simple steatosis to NASH and cirrhosis. Many with simple steatosis do not develop significant liver disease, however NASH can progress to cirrhosis, hepatocellular carcinoma and end-stage liver disease; it has become the second leading aetiology of liver disease among adults awaiting liver transplantation in the United States. 45 NASH is projected to become the leading indication for liver transplantation within the next decade (for more clinical information see the Supplementary Appendix).
In the context of this study, a simulation exercise was undertaken focusing on the assessment of the overall value of compounds in clinical development for the treatment of NASH, by adopting an early HTA perspective focusing on market access and coverage decisions with the involvement of key stakeholders, including HTA experts and proxy decision makers.
Phase b. Model Building: The Advance Value Tree Adaptation, Alternative Treatments and Evidence, Attribute Ranges and References
1. The Advance Value Tree (AVT) adaptation for NASH
As part of the AVF, the AVT is a generic value tree providing HTA-related value concerns for new medicines in a hierarchical structure of evaluation criteria. 27 Based on a structured process involving systematic review and expert consultation 46 and adopting a top-down approach, 47 the AVT consists of 5 value domains (i.e. criteria clusters), capturing all essential value attributes of new medicines in the HTA context under a prescriptive decision-aid approach: 1) burden of disease (BoD), 2) therapeutic benefit (THE), 3) safety profile (SAF), 4) innovation level (INN), and 5) socioeconomic impact (SOC), such that overall value is a function expressed as follows:

The latest available evidence from clinical studies was used to populate the performance of the alternative options across the respective criteria attributes of the AVT. The AVT was thus adapted for the context of NASH as part of a bottom-up, alternative-focused thinking approach, following the comparison of the alternative compounds, in consultation with a hepatology specialist (M.T., study co-author).25,48 This adaptation resulted in the preliminary version of the NASH value tree, which served as the basis of assessing the value of NASH compounds in the first round of DCs, comprising a total of 17 criteria attributes. The burden of disease cluster was removed because all alternative treatments were assessed for the same indication, whereas socioeconomic impact criteria were excluded because of lack of evidence.
Following the completion of the first round of DCs, the final version of the value tree was used as the starting point for the second round of DCs, that is, the preliminary version in the second part of the exercise. In arriving at the NASH-specific attributes and the respective value tree, we strived to adhere to key decision theory properties such as preferential independence and nonredundancy, thus ensuring attribute selection was methodologically correct and theoretically robust. 49
2. Alternative treatments compared and evidence considered
A total of 4 compound profiles were assessed, 3 with publicly available phase 2 results plus a hypothetical product profile (HPP); the latter was viewed as an “aspirational summary” of a hypothetical product in terms of labeling concepts, leveraging hypothetical information about the compound available at a particular time in development, 50 effectively providing a prospective summary of the characteristics of a product that could theoretically be achieved. 51 Information on the HPP was communicated by the study sponsor. Because of the commercial in confidence information surrounding the HPP, all compounds are anonymized in the study.
Given the early assessment scope of the exercise with no available drug treatment on the market for NASH, we used the most relevant clinical evidence for the assessment of the compounds, including a number of assumptions for the performance of the HPP. Expert opinion was used to specify the performance of options across specific criteria in case such information was not available.
The final performance of options used across the different criteria attributes together with the respective range of placebo arms and lower – higher (i.e., least preferred – most preferred) reference levels used in the models is shown in Supplementary Table A1; additional information on evidence considered is discussed in the Supplementary Appendix.
3. Setting attribute ranges and reference levels
For the purposes of scoring and weighting, “higher” (x_h, set at 100) and “lower”( x_l, set at 0) reference levels were defined for each attribute acting as benchmarks of an interval value scale based on which the compounds were scored, that is, v(xhigher) = 100 and v(xlower) = 0. The “higher” reference corresponded to the best available performance on that attribute and the “lower” corresponded to the worst available performance across the compounds compared. These reference levels were needed for the construction of criteria partial value functions on interval scales and the elicitation of relative weights. Given the application of an additive aggregation model, a hypothetical overall weighted preference value (WPV) score of 100 for a compound would entail the best possible performance across all criteria, whereas an overall WPV score of 0 would entail the worst possible performance across all criteria (see Appendix Table A1, last 2 columns for worst and best reference levels of all criteria).
Phase c. Model Assessment; and Phase d- Model Appraisal: DCs and MCDA Technique
In each of the 2 DC rounds, the completion of model-building, model assessment and part of the model appraisal phases took place through 3 DC meetings with key stakeholders, mimicking what would occur in the respective settings 10 ; these took the form of facilitated workshops lasting 1 to 1.5-days each and were conducted in England (London), France (Paris) and Germany (Berlin).
DC participants consisted of small groups of experts, ranging between 5 and 13 participants. We endeavoured to involve all relevant stakeholder groups and perspectives, reflecting actual assessment processes in the study countries; specifically, health care professionals, methodologists, and patient representatives were included. These sizes have been shown to be optimal, allowing efficient group processes to emerge while preserving individuality, as they are large enough to represent all major perspectives but small enough to be able to work toward agreement. 8 A summary of participant numbers and stakeholder groups in each meeting together with each DC duration is shown in Table 1.
Decision Conference Participant Numbers, Stakeholder Groups, and Durations
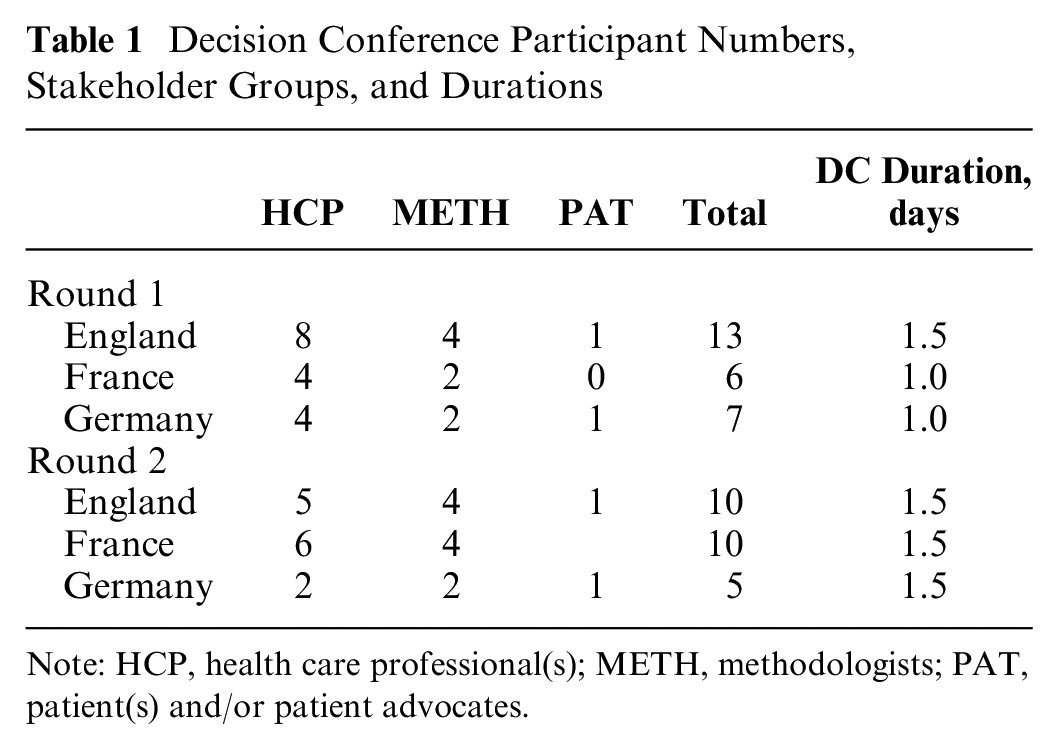
Note: HCP, health care professional(s); METH, methodologists; PAT, patient(s) and/or patient advocates.
An impartial facilitator (J.B.C., study co-author) guided the process interaction while refraining from contributing to content, essentially helping the group in how to think about the issues but not what to think,40,52 thus pointing to an interactive model-building process in which debate was encouraged and differences in opinion were actively sought in an iterative manner. Where consensus could not be reached, value judgments were selected based on majority voting, representing a single preference input for the whole group of participants and the relevant parameter was then tested in sensitivity analysis (the Supplementary Appendix contains further information about the decision conferencing process).
Compound overall value was obtained through the application of the additive aggregation model. The AVF was operationalized by adopting a typical simple additive aggregation approach, where the overall value V(.) of an option a would be given by Eq. (2) 27 :
where vi(a) is the partial value score of option a obtained by the application of the value function of criterion i to the performance of a in that criterion, wi is the weight of criterion i, and m is the total number of criteria (attributes). This function V(.)_ is effectively a multiattribute value function. 11
A MACBETH (Measuring Attractiveness by a Categorical-Based Evaluation Technique) protocol was adopted as an approach to elicit value preferences, effectively using qualitative judgments about the difference in value between different pairs of performance levels.53,54 MACBETH is based on strong theoretical foundations, 55 and its usefulness as a decision support tool has been shown through numerous applications for a variety of real-world problems56,57 as part of which semantic judgments are converted into a cardinal scale. We used M-MACBETH, 58 a decision support system based on the MACBETH approach, to elicit value preferences of DC participants and complete the MCDA model. Following the DCs, additional deterministic sensitivity analysis was conducted to address parameter uncertainty on criteria weights, by systematically exploring changes on baseline weights and their impact on the overall value rankings of the compounds (the Supplementary Appendix contains further information on MACBETH, M-MACBETH, and the robustness analysis conducted).
Results
Final Value Trees
The attributes of the final NASH value tree in each country, as emerged following discussions with DC participants, are listed in Table 2. Schematic illustrations of the final value trees emerging from each DC are shown in Supplementary Appendix Figure A1.
Criteria Definitions and Their Consideration in Each Jurisdiction per Round of Decision Conference (Their Presence Denoted by “X”)
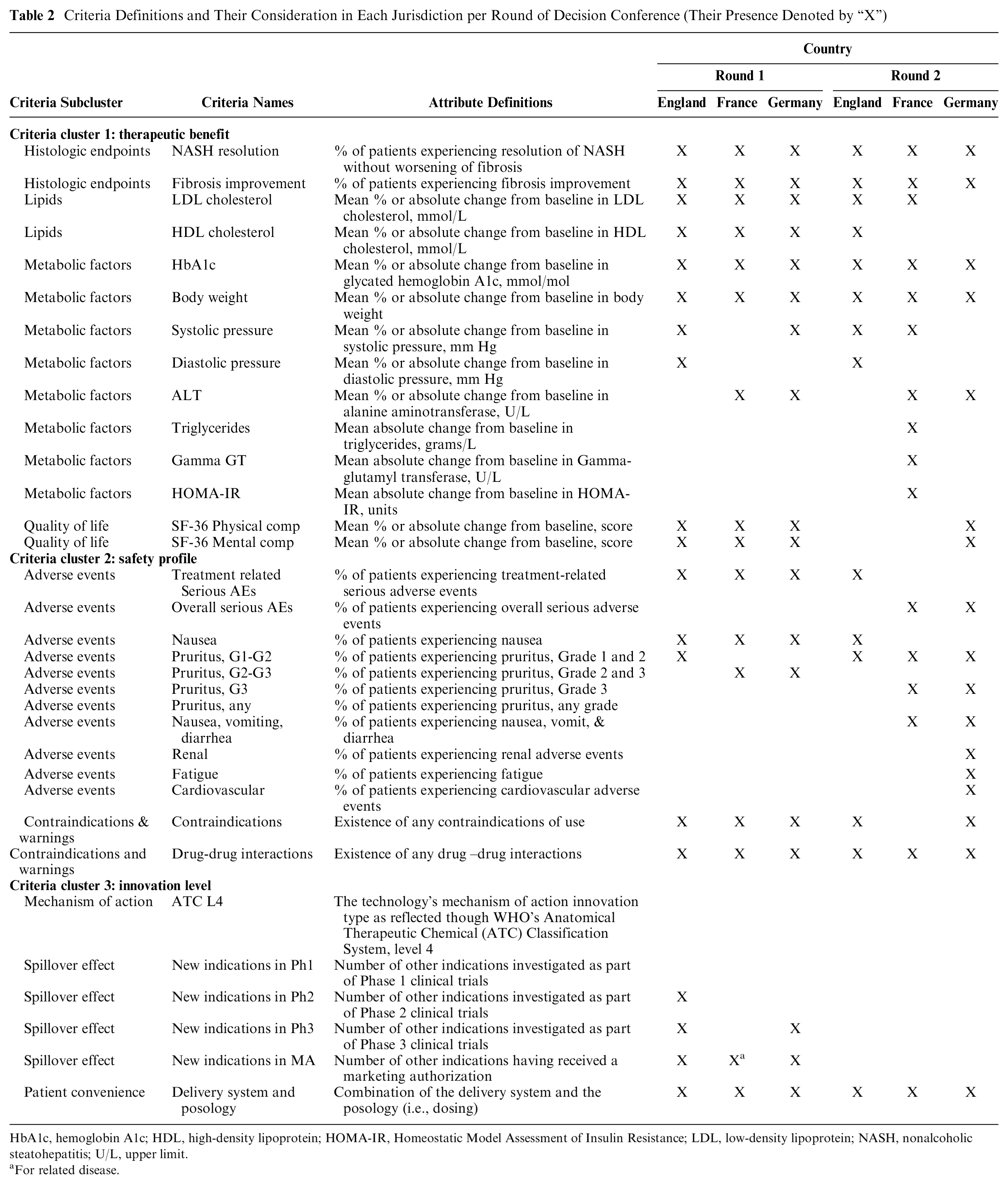
HbA1c, hemoglobin A1c; HDL, high-density lipoprotein; HOMA-IR, Homeostatic Model Assessment of Insulin Resistance; LDL, low-density lipoprotein; NASH, nonalcoholic steatohepatitis; U/L, upper limit.
For related disease.
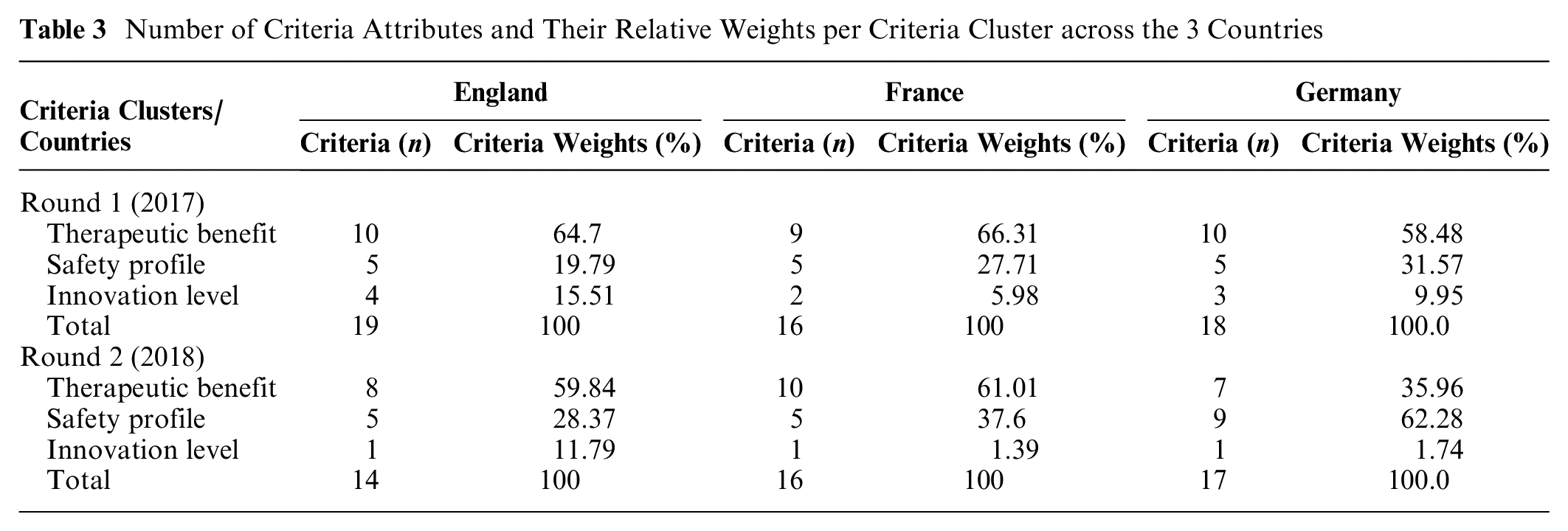
Across the 3 study countries over the 2 rounds of DCs, 14 to 19 attributes were included in the value tree, as shown in Table 3. In terms of the different criteria clusters' composition, in round 1 the THE cluster comprised 9 to 10 attributes, followed by SAF (5 attributes) and INN (2–4 attributes) clusters. In round 2, THE comprised 7 to 10 attributes, followed by SAF (5–9 attributes) and INN (1 attribute) clusters. In round 2, the value tree of each country consisted of the same or lower number of attributes compared with round 1. In both rounds of DCs, the largest number of criteria were allocated under the THE cluster, followed by SAF and INN, with the exception of the second round in Germany, where more criteria were included in the SAF cluster, followed by THE and INN.
Number of Criteria Attributes and Their Relative Weights per Criteria Cluster across the 3 Countries
A common feature of changes in the composition of value trees across all 3 countries over the two rounds was the non-inclusion of spillover effect criteria under the INN cluster because they were considered to be non-relevant for the scope of the exercise. Another common feature as evident from the English and French DCs was the non-inclusion of the SF-36 summary scores (physical and mental component scores) as they were judged to be non-clinically meaningful.
Criteria Weights
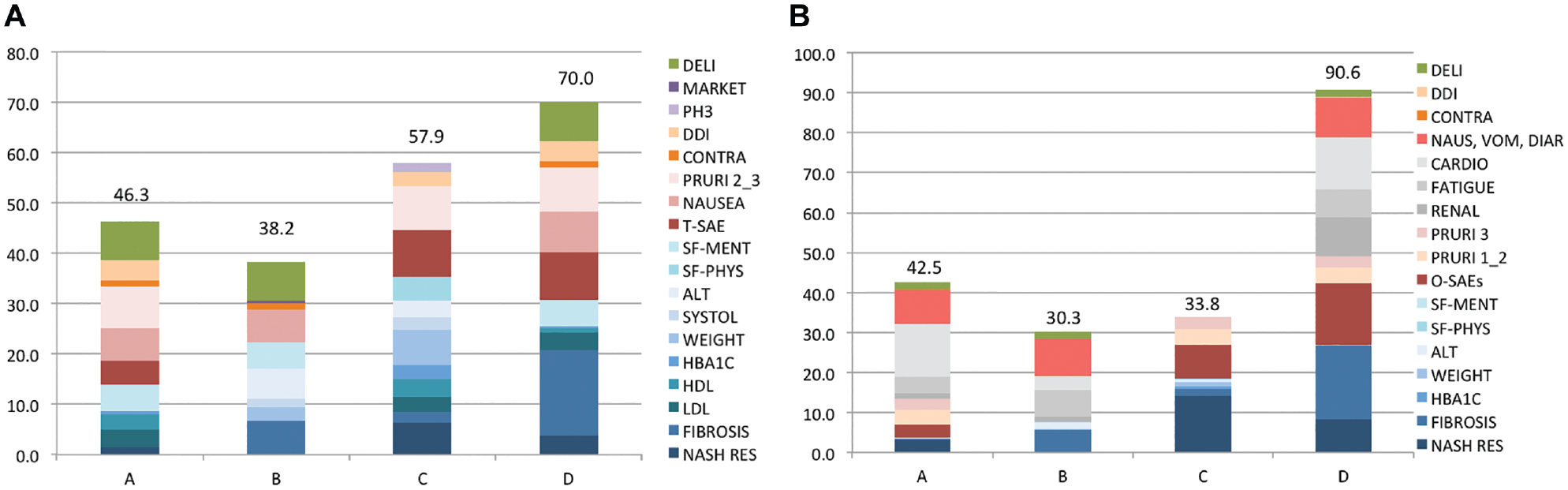
The relative weights of individual criteria across both rounds are illustrated in Figure 1. In terms of the total weights assigned across the different criteria clusters, the THE cluster always obtained the highest rank, followed by SAF and INN, with the exception of round 2 of the German DC, in which the SAF cluster outranked THE. The fact that the THE cluster always contributed to more than 50% of the model's total weight means that an improvement from the worst to the best reference level in this cluster’s criteria would always be considered more valuable than an improvement in the other criteria clusters combined. Across countries, the relative weight of the SAF cluster increased in round 2 compared with round 1 to the detriment of the THE and INN clusters, whose relative weights declined. In terms of individual criteria, the number of highest-ranked criteria assigned a relative weight of 10% or more was always observed to be higher in the second compared with the first round of DCs across all 3 countries. The relative weights of criteria and their differences across countries reflect the actual value preferences of the participants but are also influenced by the number of criteria being considered in each value tree.
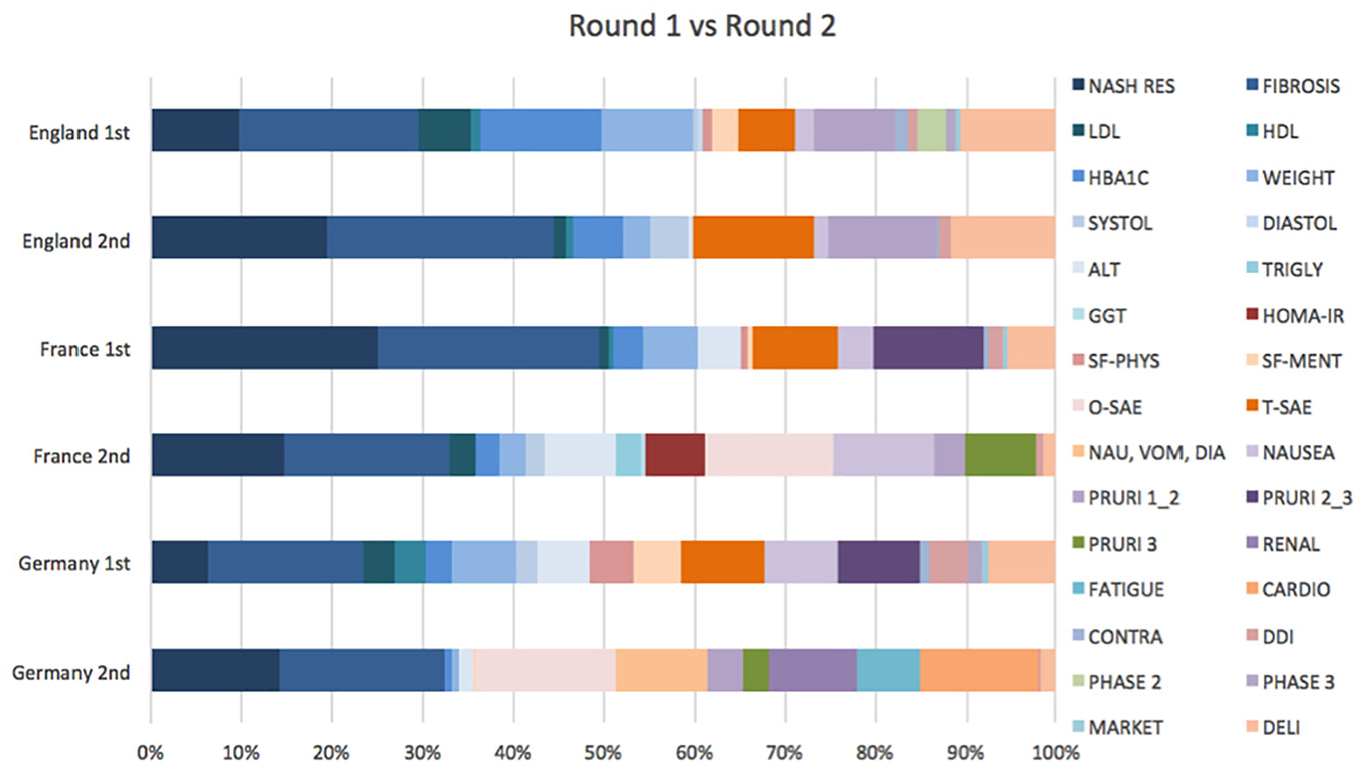
Relative weights of criteria across the 2 rounds of decision conferences. NASH RES, NASH Resolution; FIBROSIS, fibrosis improvement; LDL, low-density lipoprotein cholesterol; HDL, high-density lipoprotein cholesterol; HbA1c, hemoglobin A1c; WEIGHT, body weight; SYSTOL, systolic blood pressure; DIASTOL, diastolic blood pressure; ALT, alanine aminotransferase; TRIGLY, triglycerides; GGT, gamma-glutamyl transferase; HOMA-IR, Homeostatic Model Assessment of Insulin Resistance; SF-PHYS, SF-36 physical component score; SF-MENT, SF-36 mental component score; T-SAE, treatment-related serious adverse events; O-SAE, overall serious adverse events; NAUSEA, nausea; NAU, VOM, DIA, nausea, vomiting, and diarrhea; PRURI 1_2, pruritus grades 1 and 2; PRURI 2_3, pruritus grades 2 and 3; PRURI 3, pruritus grade 3; RENAL, renal events; FATIGUE, fatigue; CARDIO, cardiovascular events; CONTRA, contraindications; DDI, drug-drug interactions; PHASE 2, phase 2 indications; PHASE 3, phase 3 indications; MARKET, market authorized indications; DELI, delivery system and posology.
In England, the THE cluster accounted for the highest proportion of the model’s relative weight, followed by SAF and INN; this result was consistent in both rounds. Four criteria were assigned a relative weight of 10% or more in round 1 (fibrosis improvement [19.8%], HbA1c [13.4%], delivery system and posology [10.7%], body weight [10.2%]), in contrast to 5 criteria in round 2 (fibrosis improvement [25.3%], NASH resolution [19.4%], treatment-related serious adverse events [13.5%], pruritus G1,2 [12.1%], delivery system and posology [11.8%]).
In France, across both rounds, the THE cluster accounted for the highest proportion of the model’s relative weight, followed by SAF and INN. Three criteria were assigned a relative weight of 10% or more in the first round (NASH resolution [25.0%], fibrosis improvement [24.5%], pruritus G2,3 [12%]) compared with 4 criteria in the second round (fibrosis improvement [18.1%], NASH resolution [14.9%], overall serious adverse events [14.4%], nausea, vomiting, and diarrhea [11.1%]).
In Germany, there were some differences in the overall weight of clusters between rounds, such that the THE cluster was outranked by the SAF cluster in the second round in terms of their total weights, followed by INN in third place. Although only a single criterion was associated with a relative weight of 10% or more in round 1 (fibrosis improvement [17.0%]), a total of 5 criteria were assigned a relative weight of 10% or more in round 2 (fibrosis improvement [18.3%], overall serious adverse events [15.3%], NASH resolution [14.2%], cardiovascular adverse events [13.1%], nausea, vomiting, and diarrhea [10.2%]).
Of the 6 rounds, fibrosis improvement ranked first 5 times and second once, with a relative weight ranging from 17.0% to 25.3%. NASH resolution appeared in the top-3 for a total of 4 times, and serious adverse events (treatment related or overall, depending on the country) ranked second or third 4 times.
Overall Compound Rankings and Value Composition
In terms of the compounds’ overall rankings, across the 3 countries and the 2 rounds of DCs, compound D was always ranked first (overall weighted preference value (WPV) score range: 67.4–90.6). With the exception of the second round of the German DC, in which compound A ranked second and compound C third (overall scores of 42.5 and 33.8, respectively), in all remaining rounds across countries compound C ranked second and compound A ranked third (overall score ranges: 33.8–63.3 and 37.0–46.3, respectively). Compound B always ranked last (overall score range: 24.7–38.2). The largest difference between the first and second ranked compound was 48.1 points (D over A in the second DC in Germany), whereas the smallest difference was 6 points (D over C in the first DC in England).
The overall WPV scores for all compounds across the study countries and the 2 DC rounds are shown in Table 4. Stacked bar plots of the compounds’ overall WPV scores across the 3 countries over the 2 rounds of DCs are shown in Figures 2 to 4, with absolute value contributions of each criterion. It should be clear that the overall WPV score of each option depends on the criteria included in the value model, the shape of the value functions that influence the value scores, and the criteria weights that are elicited using the 2 reference levels.
Overall Weighted Preference Value (WPV) Scores of the Compounds across the 3 Countries over the 2 Rounds of Decision Conferences a
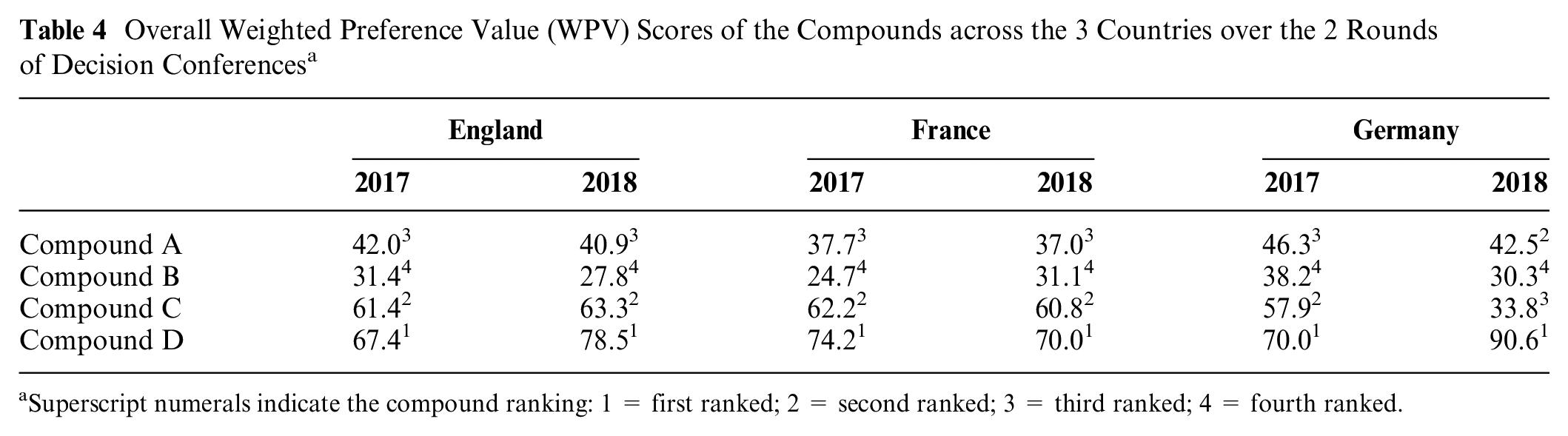
Superscript numerals indicate the compound ranking: 1 = first ranked; 2 = second ranked; 3 = third ranked; 4 = fourth ranked.
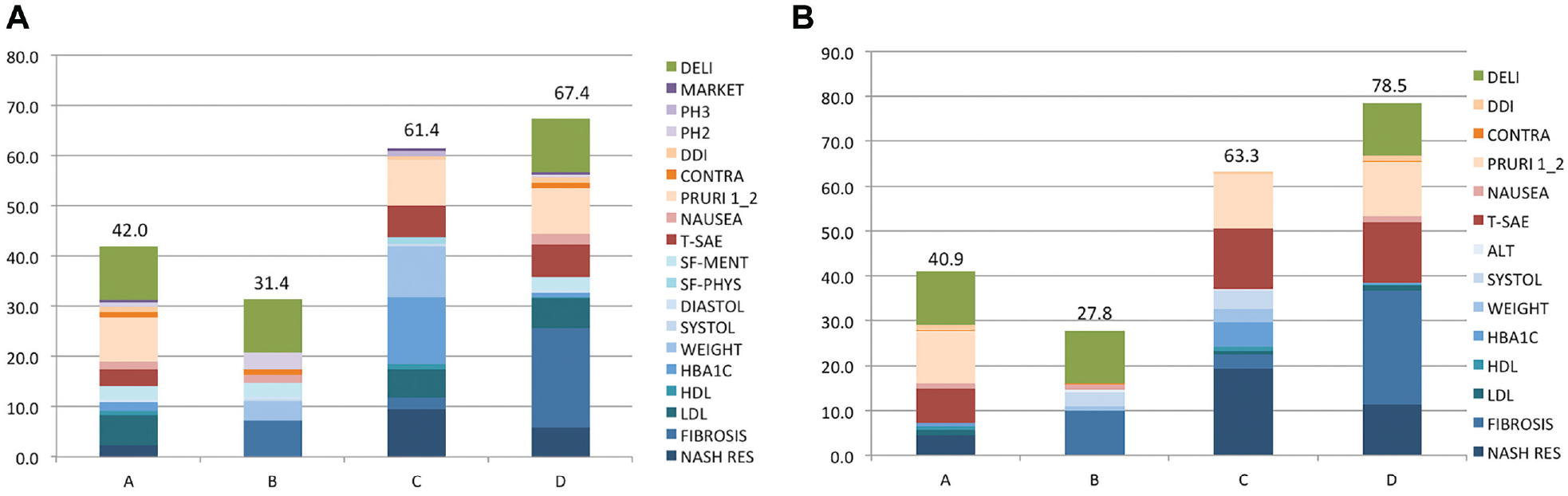
Stacked bar plots of compounds’ overall weighted preference value scores over the 2 rounds of decision conferences in England. (a) Round 1. (b) round 2.
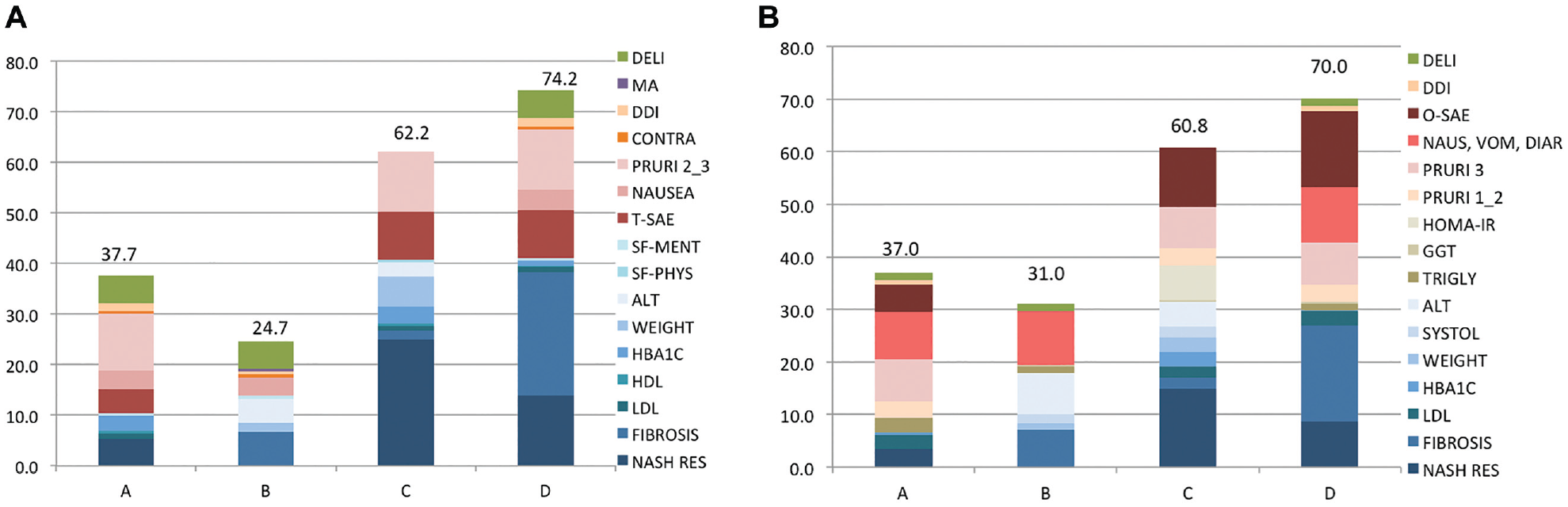
Stacked bar plots of compounds’ overall weighted preference value scores over the 2 rounds of decision conferences in France. (a) Round 1. (b) Round 2.
Stacked bar plots of compounds’ overall weighted preference value scores over the 2 rounds of decision conferences in Germany. (a) Round 1. (b) Round 2.
In the English and French DCs, the largest proportion of the leading compound’s value contribution (compound D) was always due to its performance on the THE cluster, followed by the SAF and INN clusters. By contrast, in the German DC, the largest proportion of compound's D value was accounted for by the SAF cluster in both rounds, followed by the THE and INN clusters. In terms of individual criteria, across all 3 countries and over both rounds, fibrosis improvement was always the most influential value dimension on compound’s D overall value composition, contributing the greatest value score.
The sensitivity and robustness analyses demonstrated that treatment rankings are robust to the relative criteria weights across the different settings. The only case in which a change of less than 100% of a criterion’s weight could affect the compound ranking was in the first DC round in England and France, in which a 29% reduction in fibrosis improvement (from 19.8% to 14.0%) and a 77% increase in NASH resolution (from 25% to 44.2%) would be adequate for compound C to become better ranked than compound D.
Discussion
This two-round, cross-country exercise demonstrated the application of a recently developed MCDA methodological process and value framework25,27 for a set of alternative compounds under clinical development versus a HPP in the context of early HTA. In terms of design, implementation and review of the analysis, the process adopted was in alignment with good practice guidelines on the use of MCDA in health care decisions.23,24
Compound Ranking and Value Preferences
Based on the MCDA model used, the set of evaluation criteria considered, and the respective performance of the compounds used, we found that the ranking of the compounds was virtually identical across the study countries and both DC rounds. Compound D always ranked first based on DC participants’ overall WPV scores, followed by compounds C, A, and B, with the exception of the second DC in Germany, where compound A ranked higher than compound C.
In terms of the various value reflections, with the exception of the second German DC, the THE cluster had the highest relative importance for participants across all 3 countries (59%–66% of model weight), always followed by the SAF (20%–38%) and the INN clusters (1%–16%). With the exception of the second German DC, the SAF cluster outranked the THE cluster with 62% versus 36%.
Fibrosis was the most important criterion across countries and DC rounds, having the highest relative weight in most cases, with the exception of the French DC (round 1 only), where it was assigned the second highest weight but still very close to the top-ranked criterion. In France, the 2 histologic endpoints played the most important role to stakeholders in both rounds; this partly explains why the THE cluster produced the highest relative weight across all 3 countries.
Some differences were recorded between rounds and the criteria accounting for at least 50% of the model weight in each case. In the English DCs, for at least 50% of the model’s weight to be accounted for, weights of the 3 leading criteria had to be included, adding up to 58% in the second round (the 2 histologic endpoints and treatment-related serious adverse events). By contrast, the 4 highest ranking criteria in the first round (fibrosis improvement, HbA1c, delivery system and posology, and body weight) accounted for 54% of the model’s weight. In the French DCs, for at least half the model’s weight to be captured, the weights of the four highest ranking criteria in the second round had to be included, adding up to 59% (the 2 histologic endpoints, overall serious adverse events and nausea, vomiting, and diarrhea); by contrast, the top 3 criteria in the first round accounted for 61% of total model weight (the 2 histologic endpoints and pruritus G2,3). In the German DCs, for at least half the importance of the model’s weight to be captured, in the second round the weights of the 4 highest ranking criteria had to be included, adding up to 61% (the 2 histologic endpoints, overall serious adverse events and cardiovascular adverse events). In comparison, the 5 highest ranking criteria in the first round added up to 51% (fibrosis improvement, treatment-related serious adverse events, pruritus G2,3, nausea and delivery system and posology).
Overall, nearly identical results were observed across countries and rounds in terms of compound rankings. Understandably, the direct comparison of overall value scores between options requires identical value models, comprising the same criteria sets, weights, and value functions. The ranking comparisons made in this study using ordinal scales reflect these restrictions. Nevertheless, when trying to interpret differences in results between countries, it could be argued that any disparities might be due to either “real” country differences relating to the consideration of different fundamental objectives, priorities, and preferences (as reflected through differences in criteria inclusion, relative weights assignment, and scores elicitation), or differences relating to individual participants. This was indirectly addressed through the extensive sensitivity analysis conducted, aiming to reduce parameter and, by extension, intracountry uncertainty, but also through the further insights generated in the second round of DCs, which practically validated the results of the first round.
Limitations
One of the study limitations is the lack of relative effect estimates as part of clinical evidence and the use of their absolute effects from different clinical trials with the assumption that they can be compared directly. Given the absence of head-to-head clinical trials directly comparing the compounds of interest, the small number of clinical trials available and their early phase, absolute effects from the respective single randomized clinical trials of the alternative compounds were used. If more clinical studies become available, an indirect treatment comparison could be conducted first using a common comparator to estimate the relative effects of 2 treatments versus the comparator, or a network meta-analysis combining both direct and indirect evidence available through a mixed treatment comparison. Although the placebo range was disclosed to participants during the workshops, the incremental performance difference from placebo would be needed to better understand the associated value. In real-world evaluations aiming to inform decision making, evidence synthesis would be required to take place together with evidence collection as part of the model-building phase.
A second limitation relates to the clinical trials used as the source of evidence. Only data from a single, phase 2, randomized clinical trial per compound was used with relatively small sample sizes (number of subjects randomly assigned in either arm ranging from 26–142 patients).
Third, the studies used had different populations (disease stage), different trial durations, and one did not meet its primary endpoint, all of which have implications in terms of their comparability and perceived efficacy. Differences in the definitions of histologic endpoints across studies were assumed to be comparable, considering that a consensus across NASH primary outcome definitions is lacking. Given the uncertainty around treatment effects, participants were instructed to assume that they corresponded to a specific sample size of patients, chosen based on the largest number of patients in a single active arm evident across the studies (N = 142), which helped participants to provide a value judgment across the clinical attributes.
Finally, in relation to the participatory approach adopted, not all DCs were of the same size or had the same composition of experts, particularly the second DC in Germany (5 participants), which may have contributed to a different overall compound ranking order.
Lessons Learned
Despite the limitations, this study demonstrated consistency of MCDA results following 2 rounds of preference elicitation via DCs with different participants in 3 settings, suggesting that value preferences and their differences between countries are fairly reliable.
One contribution of this study relates to the value attribution of NASH compounds in different countries as reflected through the key drivers of their overall scores. The 2 histologic endpoints of fibrosis improvement and NASH resolution had a clear influence in this context. Regarding differences in the acceptability of the evaluation criteria considered, the German experience (and, to a lesser degree, the French experience) suggests that it is paramount to submit evidence on clinically meaningful outcomes relating to mortality, morbidity, and quality of life. Alternatively, if surrogate endpoints are used, they should be accompanied with a clear impact on relevant clinically meaningful outcomes or demonstrate minimum clinically important differences. This could be informed by randomized prospective interventional studies or by focusing on the magnitude of the studies rather than follow-up duration.
A number of insights relating to the usefulness of MCDA in early HTA have been generated. In terms of the phase of clinical development, it became obvious that there will be a trade-off between data availability and prospects of influencing drug development. Regarding the preference for data on clinical versus surrogate endpoints, this seems to be universally true, but surrogates can probably be accepted if they are validated and can predict the clinical endpoint. It is recommended to provide correlations of surrogates with outcomes and/or clinically meaningful thresholds.
A critical issue observed across the different country settings was the current clinical debate given the lack of a clear disease definition, including the challenges around disease diagnosis and identification of patients in greater need. The debate around clinically meaningful outcomes was indicative in that context, with most clinical studies using histologic endpoints as surrogate markers. This suggests that a better understanding of the disease together with the development of improved clinical guidelines could potentially benefit the elevation of NASH in the national policy agendas of decision and policy makers.
In terms of methodological contribution, the analytical objectives in early HTA contexts should always be clearly defined (e.g., evaluation of current product profiles vs. design of future phase 3 trials) to facilitate preference elicitation as part of DCs or other participatory processes. With regard to improvements around evidence synthesis and summary, assuming the use of nonsynthesized clinical evidence and the existence of a common comparator (such as placebo arms), the use of performance levels compared with the comparator (e.g., incremental placebo differences) should be explored. Using performance levels, it could be easier for participants to comprehend the significance of any relevant treatment effects. However, it should be considered whether this might have an influence on the definition and interpretation of the reference levels, as an “incremental” treatment effect might also have to be present across other non-clinical criteria for a more homogeneous and easier interpretation of the results.
Importantly, for the use of non disease-specific clinically meaningful outcomes, it might be useful to derive clinically meaningful thresholds or correlations that could inform the elicitation of value judgments and preferences, for example, minimally clinically important difference for PRO instruments.
Finally, DCs should be conducted over a 2-day period to allow sufficient time for discussion and evidence synthesis tasks, the greatest trade-off being the challenge in recruiting adequate numbers of participants. Venues should be in alignment with DC good practice guidelines with U-shaped seating for direct eye contact and 2 projector screens (one with the value tree, the other with the options performance data). The pool of potential experts to contact to secure adequate DC participants should not be underestimated, particularly in follow-on rounds, as more than 125 experts were contacted to secure 25 in the second round.
Conclusion
In this study, we explored the application of the Advance Value Framework in the context of early HTA for NASH compounds in 3 EU countries and tested the consistency of results by conducting 2 rounds of preference elicitation via decision conferencing. The use of MCDA proved to be promising for early HTA while illustrating high consistency in results across countries and between study rounds. The complexity of NASH management, given the existence of patients with multiple comorbidities and clinical endpoints, enables MCDA to act as a transparent and potentially consistent approach for evaluating compounds in clinical development before market entry. The results can be used to ensure that relevant and important endpoints are included in upcoming clinical studies and to identify potential discrepancies across HTA bodies in terms of value assessment requirements. Ongoing and future research could validate and possibly supplement insights provided regarding differences in value preferences in different settings, whether for NASH or HTA appraisals more generally.
Supplemental Material
Appendix_05JUNE_online_supp – Supplemental material for Early Health Technology Assessment during Nonalcoholic Steatohepatitis Drug Development: A Two-Round, Cross-Country, Multicriteria Decision Analysis
Supplemental material, Appendix_05JUNE_online_supp for Early Health Technology Assessment during Nonalcoholic Steatohepatitis Drug Development: A Two-Round, Cross-Country, Multicriteria Decision Analysis by Aris Angelis, Mark Thursz, Vlad Ratziu, Alastair O’Brien, Lawrence Serfaty, Ali Canbay, Ingolf Schiefke, Joao Bana e Costa, Pascal Lecomte and Panos Kanavos in Medical Decision Making
Supplemental Material
Table_A2_NASH_Sensitivity_Analysis_Raw_anonymised_23MAR__online_supp – Supplemental material for Early Health Technology Assessment during Nonalcoholic Steatohepatitis Drug Development: A Two-Round, Cross-Country, Multicriteria Decision Analysis
Supplemental material, Table_A2_NASH_Sensitivity_Analysis_Raw_anonymised_23MAR__online_supp for Early Health Technology Assessment during Nonalcoholic Steatohepatitis Drug Development: A Two-Round, Cross-Country, Multicriteria Decision Analysis by Aris Angelis, Mark Thursz, Vlad Ratziu, Alastair O’Brien, Lawrence Serfaty, Ali Canbay, Ingolf Schiefke, Joao Bana e Costa, Pascal Lecomte and Panos Kanavos in Medical Decision Making
Supplemental Material
Appendix_20JUL_online_supp – Supplemental material for Early Health Technology Assessment during Nonalcoholic Steatohepatitis Drug Development: A Two-Round, Cross-Country, Multicriteria Decision Analysis
Supplemental material, Appendix_20JUL_online_supp for Early Health Technology Assessment during Nonalcoholic Steatohepatitis Drug Development: A Two-Round, Cross-Country, Multicriteria Decision Analysis by Aris Angelis, Mark Thursz, Vlad Ratziu, Alastair O’Brien, Lawrence Serfaty, Ali Canbay, Ingolf Schiefke, Joao Bana e Costa, Pascal Lecomte and Panos Kanavos in Medical Decision Making
Footnotes
Acknowledgements
We would like to thank all the participants of the decision conferences for their valuable input and feedback. Katie McClain provided excellent administrative and research support throughout the project. Huseyin Naci provided valuable advice on evidence synthesis. MT acknowledges the support of the NIHR Imperial Biomedical Research Centre. Finally, we are grateful to 3 anonymous referees for providing valuable comments and suggestions in an earlier draft of the paper. All outstanding errors remain our own.
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AA, AC, IS, and PK declare no conflict of interest. MT, VR, AO, and JBC declare honoraria from Novartis as reimbursement for their participation in the decision conference meetings that were part of work leading to this article. LS declares a grant from Gilead Sciences and consulting fees from AbbVie, Gilead Sciences, Novartis, Pfizer, Sanofi, and Theratechnologies Inc. PL is an employee of Novartis.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided by a research grant from Novartis. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report. The following author is employed by the sponsor: PL. The study sponsor did not have any influence on the design, evidence collection, or analysis of the study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.