
Abstract
Keywords
Understanding what matters to patients is critical in high-stakes clinical decisions. Treatment decisions can influence many aspects of a patient’s life beyond their clinical symptoms, including independence, emotional state, social interactions, and finances. While there is growing consensus that patients’ values should be incorporated into clinical decisions,1,2 there is little consensus on how this should be done. 3 Simply asking patients what they value is problematic, as people often do not have pre-formed ideas about what is important to them when confronted with complex or unfamiliar situations.4–6 Additionally, patients often have difficulty applying deeply held values to health decisions. 7
Values clarification exercises (VCE) aim to help patients determine what matters most to them when making a health decision.3,8 They are recommended components of patient decision aids (DAs) and can help patients choose treatments that are consistent with their values.3,9 The most common approach to values clarification is listing the pros and cons of options. 10 Other approaches include focused comparisons of the attributes of treatments and the outcomes affected, using mathematical models to assign weights to items (e.g., utility theory or stated preference approaches such as conjoint analysis, 11 best-worst-scaling, and discrete choice 12 ).
While much attention has been given to the mathematical models for assigning weights to a set of attributes and outcomes, less attention has been given to how those attributes and outcomes are selected. It is established that an individual’s values and preferences can be influenced, or even formed, by the way they are elicited; even small differences in rating procedures matter.13,14 Yet changing the attributes and outcomes discussed can shift the focus and trigger emotions, influencing how those outcomes are perceived and valued. 15
The task of selecting and organizing the attributes and outcomes to include in a VCE is most often entrusted to the developer or to expert physicians, often mirroring the outcomes reported in clinical trials or guidelines 16 or the values deemed important by the developer. However, clinical outcomes are often valued differently by patients and physicians, 17 and the inaccuracies of substituted judgment, when surrogate decision makers make decisions in lieu of the patient, have been well-documented.18,19 Thus, studies that ask patients to rate the wrong set of outcomes lack external validity.20–22
Focus groups and/or interviews are sometimes conducted to understand what matters to patients. However, extracting and prioritizing patient preferences from these discussions is difficult, subjective, and influenced by the investigator’s own perspectives. 23 Furthermore, interacting groups can inhibit creative thinking by pursuing a single train of thought for a long period, promoting premature evaluation, and inhibiting the participation of more passive members. In contrast, the nominal group technique (NGT) minimizes investigator bias, avoids focusing on a single train of thought, prompts participants to generate their own issues, captures the specific language of participants, maintains the autonomy of individual viewpoints, allows equal input by each participant, and objectively prioritizes findings.24–26 Card sorting exercises can capture how participants themselves organize ideas generated in an NGT, further minimizing investigator bias. Analyzing card sorting results using multidimensional scaling (MDS)27–29 and hierarchical cluster analysis (HCA) 30 can produce a visual “cognitive map” that facilitates obtaining input from stakeholders who lack statistical expertise. 31 This combination of NGT coupled with card sort exercises and MDS and HCA, referred to as “cognitive mapping,” has been applied in many areas, but not yet to inform the attributes included in VCE or DAs.
Our clinical focus is multiple sclerosis (MS), an immune-mediated disease of the central nervous system. 32 Choosing the best treatment for patients with MS has become more challenging because of the increasing number of disease-modifying treatments available (14 in 2017). 33 These treatments may differ in their effectiveness, side-effects, risks, costs, and method of administration. A search of the literature identified 5 studies and 1 DA that addressed MS treatment preferences,34–39 each using a different set of attributes and all but one 38 using investigator-selected attributes without specifying the selection process.
Our objective was to develop a patient-centered approach to identify the outcomes and attributes important to patients making a high-stakes medical decision regarding their MS. We sought to adapt cognitive mapping to compare the treatment goals of patients with MS to those of experienced MS healthcare providers (HCPs).
Methods
Sample
We included non-pregnant, English-speaking patients with any type of MS between the ages of 21 and 75 years, reflecting the epidemiology of MS. 40
All patient participants were identified through patient and HCP advisers with access to MS networks, using a purposive sampling design. To enhance the inclusion of disabled persons and increase geographic and racial diversity, we offered both online and in-person activities. In-person activities were conducted in handicap-accessible facilities in Denver and Colorado Springs, CO, Atlanta, GA, and Worcester, MA. Patient recruitment targeted diversity in age, duration of MS, race/ethnicity, education, and gender.
Our HCPs included neurologists, nurse practitioners, physician assistants, or registered nurses who manage 10 or more MS patients a month, using a combination of convenience and purposive sampling designs. HCP recruitment targeted diversity in gender, years of training, and type of provider.
Recruitment used snowball sampling through strategically placed ads, flyers, and invitations. Recruitment channels included MS support groups, educational events, professional organizations, health blogs, and private Facebook groups. Participants were invited to participate between April 2015 and February 2016.
Informed consent was obtained online or in-person for each study activity. This study was approved by the New England Independent Review Board.
Study Procedures
We used a multi-step cognitive mapping approach in which NGT meetings were used to elicit and prioritize treatment goals from patients and HCPs. A subsequent card sorting exercise, involving a larger sample, rated and clustered the prioritized goals. MDS and HCA were used to analyze card sort responses. NGT participants could elect to participate in subsequent card sorting activities.
Five to nine participants were assigned to each NGT group. Groups were led by an experienced moderator (NFC) and co-led by a locally respected peer. To standardize meetings across sites, instructions were provided through a series of instructional videos. Participants were asked to silently respond to one carefully worded question (pre-tested in cognitive interviews), writing down as many brief responses as they wished. Patients were asked “What do you specifically hope to achieve (or avoid), now and in the future, when you choose ways to manage your MS?” HCPs were asked: “What do you hope to achieve or avoid when you manage your patient’s MS?” Participants requiring assistance were paired with an assistant. Participants could submit sensitive topics anonymously. Next, in a round-robin, each subject read aloud one of their responses until all unique responses were recorded on a shared list. The moderator read any anonymous topics. Each item on the list was reviewed by the group for clarity and redundancy. Finally, participants were asked to silently identify and rank the 9 most important items (the maximum number that can be effectively ranked). 41
We developed a 2-step online NGT protocol that mirrored the in-person protocol. Participants could respond when and where they chose (asynchronously), spend as much time as needed, and complete the activity over multiple sessions. Instructional videos (identical to those shown during the in-person meetings) explained procedures. In step one, participants viewed the videos, read the NGT question, and submitted their responses. After all participants’ responses were submitted, the responses were consolidated independently by 2 facilitators (NFC, VS), involving another advisor to resolve any differences. In step two, 1 to 3 weeks later, participants were shown the consolidated list, asked if they agreed with the way items were combined and how they would like to change it. They were then asked to rate each item for clarity (“Is this concept clear?”, “How would you suggest it be improved?”) and redundancy (Is the item unique? If not, “which other item(s) should it be combined with?”), and then asked to rank the top 9 items.
After completing all NGTs (in-person and online), 2 consolidated lists of treatment goals were generated (1 for patients, 1 for HCPs) by carrying forward all prioritized items (receiving at least 1 point), combining items that conveyed the same meaning, and removing or rewording confusing items. MS patient and HCP advisers (BT, AH, MM, LQ, CG, AS) guided this process. We attempted to combine patient and HCP prioritized responses onto a single list, but many of the HCP items were unclear to patients.
The consolidated list of patient treatment goals was used for rating and card sorting among both patients and HCPs. Participants rated the importance of each goal by indicating the strength of their agreement or disagreement with each one, using a 5- or 10-point Likert scale (online v. in-person, respectively). Participants were then asked to use their own criteria (e.g., “how you see these items going together?”) to sort the 34 items into 3 to 10 groups containing any number of perceptually similar cards. 42 This was done either in-person using a shuffled deck of cards, or online, using customized Qualtrics software. Online participants were asked to label each group.
Data Analyses
Within each NGT meeting, weights were assigned to each ranked item (i.e., 9 points for the 1st, 1 point for the 9th) and scores from each participant were summed to develop an aggregated, prioritized list. Ratings conducted during the card sorting exercises were calculated using the mean and SD, and rescaled to a 10-point scale. Results of all of the online and in-person activities appeared similar and were combined (the online Appendix compares online and in-person findings).
Using customized software, the card sort data were transformed into a 34 × 34 co-occurrence matrix that recorded how often 2 items were sorted into the same group. MDS (“PROXCAL” software algorithm) was applied to the group co-occurrence matrix using Euclidean (i.e., straight-line) distances. MDS creates a visual “cognitive map” of the spatial relationships between the attributes that approximates the perceived similarity of items. The more often items were sorted into the same group, the closer they appeared in the diagram. The space can be multi-dimensional, but only 2-dimension solutions are interpretable. Goodness-of-fit is determined by the stress statistic (below 0.15 corresponds to a good fit).43,44
HCA (using Ward’s Linkage) was used to draw boundaries around groups of goals, demarcating conceptual clusters of related goals. A cluster tree (dendrogram) represents the distance between the clusters by the length of the branches. It illustrates potential clusters but not the actual number of clusters. Final clusters conformed to the dendrogram, using patient input to identify and label the most meaningful clusters (Appendix Figures 2A, 3A, and 4A). MDS and HCA are robust to violations of their assumptions. All analyses were performed using SPSS Statistics 23.
Results
Seventy-one participants took part in the study (47 patients, 24 HCPs; Figure 1). Our patient sample (Table 1) appears representative, as it resembles another representative study’s sample. 45 Our HCPs had an average of 10.5 years in practice (range, 1 to 32), 71% were female, and 42% were physicians (neurologists), 33% physician assistants, and 25% nurses or nurse practitioners. Forty-six percent of the HCPs who participated in the NGT meetings were affiliated with a MS Center, 31% reported seeing over 50 patients with MS each month, 62% between 11 and 50 patients, the remainder seeing approximately 10 patients/month.
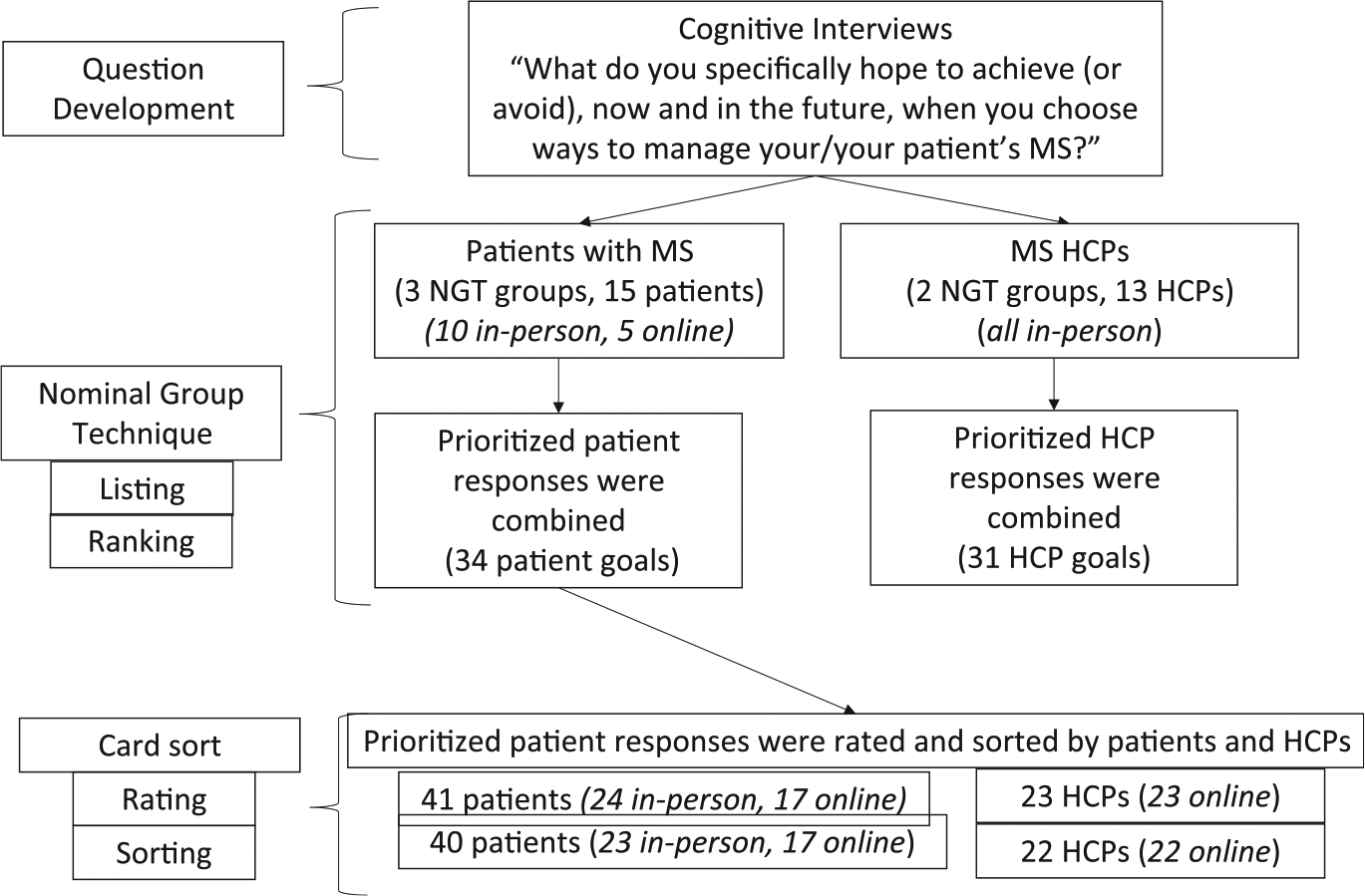
Study design and sample.
Patient Characteristics (n = 47)
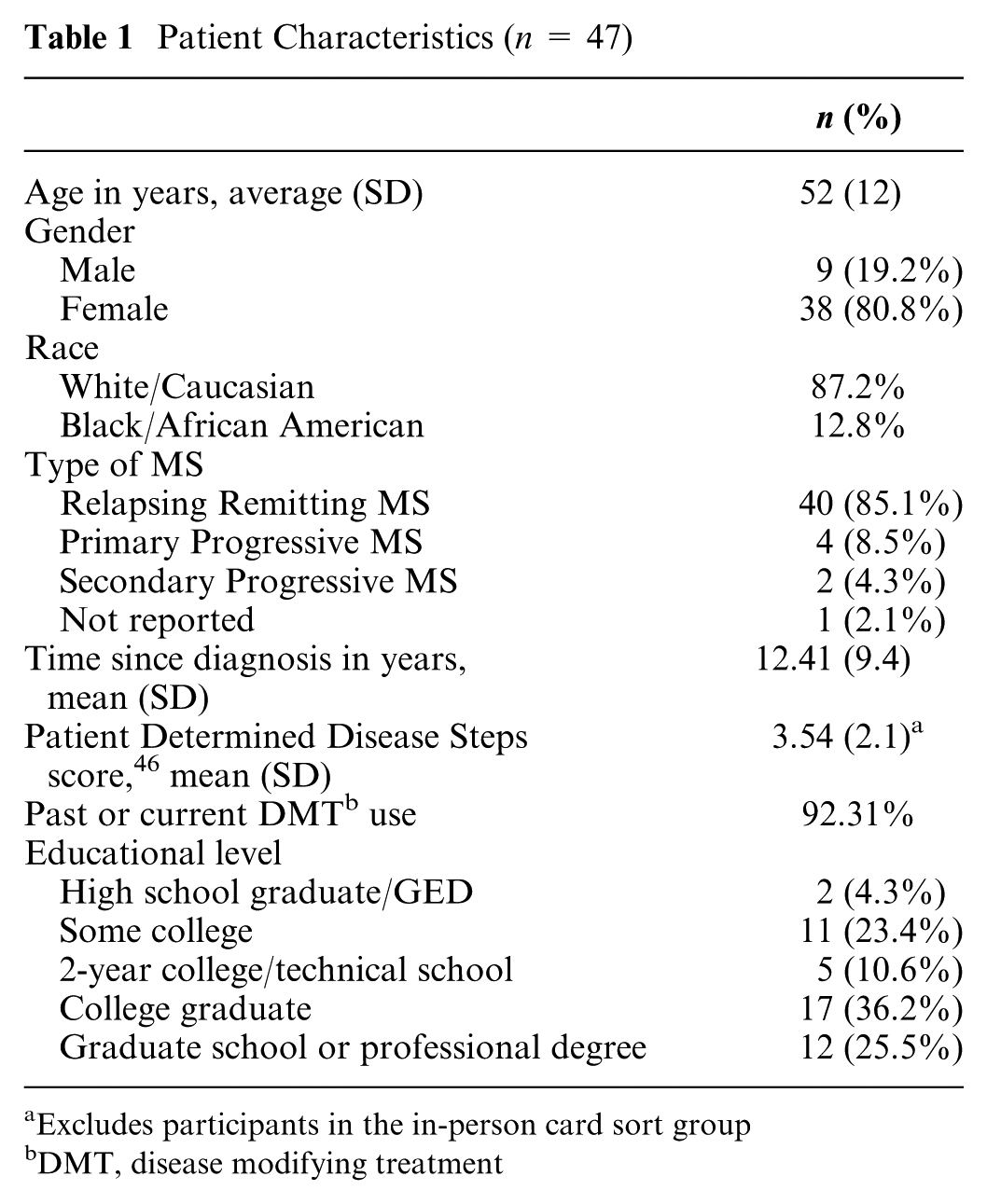
Excludes participants in the in-person card sort group
DMT, disease modifying treatment
Treatment Goals Generated by Patients and HCPs
All subjects who consented completed the NGT activities. Three patient NGT meetings (2 in-person, 1 online) generated 34 unique goals; 2 in-person HCP NGT meetings generated 31 unique goals. Many of the patient goals were not mentioned by HCPs and vice versa; in addition, differences in terminology were observed (Table 2). Among patients, maintaining bladder and bowel function was the most important symptom management goal, much more than managing pain. In contrast, HCPs endorsed pain more strongly than bladder and bowel function.
Top Ten Ranked Treatment Goals, Patient-Reported V. HCP-Reported (from 3 NGTs) a
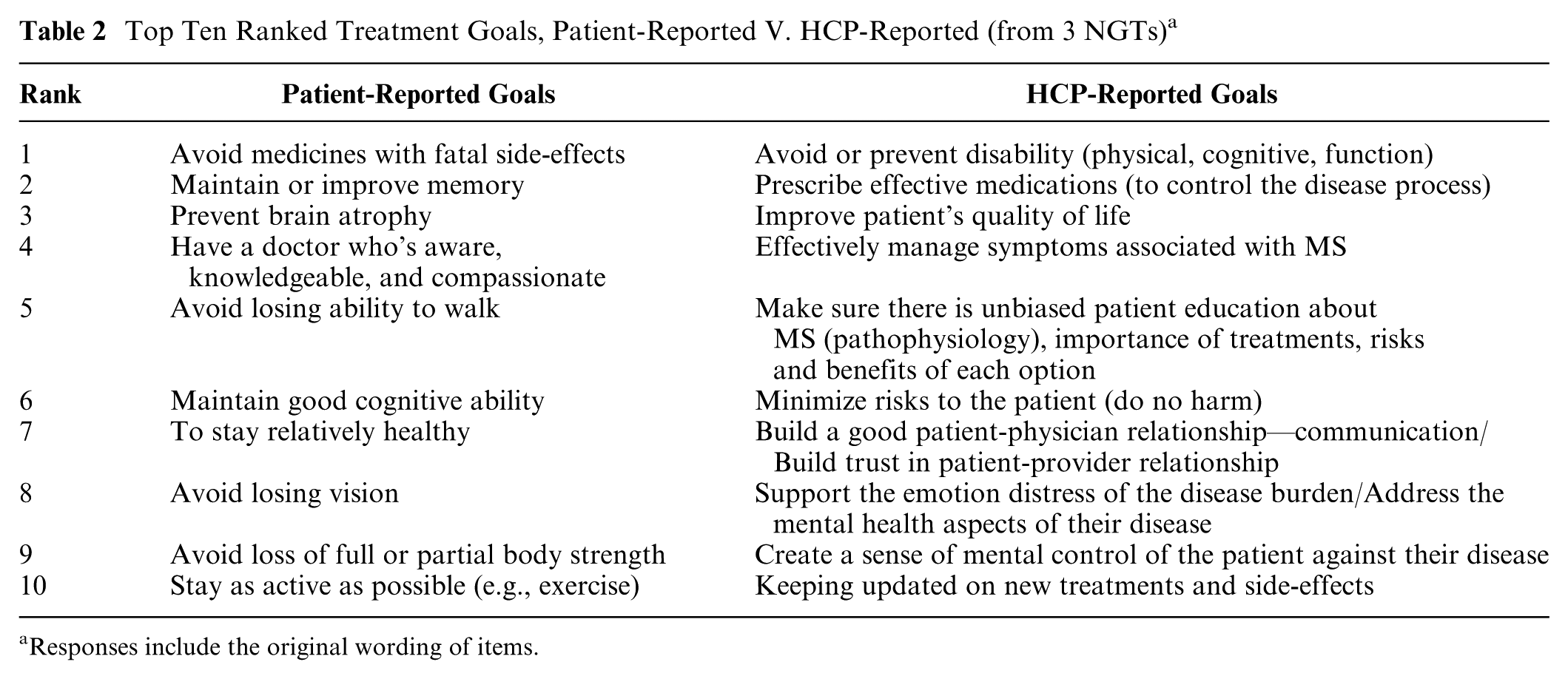
Responses include the original wording of items.
Ratings of Patient Treatment Goals
All subjects who consented to the card sorting exercise completed all ratings. Both HCPs and patients strongly endorsed most of the goals, HCPs more so than patients (mean ratings of 9.49 (0.58) and 8.83 (1.32), respectively; P < 0.05). “Avoiding medicines with fatal side effects” was the most endorsed goal for patients but one of the least endorsed goals for HCPs (Figure 2). The goals most similarly rated by patients and HCPs were “Maintain or improve memory,” “Prevent brain atrophy,” and “Stay relatively healthy.” Those with the greatest differences were “Avoid assistive devices,” “Stay working,” “Decrease pain,” and “Help with symptoms of depression,” which were more strongly endorsed by HCPs than patients.

Ratings of patients’ treatment goals. Patients v. HCPs (ranked according to differences in rating).
Cognitive Mapping
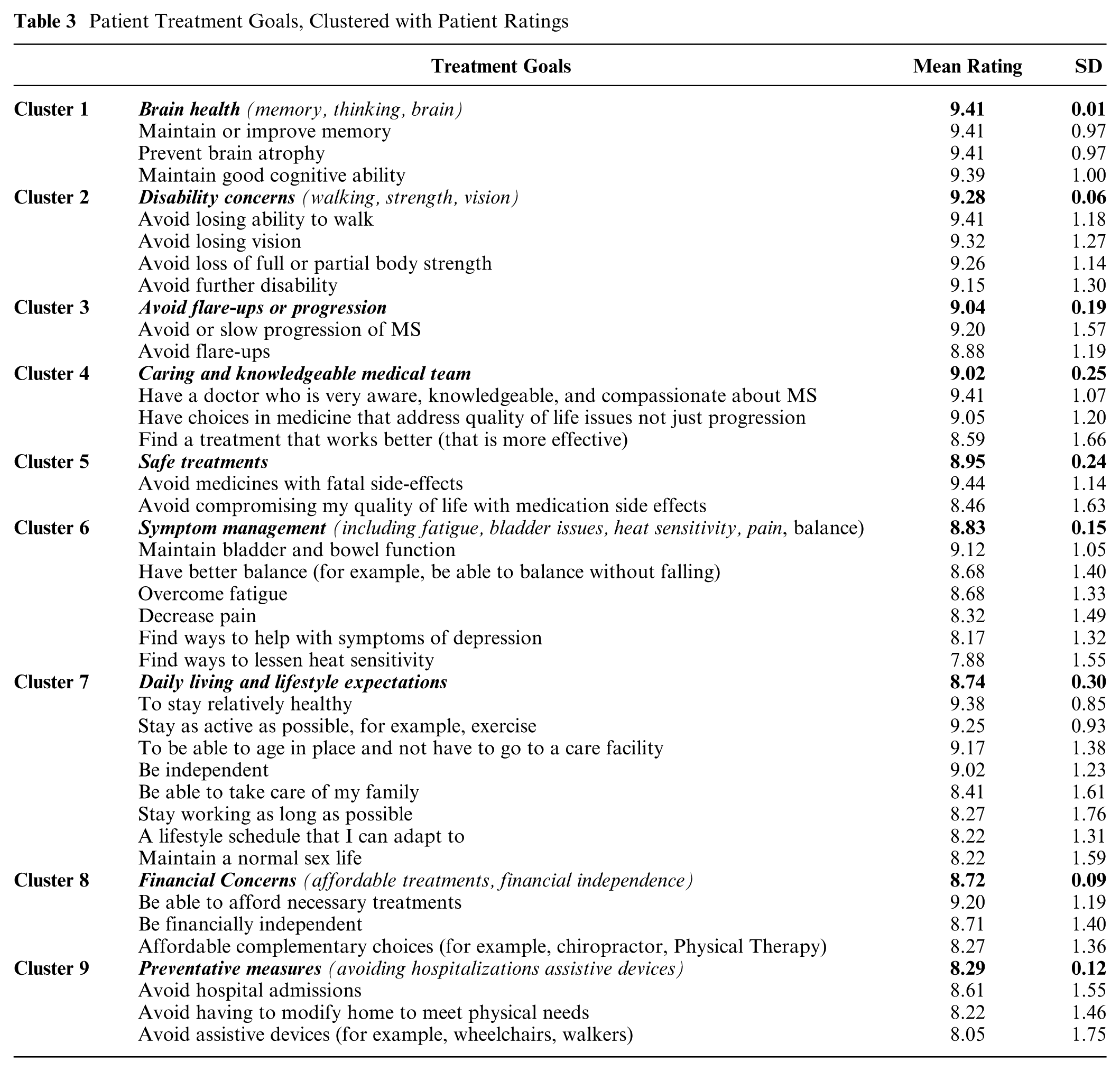
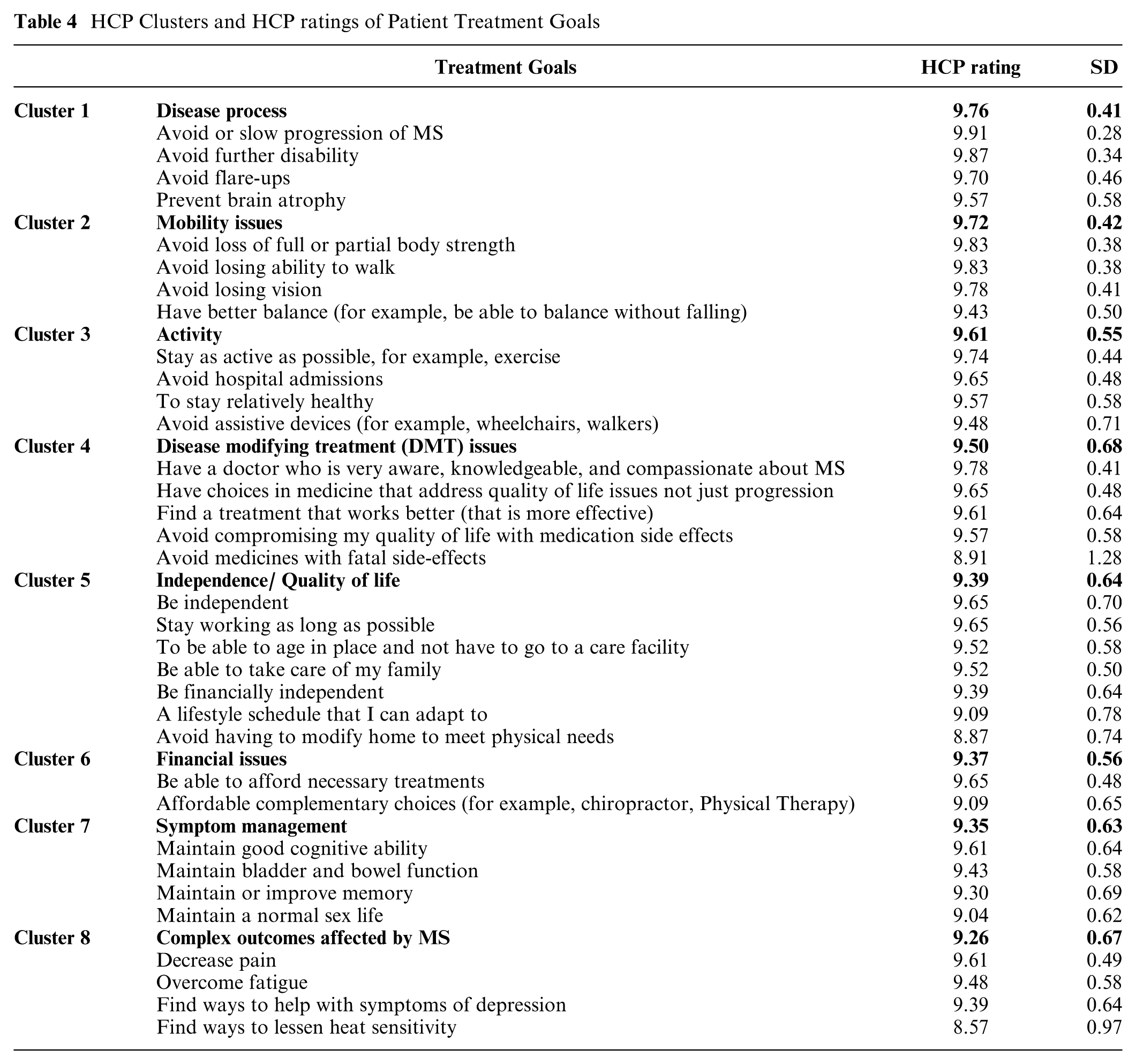
All but one person who consented to the card sorting activity completed the sorting (100% for the online sample, 95.8% for the in-person sample). The 2-dimensional solutions for the MDS analyses indicated robust goodness-of-fit measures for the patient, HCP, and combined models (stress = 0.0426, 0.0133, and 0.0319, respectively). Nine patient clusters and 8 HCP clusters were derived from the 34 patient treatment goals (Figures 3, 4; Tables 3, 4; Appendix Figure 4A). Our cluster analyses revealed areas of overlap between clusters; yet, none of the clusters were identical across the 2 cohorts. Among patients, the most important cluster was “Brain health,” followed by “Disability concerns.”
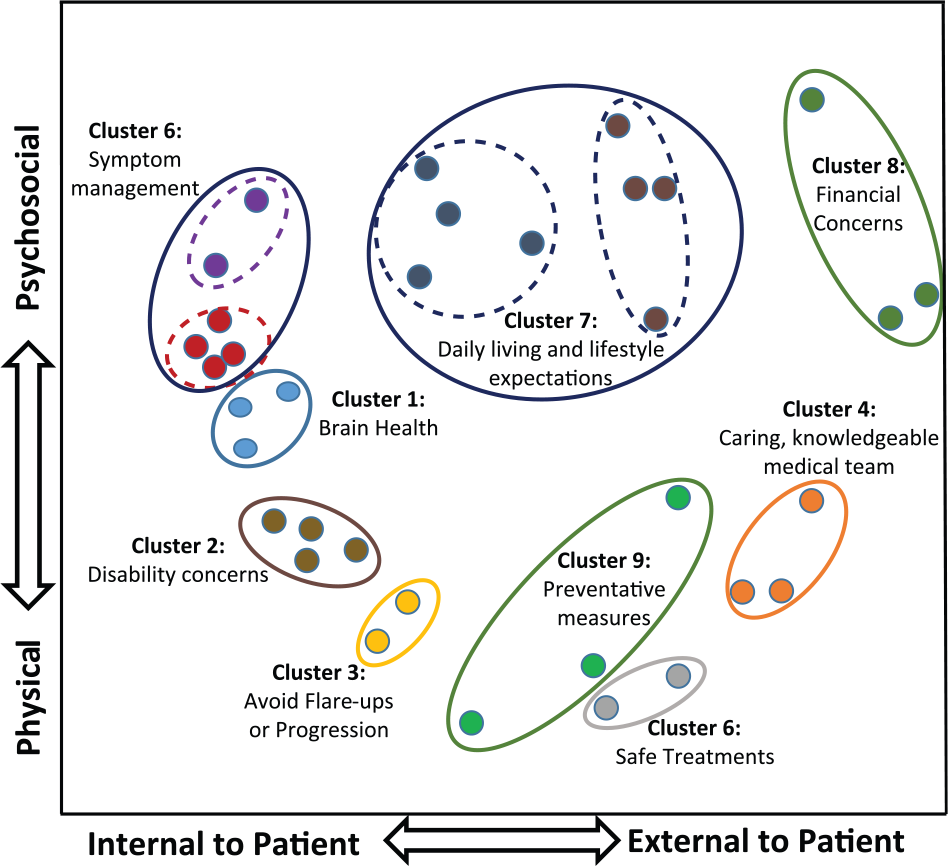
Patients’ cognitive map.
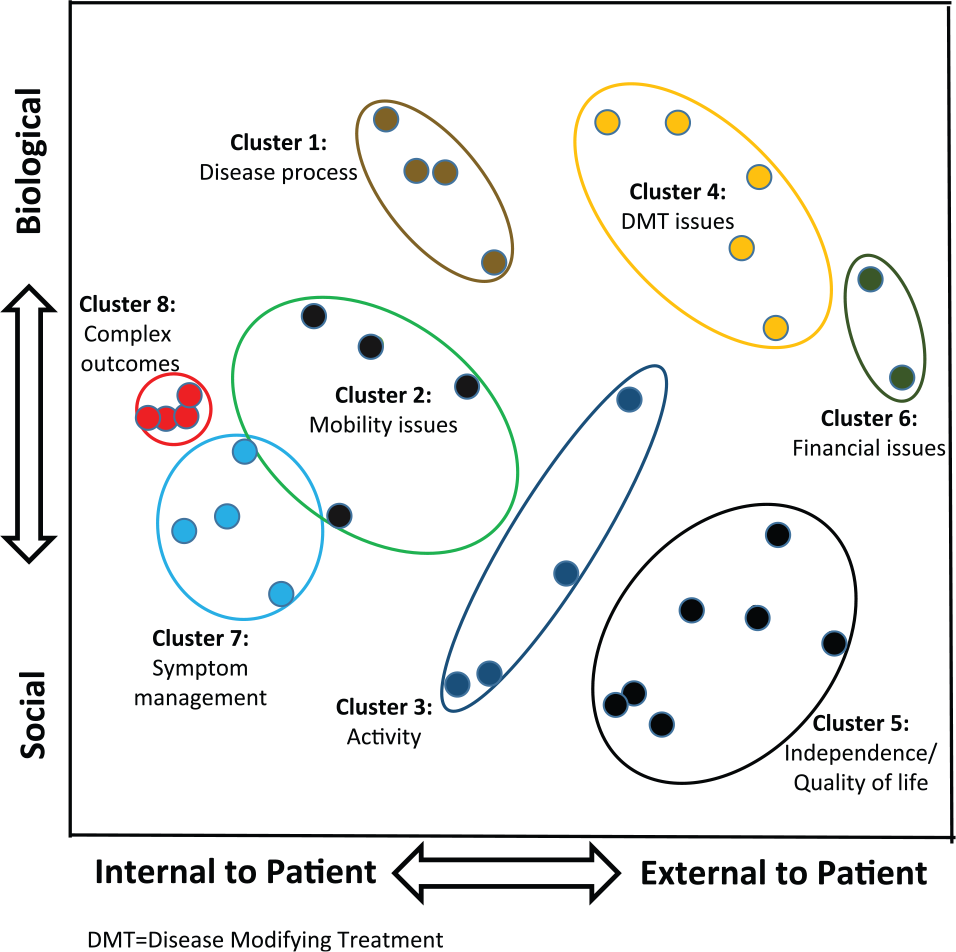
Health care providers’ cognitive map.
Patient Treatment Goals, Clustered with Patient Ratings
HCP Clusters and HCP ratings of Patient Treatment Goals
We interpreted one dimension of the patients’ cognitive map as ranging from factors internal to the patient to external to the patient; the other dimension, ranging from physical to psychosocial impact. We interpreted one dimension of the HCPs’ cognitive map as factors internal v. external to the patient; the other dimension, ranging from biological to social impact.
Discussion
We were able to adapt cognitive mapping techniques to identify and prioritize patient treatment goals and compare them to HCP goals. Our approach elicited a broad spectrum of goals directly from patient and HCP stakeholders and organized them into meaningful clusters with minimal investigator input. Many of the domains identified have not been previously reported, including “Brain health,” “Daily living and lifestyle expectations,” “Disability concerns,” “Preventative measures,” and “Medical team.” We also identified many specific preference attributes for MS that have not been previously identified, including prevent brain atrophy; avoid loss of strength; have a doctor who is very aware, knowledgeable, and compassionate; better balance; overcome fatigue; lessen heat sensitivity; be independent; maintain a normal sex life; stay working; avoid hospital admissions; avoid assistive devices; and age in place. Our identification of new domains could reflect the success of our methods or that few previous studies have asked patients themselves.
We found some differences between the treatment goals generated by patients and HCPs. Goals generated by patients more often involved improving specific day-to-day symptoms, whereas those generated by HCPs involved slowing disease progression. HCP goals appeared to reflect, in part, outcomes that they perceived they could influence with the medical interventions at their disposal. Improving conditions that were beyond their sphere of influence (e.g., heat sensitivity) were not offered by HCPs and also received lower endorsement ratings. HCPs’ stronger endorsement of pain may reflect the influence of the ‘Pain as the Fifth Vital Sign’ initiative. 47 However, because of the limited variation in HCP and patient ratings, we have less confidence in those findings.
Differences between how patients and HCP cohorts clustered treatment goals may reflect differing understandings of underlying disease processes. For example, HCPs grouped cognition and memory as symptoms along with bladder and bowel function, whereas patients grouped cognition and memory in a separate category along with brain atrophy.
HCPs used global constructs (e.g., quality of life) more frequently than did patients. Some of those global constructs could be loosely interpreted as encompassing many of the specific items that patients listed as distinct goals. However, relating the HCPs’ broad goals to the patient’s specific goals was impeded by differences in terminology and differences in the semantic meaning attached to the terms. Confusion about terms used to describe the clinical course of MS has been a recurring theme in the scientific literature on MS,48,49 with the meaning of terms such as “disability” and “progression” changing as the definitions of MS have evolved. Clinically, progression implies “progression of clinical disability,” reflected in HCPs’ grouping of “Avoiding further disability” with “Avoid or slow progression of MS,” “Avoid flare-ups,” and “Preventing brain atrophy”. In contrast, patients grouped “Avoiding further disability” with “Losing ability to walk,” “Loss of full or partial body strength,” and “Losing vision,” consistent with the lay definition of disability (conditions that limit a person’s movements). These differences underscore the potential problems with using HCP-identified instead of patient-identified goals. Moreover, because many of the terms used by patients convey a different meaning to HCPs, simply asking patients to share their goals with their HCP may not suffice to bridge communication gaps. To support shared decision making, patient goals may need to be explained to HCPs in different terms.
As the number of treatment choices for chronic diseases increases and the spectrum of clinical, functional, and economic outcomes affected by treatments increase, so do the challenges of selecting the best outcomes and attributes for inclusion in VCE and DAs. Guidance for developing DAs concluded that there is no consensus on how to select material for inclusion in DAs, recommending “needs assessment via focus groups and literature review, and direct observations of clinical interactions during office visits.” 50 Yet those traditional approaches are themselves prone to investigator bias. 24 Further, relying on a literature review can propagate errors if those published studies did not involve patients. A systematic review of patient priorities for practice care reported that 25% of the published studies included items that were “invented by the researchers,” 44% were “unclear,” and 23% were sourced from other literature. 51 VCE that do not include the attributes that matter to the decision maker will produce unreliable results. No amount of finesse or mathematical sophistication in comparing items can compensate for choosing the wrong set of outcomes. There is a pressing need to both standardize and increase the transparency of the process used to select the outcomes and attributes included in DAs and VCE. This approach addresses the issue of how to select attributes, by minimizing the influence of the researcher and allowing selections to be made by the patients.
Our study had several limitations. Comparisons of patients with HCPs was hindered by a small HCP sample. However, because MDS and HCA are not based on parametric statistics, their validity is not dependent on the size of the sample but rather on the representativeness of the participants. 47 Differences in treatment goals might be expected because HCPs were asked about their treatment goals, not patients’. However, because expert physician opinion is commonly used to identify attributes, this seemed the most meaningful approach. HCPs highly endorsed all goals, rendering differences in importance ratings less meaningful. We combined findings from online and in-person activities, recognizing that the method of collecting responses likely had some influence on those responses. The labels assigned to the dimensions identified by MDS are speculative, as are our interpretations of differences between groups. 52 This method minimizes researcher bias but does not eliminate it. Judgment and investigator input were needed to combine lists across NGTs, select the number of clusters, and interpret findings. Our protocol minimized these influences by involving non-HCP and patient advisers in all steps.
The disadvantages of traditional NGT meetings include constrained time for responding, variations in the protocol across groups, and the suppression of sensitive topics (due to round-robin reporting). The adaptations developed for this study minimize those challenges by including a protocol for the anonymous submission of topics, videos that standardize the protocol across groups, and asynchronous online activities that support more inclusive sampling and thoughtful responses by removing time limits.
Tailoring discussions about treatments to reflect outcomes of importance to the decision maker is essential to shared decision making.53,54 But the critical and often missing first step is identifying those outcomes. The patient-centered cognitive mapping approach described in this manuscript could be used to improve the validity of VCE and stated preference methods by improving the process for selecting the attributes that they include, increasing the transparency of the attribute development process and resulting in a more appropriate set of attributes. This approach could also be used to guide the content of DAs, tailor behavioral change interventions, and improve patient–provider communication. Knowing what matters to a patient could assist HCPs in understanding their patients, help build more trusting relationships, identify treatments that are a better fit for that patient, and focus on the pros and cons of treatments that are most important to the patient, thereby reducing information overload and promoting patient engagement.
The NGT is beginning to be used to understand patient preferences for MS treatments. The first study using NGTs (combined with best–worst scaling) among patients with MS was published in late 2016, 55 focusing on attributes of disease-modifying drugs.
The findings from this study have been used to develop and validate a preference assessment tool to help patients with MS explore and share their goals with their HCP. (This is available at Available at https://tinyurl.com/WhatMattersMS.) This tool is currently being expanded into a shared decision making tool for MS and will be evaluated in real-world settings. While we have focused on MS treatment goals in this study, the approach is applicable to other preference-sensitive clinical decisions. Helping patients better understand their treatment goals and making HCPs aware of their goals should improve patient-provider communication and promote shared decision making.
Footnotes
Acknowledgements
We gratefully acknowledge the contributions of Linda Quigley and Marlene McDaniel.
Financial support for this study was provided by Biogen by a contract with Five Islands Consulting LLC. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report. The following author is employed by the sponsor: Glenn Phillips, PhD.
Biogen reviewed the manuscript and provided feedback to the authors. Authors had full editorial control and approved the final content. NFC is founder and president of Five Islands Consulting LLC, which has also received consultant fees from EmmiSolutions, LLC, Epi-Q, Synchrony Group, 3D Communications, Janssen Scientific Affairs, LLC, Jazz Pharmaceuticals, AcelRx Pharmaceuticals, Inc, Astra-Zeneca and unrestricted research support from Pfizer.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.