
Abstract
Asymptomatic intracerebral hemorrhage (aICH) is a common phenomenon in patients with acute ischemic stroke (AIS) treated with endovascular thrombectomy (ET). However, the impact of aICH on the functional outcome remains widely unclear. In this study, we aimed at identifying predictors for aICH and analyzing its impact on functional outcome. Patients with AIS due to large artery occlusion in the anterior circulation treated with successful ET were enrolled in a tertiary stroke center. Patients with aICH or without intracerebral hemorrhage were included according to post-treatment CT performed within 72 h; 100 consecutive patients fulfilled the inclusion criteria and 30% classified with aICH. In logistic regression analysis, lower collateral score (OR 0.24; 95% CI 0.12–0.46, p < 0.0001) was significantly associated with aICH. Less patients with aICH achieved an independent outcome (mRS 0–2, 16.7% vs. 44.3%, p = 0.007). Poor outcome (mRS 4–6) was significantly higher in patients with aICH (41.4% vs. 70%, p = 0.021). Patients with aICH had a lower ratio of independent outcome (OR 0.23, 95% CI 0.05–0.1.05, p = 0.041) than without ICH. There were no differences concerning poor outcome (p = 0.5). Lower collateral status was a strong independent predictor for aICH. aICH after successful ET may decrease the likelihood of an independent functional outcome without influencing poor outcome.
Introduction
Up to date, multiple clinical studies have examined the impact of endovascular treatment (ET)-associated symptomatic intracerebral hemorrhage (sICH) on clinical outcome.1–3 Asymptomatic intracranial hemorrhage (aICH) is a more common phenomenon after ET in acute ischemic stroke (AIS) patients, with an occurrence of approximately 30%–40%.4–6 However, its prognostic impact remains up-to-date insufficiently evaluated and available data is often undermined by contradictory results or heterogeneous control trials.2,7 A recent clinical study from Hao et al. presented a large multicenter registry study with over 600 patients analyzing the impact of aICH in AIS patients after ET on the 90 days functional clinical outcome. According to the conclusive results, aICH decreased the probability for an excellent clinical outcome (mRS 0–1).2,5 Mitigating arguments enclosed an exclusive Asian patient cohort indicating limited translation to the western population. 5 On the contrary, minor or aICH have been suggested as an indicator of successful vessel reperfusion in patients treated with intravenous rtPA. 8 Is ET-associated aICH a negligible phenomenon and clinically innocuous or even a sign of successful vessel reperfusion? And if so, which specific risk factors are associated with an aICH after ET? To answer this set of questions, we hypothesized that aICH negatively impacts functional outcome after 90 days in AIS patients undergoing successful ET. To test and evaluate this hypothesis, we used the widely accepted Heidelberg Bleeding Classification and examined whether the occurrence of aICH affects functional clinical outcome after 90 days in patients with AIS who underwent successful ET, and evaluated risk factors of aICH in these patients. 9
Methods
Study population
AIS patients were enrolled retrospectively in our university hospital, which is a high-volume tertiary stroke center, between June 2015 and March 2018 (Figure 1). Patients with ischemic stroke with large vessel occlusion and subsequent ET were studied. As inclusion criteria, we defined: (1) evidence of large vessel occlusion of the middle cerebral artery (MCA) or terminal internal carotid artery (ICA); (2) initially performed multimodal CT protocol with CT angiography (CTA) and perfusion CT (CTP) and follow-up CT within 72 h after imaging; (3) thrombolysis in cerebral infarction scale (TICI) 2b or 3; (4) known time from symptom onset to imaging <6 h; (5) National Institute of Health Stroke scale (NIHSS) score above 3; (6) documented modified Ranking Scale (mRS) after 90 days; (7) absence of a preexisting thromboembolic or hemodynamic infarctions in admission non-enhanced CT (NECT). Patients were excluded for the following reasons: (1) occlusion in posterior circulation, (2) recanalization with TICI 0-2a, (3) inadequate clinical documentation or missing patient consent, (4) contrast extravasation, (5) inadequate image acquisition, (6) SICH after ET. Baseline patient characteristics were retrieved from medical records, including modified Rankin Scale (mRS) after 90 days. ASPECTS rating was performed by an experienced neuroradiologist and verified by an attending neuroradiologist. Discrepancies about the ASPECTS were settled by joint discussion of the two readers. Recanalization status was derived for every patient: (a) vessel recanalization after successful thrombectomy (TICI 2b or 3); (b) persistent large vessel occlusion in patients with failed recanalization after endovascular thrombectomy (TICI 0–2a) or patients who did not receive ET. The neuroradiologist who performed the intra-arterial procedure documented the TICI scores with subsequent verification by a second attending neuroradiologist. Inaccuracies were corrected in consensus reading, if necessary. This single center retrospective study was approved by the ethics committee (Ethik-Kommission der Ärztekammer Hamburg, WF-018/15) and written informed consent was waived by the institutional review board. All study protocols and procedures were conducted in accordance with the Declaration of Helsinki. The data that support the findings of this study are available from the corresponding author upon reasonable request.
Patient flowchart. Patient enrollment according to inclusion and exclusion criteria.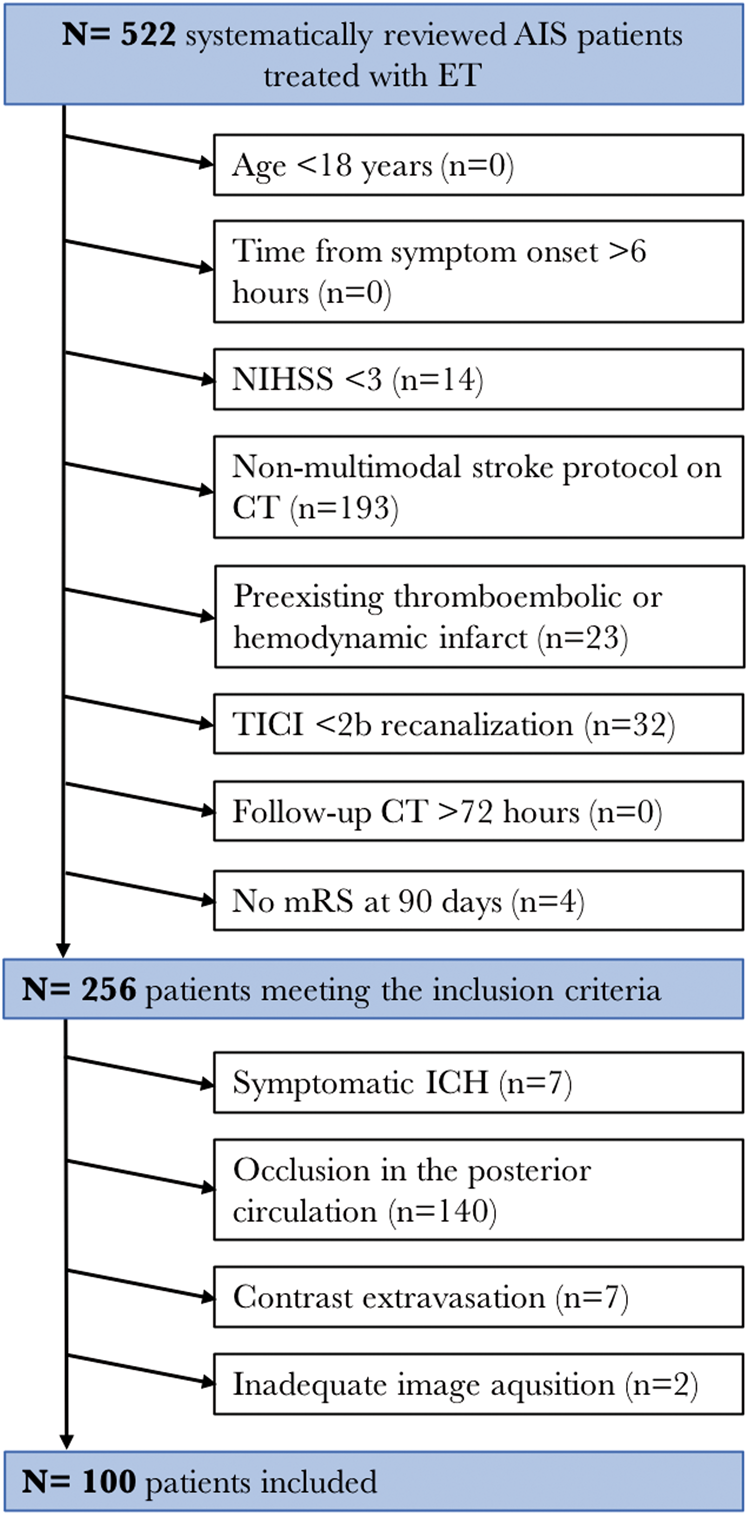
Image acquisitions
All CT scans were performed on a 256 slice scanners (Philips iCT 256) with the following imaging parameters: NECT with 120 kV, 280–320 mA, 5.0 mm slice reconstruction; CTA: 100–120 kV, 260–300 mA, 1.0 mm slice reconstruction, 5 mm MIP reconstruction with 1 mm increment, 0.6-mm collimation, 0.8 pitch, H20f soft kernel, 80 mL highly iodinated contrast medium and 50 mL NaCl flush at 4 mL/s; scan starts 6 s after bolus tracking at the level of the ascending aorta. CTP: 80 kV, 200–250 mA, 5 mm slice reconstruction (max. 10 mm), slice sampling rate 1.50 s (min. 1.33 s), scan time 45 s (max. 60 s), biphasic injection with 30 ml (max. 40 ml) of highly iodinated contrast medium with 350 mg iodine/ml (max. 400 mg/ml) injected with at least 4 ml/s (max. 6 ml/s) followed by 30 ml sodium chloride chaser bolus. All perfusion datasets were inspected for quality and excluded in case of severe motion artefacts.
Post-procedure evaluations
CTA collaterals were evaluated independently by two neuroradiologists with two (JN) and six (UH) years of dedicated neuroradiology experience, blinded to all clinical and imaging information except stroke side. Collateral status was assessed independently on admission intracranial CTA MIPs and scored according to the grading system of Souza et al. 10 into grades 0 to 4, ranging from grade 0 (no collateral) to grade 4 (increased collaterals). A follow-up CT was usually performed within 72 h after each ET; additional CT scans were performed whenever an ICH was indicated by clinical symptoms. Bleeding events were evaluated on follow-up CT and classified according to the widely accepted Heidelberg Bleeding Classification into sICH or aICH 9 (online supplementary material). Hyperdense phenomena without mass effect on CT that disappeared or weakened significantly within 24 h of ET was classified as contrast extravasation. 11 The functional outcome was assessed using the mRS at 90 days after ET by a certified investigator or study nurse. We defined two binary outcomes: independent outcome was defined as mRS score of 0–2, poor outcome was defined as mRS 4–6, respectively.12,13
Statistical analysis
Kolmogorov–Smirnov tests were used to determine if the data sets were well-modeled by a normal distribution. For categorical data, absolute and relative frequencies are given. Univariable distribution of metric variables is described by median and interquartile range (IQR). Patients without ICH versus with aICH were compared by Mann–Whitney U test for metric outcome variables and by Chi-square test for categorical outcome variables. Interrater reliability was measured with kappa statistic and calculating Cohen’s k. Logistic regression analysis was performed to evaluate potential risk factors for developing an aICH. Secondly, the association of aICH on independent and poor outcome was analyzed. Univariate analysis was followed by multivariable analysis based on significant independent variables using stepwise forward selection (inclusion: p-value in univariate analysis test ≤0.05). Two-tailed p-values of <0.05 were considered statistically significant. Statistical analyses were performed using SPSS version 25 (IBM Corporation, Armonk NY).
Results
A total of 100 patients with AIS treated with successful ET were included in this study (Figure 1). According to the Heidelberg Bleeding Classification, 30 patients (30%) were classified with aICH within 72 h after ET (Figure 2); 7 patients with classified sICH were excluded according to the exclusion criteria. Interobserver agreement in the collateral score classification was good (Cohen’s Kappa: 0.91; 95% CI 0.86–0.95; p < 0.001).
Distribution of bleeding events in patients with asymptomatic intracerebral hemorrhage after ischemic stroke according to the Heidelberg Bleeding Classification.
6
(a) Distribution of bleeding events in patients with asymptomatic intracerebral hemorrhage (aICH) after successful endovascular thrombectomy (ET). (b) Distribution of patients with asymptomatic intracerebral hemorrhage (aICH) and no intracerebral hemorrhage (ICH) after successful endovascular thrombectomy (ET).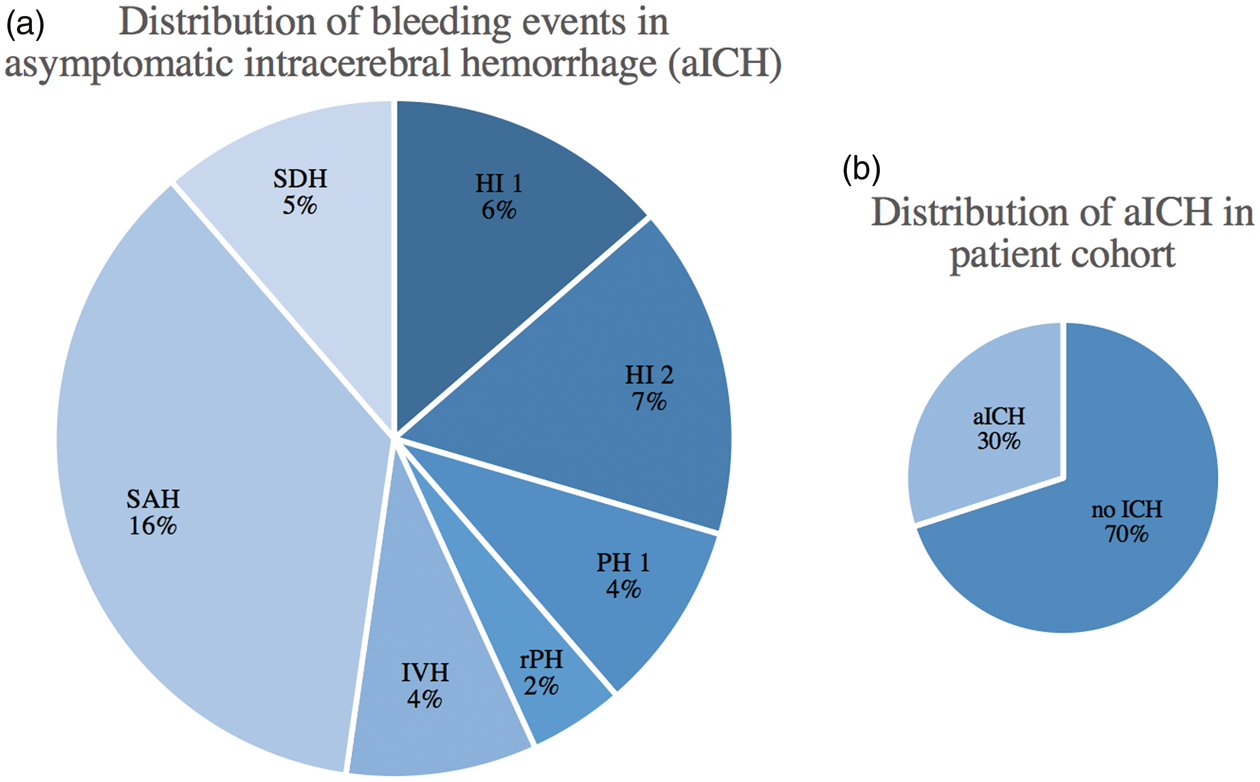
Predictors of aICH
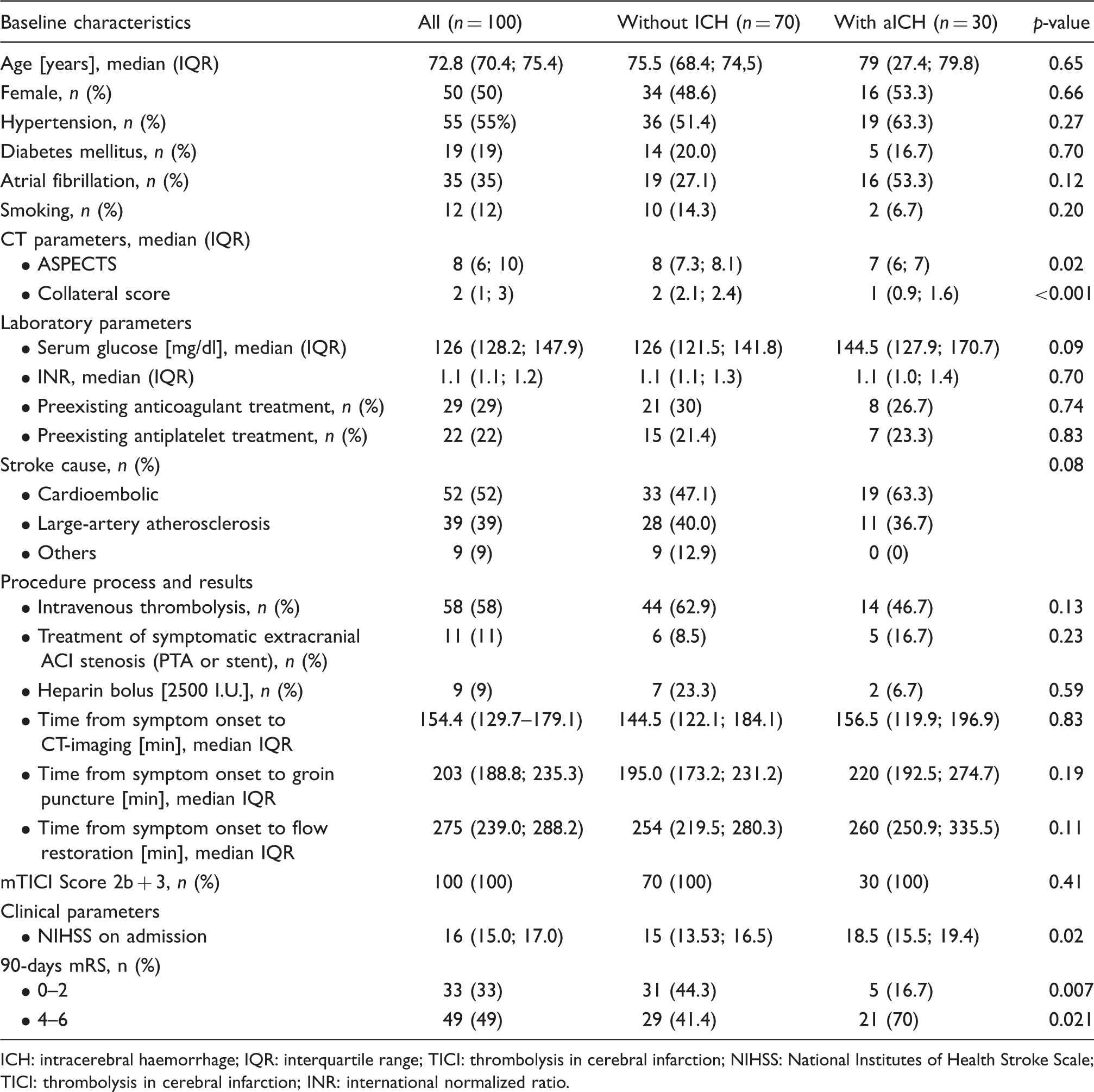
As shown in Table 1, analysis of CT parameters in aICH patients displayed a significantly lower collateral status (median 1 vs. 2, p = 0.001) and lower ASPECTS (7 vs. 8, p = 0.02). Laboratory parameters demonstrated only by tendency a higher baseline serum glucose in patients with aICH (median 144.5 mmol/L; IQR: 127.9–170.7 vs. 126 mmol/L (121.5–141.8); p = 0.09). Direct ET-associated variables demonstrated one more retrieval pass in patients with aICH with a median of 2 (IQR: 1.9–3.2 vs. 1; IQR: 1.5–2.2; p = 0.03). Clinical parameters on admission, such as NIHSS displayed a significant higher median of 18.5 (15.5–19.4) compared to a median of 15 in patients without ICH (IQR: 13.53–16.5; p = 0.02). In order to evaluate the risk factors of aICH, potential independent variables were analyzed in multivariate logistic regression. For the analysis, variables with significance (p < 0.05) in univariate analysis were determined (online supplementary material). Low collateral score (OR 0.24; 95% CI 0.12–0.46, p < 0.0001) was independently associated with aICH after successful ET (Figure 3 and online supplementary material).
Probability of asymptomatic intracerebral hemorrhage (aICH) after successful endovascular treatment by collateral score after logistic regression analysis adjusted for age and sex. Impact of collateral score (x-axis) on the probability of asymptomatic intracerebral hemorrhage (aICH) after successful recanalization (y-axis) based on multivarible linear regression analysis adjusted for sex and age. The probability for developing aICH was modulated by the level of collateral score (0–4). Collateral score was determined according to Souza et al. Malignant CTA collateral profile is highly specific for large admission DWI infarct core and poor outcome in acute stroke. AJNR Am J Neuroradiol 2012; 33: 1331–1336. aICH: asymptomatic intracerebral hemorrhage (). Comparison of baseline demographic, clinical and radiological characteristics between patients with hemorrhagic transformation and those with no hemorrhagic transformation. ICH: intracerebral haemorrhage; IQR: interquartile range; TICI: thrombolysis in cerebral infarction; NIHSS: National Institutes of Health Stroke Scale; TICI: thrombolysis in cerebral infarction; INR: international normalized ratio.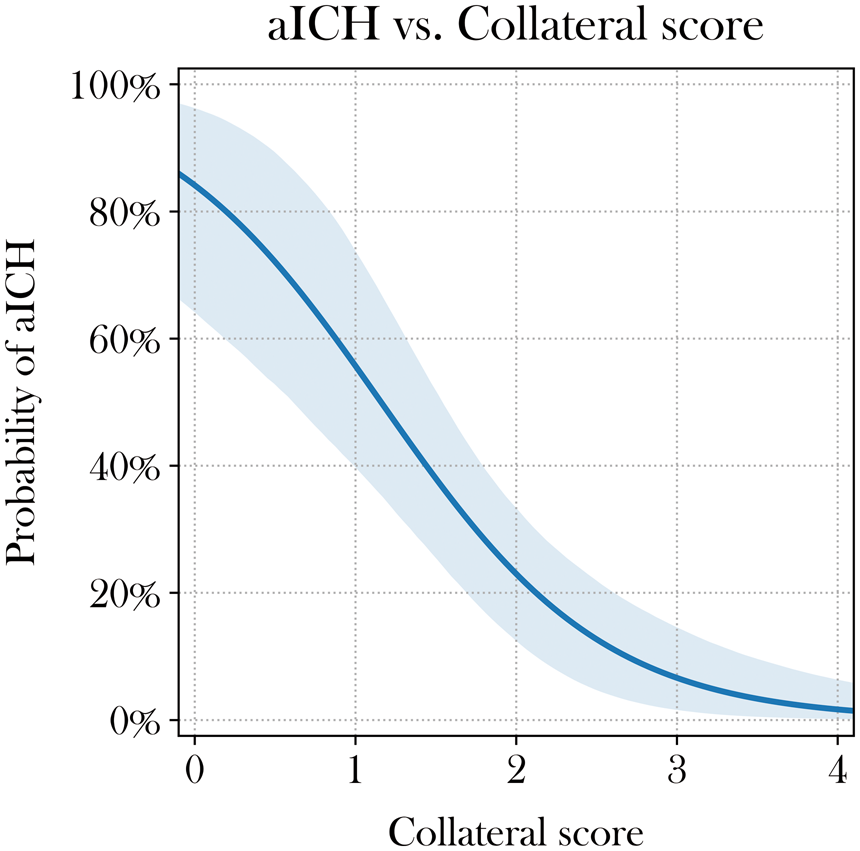
Clinical outcomes
Less patients with aICH achieved independent outcome (mRS ≤2) at 90 days (16.7% vs. 44.3% p = 0.007). Poor outcome (mRS ≤4–6) was significantly higher in patients with aICH (70% versus 41.4%; p = 0.021) (Table 1 and Figure 4).
Distribution of modified Rankin Scale (mRS) at 90 days in patients with asymptomatic intracerebral hemorrhage (aICH) and no intracerebral hemorrhage (ICH).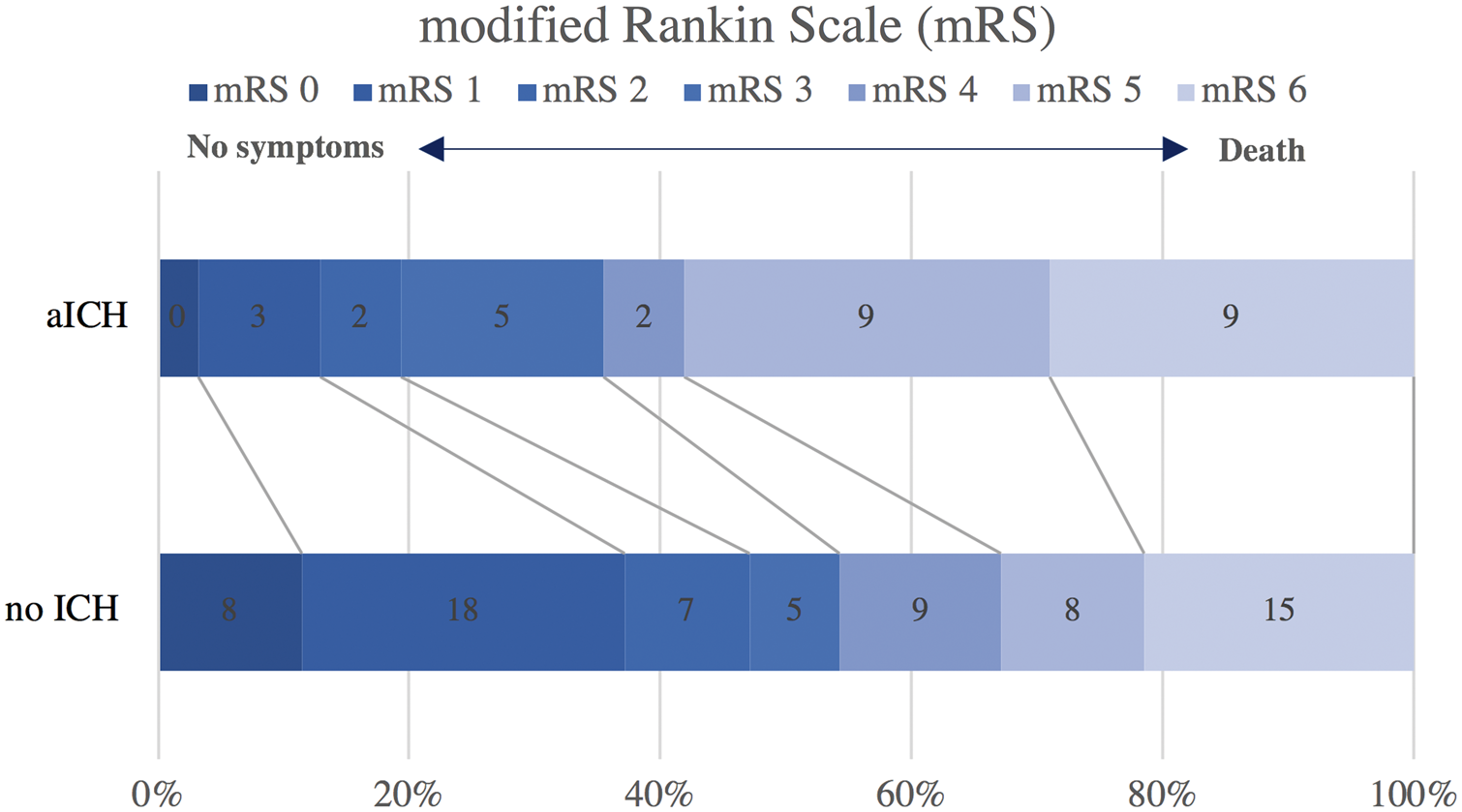
Univariate analysis of predictors of independent outcome (mRS 0–2) and poor outcome (mRS 4–6) after recanalization at 90 days.
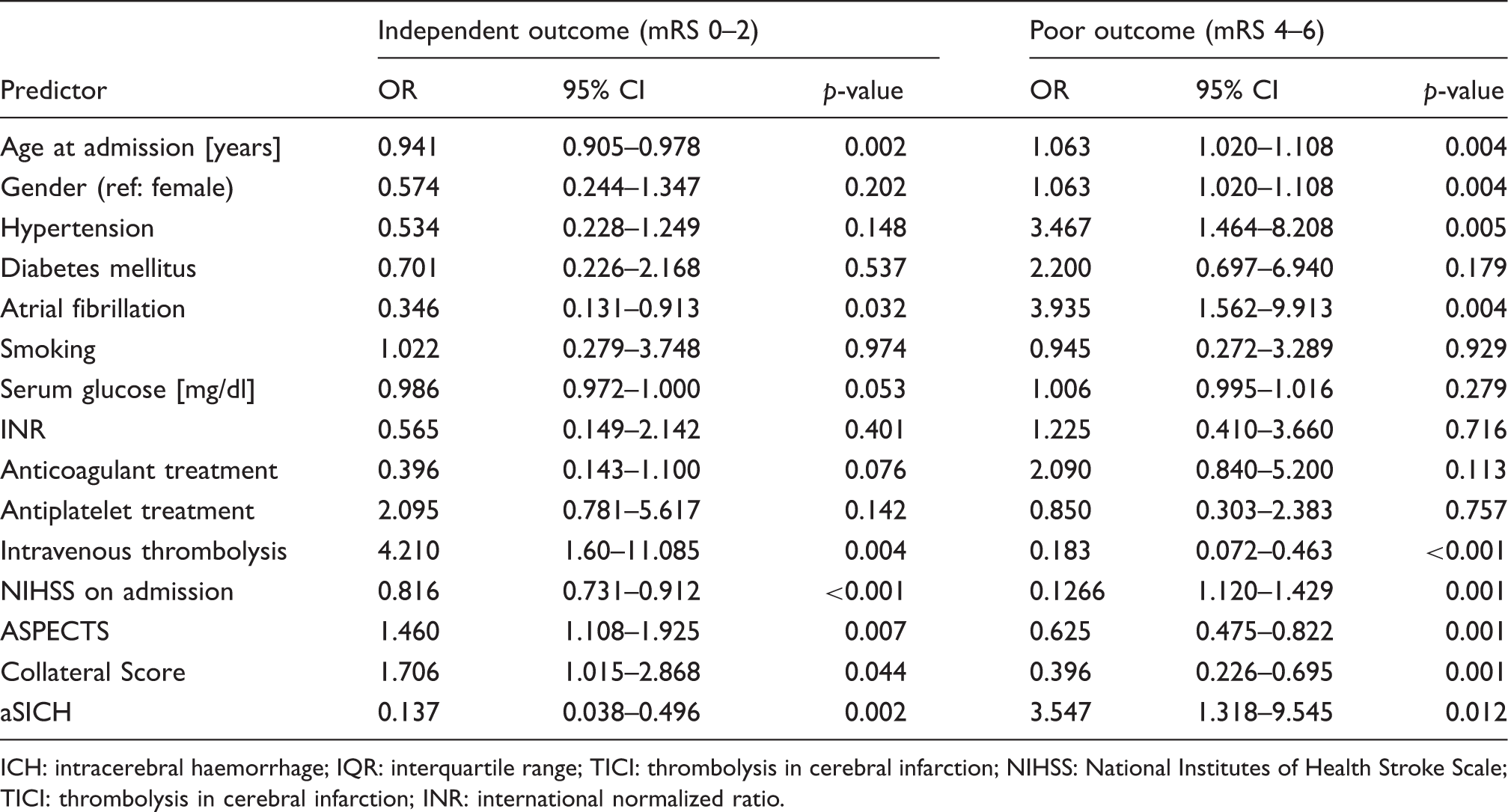
ICH: intracerebral haemorrhage; IQR: interquartile range; TICI: thrombolysis in cerebral infarction; NIHSS: National Institutes of Health Stroke Scale; TICI: thrombolysis in cerebral infarction; INR: international normalized ratio.
Multivariate analysis of predictors of independent outcome (mRS 0–2) and poor outcome (mRS 4–6) after recanalization at 90 days.
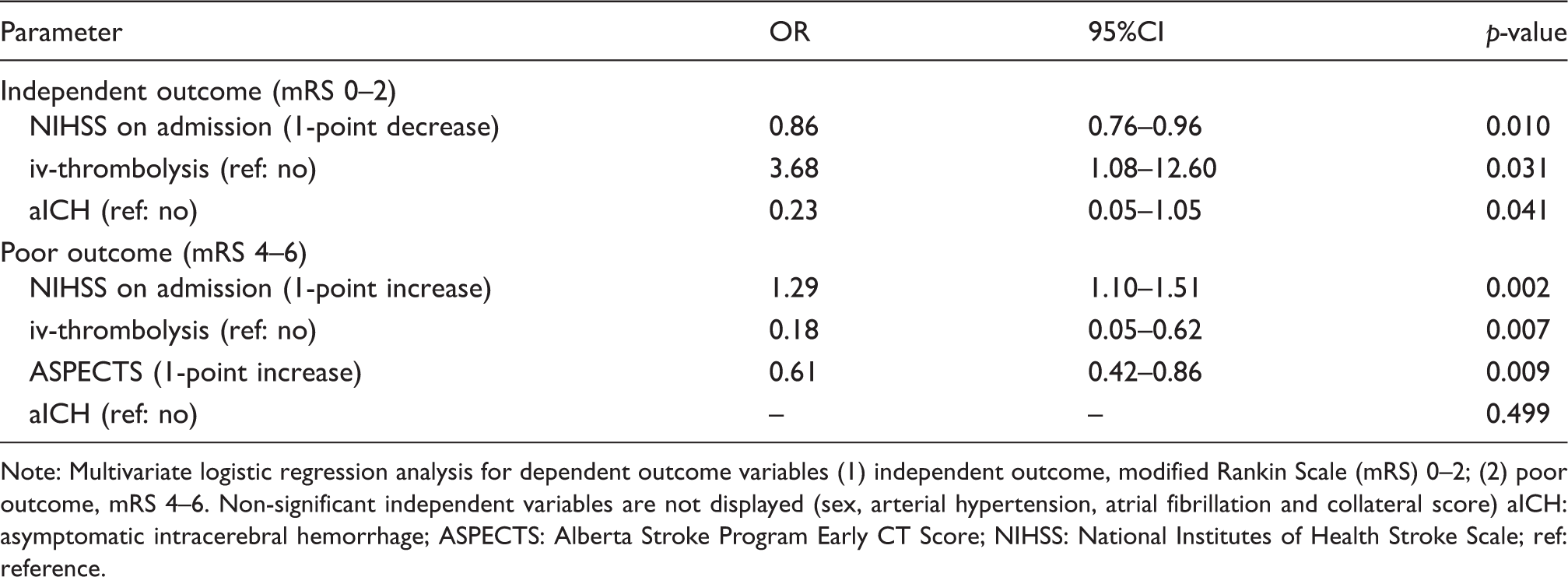
Note: Multivariate logistic regression analysis for dependent outcome variables (1) independent outcome, modified Rankin Scale (mRS) 0–2; (2) poor outcome, mRS 4–6. Non-significant independent variables are not displayed (sex, arterial hypertension, atrial fibrillation and collateral score) aICH: asymptomatic intracerebral hemorrhage; ASPECTS: Alberta Stroke Program Early CT Score; NIHSS: National Institutes of Health Stroke Scale; ref: reference.
Discussion
Our study focused on the analysis of the independent predictors of aICH and secondly, the prognostic value of aICH on functional outcome, specifically for independent outcome as opposed to poor outcome. In our study, aICH was associated with a lower ratio of independent outcome (OR 0.23; 95% CI 0.05–1.05, p = 0.041). No significant influence of aICH on poor outcome was found. These findings appear to be consistent with results from a recently published large multicenter trial study which included over 600 patients. 5 Conclusively, aICH was evaluated as a risk factor for decreased likelihood of an excellent functional outcome after ET, an effect on mortality was not given. 5 Consistent with this last notion, the proportion of patients with aICH after ET (33.5%) was similar to that reported in our study (30%), and also to that reported in the Randomized Assessment of Rapid Endovascular Treatment of Ischemic Stroke (ESCAPE) trial (36.4%). 14 Our study assesses the authors’ limitation. According to the authors, the findings may not be generalizable to other populations.
The negative effect of aICH on clinical outcome is reinforcing the identification and relevance of specific risk factors for these patients. Recently, published data provide evidence that low ASPECTS and i.v. thrombolysis are both associated with the risk of aICH after ET. 15 The early disruption of the blood–brain barrier has been attributed to this phenomenon, and yet the assessment of a collateral grading was lacking.5,15 The extent of leptomeningeal collaterals has recently been investigated as a predictor for clinical outcome and the occurrence of sICH.1,16 Noninvasive assessment of the extent of collaterals is most commonly performed using conventional CTA and provides maximal spatial and temporal resolution for depiction of the anatomical and functional capacity of collaterals.16,17 This is the first study to directly investigate the association of collateral score on the risk of aICH using an established scoring system. 10 The finding of a predominant role of collateral circulation bypasses the effect of ASPECTS and i.v. thrombolysis as previously reported. 15 In line with this, Liebeskind et al. 17 reported that successful ET may not be synonymous with subsequent clinical function, as more robust baseline collaterals determined more accurately tissue viability and subsequent clinical outcomes, including ICH events.
The results obtained in this study confirm that aICH is a common complication in AIS patient undergoing ET and appears to be associated with worse functional outcomes.5,4,18 Although initially classified as asymptomatic, aICH also impairs the long-term functional outcome beyond 90 days, with a significant higher proportion of mortality and less independent outcomes. 18 In conclusion, in contrast to the labeling, aICH may not be completely asymptomatic, and not sufficiently detectable by neurological assessment scales (e.g. NIHSS score or other scales), therefore also requiring additional consideration of radiologic markers. Our prediction model depicts a good predictive ability for the risk of aICH in patients with AIS treated with successful ET in a real-world practice. The model may aid clinicians to identify patients with the highest as well as the lowest risk of aICH, especially in patients with low collateral status. However, we cannot propose withholding treatment with ET in patients otherwise eligible according to current guidelines. To address this, future studies using a scoring system with collateral score would be conceivable. An external validation of our model is warranted. Future studies should consider using uniformed definitions and standardized procedures in diagnosing ICH.
Of note, intravenous thrombolysis (IVT) was a significant independent variable for both predicting independent and poor outcome, and thus the effect size was higher in independent outcome prediction. The results in this study are only indicative of a beneficial effect of IVT on functional outcome. Ultimately, treatment with IVT before ET remains highly controversial.19,20
Several limitations should be addressed when interpreting the results of the present study. Firstly, our study is based on a retrospective study design and a relatively small number of patients due to strict inclusion criteria to obtain a homogenous patient cohort and to avoid bias. Another point of criticism is the strict inclusion of patients with terminal ICA and MCA occlusion to obtain a homogenous patient cohort and to avoid bias. Further, different thrombectomy devices were used in our study. The types of endovascular device may influence the risk of ICH.
Conclusion
Poor collateral status was a strong independent predictor for aICH. Asymptomatic ICH after ET may decrease the likelihood of an independent functional outcome but does not influence poor outcome at 90 days in patients with AIS treated with successful ET.
Supplemental Material
Supplemental material for Clinical relevance of asymptomatic intracerebral hemorrhage post thrombectomy depends on angiographic collateral score
Supplemental Material for Clinical relevance of asymptomatic intracerebral hemorrhage post thrombectomy depends on angiographic collateral score by Jawed Nawabi, Helge Kniep, Gabriel Broocks, Tobias D Faizy, Gerhard Schön, G Thomalla, Jens Fiehler and Uta Hanning in Journal of Cerebral Blood Flow & Metabolism
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J. Fiehler: Consultant for Acandis, Boehringer Ingelheim, Codman, Microvention, Sequent, Stryker. Speaker for Bayer Healthcare, Bracco, Covidien/ev3, Penumbra, Philips, Siemens. Grants from Bundesministeriums fuür Wirtschaft und Energie (BMWi), Bundesministerium fuür Bildung und Forschung (BMBF), Deutsche Forschungsgemeinschaft (DFG), European Union (EU), Covidien, Stryker (THRILL study), Microvention (ERASER study), Philips G Thomalla has received personal fees from Acandis, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb/Pfizer, Daichi Sankyo, Stryker, grants and personal fees from Bayer, grants from the German Research Foundation, Corona Foundation, German Innovation Fund. No disclosures reported for Dres Nawabi, Broocks, Faizy, Hanning, Mr. Schön and Mr. Kniep also report no disclosures.
Author's contribution
Jawed Nawabi: Study design. Acquisition of data. Image processing. Image analysis. Data analysis. Statistical analysis. Drafting the manuscript and revising it critically. Helge Kniep: Image processing. Image analysis. Statistical analysis. Data analysis. Drafting the manuscript and revising it critically. Gabriel Broocks: Data analysis. Drafting the manuscript and revising it critically. Tobias F Faizy: Data analysis. Drafting the manuscript and revising it critically. Gerhard Schön: Study design. Statistical analysis. Data analysis. Drafting the manuscript and revising it critically. Götz Thomalla: Data analysis. Drafting the manuscript and revising it critically. Jens Fiehler: Study design. Data analysis. Drafting the manuscript and revising it critically. Uta Hanning: Study design. Acquisition of data. Image analysis. Data analysis. Drafting the manuscript and revising it critically.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.