
Abstract
The study explores whether physical activity (PA) in early adolescence limits the risk of internalizing and externalizing problems in youth with difficult temperaments, from low-income families, or exposed to impaired family functioning. Participants (N = 1312; 53% girls) were drawn from the Quebec Longitudinal Study of Child Development (QLSCD). Results revealed that difficult temperament was associated with subsequent symptoms of anxiety among youth with low PA levels. Impaired family functioning was associated with higher levels of subsequent physical aggressivity among youth with high levels of PA. These results highlight the complex role of PA in different aspects of adjustment and the importance of the quality of PA contexts in young adolescents exposed to family adversity.
Up to one-third of children and adolescents are at risk for developing adjustment problems (Danielson et al., 2021). Adjustment problems generally fall into two categories, including internalizing and externalizing problems (Gniewosz & Gniewosz, 2020). Internalizing problems refer to internal distress and include depressive and anxiety symptoms (Cosgrove et al., 2011). Specifically, depressive symptoms comprise negative emotions such as sadness and worthlessness (American Psychological Association, 2017a). Anxiety symptoms are primarily characterized by worrisome thoughts, as well as feelings of panic and fear (American Psychological Association, 2017b). Externalizing problems are directed toward the external environment and include problems such as physical aggressivity and hyperactivity-inattention (Cosgrove et al., 2011; Gniewosz & Gniewosz, 2020). Physical aggressivity refers to actions that can cause pain to others and include behaviors such as pushing, hitting, and kicking (Coie & Dodge, 1998). Hyperactivity-inattention problems refer to excessive motor activity, concentration difficulty, and distraction when performing tasks (Meinzer et al., 2018).
Although some of these problems might emerge early in childhood, they can also become more pronounced during the transition from primary to secondary school, which is characterized by multiple physical, emotional, and environmental changes occurring between the ages of 10 and 14, depending on the country and education system (Evans et al., 2018; Harris & Nowland, 2021). In Quebec, this school transition typically occurs around 12 years old, between the end of grade six and the beginning of grade seven, which respectively occur in a primary and a secondary school. The changes associated with this transition result in young adolescents simultaneously undergoing puberty, having to deal with higher school workload, and get acquainted with unfamiliar peers and teachers within a larger school environment involving multiple teachers and classes (Harris & Nowland, 2021). While some young adolescents cope successfully with these changes, others encounter negative experiences possibly leading to an increased risk of internalizing and externalizing problems (Harris & Nowland, 2021).
Besides the distress it generates, young adolescents experiencing internalizing and externalizing problems also face increased risks of having lower engagement and achievement, difficulty establishing quality relationships with their families and peers, and lower self-esteem (Luijten et al., 2021; Olivier et al., 2020). To prevent these negative consequences, some theoretical frameworks such as developmental psychopathology models highlight the importance of identifying early risk factors associated with the emergence of internalizing and externalizing problems, as well as protective factors mitigating their impacts that are amenable to intervention (Lewis & Rudolph, 2014). Well-established biological and environmental risk factors, namely difficult temperament (e.g., high negative reactivity, low self-regulatory skills) and family adversity (e.g., negative environmental experiences), contribute to the emergence of both types of problems (Devenish et al., 2017; Forbes et al., 2017; Hughes et al., 2017; McQuillan & Bates, 2017; Simpson et al., 2018; Thomas & Chess, 1977). Considering their precocity and general stability, it is important to identify intervention targets that have the potential to mitigate these risk factors (Dunn et al., 2011; Wadman et al., 2020). Physical activity (PA) practice appears to be a promising avenue, given its many well-known benefits on psychosocial adaptation (Biddle et al., 2019; Panza et al., 2020).
Difficult Temperament and Family Adversity: Risks for Internalizing and Externalizing Problems
Temperament represents innate individual differences in emotional and behavioral responses that emerge early in childhood and remain generally stable throughout development (Clauss et al., 2015). Young adolescents with difficult temperaments are at greater risk of displaying maladaptive emotional and behavioral responses, as evidenced by their important mood changes, lower attention span, and greater distractibility (McQuillan & Bates, 2017; Thomas & Chess, 1977). These behaviors can increase their risk of developing depression as well as anxiety symptoms and hyperactivity-inattention problems (Forbes et al., 2017), as also suggested by the vulnerability model (Tackett, 2006). Even when assessed early in life, difficult temperament continues to affect the development of young people into early adolescence (Forbes et al., 2017).
Family adversity requires significant adjustment by youth and is associated with subsequent physical and mental health problems (Hughes et al., 2017; McLaughlin, 2016). Family adversity can be conceptualized and measured in different ways, the most common being through cumulative exposures to various forms of family risks (Lacey & Minnis, 2020). These cumulative indicators are based on the premise that adverse childhood experiences in different life domains are more difficult to manage than challenges in one life domain (Lacey & Minnis, 2020). In a widely cited study, Felitti et al. (1998) created a cumulative risk score index of family adversity by combining seven indicators of family adversity including different types of abuse (e.g., physical, verbal) and several forms of family dysfunction (e.g., parental psychopathology). This indicator was associated with risky health behaviors (Felitti et al., 1998). Several recent studies corroborated these findings by showing that individuals who experienced four or more forms of adversity had poorer health and psychological outcomes than those experiencing fewer forms of adversity (Hughes et al., 2017; Vig et al., 2020).
Despite the usefulness of the cumulative approach and its ability to identify individuals most at risk of developing difficulties, it has a few limitations (Lacey & Minnis, 2020). First, the cumulative risk score index does not distinguish the specific influence of different types of adversity on young adolescent development (Lanier et al., 2018; McLaughlin & Sheridan, 2016). For example, early experiences of material deprivation are strongly associated with later cognitive functioning, whereas other indicators of adversity such as domestic violence are associated with emotional adjustment (McGinnis et al., 2022). Second, the cumulative risk score index does not allow for an understanding of the underlying mechanisms explaining how separate and combined indicators of family adversity affect development (Lanier et al., 2018). To address these limitations, some authors suggest studying indicators of family adversity separately (Lacey & Minnis, 2020).
Low family income and impaired family functioning are the most important indicators of family adversity (Masarik & Conger, 2017; Scully et al., 2020; Walsh et al., 2019). Low family income implies limited access to financial and human resources (e.g., education; Diemer et al., 2013; Peverill et al., 2021). Youth growing up in low-income families are more likely to experience hardship and present lower educational, social, and mental health outcomes (Devenish et al., 2017; Reiss et al., 2019). Impaired family functioning refers to the widespread presence of conflicts and tensions, which interferes with various dimensions of family life, such as communication and problem-solving (Epstein et al., 1983). Adolescence can trigger or exacerbate difficulties in family functioning. The growing need of adolescents for autonomy and independence requires significant adaptations on the part of parents, without which daily interactions can become strained (Soenens et al., 2019).
Low family income and impaired family functioning are well-documented risk factors for depression and anxiety symptoms, as well as for physical aggressivity and hyperactivity-inattention problems in young adolescents (Devenish et al., 2017; Simpson et al., 2018). In this line, the family stress model suggests that economic hardship, defined as low income and impaired family functioning (e.g., harsh parenting), impacts child well-being and, over time, increases the risk of developing internalizing and externalizing problems in young adolescents (Landers-Potts et al., 2015; Masarik & Conger, 2017).
It is essential to identify effective strategies to support resilience to limit the long-lasting risks that difficult temperament and family adversity pose for young adolescent adjustment. Psychological treatment is the typical form of support offered (Weersing et al., 2017). However, it is costly, not easily accessible, and its effects are potentially diminished by stressful life events often experienced by youth with difficult temperaments and living in adverse family contexts (Gau et al., 2012). Models of resilience suggest that engagement in positive and accessible activities may reduce internalizing and externalizing problems in youth with difficult temperaments or exposed to family adversity (Belcher et al., 2021). The practice of PA represents one of these positive activities likely to support resilience in the face of individual and contextual difficulties.
The Protective Role of PA
PA corresponds to bodily movements resulting in increased energy expenditure (Rhodes et al., 2017). Moderate to vigorous PA should average 60 minutes daily for youth transitioning from primary to secondary school (Bull et al., 2020). When practiced according to these recommendations, PA is associated with physical and mental health benefits (Biddle et al., 2019; Bull et al., 2020; Lubans et al., 2016). Despite these benefits, PA tends to decline during early adolescence (van Sluijs et al., 2021). The insufficient time devoted to PA is particularly pronounced in some individuals, including vulnerable children and adolescents (Vandermeerschen et al., 2015). Limited access to PA is problematic, as its practice could be even more beneficial for these youth compared to their more advantaged peers (Vandell et al., 2015). Different physiological and psychosocial mechanisms explain these benefits.
At the physiological level, PA allows better regulation of the hypothalamic-pituitary-adrenal axis, one of the body’s main biological stress systems (aan het Rot et al., 2009; Anderson & Shivakumar, 2013). This better regulation weakens the body’s reaction to physical and mental stressors (Anderson & Shivakumar, 2013; Brosse et al., 2002). Greater tolerance to stressors in turn may reduce depressive and anxiety symptoms (Anderson & Shivakumar, 2013; Brosse et al., 2002). PA practice also releases the norepinephrine, dopamine, and serotonin hormones and decreases blood pressure (Malhotra, 2019; Wigal et al., 2013). The latter functions are involved in improving executive functions and impulse control, leading to a reduction in behaviors typically associated with aggressivity and hyperactivity-inattention (Verburgh et al., 2014; Vysniauske et al., 2020; Wigal et al., 2013).
At the psychosocial level, PA practice, especially in an organized setting, promotes resilience in vulnerable youth, according to the Positive Youth Development framework (PYD; Hermens et al., 2017; Holt et al., 2017). PYD is an approach that focuses on the potential of positive social experiences to support youth positive development, by enabling the development of the 5Cs: connection, competence, confidence, character, and caring (Lerner et al., 2005). PA is one of those positive social experiences that, above all, help to strengthen bonds, confidence, and competence (Holt et al., 2017). These three components of the 5c model help to reduce negative emotions especially present in youth with difficult temperaments, from a low-income family, or exposed to impaired family functioning (Super et al., 2018). The quality relationship with the coach or a significant adult established through the practice of PA helps develop life skills. Personal (e.g., self-regulation, problem-solving) or social (e.g., obeying rules, self-control) life skills can then be transferred to other more challenging life contexts allowing youth to thrive (Gould & Carson, 2008; Holt et al., 2017). For example, social skills learned through PA may contribute to the reduction of externalizing problems in youth exposed to family adversity, while self-regulation skills may contribute to the reduction of internalizing and externalizing problems in youth with difficult temperaments. Overall, PA offers a context possibly mobilizing some key components of the 5Cs, which can contribute to preventing internalizing and externalizing problems in youth with difficult temperaments, coming from a low-income family, or exposed to impaired family functioning, although this question remains to be formally assessed.
Besides, social relationships and the life skills learned through PA are especially important during the transition from primary to secondary school. These acquisitions can contribute to reducing the anxiety felt by young adolescents, while also bolstering their sense of belonging to the school, two crucial elements for reducing the elevated risk of internalizing and externalizing problems found during the school transition (Coffey, 2013; Evans et al., 2018). Moreover, considering the many changes associated with this period and the decline of PA, it becomes important to support its practice considering the benefits it could have for vulnerable young adolescents transitioning from primary to secondary school (Vandell et al., 2015).
In addition to mechanisms supported by theory, empirical studies highlight several physiological and psychosocial mechanisms by which PA could help reduce problems in vulnerable adolescents. For example, Shorter and Elledge (2020) showed that truancy was reduced among low-income, rural Appalachian adolescents from cohesive families in grades 9 to 12 when they participated in extracurricular activities that included PA. However, involvement in these extracurricular activities increased substance use among youth living in high-conflict families considering their greater affiliation with deviant peers (Shorter & Elledge, 2020). Also, Sigfusdottir et al. (2011) results suggest that PA can limit symptoms of depression in adolescents in grades 9 and 10 exposed to a high level of family conflicts. Despite these encouraging results, these studies are cross-sectional and based on non-representative samples of the target population, warranting further investigation. Furthermore, they focused on the protective role of PA primarily with one form of family adversity, namely family conflict, without considering other important forms of adversity and individual risk factors including low income and difficult temperament, respectively.
Study Aims and Hypotheses
A preliminary aim of this study is to examine the association between difficult temperament, low family income, impaired family functioning, and subsequent internalizing (i.e., depression, anxiety) and externalizing (i.e., physical aggressivity, hyperactivity-inattention) problems in young adolescents undergoing the transition from primary to secondary school. The second main objective is to examine whether practicing PA protects adolescents exhibiting difficult temperaments or exposed to family adversity from subsequent internalizing and externalizing problems. More specifically, we first anticipate that childhood difficult temperament at 17 months old, low family income, and impaired family functioning at 12 years old will be associated with higher levels of depressive and anxiety symptoms as well as physical aggressivity and hyperactivity-inattention problems at 13 years old. Second, consistent with a protective effect, we expected that among youth with a difficult temperament or exposed to both forms of family adversity, those practicing a high level of PA will report lower levels of internalizing and externalizing problems at 13 years old, compared to those reporting lower levels of PA.
Method
Participants
The participants in this study come from the Quebec Longitudinal Study of Child Development (QLSCD) launched by the Institut de la Statistique du Québec (ISQ) in 1997–1998. This study includes families from several regions of Quebec, excluding those from Northern Quebec, given the greater distance between these territories and the data collection centers, and the lower population density. Initially, 2940 children aged on average 5 months old were selected from a provincial birth registry, using random sampling, stratified by region. Several attempts were made to reach the selected participants, starting with telephone contact, followed by home and neighbors visits. Of the 2940 participants contacted, some families could not be found (172). In addition, even when an initial contact was established with some other families, 93 participants could not be included in the study for the following reasons: families already participating in another longitudinal follow-up (5), families who spoke neither French nor English (81) and whose infants suffered from physical or mental disabilities (2) for which no instrument was adapted, and death of the infant (5). Thus, only 2675 families were invited to participate in the study and, of this number, 2223 (83%) gave their active consent to participate in the initial data collection. Of those, 2120 children were eligible for the longitudinal follow-up. During this follow-up, families were recontacted annually throughout the winter and spring months, until target children reached 13 years old in 2011 (except in 2007 and 2009).
The present study focuses on the data collected at 12 and 13 years old, that is, before and after the participants transitioned to secondary school. The subsample used for the study thus includes the 1312 youth (53% female and 47% male) who were still participating in the project at 12 years old. To capture background risks, the current study also uses data collected when participants were 17 months old. To account for attrition, we used sampling weights derived for this subsample (Perret et al., 2020; Scardera et al., 2020).
Procedures
At each wave of data collection, parents provided informed consent by signing a form approved by the ethics committee of the Département de la santé de l’ISQ. Data was collected through different means, including interviewer- and self-administered paper and computerized questionnaires. Mothers reported their child’s temperament and the material situation of their family through a computerized questionnaire completed by an interviewer. Mothers also provided the level of family functioning via a self-administered questionnaire. Youth reported information about their PA level and their symptoms of depression, anxiety, hyperactivity-inattention, as well as their level of physical aggressivity problems using a computerized questionnaire completed by the interviewer (for PA) or directly read and completed by youth (for symptoms of depression, anxiety, hyperactivity-inattention, and physical aggressivity).
Measures
Difficult Temperament (17 Months Old)
Mothers rated the degree to which their 17-month-old child displayed signs of a difficult temperament with a subset of six items from the Infant Characteristics Questionnaire (ICQ; Bates et al., 1979). These items (α = .79; e.g., “How easy or difficult is it for you to calm or soothe … (name) when he/she is upset?”) were rated on a 7-point response scale ranging from 1 (easy temperament) to 7 (difficult temperament). The final scores were standardized on a scale ranging from zero to 10 with high scores indicating higher levels of difficult temperament, a standard procedure applied across the QLSCD study by the ISQ to facilitate comparisons across scales and across time.
Family Adversity (12 Years Old)
Family functioning was assessed with items from the McMaster Family Assessment Device (FAD; Epstein et al., 1983). The measure included seven items (α = .83; e.g., “We can express feelings to each other”), rated on a 4-point response scale ranging from 1 (strongly agree) to 4 (strongly disagree). To differentiate between healthy and impaired family functioning, the sum of these items was dichotomized with values lower than one standard deviation (SD) below the mean referring to healthy family functioning (0) and values equivalent or greater than one SD above the mean referring to impaired family functioning (1). Low family income was reported by the mothers when their children were 12 years old and is based on a reference threshold corresponding to 50% of the median after-tax income of all individuals in Quebec (Paquet, 2002). An individual above this threshold is considered to have sufficient income (0) and an individual below this threshold is considered to have insufficient income (1).
PA (13 Years Old)
The duration, or the number of minutes and hours per day, of organized or unorganized PA, was reported by youth with the following item: “In general, on a typical day, how much time do you spend doing these [organized/unorganized] physical activities?” PA was rated on a 7-point response scale ranging from 1 (less than 10 minutes per day) to 7 (2h00 or more per day).
Internalizing Problems (13 Years Old)
Internalizing problems were measured at 13 years old using two separate scales: depressive and anxiety symptoms. Young adolescents rated their depressive symptoms on 12 items (α = .83; e.g., “Choose the sentence that best describes you: I don’t feel alone; I often feel alone; I always feel alone”) from the Children Depression Inventory (CDI; Kovacs, 1985), rated on a 3-point response scale ranging from zero (the symptom is not present) to 2 (the symptom is present and marked). Youth rated their anxiety symptoms in the past six months with four items (α = .76; e.g., “I am nervous, high-strung or tensed”) from the Social Behavior Questionnaire (SBQ; Tremblay, 1991), rated on a 3-point response scale ranging from 1 (never or not true) to 3 (often or very true). For the two internalizing scales, the final scores were rescaled to range from zero to 10 with high scores indicating higher levels of depressive and anxious symptoms, as done with most scales in the QLSCD.
Externalizing Problems (13 Years Old)
Externalizing problems were measured at 13 years old using two scales: hyperactivity-inattention and physical aggressivity problems. These two scales came from the SBQ (Tremblay, 1991). Youth rated their hyperactivity-inattention problems level in the past six months on a 7-item scale (α = .79; e.g., “I am easily distracted. I have trouble sticking to any activity”), rated on a 3-point response scale ranging from 1 (never or not true) to 3 (often or very true). Youth also rated their physical aggressivity in the past six months on a 3-item scale (α = .66; e.g., “I physically attack people”), rated on a 3-point response scale ranging from 1 (never or not true) to 3 (often or very true). The two externalizing problems scales were standardized using a scale ranging from zero to 10, with high scores indicating higher levels of hyperactivity-inattention symptoms and physical aggressivity.
Preexisting Control Variables
Key individual characteristics that could confound the associations between the predictors and outcomes were considered in the analysis: sex (0 = girl; 1 = boys), baseline PA duration, and internalizing and externalizing problems at 12 years old. For the latter three variables, the scales were the same as those used at 13 years old, described above.
Data Analytic Strategy
All analyses were performed using IBM SPSS Statistic 27. Descriptive statistics and Pearson correlations were conducted to examine the associations between study variables. Rates of missing data ranged from 1.1% to 27.7% for predictors at 17 months old and 12 years old, 28.6% for the moderator variable at 13 years old, and 6.3–6.4% for outcomes variables measured at 13 years old. Missing data were managed using multiple imputations (20 imputed datasets). Regarding the main research questions, four separate sets of models of stepwise multiple linear regressions were assessed: a first set predicted depressive symptoms, second anxiety symptoms, third hyperactivity-inattention problems, and fourth physical aggressivity problems at 13 years old. In each set of models, we first regressed outcomes variables at 13 years old on covariates (sex, baseline PA, internalizing, and externalizing problems). Then, in a second step, we added the main predictors (difficult temperament, low family income, and impaired family functioning). In the third and fourth steps, we respectively added the moderator (PA) and the two-way interactions between the predictor variables and PA (mean-centered temperament X mean-centered PA, low family income X mean-centered PA, impaired family functioning X mean-centered PA). The interaction terms were examined separately in each set of models. Continuous predictor and moderator variables were mean-centered as recommended by Kraemer and Blasey (2004), thus reducing the risk of multicollinearity between the predictors and the interaction terms (Aiken & West, 1991; Kraemer & Blasey, 2004). Statistically significant interactions were interpreted by examining the simple slopes depicting the effect of the predictor at different levels of the moderators (−1 SD, +1 SD).
Results
Descriptive Statistics and Correlations Between Study Variables.
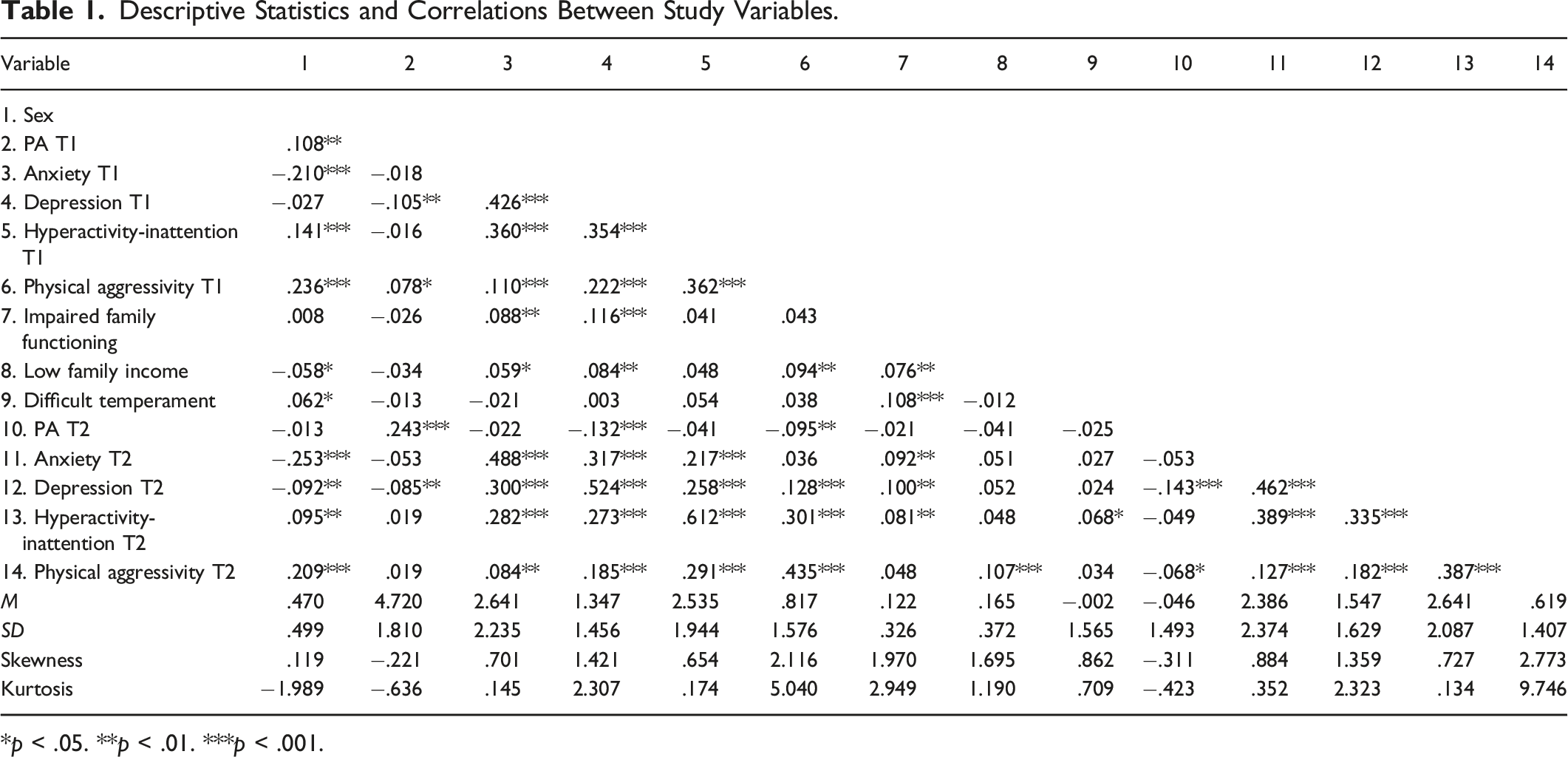
*p < .05. **p < .01. ***p < .001.
Family Adversity and Difficult Temperament and Depressive and Anxious Symptoms in Youth (T2): Main Effects and Direct Effects With PA at 13 Years Old.
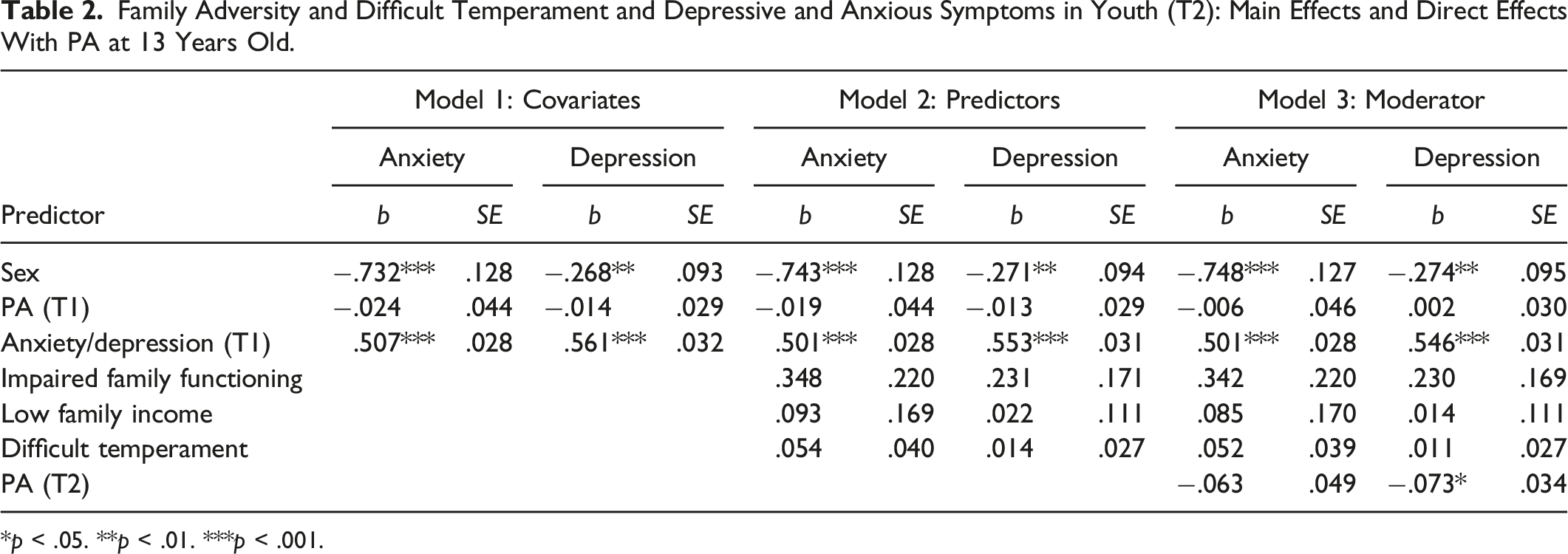
*p < .05. **p < .01. ***p < .001.
In a set of final models, we added the two-way interactions between the main predictors and PA at 13 years old. The two-way interaction between impaired family functioning and PA at 13 years old was not significantly associated with depressive and anxiety symptoms (b = .179, p = .104; b = −.154, p = .305, respectively). Similarly, the two-way interaction involving low family income and PA at 13 years old was not associated with depressive and anxiety symptoms (b = .119, p = .139; b = −.121, p = .299, respectively). The two-way interaction between difficult temperament and PA at 13 years old was not significantly associated with depressive symptoms (b = −.012, p = .623), but was related to anxiety symptoms (b = −.071, p = .023). As shown in Figure 1, difficult temperament was associated with a higher level of anxiety symptoms for youth who engage in a low amount of PA. For youth who practice a high amount of PA, difficult temperament was not associated with anxiety symptoms. Differences in anxious symptoms dependent on the level of difficult temperament and level of PA at 13 years old.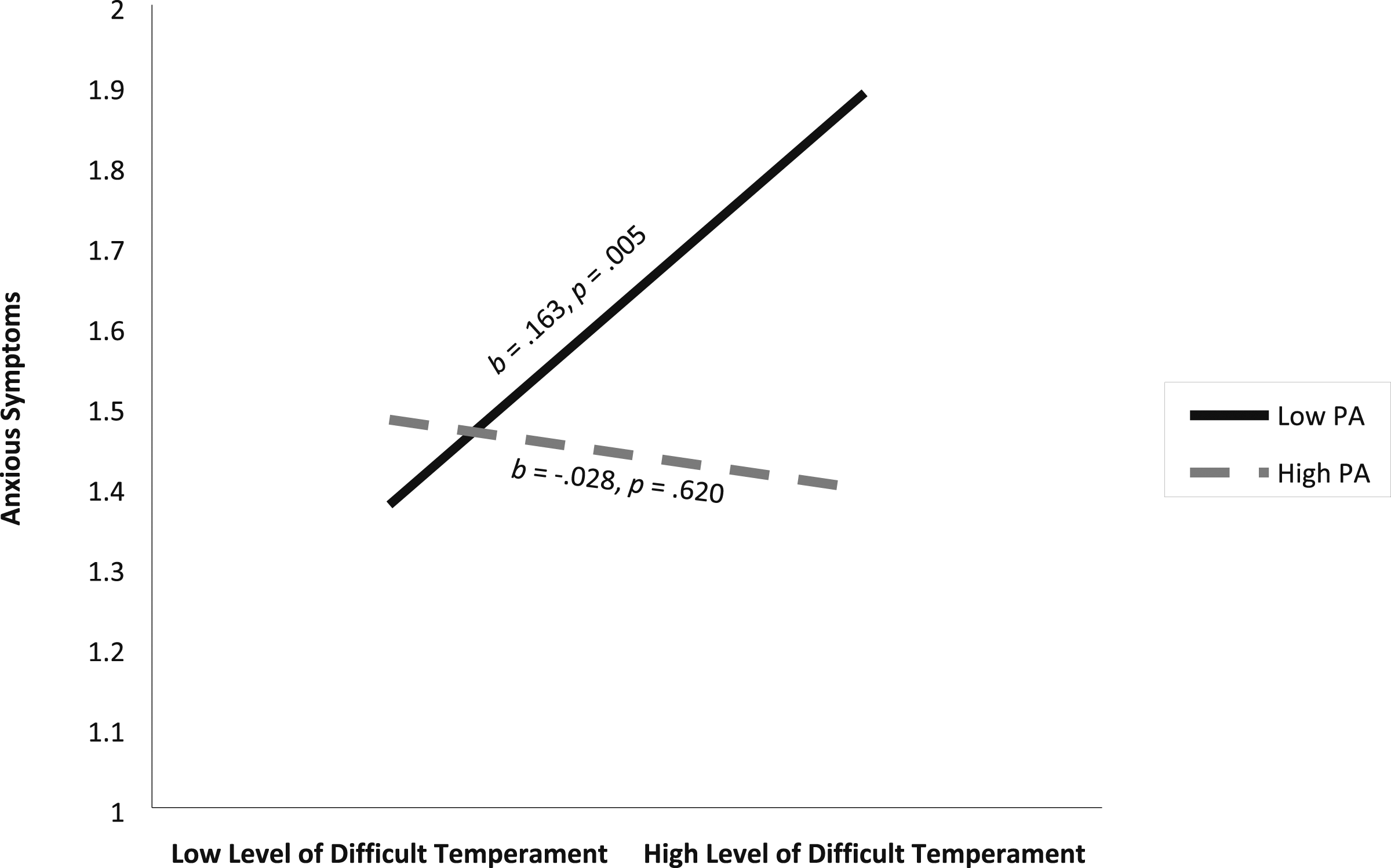
Family Adversity and Difficult Temperament and Hyperactivity-Inattention and Physical Aggressivity Problems in Youth (T2): Main Effects and Direct Effects With PA at 13 Years Old.
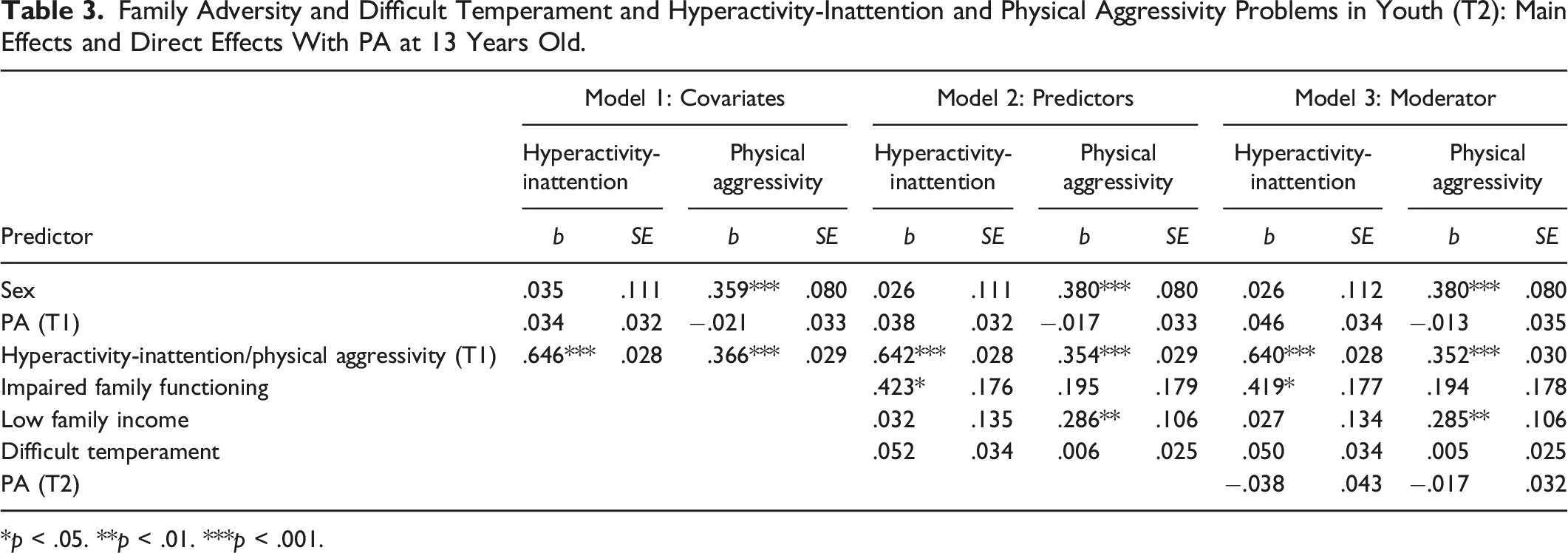
*p < .05. **p < .01. ***p < .001.
The two-way interaction between the main predictors and PA at 13 years old was added to the final sets of models. The two-way interaction between impaired family functioning and PA at 13 years old was not significantly associated with hyperactivity-inattention problems (b = −.036, p = .762), but was related to physical aggressivity problems (b = .253, p = .014). As shown in Figure 2, for youth who engage in a high amount of PA, impaired family functioning was associated with a higher level of physical aggressivity at 13 years old. For youth who engage in a low amount of PA, impaired family functioning was not associated with physical aggressivity at 13 years old. Similarly, the two-way interaction involving low family income and PA at 13 years old was not associated with hyperactivity-inattention and physical aggressivity problems (b = −.014, p = .874; b = .141, p = .063, respectively). Finally, the two-way interaction between difficult temperament and PA at 13 years old was not related to hyperactivity-inattention or physical aggressivity problems (b = −.052, p = .065; b = −.026, p = .184, respectively). Differences in the level of physical aggressivity dependent on the category of family functioning and level of PA at 13 years old.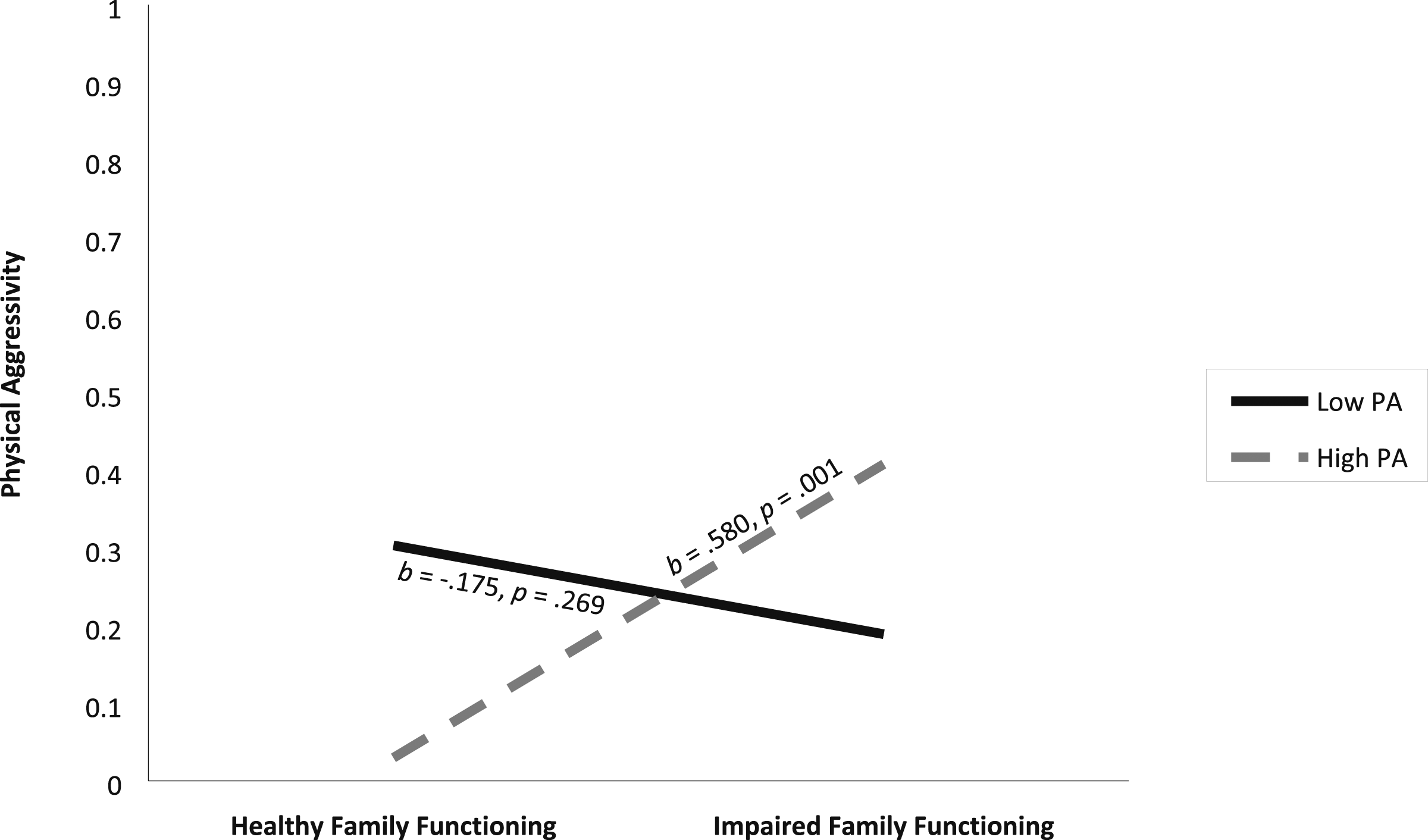
Discussion
Difficult temperament, low family income, and impaired family functioning represent risks for increased internalizing and externalizing problems in young adolescents. Although these risks are well documented, few studies shed light on the potential buffering effect of PA in preventing these adjustment problems among vulnerable young adolescents. This study examined whether PA at 13 years old reduced the risks of internalizing and externalizing problems in youth with difficult temperaments, coming from low-income families, or being exposed to impaired family functioning. Findings partially confirmed the hypotheses by showing that youth practicing PA reported lower levels of symptoms of depression, while some results were specific to youth with a difficult temperament or impaired family functioning. That is, difficult temperament was associated with symptoms of anxiety in early adolescence only among those with low levels of PA, suggesting a protective effect of PA. However, the link between impaired family functioning at 12 years old and levels of subsequent physical aggressivity was amplified among those with high levels of PA. Finally, PA was not associated with hyperactivity-inattention problems.
PA and Adjustment in Early Adolescence
Focusing first on internalizing problems, high levels of PA were directly associated with a lower risk of developing symptoms of depression, regardless of levels of difficult temperament, family income, and family functioning. These results are consistent with the conclusions of previous systematic reviews that have demonstrated the benefits of PA in reducing symptoms of depression in the general adolescent population (Biddle et al., 2019; Panza et al., 2020). A low level of PA also seems to increase the risk of developing symptoms of anxiety among young adolescents with a difficult temperament. Young adolescents with difficult temperaments are prone to report more fear, worry, and nervousness when they do not often engage in PA. This tendency might be specific when exposed to stressors such as the transition from primary to secondary school as investigated in the present study. Participating in group activities such as PA might reduce risks of internalizing behaviors during this sensitive period by providing opportunities to bond with young people also entering the new secondary school (Oberle et al., 2019). These new connections might contribute to developing a strong sense of belonging at school, which in turn reduces symptoms of anxiety (Jindal-Snape et al., 2020; Oberle et al., 2019). This opportunity to create new relationships in a positive context could be particularly beneficial for youth with difficult temperaments given their potentially limited social skills (Borowski et al., 2021).
Regarding externalizing problems, a high level of PA seems to potentiate the risks of physical aggressivity associated with impaired family functioning, instead of mitigating them. Although these results were initially surprising, they echo findings showing that certain types of organized sports (e.g., contact sports like football) that tend to promote competition and aggressivity as an acceptable means of achieving success are associated with externalizing problems (Beaver et al., 2016; Kreager, 2007; Wilson et al., 2010). Young adolescents participating in such sports can adopt these values and exhibit behaviors consistent with them (Kreager, 2007). Under some circumstances, organized sports can thus increase physical aggressivity in the general adolescent population. Such processes could possibly be more pronounced in vulnerable young adolescents exposed to certain family risk factors (e.g., lack of family support) compared to the general population of same-aged peers (Haudenhuyse et al., 2014). These young adolescents tend to exhibit comparatively high feelings of incompetence, social exclusion, and diminished ambition, which can be reinforced in sporting environments emphasizing performance and competition (Haudenhuyse et al., 2014; Super et al., 2017).
An alternative explanation pertains to youth’s participation in informal and unorganized sports that rely less on competition and structures (Kinder et al., 2020). Given their greater accessibility, youth exposed to family adversity might be overrepresented among those taking part in unorganized sports (Kinder et al., 2019, 2020; Skille & Waddington, 2006). Although informal sports are associated with greater autonomy and creativity, the lack of adult supervision sometimes found in this type of sport can increase the risk of behavioral problems such as aggressivity (Martins et al., 2021; Tomé et al., 2023; Wolf et al., 2015). This aggressivity is even more pronounced when peers seem to support it (Powers et al., 2022). Considering that youth sometimes learn antisocial values through social relationships with peers, the risks of endorsing violence as an acceptable means of resolving problems could be amplified if young adolescents do not have a supportive family environment to counter such cultural influences (Akers, 2017; Mutz, 2012). The present study suggests that youth from difficult family environments might benefit from opportunities to participate in supervised PA offering a supportive sports climate that focuses on effort and perseverance to achieve goals rather than aggressiveness and competition. This result remains surprising and ought to be replicated before leading to formal recommendations for practitioners.
Compared to symptoms of depression, anxiety, and physical aggressivity problems, PA was not associated with hyperactivity-inattention problems, which contrasts with meta-analytic results showing negative associations between PA and such behaviors (Lambez et al., 2020; Liang et al., 2021). However, these negative associations were not systematically found, and varied depending on characteristics like PA intensity, type, and duration, with noticeable effects emerging only in certain conditions (Williams et al., 2019). For instance, moderate PA performed at multiple time points appears optimal for the functioning of children and adolescents with hyperactivity-inattention problems compared with light- or vigorous-intensity PA performed at a single time point (Liang et al., 2021). Furthermore, 30 minutes of organized PA improves executive functions, helping to reduce hyperactivity-inattention problems, compared to unorganized PA performed for a longer period (Lambez et al., 2020; Williams et al., 2019). In the present study, young adolescents engaged, on average, in PA for 40–59 minutes per day. This average time spent on PA is longer than the optimal daily duration of PA for people with hyperactivity-inattention problems, considering their difficulty in focusing on an activity for an extended period (Liang et al., 2021; Williams et al., 2019). In addition, PA was assessed at a single time point and included both organized and unorganized PA, without distinguishing between them, which may explain the lack of association between PA and hyperactivity-inattention problems. When conditions are not optimal, PA may not change hyperactivity-inattention problems, which tend to be quite stable given their neurological origins (Faraone et al., 2005).
Limitations
This study has several strengths, including a prospective-longitudinal design, multiple sources of information, and a large number of participants allowing generalization of the result to the target population. However, this study is not without limitations. The correlational design of the study does not allow causal interpretations. In addition, attrition may have influenced associations, even though multiple imputations were used to minimize the risk of bias (Enders, 2010; Little, 2013). Finally, only one aspect of PA was considered, that is, its duration. Additional information including frequency and intensity would have better captured other potentially relevant dimensions of PA (Nolin, 2018). However, specifically assessing PA duration allows for a fine-grained understanding of its moderating effect distinct from other PA dimensions. Several well-established empirical studies have used a single item assessing one dimension of PA (Ganjeh et al., 2022; Gillis et al., 2023). Using a single PA item may explain the unexpected results between PA and hyperactivity-inattention problems in this study. Future studies should include measures of intensity, frequency, as well as the type of PA to examine whether it reduces hyperactivity-inattention problems and other externalizing problems such as physical aggressivity and internalizing problems in vulnerable young adolescents. In addition, it would be interesting to investigate associations by incorporating other forms of adversity. Identifying other forms of adversity that may benefit from PA can reduce the risk of mental health disorders in a larger population.
Conclusion
This study contributes to identifying potential intervention targets by having identified a protective effect of PA against symptoms of anxiety in youth with difficult temperaments. The general benefits of the PA support the importance of promoting it among parents and schools, especially during the primary-secondary school transition period. The association found between PA et aggressiveness among youth exposed to impaired family functioning underscores the need to consider potential downsides of PA, and potential avenues for reducing them, for instance by strengthening sports cultures focusing on self-improvement and perseverance rather than a focus on performance and competition.
Footnotes
Acknowledgments
We would also like to acknowledge the Social Sciences and Humanities Research Council (Conseil de Recherches en sciences humaines) and the Fonds de recherche du Québec - Société et culture for their support of the first author through their scholarship programs.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Sport Canada Research Initiative (SCRI) and Social Sciences and Humanities Research Council (grant number [435-2017-0784] (awarded to Frédéric Nault-Brière)). The Quebec Longitudinal Study of Child Development (QLSCD) was conducted by the Institut Statistique du Québec and was made possible through the generous fundings provided by Le Ministère de la Santé et des Services Sociaux, Le Ministère de la Famille, Le Ministère de l’Éducation du Québec, La Fondation Lucie et André Chagnon, L’Institut de Recherche Robert-Sauvé en Santé et en Sécurité du Travail, Le Centre Hospitalier Universitaire Sainte-Justine, Le Ministère de l’Emploi et de la Solidarité Sociale, Le Ministère de l’Enseignement Supérieur. Fatima Alawie is supported in part by funding from the Social Sciences and Humanities Research Council (Conseil de Recherches en sciences humaines) and Fonds de recherche du Québec-société et culture (FRQSC). Source: Data compiled from the final master file ‘E1-E24’ from the QLSCD (1998–2021), ©Gouvernement du Québec, Institut de la statistique du Québec.
Data Availability Statement
The data has been obtained from a third party: The data analyzed in this study was obtained from the Institut de la statistique du Québec (ISQ) and, as stipulated in clauses 10 and 11 of the ISQ Act (Canada), access to the data is restricted to the parties identified in the partnership agreement signed to ensure the conduct of the study and which describes the author’s right. In the QLSCD cohort, the participants only consented to share their data with the study’s financial partners, affiliated researchers, and their collaborators. Those partners and researchers have only access after signing a data-sharing agreement. For other researchers, requests to access these data can be directed to the ISQ Research Data Access Services - Home (Service d’accès aux données). For more information, contact Marc-Antoine Côté-Marcil (![]() .
.