
Abstract
Background:
Drug-induced prolongation of cardiac repolarization limits the treatment with many psychotropic drugs. Recently, the contribution of polygenic variation to the individual duration of the QT interval was identified.
Aims:
To explore the interaction between antipsychotic drugs and the individual polygenic influence on the QT interval.
Methods:
Retrospective analysis of clinical and genotype data of 804 psychiatric inpatients diagnosed with a psychotic disorder. The individual polygenic influence on the QT interval was calculated according to the method of Arking et al.
Results:
Linear regression modelling showed a significant association of the individual polygenic QT interval score (ßstd = 0.176, p < 0.001) and age (ßstd = 0.139, p < 0.001) with the QTc interval corrected according to Fridericia’s formula. Sex showed a nominal trend towards significance (ßstd = 0.064, p = 0.064). No association was observed for the number of QT prolonging drugs according to AZCERT taken. Subsample analysis (n = 588) showed a significant association of potassium serum concentrations with the QTc interval (ßstd = −0.104, p = 0.010). Haloperidol serum concentrations were associated with the QTc interval only in single medication analysis (n = 26, ßstd = 0.101, p = 0.004), but not in multivariate regression analysis. No association was observed for aripiprazole, clozapine, quetiapine and perazine, while olanzapine and the sum of risperidone and its metabolite showed a negative association.
Conclusions:
Individual genetic factors and age are main determinants of the QT interval. Antipsychotic drug serum concentrations within the therapeutic range contribute to QTc prolongation on an individual level.
Introduction
Drug-induced dysregulation of cardiac repolarization leading to prolongation of the QTc interval is an important risk factor for the development of torsade de pointes (TdP) tachyarrhythmia and sudden cardiac death (Roden, 2004). Psychopharmacological drugs prolong the QT interval, rendering drug-induced sudden cardiac death to be a key issue for the safety of psychopharmacological treatment (Beach et al., 2013, 2018; Wenzel-Seifert et al., 2011). On the molecular level, drug-induced prolongation of the QT interval involves mechanisms resembling those of congenital long QT syndromes, most notably inhibition of ion channel conductance such as the delayed rectifying hERG (KCNQ2) potassium channel, but also other proteins such as the nitric oxide synthase 1 adaptor protein (NOS1AP) (Kannankeril et al., 2010; Napolitano et al., 2015; Sanguinetti and Tristani-Firouzi, 2006). The affinity of psychotropic drugs towards cardiac ion channels is lower than their affinity towards their primary pharmacological targets such as the dopamine D2- or the serotonin 5-HT2A-receptor and the Kd of ion channel inhibition is above the therapeutic range (Abi-Gerges et al., 2011; Hiemke et al., 2018; Silvestre et al., 2014). Nevertheless, due to accumulation of drugs in cardiac tissues leading to locally toxic concentrations or accidental intoxication, QT prolongation is feasible even under therapeutic drug concentrations (Mikkelsen et al., 2018). However, clinical studies on this topic showed inconsistent results. An association of QTc prolongation was observed for antipsychotic polypharmacy when correcting the QT interval using Bazett’s formula, but not when using Fridericia’s formula, thereby possibly pointing at the limitations of different QTc correction formulas (Barbui et al., 2016; Elliott et al., 2018; Nosè et al., 2016). Recently, common genetic variants were identified to exhibit a strong additive effect on the duration of the individual QT interval (Arking et al., 2014; Newton-Cheh et al., 2009; Pfeufer et al., 2005). Since the effects of drugs and genetics are supposed to be additive, drug-induced QTc prolongation may act as a second hit on genetically predisposed individuals leading to sudden cardiac death (Roden, 2008; Strauss et al., 2017). Therefore, we hypothesized that individual genetic factors may explain an individual prolongation of the QT interval upon administration of antipsychotic drugs with serum concentrations within the therapeutic range.
Material and methods
Patient sample and genotyping
Genotype data generated with Illumina PsychArray BeadChip as part of the Psychiatric Genomics Consortium initiative (PGC) and approved by the Ethics Committee of the University of Würzburg [72/99; 184/11] in accordance with the Declaration of Helsinki, was available for 2062 inpatients of the Department of Psychiatry and Psychotherapy at the University Hospital (Clinic) of Würzburg diagnosed with a psychotic disorder according to the criteria of DSM-5. All subjects were unrelated and of German Caucasian descent. Written informed consent was obtained from all patients. This sample was retrospectively screened for routine clinical data in accordance with the local ethics committee. Patients were considered for further analysis when drugs had been administered in steady state (applied without change for at least four consecutive half-lives) and coincident electrocardiography was available. Patients were excluded with signs of or a previously documented atrial fibrillation, QRS duration greater than 120 ms, bundle branch block, intraventricular conduction delay, electronic pacemaker, congestive heart failure and dilated cardiomyopathy, in line with the exclusion criteria used by the GWAS analysis by Arking and coworkers (Arking et al., 2014) or lithium levels above 0.8 mmol/L were excluded. Taken together, 804 patients were analysed based on these criteria.
Single nucleotide polymorphism (SNP) selection and calculation of the score for the individual polygenic influence on the duration of the QT interval
Polygenic scores for the individual polygenic influence on the duration of the QT interval were calculated in the imputed target sample based on the summary statistics of the genome-wide association study by Arking and coworkers (Arking et al., 2014). Regarding our sample, only SNPs with an INFO imputation quality score > 0.6 and a minor allele frequency > 0.01 and < 0.99 were used for calculation. Strand ambiguous SNPs were removed, leaving 3,597,705 overlapping SNPs between the discovery and the target sample. We performed p-value-informed clumping with a cut-off r2 = 0.1 using a 500-kb window (index variant p-value threshold = 1, clumped variant p-value threshold = 1) according to the European subsample of the 1000 Genomes Project phase 1 as a reference (1000 Genomes Project Consortium et al., 2012). The number of effect alleles for each variant below a given threshold of the p-value (p < 5 × 10−8, p < 1 × 10−6, p < 1 × 10−4, p < 0.001, p < 0.01, p < 0.05, p < 0.1, p < 0.2, p < 0.5, p < 1) was multiplied by the effect estimates in milliseconds of the discovery sample. The sum of per allele scores across an individual represents the individual polygenic influence on the QT interval. If not indicated otherwise, the calculated score used included variants with a p-value below 5 × 10−8, corresponding to previous analyses (Noseworthy et al., 2011; Strauss et al., 2017). The genetic population structure inference of the sample was taken into account in all calculated models using principal component analysis (Price et al., 2006).
Electrocardiography
Electrocardiography was performed with a Cardiofax ECG-1350 (Nihon Kohden, Rosbach, Germany) by a 12-lead recording and automated analysis of the heart rate and uncorrected QT interval. The validity of the measurement was verified by a trained physician and inconsistent measurements were excluded from further analysis. The QT interval depends on the heart rate and several methods have been developed to perform a reliable frequency adaption. Recent genetic studies on the QT interval have adopted using Fridericia’s formula, which corrects the QTc interval using the cubic root of the RR interval for a wide range of heart rates contrary to Bazett’s formula using the square root of the RR interval (Arking et al., 2014; Newton-Cheh et al., 2009; Pfeufer et al., 2005). We adhered to the correction using Fridericia’s formula in our study.
Drug serum concentration measurement
Drug serum concentration measurement was performed on a routine basis during treatment in a naturalistic setting. Trough-level measurement was conducted under steady state conditions upon applying the last dose for at least four elimination half-lives. Drug concentration was determined by isocratic liquid chromatography (HPLC) with reversed phase columns and photometric detection as previously published (Scherf-Clavel et al., 2019). Analysis was carried out in the Laboratory for Therapeutic Drug Monitoring of the Department of Psychiatry, Psychosomatics and Psychotherapy, University Hospital of Würzburg. Internal and external quality control programs by Cardiff Bioanalytical Services (The Cardiff Medical Center, Cardiff, UK, prior to 2011) and Instand e.V. (Düsseldorf, Germany, from 2011 to present) were operated regularly without rejection.
Statistical analysis
Statistical analysis using descriptive statistics, multiple linear regression modelling and ANOVA as indicated in the text was performed using SPSS version 26.0 (IBM, Armonk, USA). A p-value < 0.05 was considered to be statistically significant if not indicated otherwise. Regression models calculated using polygenic scores were corrected for genetic population structure inference by including the first and second component of the principal component analysis of the genotype data of the complete patient sample. The number of QT prolonging drugs each patient received was calculated referring to drugs listed with known, potential and conditional risk according to AZCERT (www.crediblemeds.org, Oro Valley, USA) retrieved on 15 January 2021 (Schwartz and Woosley, 2016).
Results
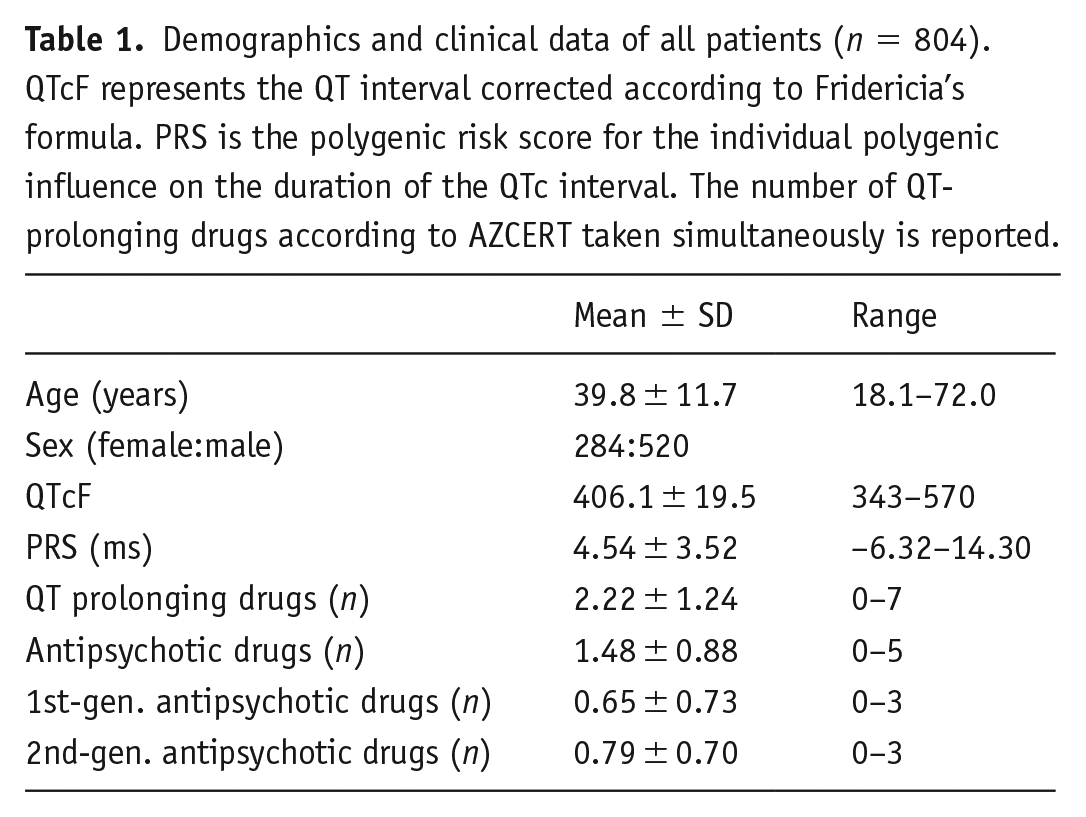
Eight hundred and four patients were included into analysis (Table 1). Following previous analyses, a score for the individual polygenic influence on the QT interval was calculated using a cut-off of p < 5 × 10−8 on a genome wide level, including 71 single nucleotide polymorphisms (Arking et al., 2014; Strauss et al., 2017). QT prolonging drugs administered in the sample and considered in the analyses were selected according to AZCERT and are presented in Table 2.
Demographics and clinical data of all patients (n = 804). QTcF represents the QT interval corrected according to Fridericia’s formula. PRS is the polygenic risk score for the individual polygenic influence on the duration of the QTc interval. The number of QT-prolonging drugs according to AZCERT taken simultaneously is reported.
Summary of drugs reported to prolong the QTc interval according to AZCERT. The number of study participants taking the corresponding drug as well as AZCERT risk category and pharmacological drug class according to the Neuroscience-based Nomenclature (nbn) are given (Nutt and Blier, 2016).
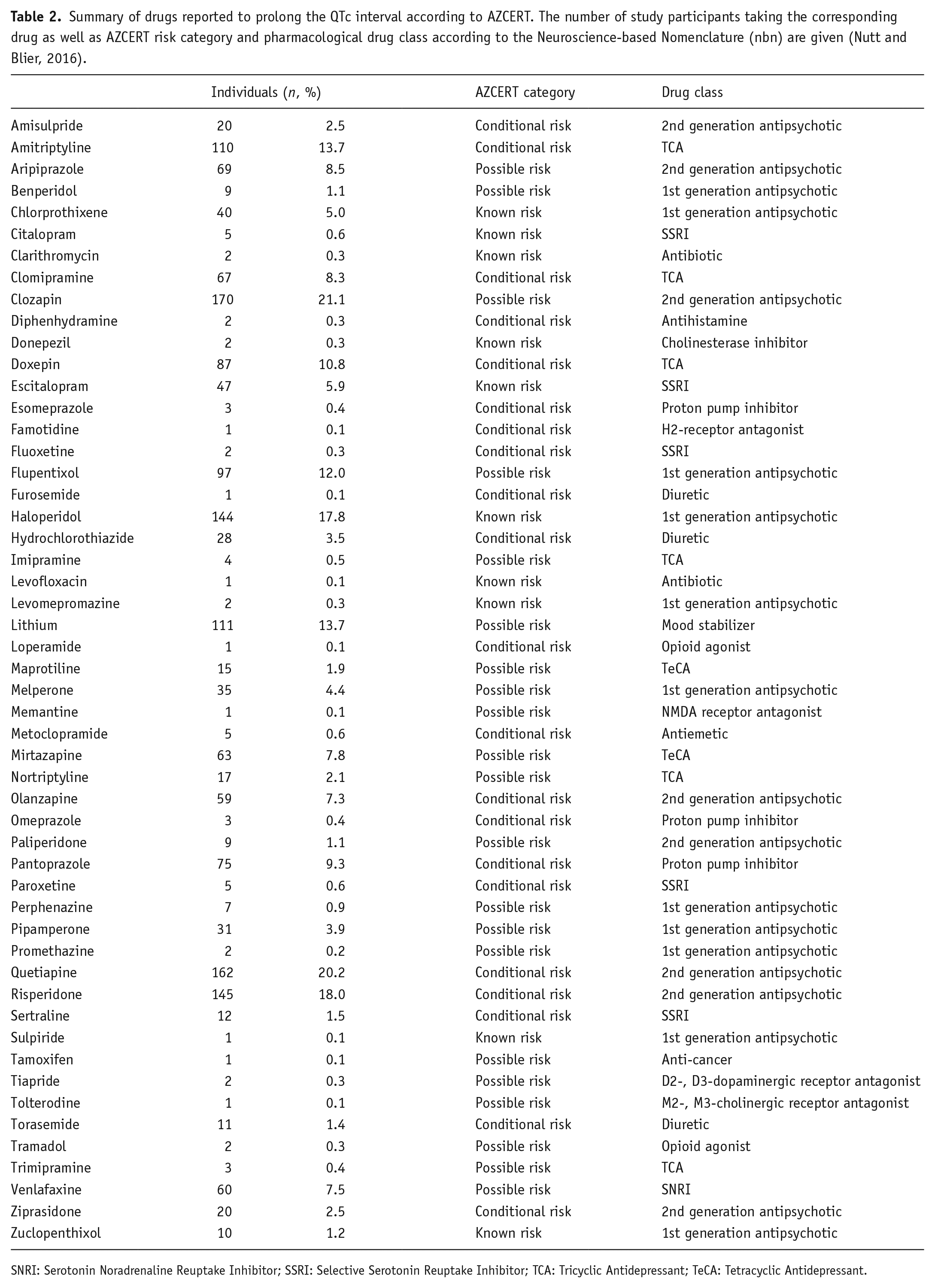
SNRI: Serotonin Noradrenaline Reuptake Inhibitor; SSRI: Selective Serotonin Reuptake Inhibitor; TCA: Tricyclic Antidepressant; TeCA: Tetracyclic Antidepressant.
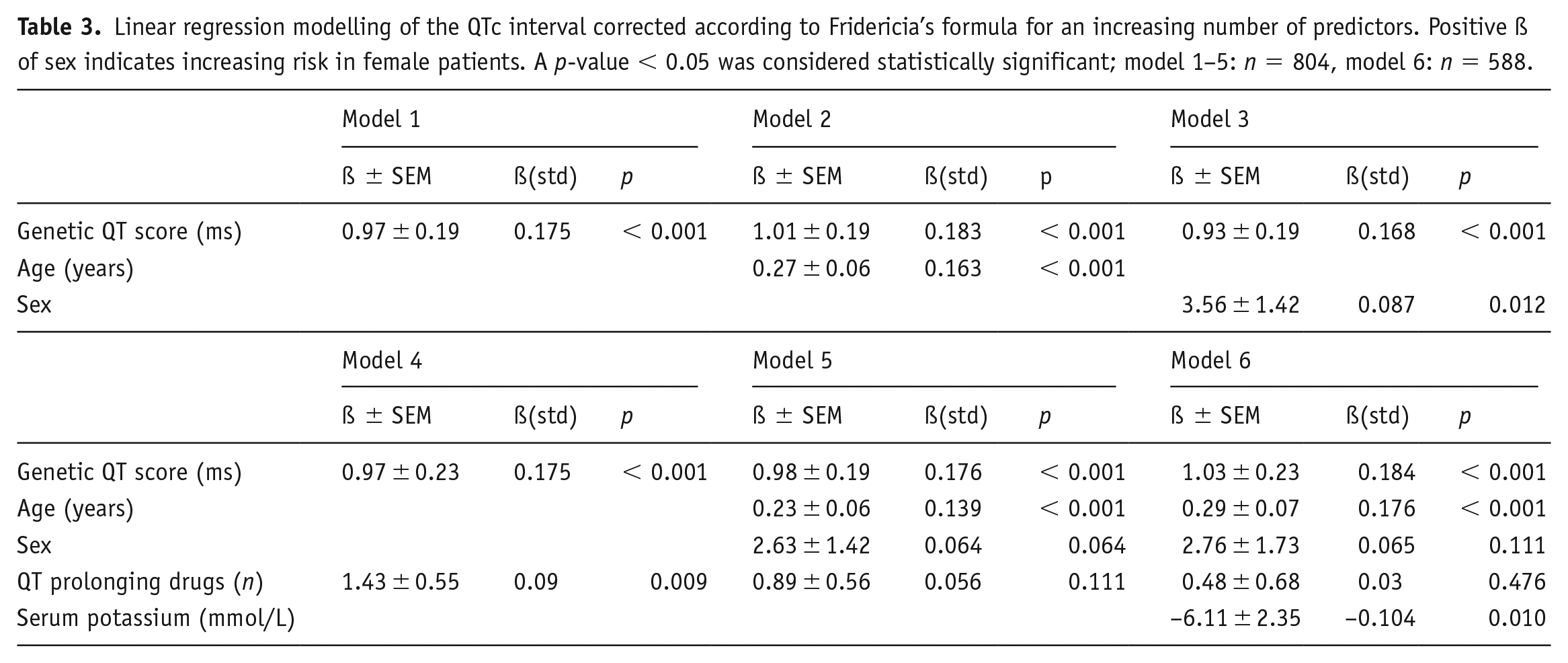
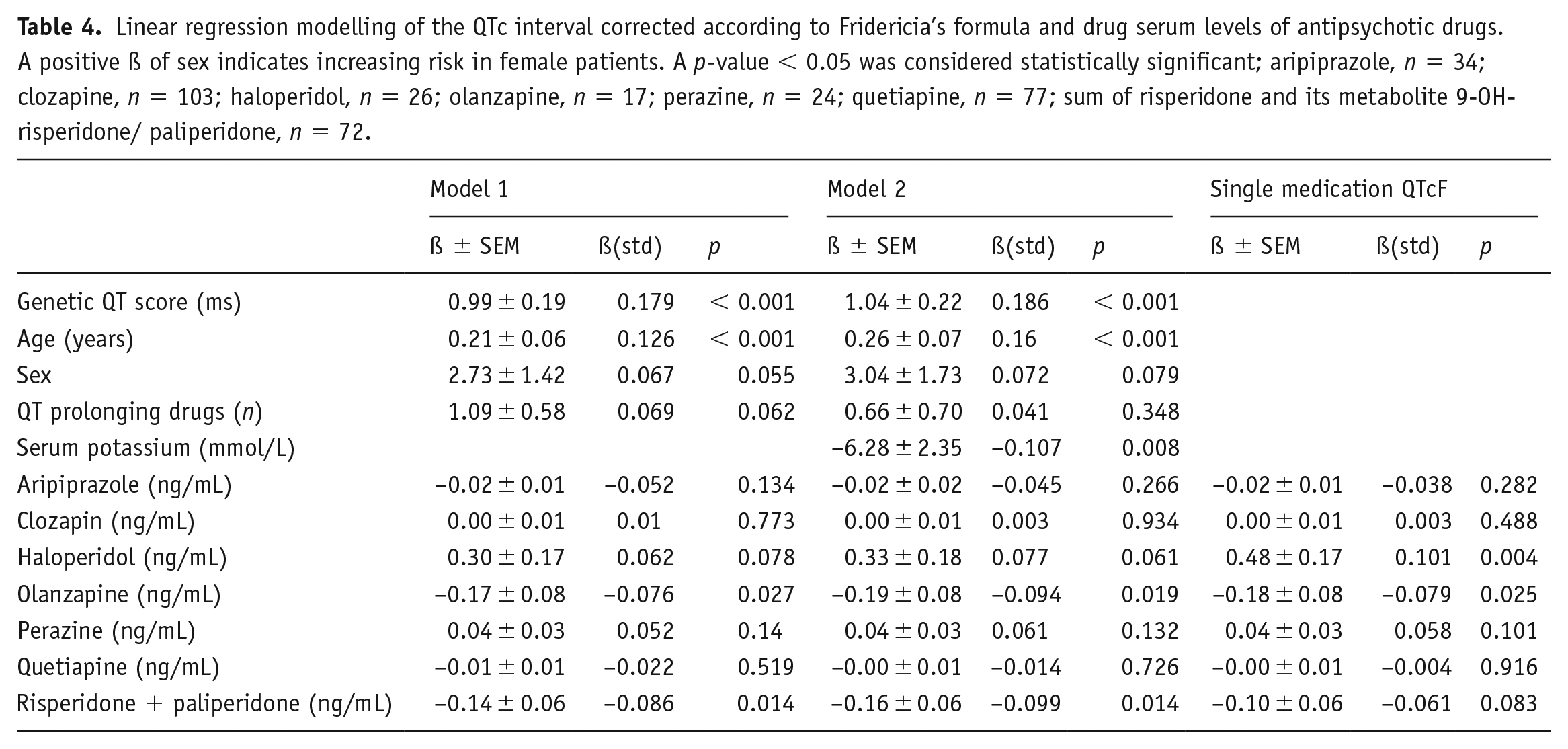
Linear regression modelling of the heart-rate corrected QTc interval according to Fridericia’s formula was conducted for an increasing number of predictors as shown in Table 3. Across all models, the individual polygenic QT interval score showed a significant association with a robust effect size with the heart-rate corrected QTc interval according to Fridericia’s formula in line with previous reports (Arking et al., 2014; Strauss et al., 2017). Taking additionally age, sex and the number of QT-prolonging drugs applied into account revealed a significant effect for each pair of predictors. However, upon inclusion of all predictors, a significant effect was observed for the individual polygenic QT interval score (ßstd = 0.176, p < 0.001) and age (ßstd = 0.139, p < 0.001) only. Sex showed a nominal trend towards significance, but the number of QT-prolonging drugs did not. In the subsample with electrolyte measurements, the QTc interval showed a significant association with decreasing potassium concentrations as expected (n = 588, ßstd = −0.104, p = 0.010). In order to investigate a link between antipsychotic drugs and subsequent prolongation of the QT interval, the relationship between drug serum concentrations of antipsychotic drugs and the QTc interval was analysed (Table 4). In single medication analysis, increasing concentrations of haloperidol (n = 26, ßstd = 0.101, p = 0.004) and decreasing concentrations of olanzapine (n = 17, ßstd = −0.079, p = 0.025) showed a nominal significant association with the QTc interval. No association was observed for aripiprazole, clozapine, perazine and quetiapine. In multivariate regression modelling of the QTc interval taking the individual polygenic QT interval score, age, sex, the number of QT-prolonging drugs applied and the serum level of antipsychotic drugs into account, a nominal significant negative association of the QTc interval with olanzapine serum concentrations (n = 17, ßstd = −0.076, p = 0.027) and the sum of the concentrations of risperidone and its metabolite 9-OH-risperidone/paliperidone (n = 72, ßstd = −0.086, p = 0.014) was observed. These nominal associations were maintained when controlling for potassium serum concentrations.
Linear regression modelling of the QTc interval corrected according to Fridericia’s formula for an increasing number of predictors. Positive ß of sex indicates increasing risk in female patients. A p-value < 0.05 was considered statistically significant; model 1–5: n = 804, model 6: n = 588.
Linear regression modelling of the QTc interval corrected according to Fridericia’s formula and drug serum levels of antipsychotic drugs. A positive ß of sex indicates increasing risk in female patients. A p-value < 0.05 was considered statistically significant; aripiprazole, n = 34; clozapine, n = 103; haloperidol, n = 26; olanzapine, n = 17; perazine, n = 24; quetiapine, n = 77; sum of risperidone and its metabolite 9-OH-risperidone/ paliperidone, n = 72.
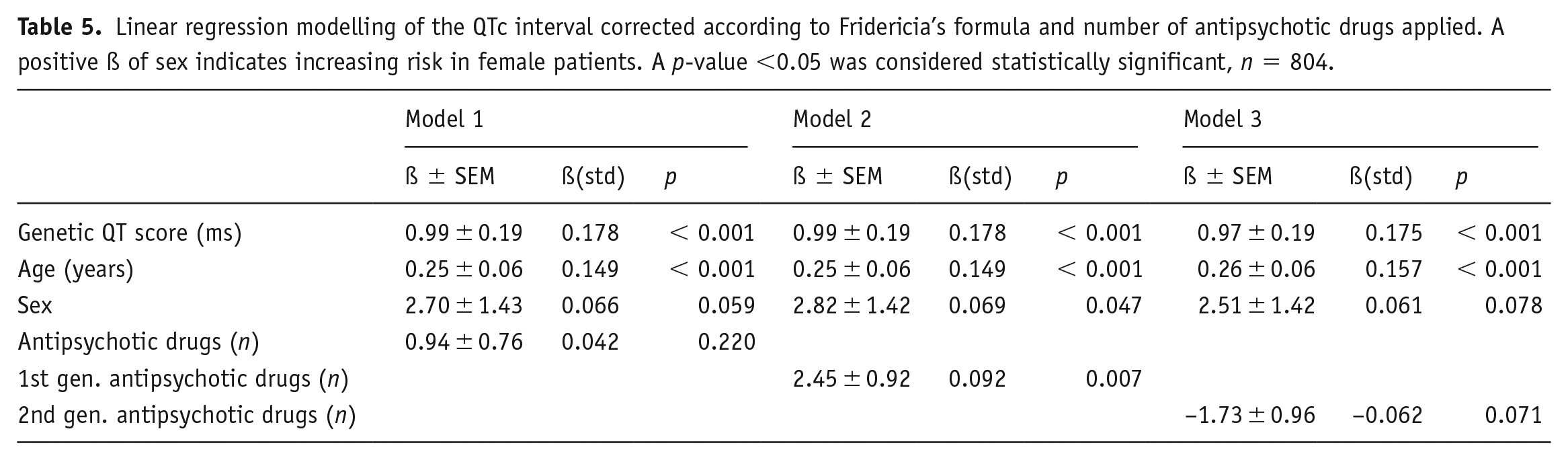
To further analyse QTc prolongation upon antipsychotic polypharmacy, a possible link between the number of antipsychotic drugs applied and the QTc interval was investigated (Table 5). Across the complete sample, a significant association was observed between the number of first-generation antipsychotic drugs applied and the QTc interval (ßstd = 0.092, p = 0.007). Controlling for potassium serum levels, the association remained at nominal significance with a comparable effect size (ßstd = 0.080, p = 0.046). Subsample analysis showed that this association was mediated by participants receiving additionally second-generation antipsychotic drugs. No association was observed for the total number or the number of second-generation antipsychotic drugs applied.
Linear regression modelling of the QTc interval corrected according to Fridericia’s formula and number of antipsychotic drugs applied. A positive ß of sex indicates increasing risk in female patients. A p-value <0.05 was considered statistically significant, n = 804.
Discussion
Antipsychotic drugs may delay cardiac repolarization and raise the risk for sudden cardiac death in the presence of risk factors such as spontaneous depolarization or electrolyte disbalance (Glassman and Bigger, 2001; Raschi et al., 2013; Salvo et al., 2016; Turker et al., 2017). Our results confirm the concept of a repolarization reserve and point at the strong additive polygenic effects on the individual duration of the QT interval (Strauss et al., 2017). However, the overall effect size of the genetic effect was small, in line with a previous report suggesting that the individual polygenic QT interval score and clinical variables explained about 10–15% of the variation of the QT interval (Rosenberg et al., 2017).
Our data emphasize the use of Fridericia’s formula to correct the QTc interval, which applies the cubic root of the RR interval, contrary to Bazett’s formula applying the square root. The problem of QTc overcorrection due to Bazett’s formula becomes uncovered in patient samples receiving tachycardia inducing mediations: correction with Bazett’s formula yields a highly significant association between the QTcB interval and serum levels of clozapine (n = 103, ßstd = 0.169, p < 0.001), contrary to results using Fridericia’s formula (n = 103, ßstd = 0.003, p = 0.488). Correction of the QTc interval using Fridericia’s formula was therefore also applied in recent genome-wide association studies of the QT interval in order to minimize the correction error, still acknowledging that any correction formula may introduce uncertainty on an individual level of the QTc interval (Arking et al., 2014; Isbister and Page, 2013). Taken together, the partial agreement of our results with previous studies may therefore result not only from correction of the genetic effect and different inclusion/exclusion criteria in our sample, but also from applying Fridericia’s formula, since our results are generally in line with studies applying Fridericia’s formula (Barbui et al., 2016; Beach et al., 2013, 2018; Elliott et al., 2018; Hasnain and Vieweg, 2014; Meid et al., 2017; Nielsen, 2012; Noordam et al., 2015; Nosè et al., 2016; Wenzel-Seifert et al., 2011).Drug-induced QT prolongation depends on the drug serum concentration. We observed a significant association of haloperidol serum concentrations with the QTc interval in single medication analysis, which retained a comparable effect size albeit only significant at nominal trend level in multivariate regression modelling. This result may be related to the small number of patients for which haloperidol serum concentration measurements were available and must be tested for replication in larger samples, yet agree with reports pointing at an increased risk for sudden cardiac death with haloperidol (Beach et al., 2018). No association between individual drug serum concentrations within the therapeutic range and prolongation of the QTc interval could be discerned for the antipsychotic drugs aripiprazole, clozapine, olanzapine, perazine, quetiapine and risperidone after correction for the genetic effect and the number of QT prolonging drugs.
Several limitations apply to the results. The sample represents a naturalistic cohort during inpatient treatment. The individual polygenic QT interval score was based on genome wide significant single nucleotide polymorphisms. Therefore, rare variants or copy number variations were not adequately reflected. No data on the individual QT interval without or prior to initiating drug treatment were available. Due to the naturalistic sample, type and number of comedication were not restricted or limited. Thus, pharmacodynamic drug interactions may have biased the results, for example, by additive effects on the QT interval. We aimed to correct for these effects by accounting for the number of drugs taken and known to induce QT prolongation according to the AZCERT classification (Schwartz and Woosley, 2016), yet no significant effect was observed. Since QT prolongation due to polypharmacy may be modulated by the exact combination of drugs, future studies in larger samples may test to use the AZCERT classification of the combination partners for a better risk stratification (Meid et al., 2017). Moreover, data on cardiac events are unavailable and we used only the QT interval to assess the risk of sudden cardiac death due to widespread clinical adoption. Future studies may therefore consider a detailed cardiac risk estimation by including T-peak to T-end interval and QT dispersion (Acciavatti et al., 2017).
From a clinical point of view, our data suggest that clozapine and quetiapine exhibit the lowest risk for QTc prolongation and hypokalaemia due to the diuretic medication being a strong modifiable factor for QT prolongation due to comedication. Serum concentrations of antipsychotic drugs within the therapeutic range contribute to QTc prolongation rather modestly compared to genetic determinants of the individual patient and age, which possibly also reflects comorbidities. Due to the incomplete correlation between drug dose and drug serum levels, safe daily dose estimates can be hardly given, and we suggest performing therapeutic drug monitoring of antipsychotic drugs on a regular basis (Hiemke et al., 2018). A cardiological assessment might be helpful when repeatedly monitoring an individual QTc prolongation using Fridericia’s formula of more than 20 ms (one standard deviation of our sample) upon initiating antipsychotic treatment. Taken together, our results underline that careful clinical analysis of all QT prolonging factors is the most important risk-reducing step one can make to minimize the cardiac arrhythmias due to antipsychotic treatment (Beach et al., 2018).
Footnotes
Acknowledgements
We are grateful to all individuals who participated in this study and the staff of the Therapeutic Drug Monitoring Laboratory of the Department of Psychiatry, Psychosomatics and Psychotherapy, University Hospital of Würzburg: R. Burger, M. Burger, K. Balcioglu and M. Weyer.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J. Deckert is the co-recipient of a grant of the Bavarian State Government to BioVariance and an investigator in a European grant to P1Vital. L. Hommers, M. Scherf-Clavel, R. Stempel, J. Roth, M. Falter, M. Mattheisen, S. Unterecker and M. Gawlik have no conflicting interests.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this work was supported by the Federal Ministry of Education and Research (BMBF) within the framework of the Comprehensive Heart Failure Center, Wuerzburg. It was also supported by the Interdisciplinary Center for Clinical Research, University of Wuerzburg (N-258 to LH) and Deutsche Forschungsgemeinschaft (project 221226493 to MG).
Role of the sponsors
The supporters had no role in the design, analysis, interpretation, or publication of this study.
Ethical approval
All procedures performed in the analysis involving human participants were in accordance with the ethical standards of the local ethics committee (vote no. 72/99 and 184/11) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Patients were recruited and enrolled in the study after written informed consent.