
Abstract
Cerebral amyloid angiopathy (CAA) is a common cause of cognitive impairment in older individuals. This study aimed to investigate predictors of dementia in CAA patients without intracerebral hemorrhage (ICH). A total of 158 non-demented patients from the Stroke Service or the Memory Clinic who met the modified Boston Criteria for probable CAA were included. At baseline, neuroimaging markers, including lobar microbleeds (cerebral microbleeds (CMBs)), white matter hyperintensities (WMH), cortical superficial siderosis (cSS), magnetic resonance imaging (MRI)-visible centrum semiovale perivascular spaces (CSO-PVS), lacunes, and medial temporal atrophy (MTA) were assessed. The overall burden of small vessel disease (SVD) for CAA was calculated by a cumulative score based on CMB number, WMH severity, cSS presence and extent and CSO-PVS severity. The estimated cumulative dementia incidence at 1 year was 14% (95% confidence interval (CI): 5%–23%), and 5 years 73% (95% CI: 55%, 84%). Age (hazard ratio (HR) 1.05 per year, 95% CI: 1.01–1.08, p = 0.007), presence of MCI status (HR 3.40, 95% CI: 1.97–6.92, p < 0.001), MTA (HR 1.71 per point, 95% CI: 1.26–2.32, p = 0.001), and SVD score (HR 1.23 per point, 95% CI: 1.20–1.48, p = 0.030) at baseline were independent predictors for dementia conversion in these patients. Cognitive deterioration of CAA patients appears attributable to cumulative changes, from both vasculopathic and neurodegenerative lesions.
Introduction
Cerebral amyloid angiopathy (CAA) is a common age-related cerebral small vessel disease (SVD) and an increasingly recognized cause of vascular cognitive impairment and dementia in the elderly. 1 Spontaneous lobar intracerebral hemorrhage (ICH) is the most commonly recognized clinical presentation in CAA patients. 2 However, the majority of the patients with CAA never experience ICH during their lifetime. 3 The broad availability of magnetic resonance imaging (MRI) has increased the ability to diagnose probable CAA patients without ICH based on the presence of multiple strictly lobar microbleeds. 4 Many patients with probable CAA are evaluated and diagnosed in memory clinics with cognitive impairment or in stroke services with stroke-like symptoms.
Previous studies have reported that SVD related neuroimaging markers, rather than ICH characteristics, are associated with the long-term dementia incidence in patients with ICH.5,6 The association between CAA pathology and cognitive impairment has been widely reported.7–9 However, it is still unclear how patients deteriorate over time and, if so, what risk factors predict cognitive deterioration and dementia conversion in CAA patients who do not present with ICH.
Characteristic clinical neuroimaging features of CAA include cerebral microbleeds (CMBs), white matter hyperintensities (WMH), enlarged perivascular spaces (PVS) in the cerebral white matter, and cortical superficial siderosis (cSS). 2 Recently, a SVD score based on these four most salient MRI markers of CAA was shown to be correlated with CAA severity at autopsy. 10 Additionally, global cortical atrophy (GCA) and medial temporal atrophy (MTA) are established neuroimaging features of both SVD injury and neurodegenerative disorders.11–13 A recent study reported cortical thinning and hippocampal atrophy in sporadic and hereditary CAA patients. 14 However, it is unknown whether any of these individual neuroimaging markers predict dementia conversion in patients with CAA or whether dementia conversion is more strongly associated with the cumulative effect of SVD (measured by the SVD score). We hypothesized that the progression to dementia in CAA patients without ICH is best predicted by cumulative injuries rather than by any one injury type.
Methods
Study population
We included consecutive patients meeting modified Boston criteria for probable CAA
15
in the absence of ICH who presented between January 1994 and November 2015 to the Massachusetts General Hospital Stroke Service (inpatient and outpatient services) and Memory Clinic associated with the Massachusetts Alzheimer’s Disease Research Center.
16
A total of 647 patients with CMBs but no ICH were assessed for eligibility, including 205 subjects from the Stroke Service
17
and 442 subjects from the Memory Clinic. Inclusion criteria included age ≥ 55 years old; MRI results meeting one of the two criteria: (a) multiple microbleeds restricted to lobar, cortical, or corticosubcortical regions (cerebellar microbleeds allowed) or (b) a single lobar, cortical, or corticosubcoritcal microbleed and focal or disseminated superficial siderosis; absence of other cause of hemorrhage or superficial siderosis. Patients with a history of ICH or with ICH at baseline were excluded. Additionally, patients with strictly deep microbleed(s), mixed (deep and lobar) microbleeds, CAA related inflammation, and patients with MRI scans inadequate for SVD markers assessment (missing sequences or degraded quality) were excluded (n = 386). Furthermore, patients with the diagnosis of dementia at baseline and patients without a neurological follow-up visit were excluded (n = 103). A total of 158 patients (87 patients from the Stroke Service, 71 from the Memory Clinic) were included into the analysis. Figure 1 shows the flow chart of enrollment. This study was performed in accordance with the guidelines and with approval of the institutional review boards from our institution.
“Other” refers to patients excluded for being scanned for unrelated events or as part of a systematic and non-related protocol for different diseases. “Mixed” refers to the mixture of lobar and deep.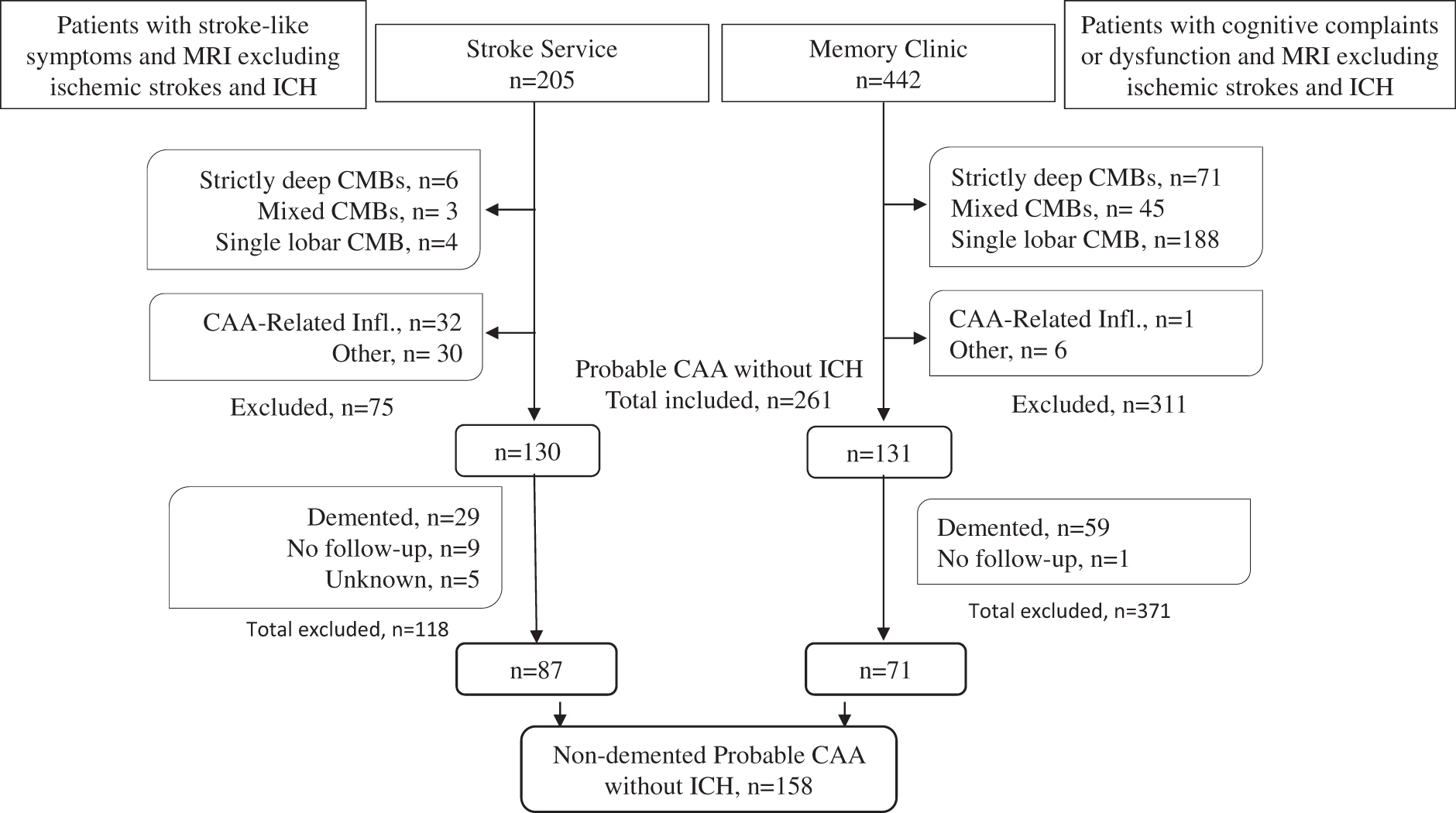
Baseline clinical data
The baseline clinical data, including demographic variables, medical history, and cognitive status, were obtained at the hospital visit through in-person interview with patients or surrogates within 3 months of the baseline MRI scan. Based on the clinical assessment of daily living function status and neuropsychological tests, patients were diagnosed as cognitively normal, mild cognitive impairment (MCI), or dementia according to National Institute on Aging and Alzheimer’s Association workgroup criteria. 18
Baseline neuroimaging acquisition and analysis
All participants underwent a clinical 1.5 T MR scan (Siemens Healthcare, Magnetom Avanto, Erlange, Germany) using a standardized protocol. MRI sequences for all subjects included whole brain T1-weighted, T2-weighted, T2*-weighted gradient-recalled echo (T2*-GRE; echo time (TE) 750/50 ms, 5 mm slice thickness, 1 mm inter-slice gap) and fluid attenuated inversion recovery (FLAIR; TR/TE 10,000/140 ms, inversion time 2200 ms, 5 mm slice thickness, 1 mm inter-slice gap).
Neuroimaging markers of SVD were evaluated according to STRIVE consensus criteria.
19
MRI images were analyzed blinded to all clinical information by two trained raters (G.B. & A.C.) and consensus was obtained for each case. The imaging markers measured in this study include WMH severity; presence of lacunes; number of CMBs; absent, focal or disseminated cSS; presence and severity of enlarged PVS; MTA and GCA. WMH volumes were measured on axial FLAIR sequences using a previously described semi-automated segmentation method in MRIcron software (University of South Carolina, USA).
20
Periventricular and deep WMH were also classified using the 0–3 Fazekas scale,
21
and the sum of these two scores was used to represent the total severity of WMH of each subject as previously described.
22
Lacunes were defined as round or ovoid fluid-filled cavities of between 3 and 15 mm in diameter and were dichotomized as being present or absent.
19
Lobar CMBs were defined on axial blood-sensitive MR images as punctate foci of hypointensity less than 10 mm in diameter, distinct from vascular flow voids and leptomeningeal hemosiderosis.
23
Superficial siderosis was defined as curvilinear hyposignal in the superficial layers of the cerebral cortex, distinct from the vessels. FLAIR images were used for anatomical confirmation of the gyral location of these signal hypointensities. According to a validated scale, the status of cSS was classified as absent, focal (restricted to ≤3 sulci), or disseminated (affecting 4 or more sulci).
15
Enlarged PVS were rated on axial T2-weighted MR images, in the basal ganglia (BG) and centrum semiovale (CSO), using a validated 4-point visual rating scale.
23
GCA was rated on axial brain T1 weighted imaging. The mean score for cortical atrophy throughout the complete cerebrum was classified as 0 (no cortical atrophy), 1 (mild atrophy, opening of sulci), 2 (moderate atrophy, volume loss of gyri), and 3 (severe atrophy, “knife blade” atrophy).
24
T1-weighted coronal images were displayed for MTA evaluation. MTA was visually scaled from 0 to 4 based on the width of the choroid fissure, the width of the temporal horn, and the height of the hippocampal formation.
25
We subsequently categorized the four signature MRI markers of CAA (lobar CMBs, WMH according to Fazekas, CSO-PVS, and cSS) according to the recently published MRI SVD score for CAA, yielding an ordinal score of total SVD burden ranging from 0 to 6.
10
Figure 2 illustrates the examples of CAA related neuroimaging markers including CSO-PVS, lobar CMBs, cSS, and lacune.
Multiple bilateral lobar microbleeds (CMBs) detected on T2*-GRE. These microbleeds are round or ovoid shaped hypointense signal on T2*-GRE/SWI and generally 2–5 mm in diameter (a). Centrum semiovale perivascular spaces (CSO-PVS) with signal intensity similar to CSF detected on T2. These fluid-filled spaces follow the typical course of a vessel and appear linear, round, or ovoid (b). Focal cortical superficial siderosis (cSS) detected as curvillinear signal in the superficial layer of the cerebral cortex on T2*-GRE (c). One lacune detected on T2-FLAIR (d). Lacunes are generally round or void (3–15 mm in diameter), subcortical and fluid-filled cavity with signal intensity similar to CSF.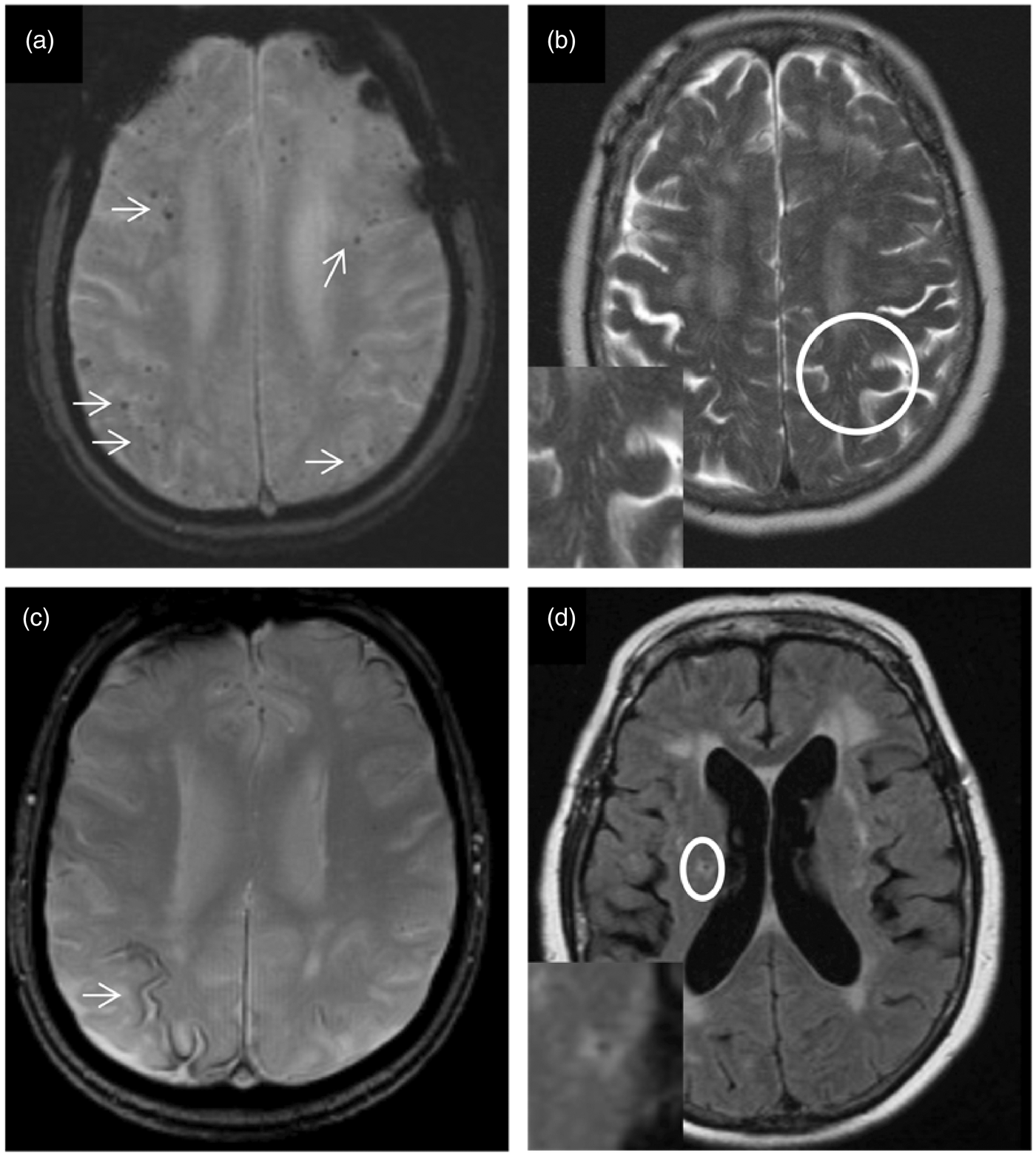
Cognitive status on follow-up
Clinical visits were systematically reviewed to determine if dementia was present at follow-up. If dementia occurred, time to event was recorded. Clinical events including ischemic stroke and hemorrhagic stroke were recorded during follow-up. Diagnosis of normal cognition, MCI, and dementia was determined based on the clinical assessment of daily living function status according to National Institute on Aging and Alzheimer’s Association workgroup criteria.18,26 Patients with normal cognition or MCI at follow-up were characterized as “non-converters,” while those who developed dementia were characterized as “converters.” The tests employed include Blessed Dementia Scale (BDS) and Clinical Dementia Rating (CDR).
Statistics
Comparisons on demographic characteristics and medical history between probable CAA patients from the Stroke Service and the Memory Clinic were performed using the independent sample t-test for continuous variables and chi square test for categorical variables as appropriate. Mann–Whitney U test was conducted for the comparison of WMH volume and CMB number because of their skewed distributions.
Time to event was calculated by subtracting the date of baseline MRI scan from the date of dementia diagnosis or the last reliable follow-up time point for non-convertors. Last reliable follow-up time was set as censoring time in the survival analyses. Univariable Cox proportional hazards models were conducted to calculate unadjusted hazard ratio (HR) for the risk of dementia conversion of each potential neuroimaging predictor and any other plausible or previously reported potential predictors, including age, sex, education, history of hypertension, hypercholesterolemia, diabetes mellitus, ischemic stroke, transient ischemic attack, and cardiac artery disease. The variables with p values less than 0.1 in the univariable analysis were entered into multivariable Cox proportional hazards models. Two separate multivariate analyses were performed including either selected individual neuroimaging markers of CAA or the total SVD composite score. Stepwise backward elimination was subsequently used to generate the best minimal model by eliminating non-significant variables (p > 0.05). Multicollinearity was assessed using variance inflation factors (VIF) and predictors with VIF > 2.5 were removed from the model.
The SPSS 21 statistical package was used for statistical analysis (IBM Corp., Armonk, NY), and JMP Pro 12 (2015, JMP® Pro 12. Cary, NC: SAS Institute, Inc) was used for distribution profiler and 5-year prediction. Significance level was set at 0.05 for all analyses.
Results
Demographic, clinical, and neuroimaging characteristics of CAA patients at baseline
Demographic, clinical, and neuroimaging characteristics of the patients at baseline.
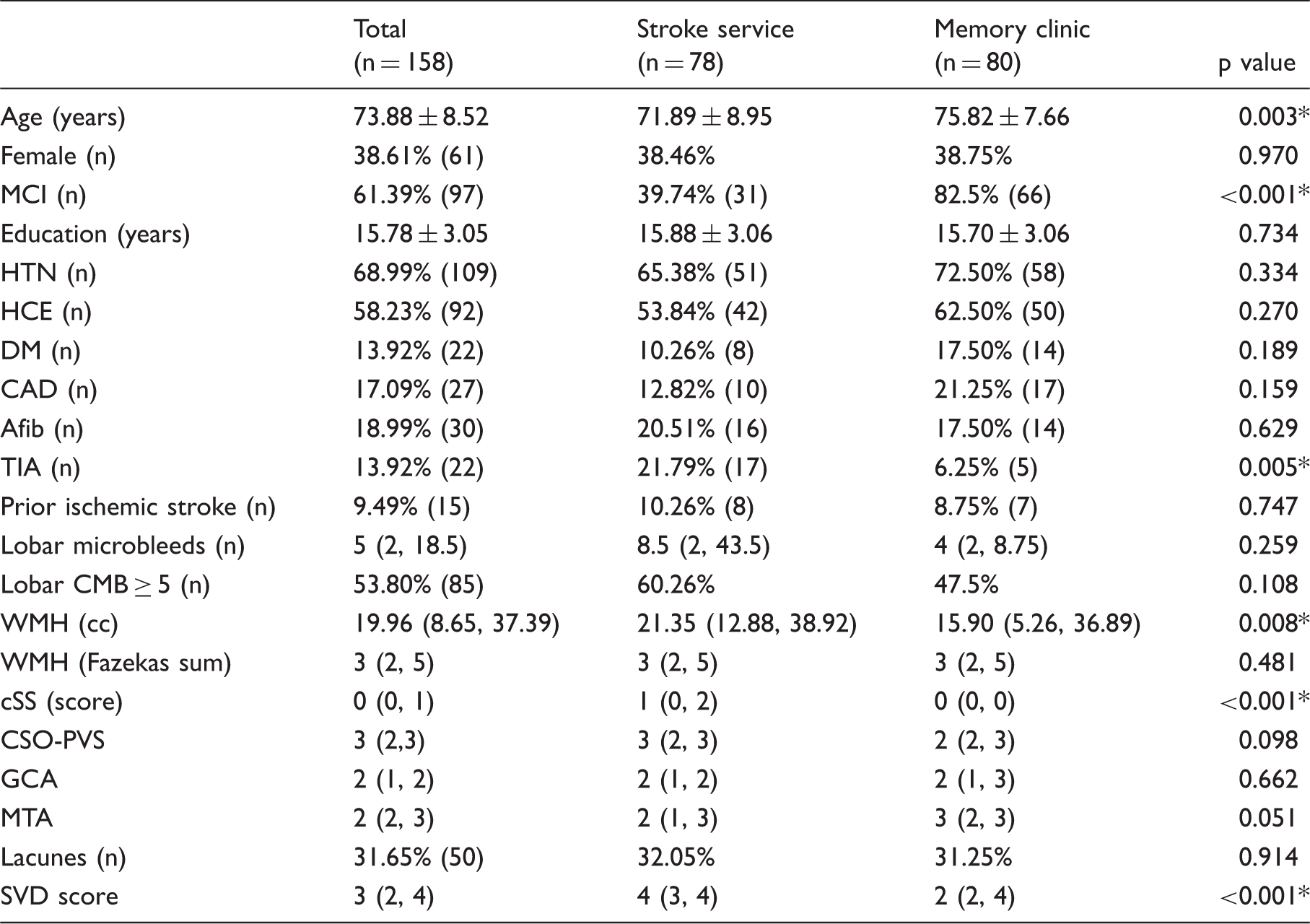
Data with normal distribution were shown as Mean ± SD. Nominal data were displayed with the prevalence and number of presence. Ordinal data were shown as median (25%, 75%). HR: hazard ratio; HTN: hypertension; HCE: hypercholesterolemia; DM: diabetes mellitus; CAD: cardiac artery disease; Afib: atrial fibrillation; TIA: transient ischemic attack; CMBs: cerebral microbleeds; WMH: white matter hyperintensity; cSS: cortical superficial siderosis; CSO-PVS: centrum semiovale enlarged perivascular space; GCA: global cortical atrophy; MTA: medial temporal atrophy; SVD: small vessel disease. * Significance.
Comparison with adjustment of age and MCI status at baseline (p = 0.674).
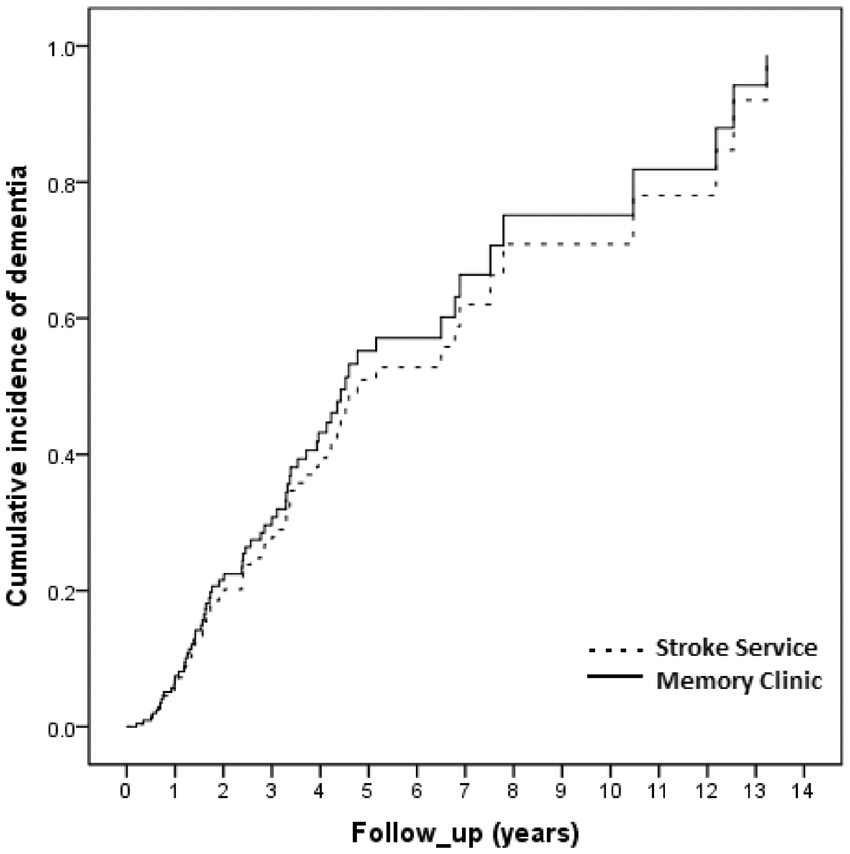
Cumulative incidence of dementia during follow-up
During the follow-up period (median 2.30 years, interquartile range 1.18–4.41 years), 16 patients with normal cognitive function (26%) and 53 patients with MCI (55%) at baseline converted to dementia. The estimated cumulative dementia incidence at 1 year was 14% (95% confidence interval (CI): 5%–23%), and 5 years was 73% (95% CI: 55%–84%) for patients with probable CAA without ICH.
Predictors of dementia conversion in CAA
Univariate association with dementia conversion in CAA patients from Stroke Service and Memory Clinic.
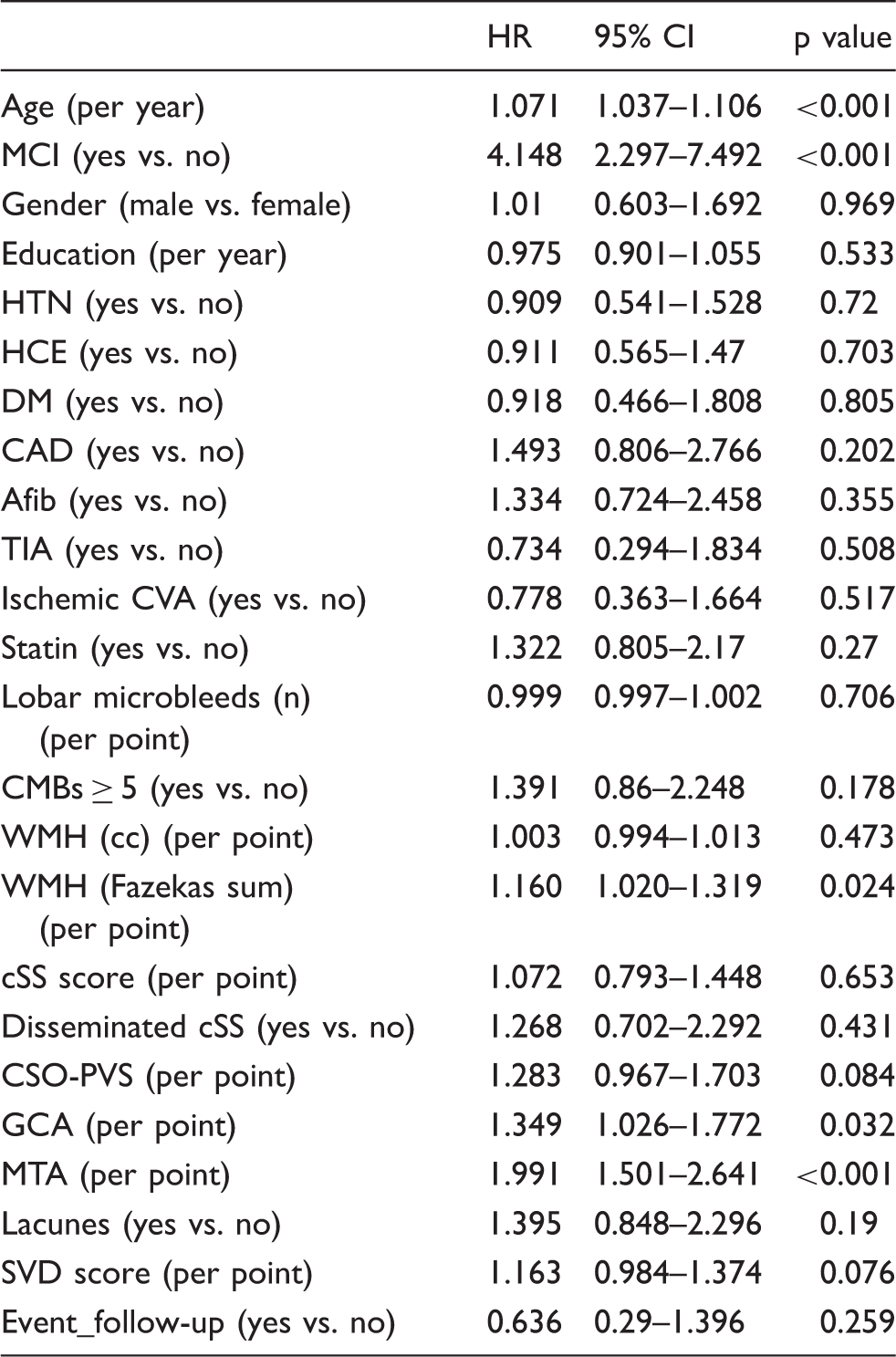
HR: hazard ratio; MCI: mild cognitive impairment; HTN: hypertension; HCE: hypercholesterolemia; DM: diabetes mellitus; CAD: cardiac artery disease; Afib: atrial fibrillation; TIA: transient ischemic attack; CVA: cerebrovascular attack; CMBs: cerebral microbleeds; WMH: white matter hyperintensity; cSS: cortical superficial siderosis; CSO-PVS: centrum semiovale enlarged perivascular space; GCA: global cortical atrophy; MTA: medial temporal atrophy; SVD: small vessel disease.
Statistically significant predictors for dementia conversion in multivariate models in the whole group.
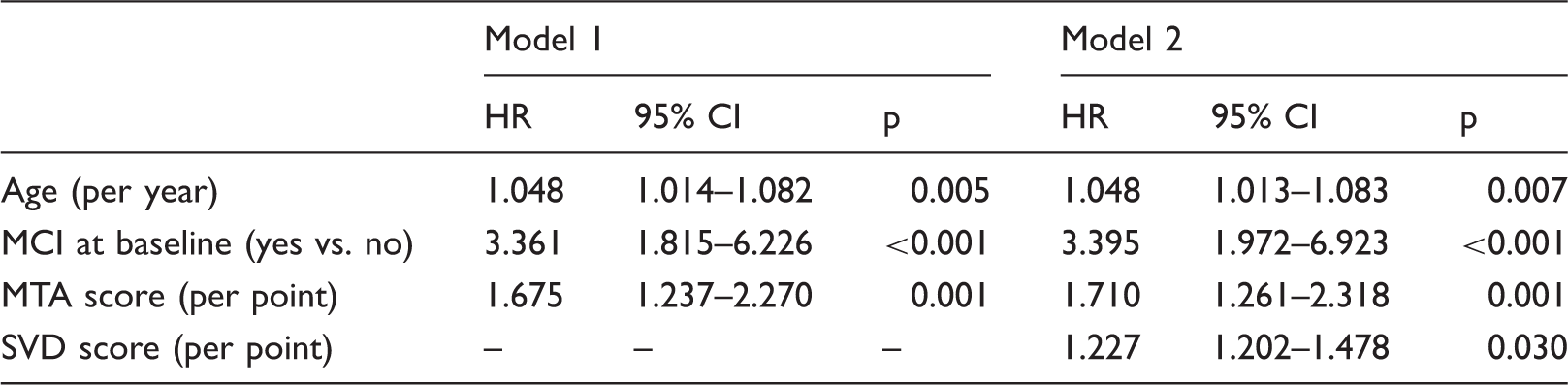
Individual neuroimaing markers were included in model 1. The SVD (small vessel disease) score, but not its individual neuroimaging component, was included in model 2. MCI: mild cognitive impairment; MTA: medial temporal atrophy.
Discussion
The main findings from our study demonstrate that probable CAA patients without ICH seen in neurology clinics are at high risk of developing dementia. Age, MCI at baseline, MTA and SVD score for CAA were independent predictors for dementia conversion in these patients. These results confirmed our hypothesis that total burden of SVD more reliably identifies CAA patients at high risk for dementia compared to any single SVD-related neuroimaging marker.
Multiple, strictly lobar MBs without ICH have a positive predictive value of 87.5% for CAA in the hospital context according to the results from a recent clinicopathological study. 4 In this study, we used the modified Boston criteria with inclusion of cSS. These criteria increased the diagnosis sensitivity from 89.5% to 94.7% and reached the diagnosis specificity of 81.2% in a histopathologically proven CAA cohort. 15 A previous retrospective study investigated the longitudinal cognitive change in normal subjects with multiple lobar microbleeds and found that subjects with probable CAA demonstrated faster cognitive decline in executive function compared with these without lobar microbleeds. 27 Similarly, lobar microbleeds are the strong determinant for decline in information processing speed in the general population after adjustment for age, sex, and education level. 28 Moreover, two recent studies have investigated dementia incidence among ICH survivors,5,6 finding that CAA related neuroimaging markers, rather than ICH volume and location, were predictors of long-term dementia incidence.5,6 These studies together support the important role of CAA-related SVD in ICH survivors. Our results suggest CAA may lead to cognitive decline even in patients without ICH. Longitudinal studies comparing probable CAA patients without ICH to elderly individuals without CAA on cognitive progression are required.
Previous studies have examined the association between various SVD neuroimaging markers and cognitive impairment in different cohorts.29,30 In CAA, it has remained unclear as to whether cognitive impairment is mainly driven by the cumulative effects of multiple lesion types or a single lesion type. 31 Our results showed that SVD score (a composite measure of CAA-related vasculopathic change 10 ) was an independent predictor for dementia conversion in patients with probable CAA without previous ICH, while no individual CAA-related neuroimaging marker, including number of microbleeds, severity of WMH, EPVS, and cSS, was a predictor for dementia conversion in our study. We also did not find significant interaction effect between SVD score and any other predictors, including MCI, MTA, and age, although there is limited power to detect such interactions. These results are in line with our previous study in patients with CAA, which demonstrated that the number of CMBs or WMH volume was not related with executive function and processing speed. 32 Therefore, it is likely that cognitive decline in CAA is related to the accumulation of multiple ischemic and hemorrhagic lesions, which exert global effects on the brain.32,33 SVD score appears to be a robust marker of future risk of dementia in patients with CAA. This composite SVD score was proposed to summarize the gross burden of SVD pathological change in CAA; however, each individual neuroimaging marker has different weight on dementia conversion. Therefore, predictive value of CAA score decreases for these cases dominated with one injury type only. Longer term and prospective studies across a range of settings are needed to further confirm and extend these results.
In our study, we also showed that MTA significantly predicted the progression of MCI to dementia in CAA patients without ICH, which is in agreement with previous studies reporting the predictive value of MTA on cognitive decline and dementia conversion in patients with cerebrovascular diseases.34–37 These studies support the important implication of MTA in cerebrovascular disease, though it has also been long recognized as a neuroimaging feature of Alzheimer’s disease.38–40 Moreover, patients with hereditary CAA-Dutch type (HCHWA-D), a monogenetic disease with minimal or no concomitant Alzheimer’s disease pathology, appear to have smaller hippocampal volumes compared with healthy controls. 14 This suggests that hippocampal atrophy may occur independently of Alzheimer’s disease pathology in patients with sporadic CAA. Additionally, our result emphasizes that MTA might be a useful clinical indicator of dementia conversion in probable CAA without ICH.
The study has limitations. The follow-up time was not systematic because of the retrospective design of this study. Dementia diagnosis might have been delayed because of the lack of consistent regular follow-up. Moreover, the different emphasis of the clinical evaluation between Stroke Service and Memory Clinic may result in bias in the definition of dementia. Additionally, since all patients were recruited retrospectively from clinical care, we lack the identical complete standardization of testing. However, detailed clinical notes and available neuropsychological tests were reviewed to confirm the diagnosis of dementia or MCI in each case.
In summary, our study demonstrated a high risk of dementia conversion among patients with probable CAA in the absence of ICH. In these probable CAA patients, age, MCI, MTA, and the SVD score for CAA independently predicted dementia conversion. Future large longitudinal prospective studies in various clinical and non-clinical populations are needed to confirm the predictive value of these neuroimaging markers in CAA-related cognitive deterioration.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: NIH grants R01AG047975, R01AG026484, P50AG005134, and K23AG02872605 (A. Viswanathan). This study is not industry sponsored.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors’ contributions
Conception and design of the study: LX, GB, AV; acquisition and analysis of data: LX, GB, AC, MJJ, DR, PF, MP, AA, MEM, KS, SMG, MEG; data management: AA, KS, MEM; drafting a significant portion of the manuscript or figures: LX, GB, AV; critical revisions: GB, AC, YR, DB, SMG, AV; Funding: AV.