
Abstract
The relation between hypertension (HTN) and cognition has been reported inclusive results, which may be affected by disease duration. Our study aimed to examine the influence of HTN duration on cognition and its underlying white matter (WM) changes including macrostructural WM hyperintensities (WMH) and microstructural WM integrity. A total of 1218 patients aged ≥55 years with neuropsychological assessment and a subgroup of 233 people with imaging data were recruited and divided into 3 groups (short duration: <5 years, medium duration: 5–20 years, long duration: >20 years). We found that greater HTN duration was preferentially related to worse executive function (EF), processing speed (PS), and more severe WMH, which became more significant during long duration stage. The reductions in WM integrity were evident at the early stage especially in long-range association fibers and then scattered through the whole brain. Increasing WMH and decreasing integrity of specific tracts consistently undermined EF. Furthermore, free water imaging method greatly enhanced the sensitivity in detecting HTN-related WM alterations. These findings supported that the neurological damaging effects of HTN is cumulative and neuroimaging markers of WM at macro- and microstructural level underlie the progressive effect of HTN on cognition.
Keywords
Introduction
Hypertension (HTN) is a highly prevalent disease among the elderly. 1 Despite the general opinion that HTN was associated with cognitive decline, some studies have found no association or even a protective effect between HTN in later life and cognition.2 –4 One of the key factors for this discrepancy was HTN duration, since sufficient time of disease was necessary to cause measurable cognitive changes. 4 Several longitudinal studies with varying follow-up periods assessed the effect of chronic HTN on cognition or dementia risk, and we found that those with longer follow-up (>20 years) were more likely to detect detriment impact of HTN,5 –8 whereas studies with shorter follow-up times (<5 years) tended to fail to find significant relationships.9 –12 Increasing time of HTN could lead to both cognitive impairment and increased dementia risk,13 –15 independent of age of onset. 4 It’s likely a slowly developing hazarding process as cognitive changes may not present in early stage but become more apparent after 20 years or more of HTN. 14
Notably, HTN did not equally target different cognitive domains. The extent of cognitive detriments seemed more pronounced for executive function (EF) and processing speed (PS) abilities.2,3,16 Most studies focused primarily on various measures of blood pressure (BP) level and it remains unclear whether HTN continuously deepens its impact on EF and PS or expands its influence on wider cognitive domains with the prolongation of HTN. Besides, few studies have examined whether the degree of cognitive impairment is positively correlated with HTN course.
The pathological mechanisms behind the relation between HTN and cognition have received increasing attention, but they have not been fully elucidated yet. Compared with gray matter, white matter (WM) structure is more susceptible to the effect of greater HTN duration. 17 BP measured two decades or more was found to be related to structural brain changes, notably within WM. 17 Long-standing HTN may induce cerebrovascular alterations including vascular modeling, atherosclerosis and autoregulation dysfunction, leading to cerebral hypoperfusion or ischemia over time.18,19 WM, which is located at the watershed area of blood supply, is particularly vulnerable to hypoperfusion or ischemia. 20 This can result in WM structural alterations, including WM integrity degeneration and subsequent white matter hyperintensities (WMH), which were early and common brain lesions among hypertensives,1,19,21 and could effectively predict the risk of cognitive changes and dementia.22,23
A growing body of research suggested that WM structure may modulate the connection between HTN and cognition,24,25 but the impact of HTN duration on this relation has been less extensively studied. To our knowledge, most studies only reported the pairwise association. For example, it has been suggested that 5-year and 20-year duration of HTN among older adults was respectively related to 3 or 20-fold increase in WM damage risk. 26 Those with greatest HTN duration had largest WMH. 27 Regarding WM microstructure, only a study by McEvoy et al. 28 indicated that individuals with HTN duration >5.6 years was related to altered diffusion properties in several tracts. However, it’s currently unknown whether impact of HTN duration on WM structure would further exhibit cumulative harms to cognition. Moreover, some studies have confirmed that a wide range of WM tracts could be affected by HTN, and this relation seemed to be more pronounced for long-range fibers linking frontal and posterior areas,25,28 but whether these areas were targeted earliest by HTN pathology remains unclear. Therefore, the spreading pattern of WM fibers disruption in different stages and its link with cognition warrants clear define.
Moreover, traditional diffusion tensor imaging (DTI)-derived metrics may be limited due to extracellular water contamination and thus, a free water (FW) elimination model was proposed to enhance tissue specificity of DTI measures. 29 The use of FW imaging has shown promising in increasing the sensitivity of identifying clinically relevant brain changes such as in mild cognition impairment 30 and dementia, 31 but has not previously been studied in the context of HTN. Therefore, we wanted to utilize these two methods to examine which approach was more sensitive for detecting WM integrity changes in the progress of HTN and the location of these alterations. Greater sensitivity in detecting microstructural abnormalities may help identify individuals at greatest risk for cognitive decline.
As a modifiable risk factor, examining the cumulative effect of HTN might provide a new perspective for alleviating and delaying cognitive impairment. To address the gaps in previous literatures, we aim to clarify the impact of HTN duration on cerebral WM structure and cognition in older hypertensive patients, which could aid in providing early signature of damage and better understanding the HTN-related neural mechanism. Based on previous studies, we hypothesized that with the extension of HTN duration, hypertensive older adults would (1) demonstrate worse performance in multiple cognitive domains, especially EF and PS; (2) exhibit more severe WMH; (3) show reduced WM tracts integrity, spreading from long-range association fibers to whole brain; (4) More importantly, increasing macro- and micro-WM structural changes will be related to cognitive dysfunction; (5) FW imaging method would improve the sensitivity to microstructural alterations that occur early in the development of HTN.
Material and methods
Participants
Participants were randomly recruited from the Beijing Aging Brain Rejuvenation Initiative (BABRI) Study Group. 32 Inclusion criteria were as follows: (1) right-handed and native Chinese speakers; (2) ≥55 years old; (3) ≥6 years of education; (4) nondementia with normal daily living abilities, and scored ≥24 on the Mini Mental Status Examination (MMSE); 33 (5) no history of brain injury or tumors, intracranial hemorrhage, nephritis, neurological or psychiatric disorders, or addiction; (6) no conditions known to impact cerebral function, including alcoholism, Parkinson’s disease, or epilepsy.
All the participants reported that they were clinically diagnosed with HTN by a physician (i.e., SBP ≥140 mmHg and/or DBP ≥90 mmHg) or had a history of taking oral antihypertensive medications. Medical history of other comorbid diseases such as coronary heart disease (CHD), diabetes, hyperlipidemia (HLP) and cerebrovascular diseases (CVD) were also recorded. The BP-lowering medication comprises angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, calcium antagonists, diuretics, β-blockers, or compound antihypertensives. The duration of HTN in years was defined as the time interval between age at imaging assessment date and the age at which participants reported when a doctor first diagnosed HTN. 27 Participants was divided into three stages: short duration (<5 years), medium duration (5–20 years) and long duration (>20 years), which was primarily informed by prior studies that directly investigated HTN duration and longitudinal research with different follow-ups, highlighting the potential significance of 5 and 20-year cutoffs.5,9,14,26,34
A total of 1218 participants (782 women, 436 men, aged 55–91 years [68.65 ± 7.30 years]) took the neuropsychological assessment, including 333 participants with short duration HTN (217 women, 116 men, aged 55–89 years [66.34 ± 6.85 years]), 427 participants with medium duration HTN (275 women, 152 men, aged 55–86 years [67.89 ± 7.13 years]) and 458 participants with long duration HTN (290 women, 168 men, aged 55–91 years [71.02 ± 7.11 years]). MRI data was acquired from a subsample of 233 participants (150 women, 83 men, age 55–82 years [67.09 ± 6.47 years]) after their initial neuropsychological assessment.
The current study conformed to the principles of the Declaration of Helsinki and was approved by the Ethics Committee and Institutional Review Board of Beijing Normal University Imaging Center for Brain Research. Data was anonymized and all the participants gave their informed consent, written.
Neuropsychological assessment
All participants received comprehensive neuropsychological assessments including (1) MMSE indexing global cognitive function; 33 (2) Auditory Verbal Learning Test (AVLT) 35 and Rey-Osterrich Complex Figure test (ROCF delay) 36 indexing memory; (3) Trail Making Test-A (TMT-A) 37 and Symbol Digit Modalities Test (SDMT) 38 indexing PS; (4) Category Verbal Fluency Test (VFT) 39 and Boston Naming Test (BNT) 40 indexing language ability; (5) Trail Making Test-B (TMT-B) 37 and Stroop Color and Word Test (Stroop-C) 41 indexing EF.
Data acquisition
MRI data were acquired using a Siemens Trio 3 T scanner at the Imaging Center for Brain Research of Beijing Normal University. T1-weighted, sagittal 3D magnetization-prepared rapid gradient echo sequences were acquired and covered the entire brain [176 sagittal slices; repetition time (TR) = 1900 ms; echo time (TE) = 3.44 ms; slice thickness = 1 mm; flip angle = 9°; inversion time = 900 ms; field of view (FOV) = 256 × 256 mm2; acquisition matrix (AM) = 256 × 256]. A T2-weighed fluid-attenuated inversion recovery (T2-FLAIR) sequence was applied to measure WMH [TR = 9000 ms; TE = 81 ms; slice thickness = 3 mm; flip angle = 150°; number of slices = 25]. Diffusion imaging data was acquired using a single-shot echo-planar imaging sequence [coverage of the whole brain; 2 mm slice thickness with no section gap; 70 axial slices; TR =9500 ms; TE = 92 ms; flip angle = 90°; 30 diffusion directions with b = 1000 s/mm2 and an additional image without diffusion weighting (b = 0 s/mm2); FOV = 256 × 256 mm2; AM = 128 × 128; number of signals acquired= 3].
WMH assessment on FLAIR scans
WMH was automatically segmented by the lesion prediction algorithm (LPA, Chapter 6.1) 42 as included in the freeware Lesion Segmentation Toolbox (LST version 3.0.0, https://www.statistical-modelling.de/lst.html) for Statistical Parametric Mapping (SPM12). LPA segmented WMH lesions in new images by estimating the lesion probability for each voxel. The threshold for producing lesion probability maps was 0.2 and total lesion volume was extracted. Meanwhile, we used Computational Anatomy Toolbox (CAT12, https://neuro-jena.github.io/cat/), to estimate the total intracranial volume (TIV) via T1-weighted images, and obtained a fraction index by dividing WMH volume by corresponding TIV (WMH volume/TIV) for further analyses.
Diffusion imaging data processing
The preprocessing and analyses were performed with FMRIB’s Diffusion Toolbox (FDT) in FMRIB Software Library (FSL version 5.0.7, https://fsl.fmrib.ox.ac.uk/). The preprocessing steps include corrections of eddy current distortions and head movement with eddy_correct, extraction of brain mask with brain extraction tool (BET) and calculation of diffusion tensors using DTIFIT program. Voxel-wise fractional anisotropy (FA), mean diffusivity (MD), axial diffusivities (AD) and radial diffusivities (RD) maps were then derived. FA provides an overall measure of WM health, maturation, and organization; MD reflects the average degree of diffusion; AD reduction represents axonal loss, whereas increased RD is linked to reduced myelin integrity.43,44
In addition to the conventional DTI model, we also used the FW imaging method, which was based on the bi-tensor model within each voxel including a FW compartment (isotropic tensor) and a tissue compartment (FW-corrected tensor). 29 The FW compartment models extracellular water molecules that are free to diffuse and unrestricted by their surroundings. The fractional volume of FW compartment (the FW measure) was used to indicate the contribution of FW per voxel and provide a FW map, ranging from 0 to 1. In contrast, the tissue compartment models water molecule restricted by tissue membranes and reflects WM microstructure after correcting the contamination of FW signal. Therefore, the derived parameter of FW-corrected FA (FAt) was more sensitive to WM degeneration than traditional DTI measures.30,31 FAt depends on two separate measures, ADt and RDt, which were also calculated for extra investigations. The FW model was conducted with MarkVCID MRI Free Water Imaging Biomarker Kit. 45
Group differences of corrected or uncorrected diffusion metrics were measured on the WM skeleton using Tract-Based Spatial Statistics (TBSS) analysis. 46 TBSS analyses for diffusion metrics included following steps: 1) Each participant’s FA image was spatially aligned to a standard space by nonlinear registration algorithm; 2) Aligned FA maps were averaged to generate a mean FA image and then thinned to produce a mean FA skeleton representing the center of all tracts common to all subjects and the threshold at FA value for the skeletonization was 0.20; 3) Each participant’s FA image was then projected onto the mean FA skeleton; 4) voxel-wise cross-subject statistics were calculated for each point within the common skeleton. Above-mentioned FA transformations were also used to project other metrics onto the TBSS skeleton for additional analysis.
To further remove the effect of WMH and examine WM integrity within the normal-appearing white matter (NAWM), we also performed tissue segmentation. Specifically, the T1-weighted image was first non-linearly normalized to the Montreal Neurological Institute (MNI). Then, the T2-FLAIR image of each subject was co-registered to the individual T1-weighted image. The transformations from the previous two steps were applied to the WMH lesion mask maps, resulting in MNI-space lesion map for each subject. A threshold of 0.5 was used for obtaining the lesion mask in MNI space. Finally, the NAWM regions were derived by removing WMH lesion from the significant regions of subject-level skeletonized images derived from TBSS. Mean original and FW-corrected metrics within NAWM for each individual were extracted.
Statistical analysis
Statistical analyses were performed with R version 4.2.1. All the following analyses were adjusted for age, sex, educational years, BP-lowering medication components and other comorbid diseases including CHD, diabetes, HLP and CVD. One-way analysis of variance (ANOVA) was carried out to examine the group differences in age, education, SBP and DBP level. Chi-square test was performed to compare the sex ratios and comorbid diseases (yes/no) of the three groups. To specify the influence of HTN duration on cognitive domains and WMH, analysis of covariance (ANCOVA) was conducted. All data was tested for normality with the Shapiro-Wilk test and Q-Q plot, and the non-normally distributed data was logarithmically transformed. Correlations between HTN duration and different cognitive domains, as well as the relation between HTN duration and WMH were measured using linear regression modelling.
Because the inevitable relation between disease duration and age, the age of the three groups might have been unbalanced. We also conducted the propensity score matching (PSM) to further minimize the potential effect of age. 47 The matching approach was set as the nearest neighbor algorithm with the caliper value of 0.5. We then analyzed the outcomes of cognition in age-matched groups to verify the effect of disease course on cognition, with other confounders still controlled.
For diffusion imaging data, voxel-wise statistical analyses of TBSS were conducted with nonparametric permutation-based inference tool (“randomize”, part of FSL) with the general linear model (GLM) as statistical modeling. Pair-wise group comparisons were performed and significance threshold was p < 0.05 (5000 permutations, family-wise error (FWE) correction for multiple comparisons correction with the threshold-free cluster enhancement (TFCE). WM tracts were identified using the Johns Hopkins University (JHU) DTI-based atlas including 20 main fiber tracts. For both original and FW-corrected DTI measures exhibiting significant group differences as determined by TBSS, we further examined its group differences within the NAWM using ANCOVA.
Next, we calculated the relationship between WM structure and cognitive domains showing significant group differences. Linear regression analyses were conducted to see if WMH volume could predict cognition. We also extracted the average values of diffusion metrics on WM fibers affected by HTN duration and assessed its relation with the neuropsychological scores with linear regression analyses (false discovery rate (FDR) correction for multiple WM fibers). The associations between these NAWM measures and cognition were also accessed.
Data visualisation for cognition and WMH were conducted with R packages including gglpot2 (version 3.4.1, https://ggplot2.tidyverse.org) and ggbeeswarm (version 0.6.0, https://github.com/eclarke/ggbeeswarm); Results for diffusion data were visualized with MRIcroGL (https://www.nitrc.org/projects/mricrogl) and BrainNet View (https://www.nitrc.org/projects/bnv). 48
Results
Effect of HTN duration on demographic and neuropsychological characteristics
Three groups did not show significant differences in sex (χ2 = 0.30, p = 0.862) and education (F (2, 1215) = 0.32, p = 0.729), but indicated differences in age (F (2, 1215) = 46.39, p < 0.001,
Demographic, clinical and cognitive characteristics among all participants (n = 1218) and cognitive correlations with hypertensive duration.
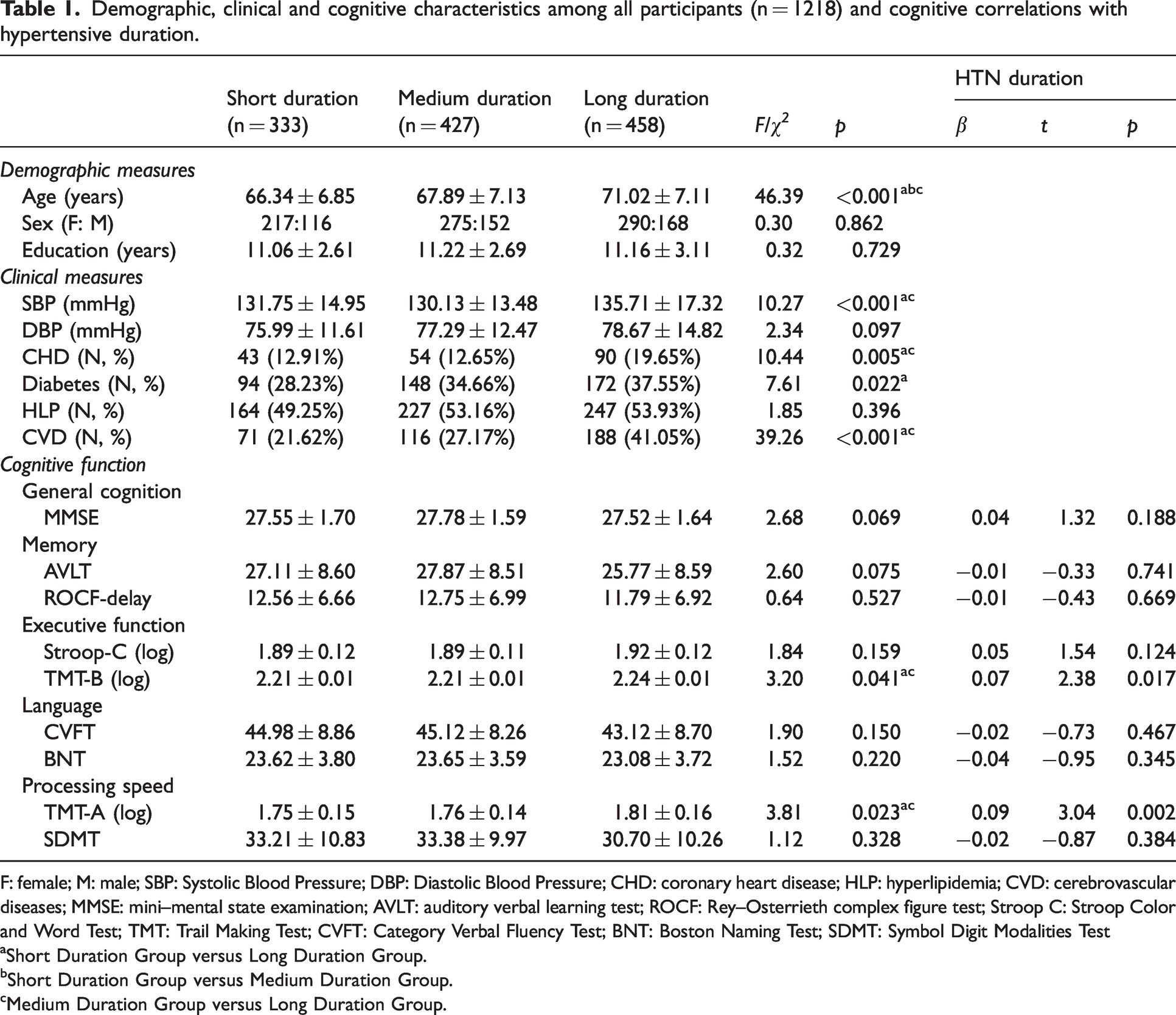
F: female; M: male; SBP: Systolic Blood Pressure; DBP: Diastolic Blood Pressure; CHD: coronary heart disease; HLP: hyperlipidemia; CVD: cerebrovascular diseases; MMSE: mini–mental state examination; AVLT: auditory verbal learning test; ROCF: Rey–Osterrieth complex figure test; Stroop C: Stroop Color and Word Test; TMT: Trail Making Test; CVFT: Category Verbal Fluency Test; BNT: Boston Naming Test; SDMT: Symbol Digit Modalities Test
Short Duration Group versus Long Duration Group.
bShort Duration Group versus Medium Duration Group.
cMedium Duration Group versus Long Duration Group.
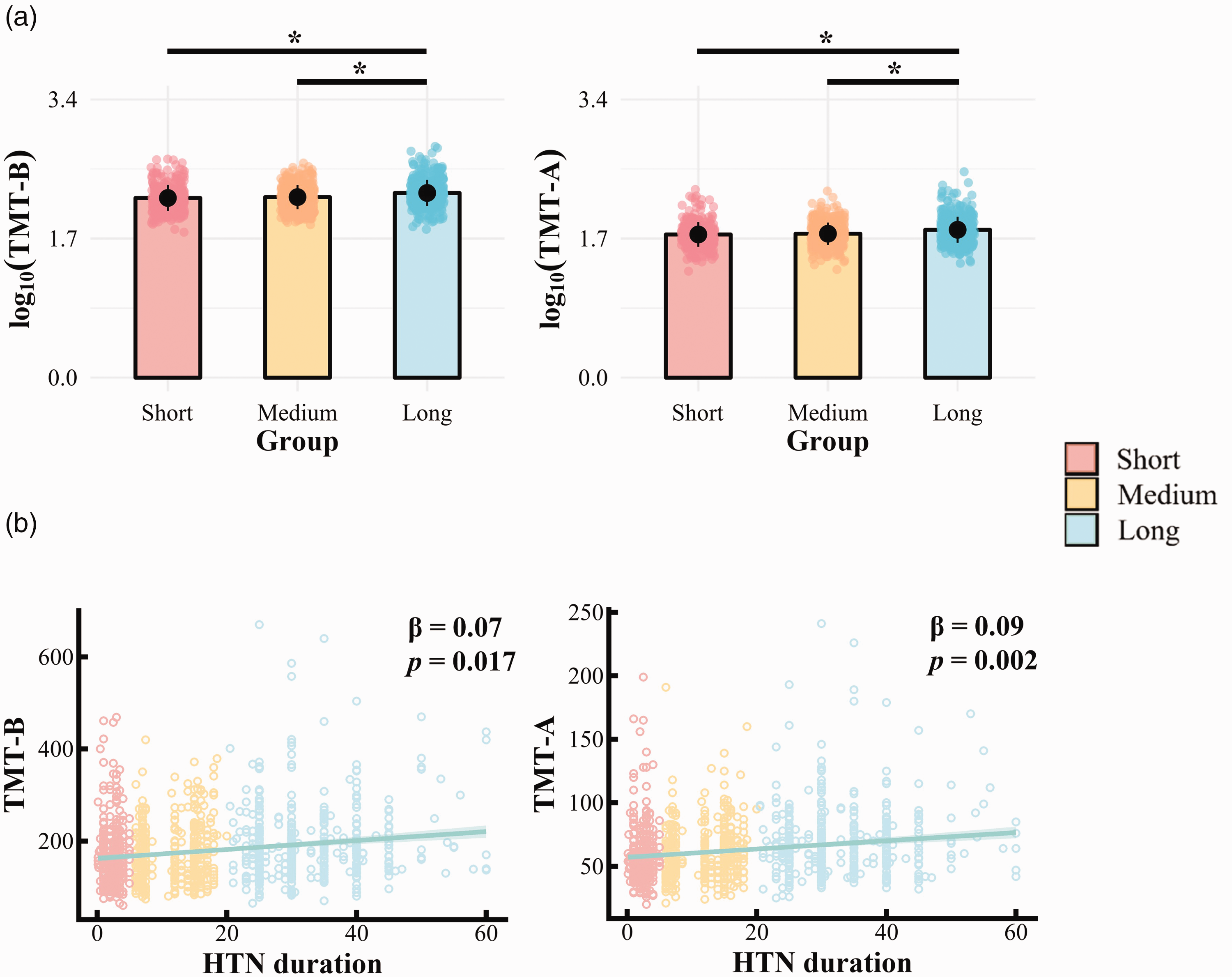
Effect of hypertension (HTN) duration on cognition. (a) Group differences by HTN duration in neuropsychological tests. *p < 0.05. (b) Relationship between HTN duration and cognition.
Further analysis focused on whether HTN duration, as a continuous variable, can predict cognition. Results showed that longer HTN duration was significantly related to worse EF (TMT-B: β = 0.07, 95% CI: 0.01 to 0.12, p = 0.017) and PS (TMT-A: β = 0.09, 95% CI: 0.03 to 0.14, p = 0.002) after controlling the confounders (see Table 1, Figure 1). There were no significant associations between HTN duration and other neuropsychological assessments (all p > 0.05).
To avoid confounding effect, PSM was used to balance the age differences between groups. We compared the outcomes of cognition in 300 short duration patients (aged 57-89 years [67.18 ± 6.47 years]), and 300 age-matched medium duration (aged 55-86 years [67.16 ± 6.78 years]) and long duration patients (aged 55-86 years [68.13 ± 6.33 years]). Post-PSM results were consistent with pre-PSM: there were still significant difference between groups in TMT-B (F (2, 1215) =3.85, p = 0.022,
Effect of HTN duration on WM structure
Effect of HTN duration on macrostructural WMH. Demographic characteristics of the imaging sample for WMH analysis was shown in Supplemental Table 1. Patients with different hypertensive duration indicated significant differences in WMH volume (F (2, 230) = 6.05; p = 0.003,
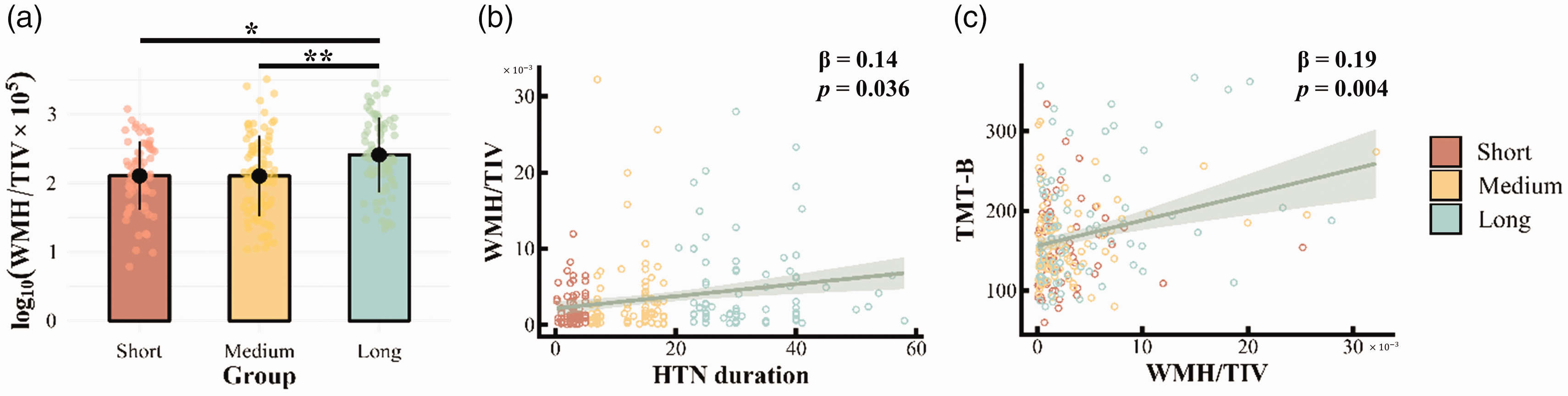
Effect of hypertension (HTN) duration on macrostructural white matter hyperintensities (WMH). (a) Group difference by HTN duration in WMH, *p < 0.05, **p < 0.01. (b) Relationship between HTN duration and WMH. (c) Relationship between WMH and executive function (EF).
Linear regression results also indicated that increasing HTN duration was related to higher volume of WMH (β = 0.14, 95% CI: 0.01 to 0.27, p = 0.036, see Figure 2).
Effect of HTN duration on microstructural integrity. Compared with the short duration group, medium duration group presented significantly reduced FAt and ADt values, which were consistently found in left inferior fronto-occipital fasciculus (IFOF.L) and left inferior longitudinal fasciculus (ILF.L) (FWE-correction, p < 0.05, see Table 2, Figure 3, Supplemental Figure 1). FA, MD, RD, AD, RDt and FW indices indicated no significant difference between these two groups.
Group differences by hypertensive duration in white matter integrity of imaging subsample (n = 233).
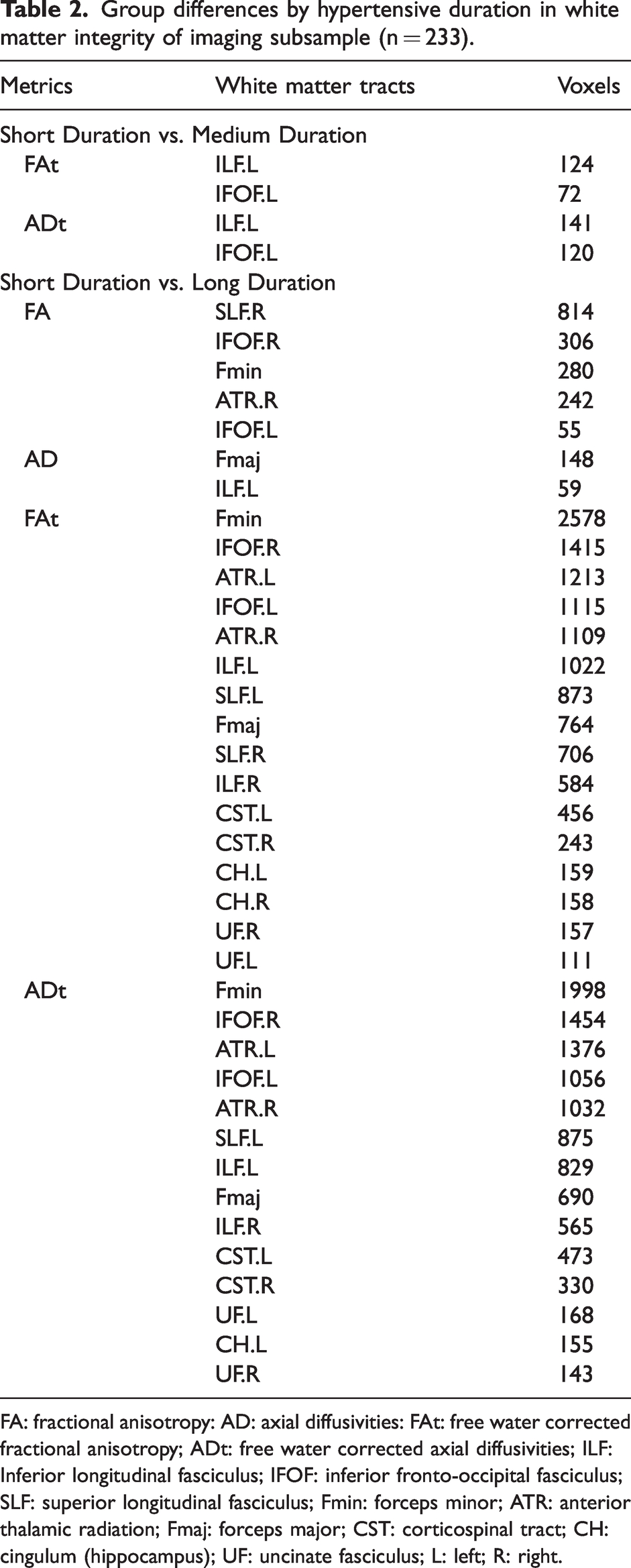
FA: fractional anisotropy: AD: axial diffusivities: FAt: free water corrected fractional anisotropy; ADt: free water corrected axial diffusivities; ILF: Inferior longitudinal fasciculus; IFOF: inferior fronto-occipital fasciculus; SLF: superior longitudinal fasciculus; Fmin: forceps minor; ATR: anterior thalamic radiation; Fmaj: forceps major; CST: corticospinal tract; CH: cingulum (hippocampus); UF: uncinate fasciculus; L: left; R: right.
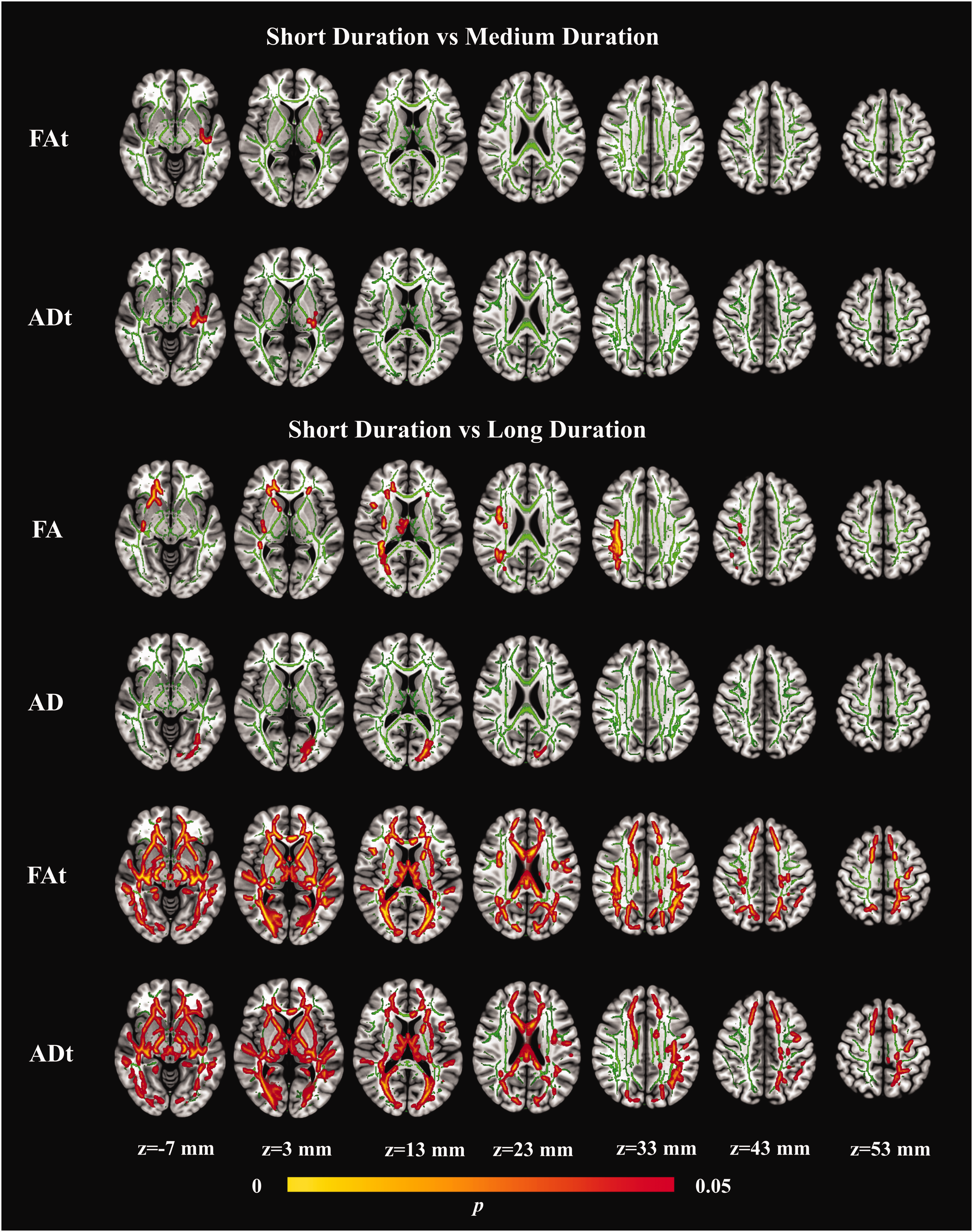
The tract-based spatial statistics (TBSS) results of the diffusion metrics indicating significant group differences (FWE-corrected, p < 0.05). Green indicated the TBSS skeleton. White matter regions showing decreased fractional anisotropy (FA), axial diffusivities (AD), free water (FW) corrected fractional anisotropy (FAt) or FW corrected axial diffusivities (ADt) in Long Duration Group and Medium Duration Group, compared to Short Duration Group.
With HTN processing to long duration, more disrupted regions could be observed. Long duration group had significantly lower FA values cross multi-WM fibers than short duration group including right superior longitudinal fasciculus (SLF.R), bilateral IFOF, forceps minor (Fmin), right anterior thalamic radiation (ATR.R), and decreased AD value in forceps major (Fmaj) and ILF.L, and these locations overlapped with the group differences in FAt and ADt. However, wider altered regions were identified when applying the FW-corrected metrics. WM where reduced FAt value overlapped with lower ADt included Fmin, bilateral IFOF, bilateral ATR, left SLF, bilateral ILF, Fmaj, bilateral corticospinal tract (CST), left cingulum (hippocampus) (CH.L), and bilateral uncinate fasciculus (UF). Besides, FAt was significantly decreased in SLF.R, CH.R (FWE-correction, p < 0.05). No significant differences were detected by MD, RD, RDt and FW measures. There was no statistically significant difference between medium duration and long duration group (all p > 0.05).
Effect of HTN duration on microstructural integrity in NAWM. Patients with different hypertensive duration indicated significant differences in FA, AD, FAt and ADt values in NAWM; long duration group exerted reduced values in all indices of integrity in NAWM than both short and medium duration group (see Supplemental Table 2). Compared with short duration group, NAWM for four measures were significantly lower in medium duration group.
Result of linear regression analyses also indicated that increasing HTN duration was consistently related to lower FA, AD, FAt and ADt in NAWM.
Association between WM structure and cognition
Association between macrostructural WMH and cognition. We then examined the correlations between WMH and the cognitive domains exhibiting significant intergroup differences (i.e., TMT-B, TMT-A) and found that WMH volume was significantly correlated with worse EF (TMT-B time: β = 0.19, 95% CI: 0.06 to 0.32, p = 0.004) but not with PS (p > 0.05) (see Figure 2).
Association between microstructural integrity and cognition. The correlations between the diffusion values in WM tracts where differences were observed between groups (i.e., FA, AD and FAt, ADt) and cognitive domains with significant differences (i.e., TMT-B, TMT-A) were also calculated. Regression analyses indicated that lower FA, FAt and ADt values of Fmin, IFOF.L and ATR.R were related to worse TMT-B performance (see Table 3, Figure 4). Besides, reduced FA value of IFOF.R, SLF.R, or reduced FAt value of ATR.L, CST.R, Fmaj, bilateral SLF, UF.R, or ADt value of ATR.L, Fmaj, CST.R and UF.R were associated with TMT-B. There was no significant relationship between uncorrected AD and cognition. There were also no correlations between TMT-A and diffusion metrics (all p > 0.05).
Linear regression analyses of white matter integrity with significant group differences predicting cognitive function in imaging subsample (n = 233).
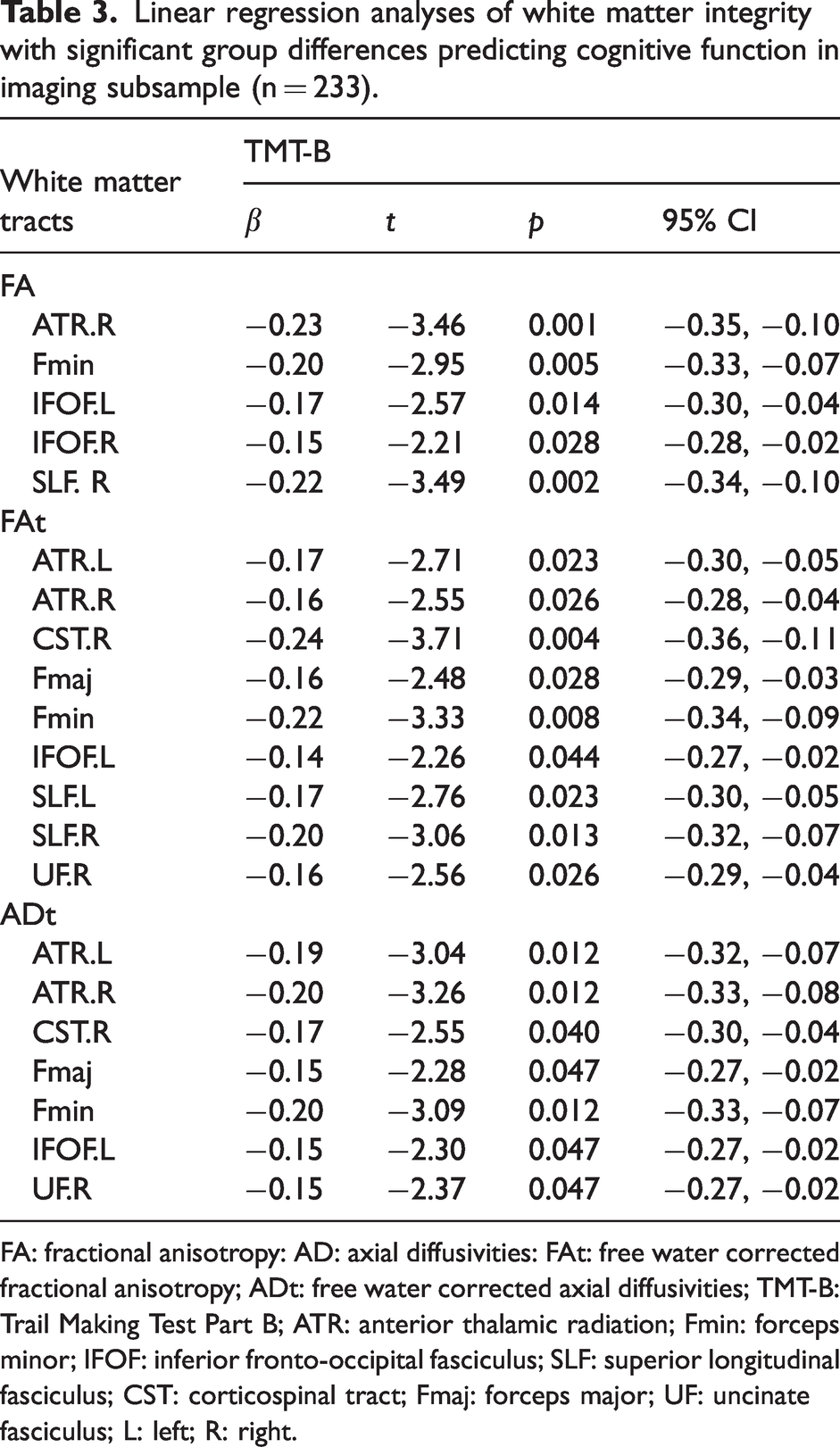
FA: fractional anisotropy: AD: axial diffusivities: FAt: free water corrected fractional anisotropy; ADt: free water corrected axial diffusivities; TMT-B: Trail Making Test Part B; ATR: anterior thalamic radiation; Fmin: forceps minor; IFOF: inferior fronto-occipital fasciculus; SLF: superior longitudinal fasciculus; CST: corticospinal tract; Fmaj: forceps major; UF: uncinate fasciculus; L: left; R: right.
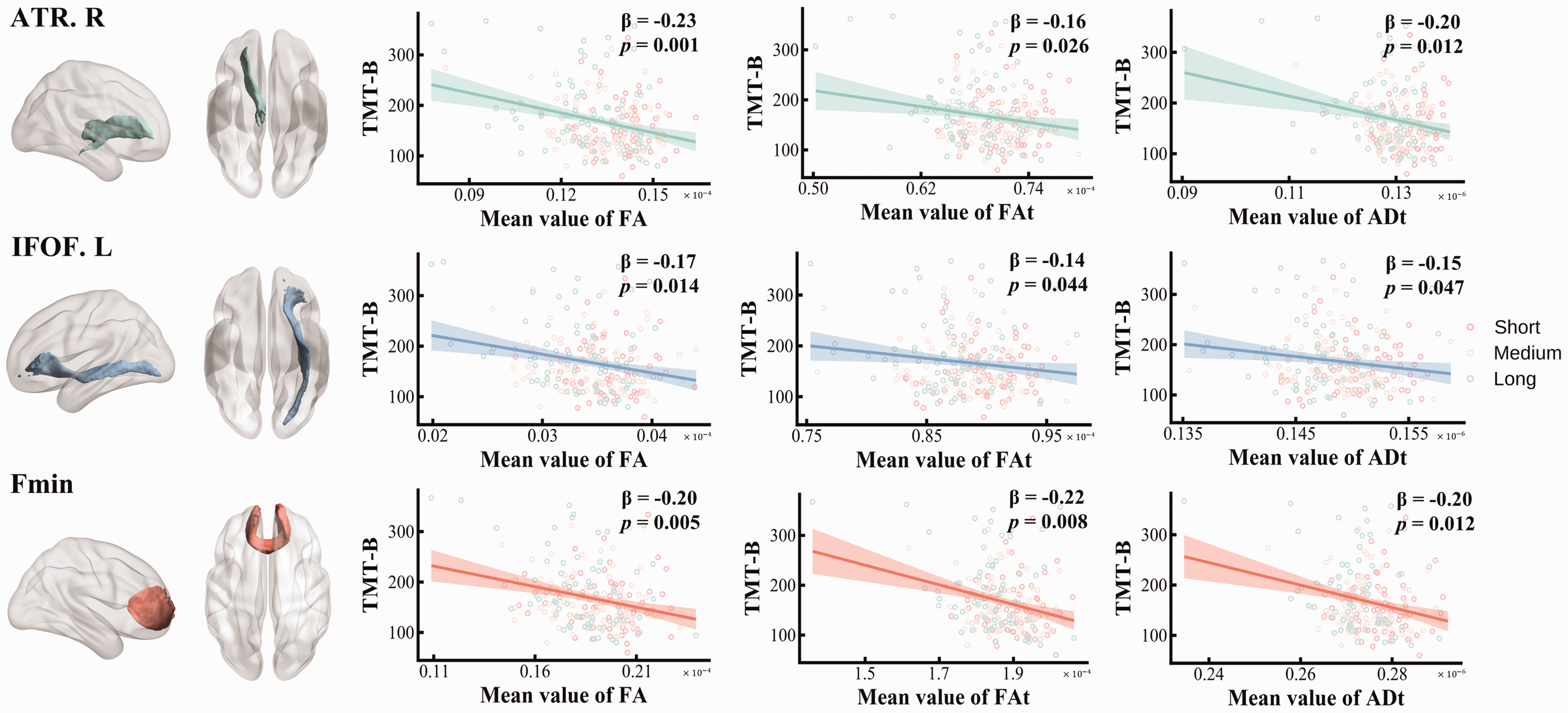
The relationship between diffusion metrics and cognition. The negative relationships between white matter tracts including right anterior thalamic radiation (ATR.R), left inferior fronto-occipital fasciculus (IFOF.L) and forceps minor (Fmin) and executive function (EF) were consistently detected by FA, FAt and ADt values.
Association between microstructural integrity in NAWM and cognition. We further examined the correlations between diffusion values (FA, AD, FAt and ADt) with significant group differences in NAWM and cognition. We found that lower values of all the metrics except AD in NAWM could predict TMT-B performance (see Supplemental Table 3).
Discussion
In line with our hypothesis, we observed the dependent effect of HTN duration on cognition and WM structure by considering HTN duration as both categorical and continuous variable. Specifically, we observed that (1) greater HTN duration was preferentially related to worse EF and PS, as well as more severe WMH, which became more significant in the long duration stage; (2) longer HTN duration led to greater reductions in WM integrity, which could occur at the early stage, especially in the long-range association fibers including the ILF and IFOF and then scattered through the whole brain during the long duration course; (3) with the progression of HTN, macrostructural WMH and reduced microstructural integrity of specific tracts were consistently related to EF ability; (4) Subtle changes of WM integrity within NAWM caused by HTN duration, could also subsequently contribute to executive dysfunction, which was independent of effect of WMH. (5) compared with conventional DTI method, FW imaging model was more effective at detecting earlier and more extensive WM alterations.
The pattern of cognitive decline with the development of HTN
While numerous studies have confirmed the relation between HTN and cognition, few have examined total duration of HTN as an independent risk factor for cognitive decline. Our results indicated that HTN duration was predominantly impaired EF and PS, but not with other domains. Such a pattern was consistently observed in other studies.3,25,49 Impaired cerebrovascular reactivity, an important mechanism of HTN-related outcomes, also related to EF and PS. 50 These two cognitive processes rely heavily on prefrontal and associated substrates, and thus may be most susceptible to the effects of HTN.16,51 It's important to note that EF can be split into distinct components. For instance, TMT-B test mainly reflects set switching domain (mental flexibility), while Stroop-C test indicates ability of inhibitory control. 52 The significant effect on TMT-B rather than Stroop-C may indicate that the deleterious effect of HTN on EF was mainly related to disrupted mental flexibility.
Additionally, we found that only when HTN progressed to long duration can patients exhibit significant EF and PS differences, and there was no significant difference between individuals with short and medium duration, which may indicate the damaging effects of HTN in cognition is cumulative. Li et al. 14 also indicated that cognitive impairment may not be apparent in the early phase of HTN (<6 years), but as HTN duration increased (>20 years), cognition may gradually decline from MCI to dementia. The plausible explanation may be the impact of HTN on the pathological changes in cerebral blood vessels critical for cognition is also cumulative. 3 Therefore, it’s important to have diagnosis and intervention at the early stage of onset to prevent deepened damage on cognition.
The pattern of macrostructural WMH with the development of HTN
Our results also indicated that individuals with a longer duration of HTN were more likely to have WMH. Previous studies have consistently confirmed the association between BP level and WMH21,53 –55 and our study further validated the relation between HTN and WMH from the perspective of disease course.
Consistent with the pattern of cognition, the results of group comparison indicated that only when HTN progressed to long duration could patients show significant WMH differences, and there is no difference between short and medium duration group, which suggested the damaging effects of HTN in WMH was also cumulative. According to previous studies, macroscopic WM lesions did not differ between those with recent onset HTN and those with 3-6 year HTN, 56 but 20-year duration of HTN was related to increased odds WM lesions among the older adults. 26 Therefore, long-term exposure to HTN, rather than transient increased BP, was critical for WMH formation. 57 During the early stages, there would be adaptive autoregulation responses to protecting downstream microvessels from increased transmural pressure, but with prolonged HTN exposure, this process can become maladaptive, resulting in the development of further pathologies such as autoregulation dysfunction, decreased cerebral blood flow and ischemic injury that gradually contribute to apparent WMH.19,26,58
The pattern of microstructural integrity with the development of HTN
Our finding also indicated that WM microstructural integrity decreased as the duration of HTN extended, which were primarily observed in the FA/FAt and AD/ADt measures but not RD/RDt, suggesting that prolonged HTN predominantly contributes to the deterioration of axonal architecture. We also differentiated the integrity in WMH and NAWM, and our results suggested that the subtle changes in NAWM were also affected by HTN duration. However, few studies have examined impact of HTN duration on WM integrity before. One previous study showed that individuals with longer history of high SBP would have lower FA, 59 which indicated that longer incubation time may underline the association between HTN, cerebrovascular alterations and WM abnormalities.
Notably, different from the pattern of cognition and WMH, both medium and long duration groups had worse WM microstructure than short duration group but there were not differences between these two groups, indicating that HTN-related disruptions in WM microstructure occurred early and may persisted to longer duration. According to previous study, even pre-HTN was related to altered WM microstructure in several tracts. 60 Once BP rises above normal, subtle but harmful WM integrity changes can occur rather quickly and these changes may be hard to reverse, even if BP is nudged back into the normal range with treatment. 28 Considering alterations in WM microstructure took place earlier than WM macroscopic changes, it could potentially be an early warning sign of HTN-related brain changes.19,61,62
We also identified the spreading pattern of WM microstructural changes in HTN processes, with long-range association fibers such as ILF.L and IFOF.L showing reduced integrity in the early stages. When HTN progresses to long-standing HTN (> 20 years), individuals had disrupted WM microstructure in most tracts. Various studies have highlighted the regional vulnerabilities of long-range association fibers connecting anterior to posterior cerebral regions such as the IFOF, ILF, SLF and UF25,28,60 and we further confirmed that these were also the areas targeted earliest by HTN. These tracts were particularly sensitive to the insults of HTN because they mainly located within the watershed areas that is supplied by distal, small and penetrating arterioles, which are highly vulnerable to HTN-induced hypoperfusion and arteriosclerotic changes.18,19,25 With the progression of HTN, it would affect a variety of tracts, including association fibers, thalamic radiations, and projection fibers. This may result from the cumulative impact of prolonged HTN, which exacerbates widespread WM pathology. Sustained high BP disrupts cerebrovascular structures and facilitate oxidative stress and neuroinflammation, which have a critical role in axonal loss and WM changes.63 –65 Therefore, it’s important to implement early intervention to prevent the progression of whole-brain WM damage and preserve brain health.
The association between WM structural alterations and cognitive decline
Both macrostructural WMH and microstructural integrity were consistently observed to be related to EF, indicating the mechanism by which long-term HTN may lead to cognitive dysfunction seems to be related to its chronic and detrimental impact on WM structure. Several longitudinal research has indicated that WMH progression over the follow-up periods was related to neurobehavioral functioning decline in HTN.49,66,67 The most commonly observed cognitive changes associated with WMH burden is EF.68,69 Executive dysfunction in individuals with HTN appears to be connected to widely distributed WMH, with a greater degree of involvement in the frontal regions.70 –72
Regarding the microstructural changes, among the WM fiber bundles initially affected (i.e., ILF and IFOF), we identified a significant correlation between IFOF and deteriorating EF. Some previous studies have highlighted the mediating role of IFOF in HTN and EF.25,73 As HTN progressed, the diminished WM integrity and axonal loss in a wider range of WM fibers were related to worse EF, especially the ATR.R, IFOF.L and Fmin, which could be consistently detected by FA, FAt and ADt. Other studies have also reported on the roles of these fibers in the HTN-related executive dysfunction.25,73,74 These fibers are mainly long-range fibers located or connecting the anterior regions. 25 Pathological changes in these fibers can undermine the connection between cortical regions, which may consequently lead to a progressive impact on EF that is mainly served by prefrontal substrates. 75
In addition, some studies have identified HTN-related WM microstructural disruptions, revealing an anterior-to-posterior gradient.28,76,77 This pattern implies that while the adverse effects of persistent HTN extend throughout the brain, they are more pronounced in anterior WM fibers in frontal areas and less prominent in posterior fiber bundles in temporal or occipital regions. Our finding of a disproportionate association between WM fiber disruptions and cognition also partially corresponds with this observed anterior-to-posterior gradient in HTN-related WM pathological changes.
The results of the relations between HTN duration, integrity in NAWM and EF were also in line with previous studies, which suggested that microstructural disintegration of NAWM was evident among HTN individuals, 78 and diffusion measure in NAWM was related to both IQ and EF. 79 Original and FW-corrected DTI metrics within NAWM demonstrate great sensitivity to microstructural abnormalities in various conditions such as CVD and dementia.78,80 Variations in DTI measures within NAWM may hold potential as valuable prognostic indicators for cognitive decline.80,81
The improved sensitivity to early WM changes by FW imaging method
The association between HTN, uncorrected DTI metrics in WM and cognition has been reported by many literatures,59,82 but their association with FW corrected measures has not been examined. Our observations have demonstrated that FW imaging method is capable of detecting the microstructural changes in WM during the early stages of HTN, which cannot be identified through traditional DTI methods. The use of FW-corrected metrics also increased the sensitivity of identifying a greater number of WM tracts that were affected by HTN length, which in turn could be better related to cognitive changes.
As brain atrophy increases in the aging brain, diffusion measures of WM tissue would be greatly affected by the partial volume effects (PVEs) due to cerebrospinal fluid contamination. 83 Besides, the neuroinflammation process occurring in HTN18,19 also increases the extracellular FW content, 84 which demonstrates the need of considering the FW imaging method when studying WM and cognitive changes among the older HTN population. Increasing studies have shown that FW correction algorithm is a promising method to observe more subtle changes in WM microstructure as it enhances the tissue specificity of the DTI-derived diffusion indices by removing PVEs,29,85 and our study extended these findings to older HTN population. Better estimation of WM indices could be more strongly predictive of cognitive alterations, indicating that FW metrics of WM played a unique role in cognitive changes and should be incorporated in models of aging, CVD, and dementia. 86
Additionally, our study also indicated that FW imaging method improved the consistency of different WM indices. Regions of lower FAt values highly corresponded to lower ADt values, but we found no overlap between traditional FA and AD values. The improved consistency has also been found in the context of Alzheimer’s disease. 87 Overall, FW-elimination DTI provides not only early detection of HTN pathology, but also provides more sensitive and consistent DTI-based biomarkers in different disease stages, and thus better capturing hypertensive pathologic processes.
Limitations and future prospects
Despite the considerable strengths of our study, certain limitations need to be acknowledged. Firstly, the cross-sectional nature of the data restricts our ability to make conclusive causal claims. Longitudinal tracking in future research, may provide valuable insights to explore the impact of HTN duration on both brain and cognition. Secondly, our categorization of HTN duration was based on established research and considerations of participants’ distribution, which may have resulted in relatively broad groupings. Future studies could expand the sample size to have a more refined categorization of the disease course. Thirdly, the age of HTN diagnosis was reported as whole numbers and the potential for recall biases exists. Inclusion of detailed medical records from hospitals in future could enhance the accuracy of this information. Fourthly, the reliability and validity of cognitive tests have raised concerns by research, prompting us to use different measures assessing the same domain. Although significant result was not observed in SDMT tests, it was evident that HTN duration indeed exerted a more pronounced impact on PS (reflected by TMT-A) compared to other cognitive domains including memory and language. This discrepancy may be attributed to differences in the sensitivity or contents being measured between the two tests. Therefore, future research should incorporate a broader range of tests to comprehensively assess PS and validate our findings.
Conclusions
Our study is the first study to examine the effect of HTN duration on both white matter macro- and microstructural structures and its link to cognitive domains. We found that the damaging neurological effects of HTN was cumulative, which mainly targeted the EF and PS domains among the elderly. HTN duration is an important determinant of both macrostructural WMH and microstructural disruptions, particularly spreading from the long-range WM fibers to the whole brain. Increasing alterations of WMH and WM integrity underlie the progressive effect of HTN on cognition. FW-elimination metrics were more sensitive and accurate imaging markers for investigating the WM and cognitive changes with the development of HTN. The idea of a slowly progressive effect of HTN on brain and cognition underscored the importance of early intervention. Treating HTN in time and shorting the HTN duration may prevent WM alterations, which potentially preserves cognitive function of elderly person.
Supplemental Material
sj-pdf-1-jcb-10.1177_0271678X231214073 - Supplemental material for Effect of the duration of hypertension on white matter structure and its link with cognition
Supplemental material, sj-pdf-1-jcb-10.1177_0271678X231214073 for Effect of the duration of hypertension on white matter structure and its link with cognition by Zilin Li, Feng Sang, Zhanjun Zhang and Xin Li in Journal of Cerebral Blood Flow & Metabolism
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by STI2030-Major Projects (2022ZD0211600), Natural Science Foundation of China (32171085, 31971038 and 32071100) and Tang Scholar.
Acknowledgements
The authors thank the staff and senior citizen participants in the BABRI study.
Authors’ contributions
ZL conceptualized the study, analyzed the data, interpreted the findings and drafted the manuscript. FS contributed to the data analysis and interpretation. XL and ZZ obtained the funding for the research, conceptualized the study and revised the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplementary material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.