
Abstract
Background:
High-quality recommendations require rigorous methods based on strong evidence to improve clinical practice. In palliative and end-of-life care, expert consensus is sometimes achieved through nominal group techniques. However, its practical challenges are often underestimated, potentially compromising the rigour and the quality of the recommendations.
Methodological reflections:
The methodological reflections on developing recommendations using the nominal group technique are discussed in this paper. These reflections are drawn from its theoretical foundations and applications in palliative care research, including a Taiwanese study on preparing families for a relative’s death. We highlight key issues such as the omission of pilot meetings and the underestimation of practical challenges in conducting group meetings, including time constraints and real-world uncertainties, especially during the stages of listing, clarifying, voting and ranking recommendations. Cultural factors are often overlooked, as seen in the example study, where the moderator avoided interruptions to show respect and politeness during the meeting. Additionally, valuable data gathered during meetings is often underutilised. These factors collectively can undermine the quality of recommendations. Based on these insights, we offer suggestions for improvement.
Key suggestions:
Pilot meetings should be conducted and reported to demonstrate how they inform the main meeting, ensuring research rigour and recommendation quality. Sufficient time should be allocated for listing and clarifying recommendations and in societies with specific etiquettes (e.g. minimising interruptions to show politeness). Further qualitative analysis of meeting transcripts is suggested to better understand the context and rationale behind the recommendations and enhance their applicability and clarity.
Keywords
Developing practice recommendations based on evidence using rigorous and transparent methods is essential for enhancing healthcare quality through formal consensus methods such as the nominal group technique.
The nominal group technique is a structured method for identifying priorities, reaching consensus and developing recommendations, but despite its wide use in healthcare research, it remains underutilised in palliative care.
We reinforce the value of conducting pilot meetings and highlight the practical challenges of conducting nominal group technique meetings, as difficulties arise from multiple tasks, time constraints, practical complexities and real-world uncertainties, particularly during the recommendation listing, clarification, voting and ranking phases.
Cultural factors in applying the nominal group technique are overlooked, as shown in the example study, including the need for more time to summarise and record participants’ verbal recommendations in written Traditional Chinese (which uses complex characters with many strokes) and the necessity of adhering to etiquette by minimising interruptions to demonstrate politeness.
Existing palliative care research using nominal group techniques often underutilises valuable qualitative data from group meetings, overlooking opportunities to reflect on their conduct or address practical challenges that have been encountered during the process through post-meeting qualitative analysis.
Pilot meetings should be conducted and reported to show how they inform the main meeting, ensuring research rigour to improve recommendation quality.
Sufficient time should be allocated for conducting nominal group technique meetings, particularly for listing and clarifying recommendations, with culturally appropriate consideration given to societies where interruptions are avoided to show politeness, necessitating prior arrangements made with participants.
Further qualitative analysis of group meeting transcripts through a more interpretive qualitative approach (e.g. framework analysis), particularly of discussion during recommendation listing and clarification, is recommended to reflect on meeting conduct, gain deeper insights into the context and rationale behind participant-generated recommendations, and enhance their applicability and practicability.
Background
Implementing research findings into clinical practice is essential for enhancing patient care and maintaining healthcare quality.1–3 The quality of recommendations depends on the strength of the underlying evidence. 1 In palliative and end-of-life care research, expert consensus together with engaging practitioners in the stage of developing evidence-based recommendations is vital.2–4 Formal consensus methods, such as the Delphi method and nominal group technique, are commonly used to establish consensus and involve practitioners in the process.5–9
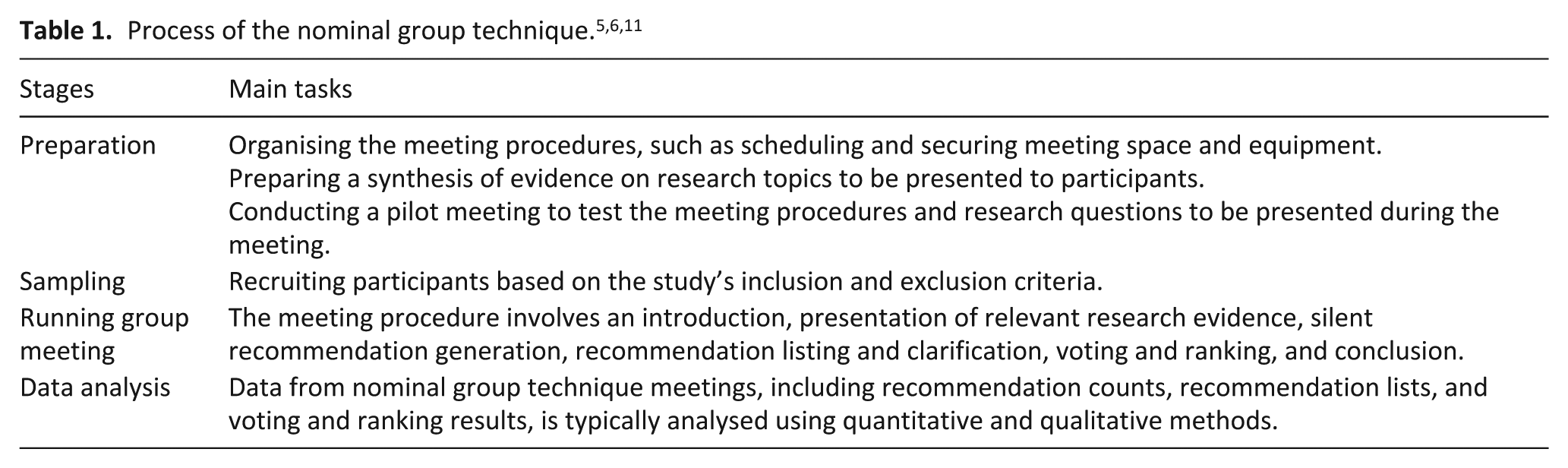
The nominal group technique, developed in the 1970s, is a structured method for generating recommendations that prioritise group consensus over diverse perspectives.8,10–12 Unlike the multi-round Delphi method, it is more time-efficient and less demanding for participants, requiring only a single session. 5 This method ensures equal participation opportunities to contribute,5,11 preventing domination by certain individuals, a common issue in focus groups.13,14 The technique comprises four stages: preparation, sampling, group meeting and data analysis5,11,12,15 (Table 1). The preparation stage involves practical tasks such as planning the meeting, setting its duration, and arranging space and equipment, alongside research-related tasks like gathering relevant evidence5,7,9 and conducting pilot meetings. 5 In the sampling stage, participants with diverse expertise are selected, usually through purposive sampling,5,9,12 to enhance data quality and minimise social hierarchy effects. 5 Nominal group meetings typically involve five to ten participants, depending on the research scope and participants’ availability, ensuring adequate data collection while providing equal opportunities for all participants to contribute.5,9,15
Group meetings are the core of the nominal group technique, following a structured process of introduction, recommendation generation, listing, voting and ranking.5,11 The moderator begins by outlining objectives and expected outcomes, followed by brief participant introductions.11,15 Relevant research evidence is presented before introducing the meeting’s research questions.5,16,17 Participants then generate recommendations individually and silently, without discussion.5,11,12 Next, they take turns sharing one recommendation at a time, trying to avoid repetition while promoting equal participation and diverse input.12,15,18 A discussion phase follows for clarification before voting and ranking to reach consensus.11,15 The meeting concludes with a summary of key outcomes, expressions of gratitude and final questions. 5 Meetings typically last 90–120 min,5,15 depending on group size, the number of research questions and available time. 18 Two moderators usually lead the session, with one facilitating and the other observing and taking notes. Collected data, including recommendation lists, counts and voting results, are analysed using quantitative and qualitative methods.5,15
The nominal group technique serves multiple research purposes, including developing recommendations, solving problems, establishing priorities and building consensus.5,8,19 It is suited to explore sensitive or under-researched topics, 5 which are common in palliative care. Although widely applied in healthcare and nursing, 6 its application in palliative care research remains limited. 20 This paper aims to provide methodological reflections on the technique, drawing from its theoretical foundations and applications in selected exemplar palliative care studies. While focused on this field, the insights may be relevant more broadly.
Relevant literature was identified through Scopus and Google Scholar using the keywords ‘nominal group technique’ and ‘palliative care’. Sixteen papers published between 2006 and 2024 were selected based on relevance to palliative care.16,21–35 A summary of how the method has been used is available in the supplementary file (S1). Collectively, these studies demonstrate the technique’s adaptability. It has been used to explore research conduct.24,26 research priorities, 16 clinical practice,28,31,32 outcome measurement29,33,35 and professional education. 23 Many studies included participants in varied roles,16,21,24–33,35 such as patients, family members and healthcare professionals,24,35 demonstrating the technique’s capacity to capture diverse perspectives. Some studies combined the technique with other research methods.21,24,28 Seven studies presented relevant evidence during meetings,16,24–29 which can enhance recommendation quality, participant engagement and group cohesion.5,7 However, nine studies omitted this step,21–23,30–35 possibly to emphasise participants’ lived experiences, underscoring the method’s flexibility.
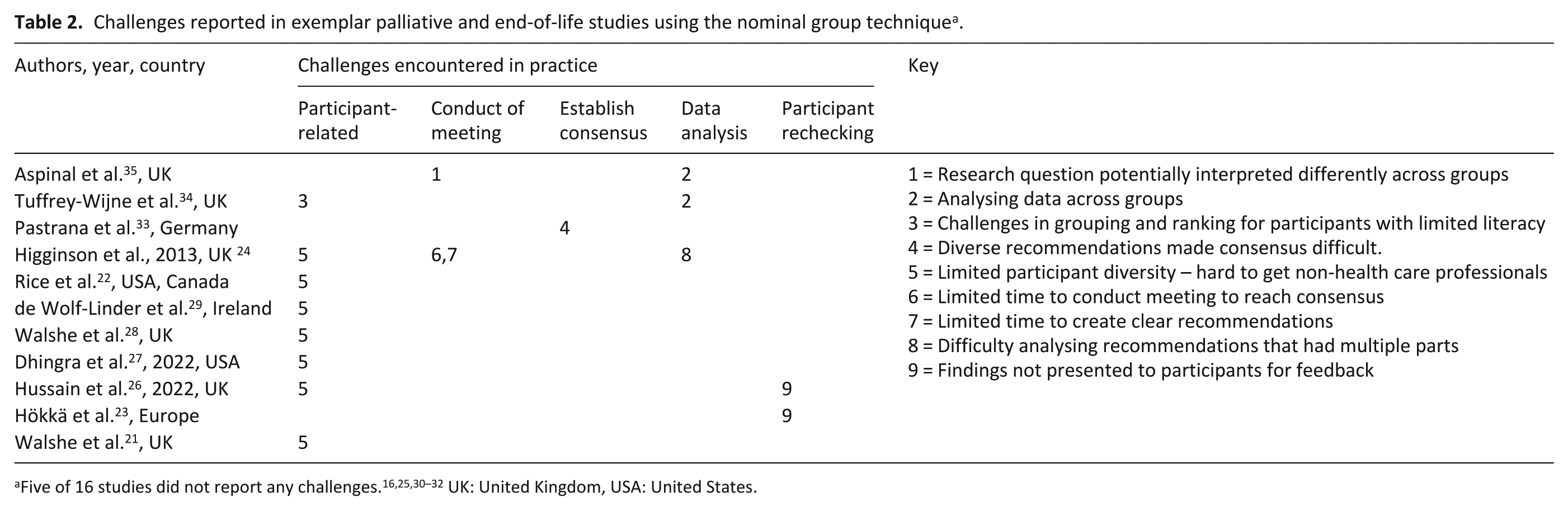
Challenges in applying the nominal group technique were reported in 11 studies (see Table 2 for details), including participant recruitment,21,22,24,26–29,35 the conduct of the meeting,24,34,35 reaching consensus, 33 data analysis,24,34,35 and verification of recommendations with participants after the meeting.23,26 In contrast, five studies did not state any challenges.16,25,30–32 Overlooking these issues can compromise methodological rigour and the quality of recommendations produced. These challenges are further reflected upon in relation to our study, as discussed below.
Challenges reported in exemplar palliative and end-of-life studies using the nominal group technique a .
A practical example of the nominal group technique
The example study is part of a larger project aimed at improving the preparation for a relative’s death in Taiwan36–38 underpinned by critical realism, acknowledging that truth is contextualised 39 This study aimed at developing recommendations for healthcare professionals on preparing families for a relative’s death using the nominal group technique. On 8th July 2023, a nominal group meeting was held in Taiwan with ten specialist palliative care professionals, including two physicians, six nurses, one psychologist, and one chaplain. The participants generated and voted upon 42 recommendations, resulting in a prioritised list.
Methodological reflections on the nominal group technique
The real-world challenges of applying the nominal group technique are explored, addressing both its theoretical foundations and practical applications in palliative care research.
The absence of pilot meetings or poor reporting
Pilot meetings are recommended to refine meeting procedures, improve the clarity of research questions to be presented and enhance moderator confidence.5,12,15,40 By addressing potential challenges in advance, they help ensure smoother main sessions and improve recommendation quality.5,9,40 For methodological rigour and transparency, changes made following pilot findings and their impact on the formal session should be reported. However, pilot meetings were often omitted or poorly documented in the exemplar palliative care studies.16,21,24–35 Only two studies reported conducting pilot meetings.22,23 One found no relevant outcomes, 23 while the other extended discussion time but made no protocol changes. 22 However, the pilot involved research team members rather than intended participants (family caregivers) and lacked details on the original or revised discussion duration, limiting transparency.
In contrast, our study reinforced the value of pilot meetings by providing feedback that refined the main session. The pilot, held on 8 June 2023 with 10 specialist palliative care nurses who did not participate in the main meeting, tested all procedures and led to key modifications. While recommendations are usually grouped into themes during the clarification stage 18 or in post-meeting analysis,15,35 pilot feedback suggested introducing predefined themes, such as clinical care and education, during the listing stage. This helped identify recurring recommendations and streamline voting and ranking. Other refinements included sharing meeting objectives, procedures and research questions with participants in advance to allow for preparation and questions beforehand. Typing recommendations into a laptop and using voting software to improve efficiency and reduce manual errors was also suggested. Recognising the need for sufficient time, the meeting duration was extended from 140–150 min to allow more time for presenting evidence and listing and clarifying recommendations while slightly reducing the time for voting and ranking.
Lack of clarity in defining group consensus
Establishing group consensus is a central goal of the nominal group technique. For methodological rigour, researchers should clearly define what constitutes consensus, including how it will be identified and measured. 5 Theoretically, consensus refers to the degree of individual or overall group agreement and whether the collective views demonstrate sufficient alignment. 5 In practice, consensus is typically reached through independent voting and ranking, followed by aggregation of results without further participant comments. 11 Additional voting rounds may be conducted if needed. 5 Importantly, verifying that participants accept the final outcomes confirms whether consensus has been achieved. This poses a methodological challenge in studies involving multiple groups, where researchers must decide whether to assess consensus within each group or across all groups collectively.
In the exemplar palliative care studies, definitions and processes for reaching consensus varied in rigour and transparency. Some followed clear procedures,24,25 while others lacked sufficient detail.16,22,23,27,29–32,34,35 Most commonly, consensus was achieved by selecting the top five27,29–32,34,35 or top ten16,21,23 recommendations after a single one voting round. However, few studies reported whether participant feedback was sought or whether additional rounds were conducted to confirm agreement. Only one study explicitly stated that consensus was reached when participants had no further comments and results were finalised 25 while another defined consensus as full participant agreement during the clarification phase rather than the ranking process. 22 Moreover, multi-group studies rarely described how consensus was established across groups.22,23,27,31,34,35 A few used follow-up online surveys to assess cross-group consensus.17,24,32,41,42 Some used statistical measures such as median score and interquartile ranges,17,24,41,42 while another asked participants from multiple groups to prioritise the top five recommendations based on perceived importance. 32 However, these approaches seldom addressed whether any disagreement remained, raising concerns about the robustness of consensus verification. Follow-up surveys may offer a practical solution for assessing consensus across groups.
In our example study, 42 recommendations were voted upon, and the 10 receiving the highest number of votes were prioritised. As the results were accepted by all participants, no additional voting rounds were required.
Overall, the lack of consistent definition and transparent reporting criteria for establishing consensus can compromise the reliability of nominal group technique studies. Clear operationalised definitions and explicit procedures for establishing consensus are essential for ensuring methodological rigour.
Underestimate the practical challenges of conducting group meetings
Practical challenges in conducting nominal group meetings are often underestimated, yet they can undermine the rigour of the method and the quality of recommendations developed. 9 One possible reason for this may be the technique’s inherent flexibility. Although theoretically structured, the nominal group technique varies in formats, research objectives and participant needs.6,18,35,43 Meetings may be conducted in person or online 6 and may involve a single session or multiple sessions with different groups,8,12,17,31,35 held either simultaneously12,17 or asynchronously.8,31,35 Standard procedures involve listing recommendations without discussion, grouping similar ones and prioritising them through ranking and votes. 5 However, the procedure of generating recommendations can be different. While recommendations are often written during meetings, 35 some studies asked participants to prepare them in advance.8,19 Some adaptations allow discussion during the listing phase or grouping recommendations into broader themes during meetings.18,40,43 This adaptability is evident in the exemplar palliative care studies. Some conducted one in-person meeting25,30,33; others organised multiple in-person sessions for different groups, either simultaneously16,24,26,29 or asynchronously.22,27,28,31,32,34,35 Some opted for multiple online sessions for separate groups at different times.21,23 These format and timing choices reflect efforts to accommodate participants while maintaining the integrity of the consensus process. However, most studies did not report challenges encountered during meetings.16,21–23,25–33 Only a few noted specific difficulties,24,35 such as applying the same research question to different types of participants. 35
The structured design and practical flexibility of the nominal group technique are strengths, but they do not eliminate implementation challenges.18,43 In our example study, despite a pilot meeting conducted, several issues arose during recommendation listing, clarification, voting and ranking. These challenges stemmed from managing multiple tasks under time pressure, linguistic complexity and real-world uncertainties. While recommendations should be recorded as accurately as possible to preserve participants’ original wording,12,15 it was difficult in practice. None of the exemplar palliative care studies reported challenges with capturing participants’ voices,16,21–35 but in our case, recording participants’ verbal recommendations in written Traditional Chinese, a language with complex characters and many strokes, within time constraints was challenging. This increased time pressure also raised the risk of human errors in subsequent voting and ranking stages. In our study, eight recommendations tied in voting, but three of the tied ones were missed in the final listing of the top ten recommendations.
Technologies, such as laptops, projectors and voting software, can streamline the meeting process and reduce manual errors.21–23,31 However, technical difficulties may still arise. In our case, typing handwritten recommendations in Traditional Chinese for voting software was more time-consuming than in English, increasing the likelihood of errors. Additionally, Mentimeter was planned to be used for ranking, but it failed during the meeting despite prior testing, so we had to switch to paper-based ranking.
Our study illustrates that practical challenges of conducting nominal group meetings can occur even after pilot meetings. Greater attention to these real-world barriers is essential to ensure robust application of the nominal group technique.
Insufficient attention to cultural contexts
Cultural context is often overlooked in applying the nominal group technique. 43 This limitation is apparent in the exemplar palliative care studies, likely due to studies predominately being conducted in Western societies, including the United Kingdom,16,17,21,24–26,28,32,34,35,41,42 Europe,23,29–31,33 the United States 27 and Canada. 22 Our study underscores the importance of considering cultural factors when applying the nominal group technique, 43 particularly in non-Western contexts, to ensure both methodological rigour and cultural sensitivity.
In our example study conducted in Taiwan, cultural and linguistic factors affected the recommendation listing stage and prolonged the session. Summarising participants’ verbal recommendations during the listing stage was challenging. Participants struggled to make succinct suggestions, often presenting multiple recommendations at once, and had difficulty articulating their thoughts on death preparation. These patterns may reflect communication styles within Taiwanese culture. 44 Consequently, the moderator needed to interpret participants’ statements, identify key points being made and confirm these with them. Despite awareness of time constraints, the moderator did not necessarily interrupt participants to manage the session, as avoiding interruptions to show respect and politeness is a cultural norm in Taiwan. 44 Additionally, writing recommendations in Traditional Chinese slowed down the real-time documentation process. Therefore, much more time was spent on listing, clarifying and discussing recommendations than expected; our entire session still exceeded the adjusted duration (150 min) based on a pilot by approximately 80 min.
Underutilisation of the rich qualitative data from group meetings
A reductionist approach, consolidating similar recommendations during meetings to minimise post-meeting analysis, is often used in the data analysis of the nominal group technique, 10 leading to methodological challenges. 12 Consequently, greater emphasis is placed on quantitative data for voting and ranking outcomes and cross-group comparisons. 43 In contrast, qualitative analysis tends to be inconsistently applied and usually limited to the synthesis of participant-generated recommendations. 17 In-depth analysis of meeting transcripts is rare and often poorly reported, 45 leading to underutilisation of rich qualitative data from group meetings and loss of contextual insights into how recommendations are developed.15,43
This pattern is reflected in the exemplar palliative care studies. Voting and ranking results were typically analysed using descriptive statistics and compared across groups when needed.22,27,31,34,35 Qualitative data, including participant-generated recommendations,17,22,23,28,31,35 scribe notes26,29 and meeting transcripts,25,27,32,33 were analysed less consistently. Most studies focused on synthesising recommendations or scribe notes, often neglecting deeper insights available in transcripts.22,23,26,28,29,31,35 Thematic analysis was commonly used23,25–29,33,35, while some studies applied content analysis,22,32 or did not specify the method.17,24,31. A few studies omitted post-meeting qualitative analysis,16,30,34 possibly due to using reductionist approaches during meetings, which reduced the need for further analysis. 10
While some exemplar palliative care studies analysed transcripts,25,27,32,33 few reflected on how meetings were conducted or practical challenges encountered. In our example study, challenges arose despite prior piloting. Although the moderator aimed to remain neutral,40,45 interactions during the recommendation listing and clarification stages proved complex. Time constraints and data complexity contributed to errors in voting and ranking, with recommendations made on the day missing important information from deeper discussions. This highlighted the need to critically examine the conduct of group meetings and the researcher’s role. An interpretive qualitative approach can offer greater insight into the context and reasoning behind participants’ recommendations and enhance the relevance and applicability of findings.
In our study, framework analysis was chosen to allow structured interpretation within a predefined theme framework.46,47 The process followed five stages: familiarisation, framework development, indexing, charting, and mapping and interpretation. 47 The meeting recording was transcribed and reviewed to familiarise the researcher with the data. A framework was developed that included the recommendations listed and agreed upon by participants, along with the top 10 ranked recommendations. It also incorporated summaries of discussions about each recommendation (e.g. how they were developed through group interactions), reflections on the meeting process (e.g. missed or misunderstood recommendations), challenges faced by staff in death preparation, and refined recommendations for preparing patients and families for an expected death. This framework guided the annotation, categorisation and synthesis of data under relevant headings, enabling refinement, elimination of duplicates and consolidation of related recommendations. During this process, the three tied recommendations missed in the final ranking were reintroduced and incorporated into the refined top-ranked recommendations, which included predicting life expectancy, delivering appropriate end-of-life care and supporting families’ psychological needs. Table 3 illustrates how this recommendation evolved into a more comprehensive form through analysis.
Refining the top one recommendation from the nominal group meeting through framework analysis in the example study.
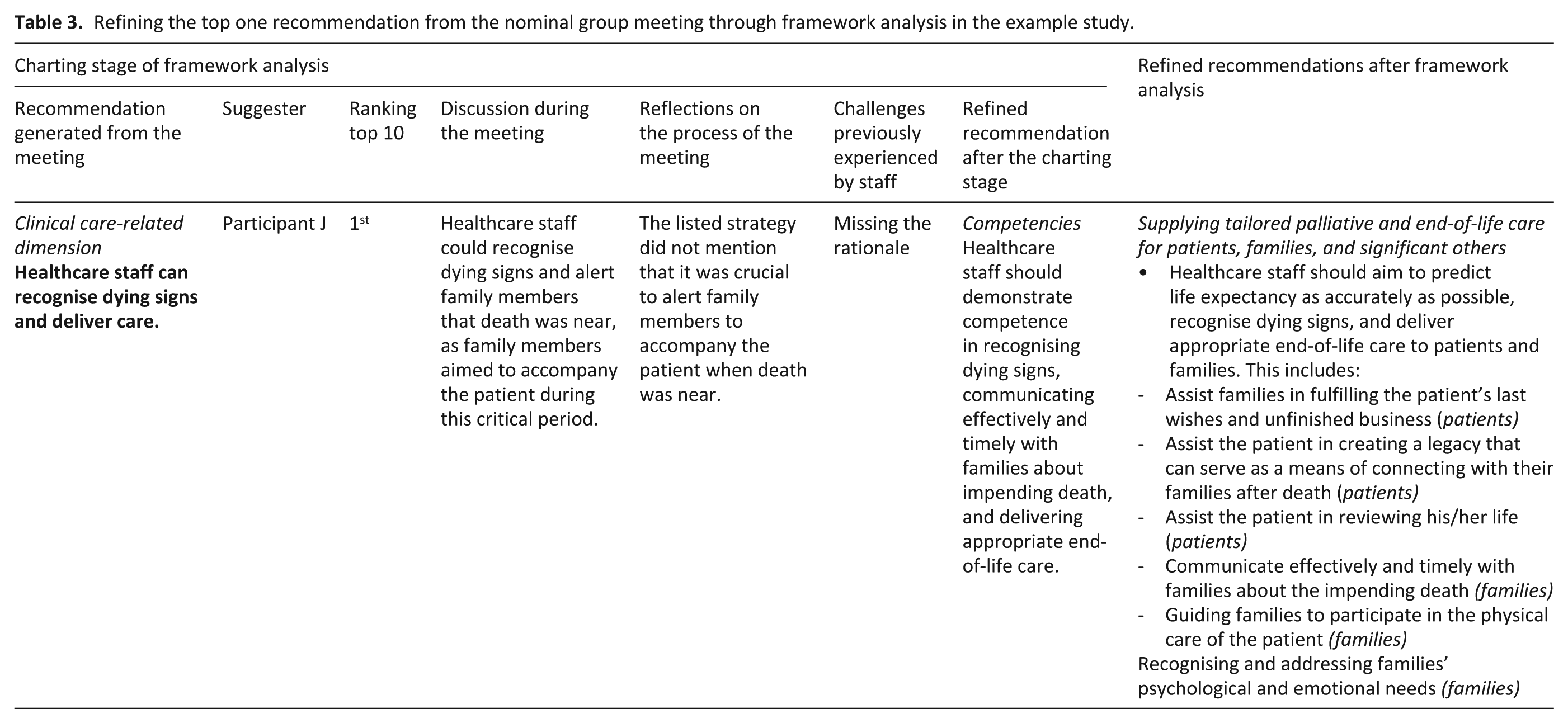
The final recommendations were developed from participants’ input and discussions, but their wording was modified for clarity and practical relevance. The final recommendations were not returned to participants for review or re-ranking due to no consent obtained for a follow-up.
Our study demonstrates the value of in-depth transcript analysis using an interpretive approach. Although the nominal group technique emphasises preserving participants’ original wording, this may limit the practical utility of recommendations. A more interpretive lens enhances clarity, feasibility and contextual relevance, while also providing deeper insights into the reasoning behind recommendations. It allows researchers to evaluate all recommendations within a broader context rather than focusing solely on the top ten generated during the meeting.
Suggestions for supporting good practice in using the nominal group technique
The nominal group technique aims to build consensus by engaging practitioners in generating and prioritising recommendations.5,9 Based on our methodological reflections, we suggest several strategies for future research to strengthen its application and enhance recommendation quality (Table 4). These insights developed in palliative care research are relevant to other fields.
Key suggestions for conducting nominal group techniques research.
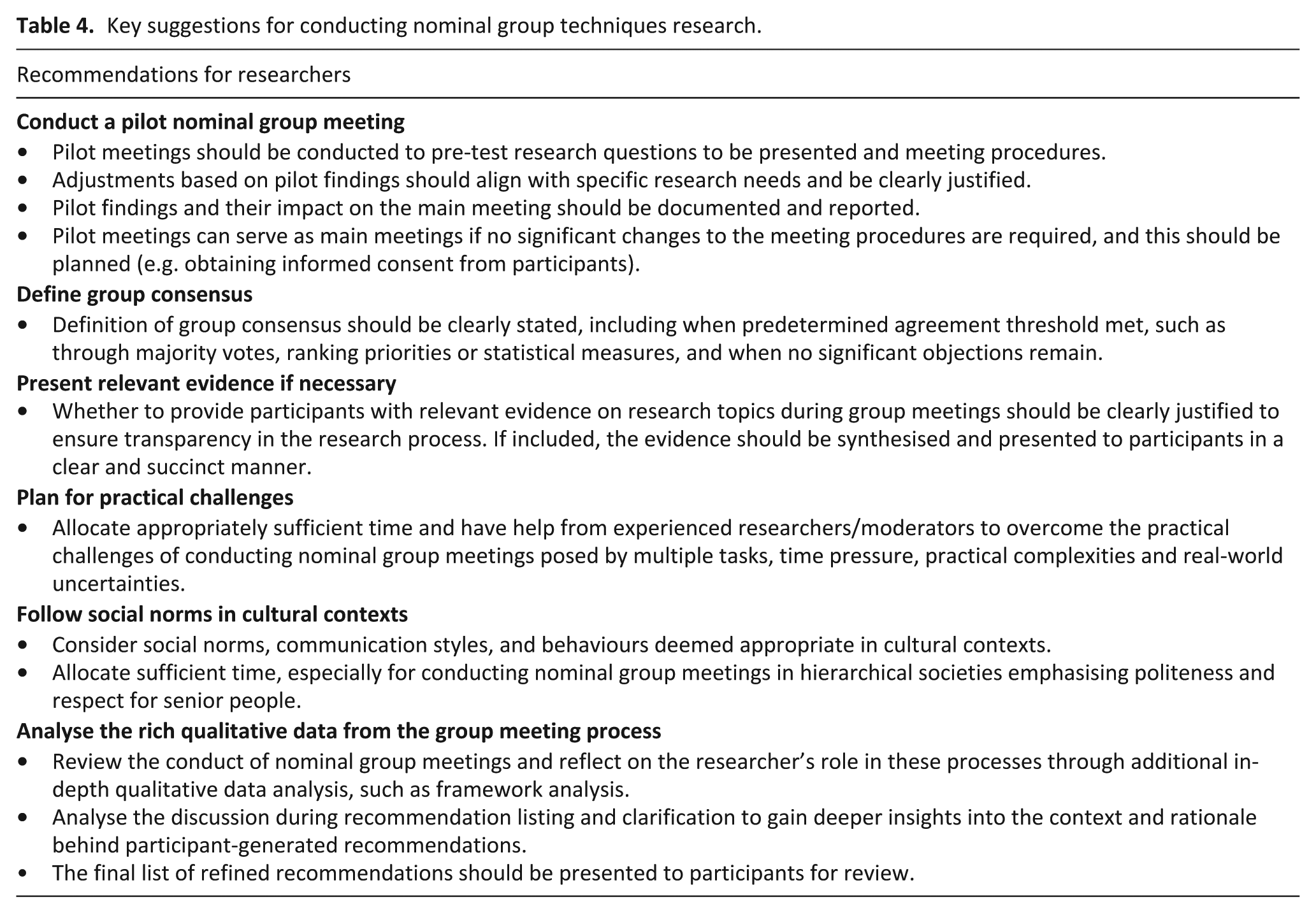
Pilot meetings should be conducted to test research questions to be presented, refine meeting procedures, and report their impact on the main meeting. If no significant changes to the procedures are required, these pilot meetings can serve as main meetings, and data can be analysed to generate findings. This should be planned so that informed consent can be obtained. We also recommend that researchers clearly justify whether relevant evidence will be presented to participants during meetings to enhance transparency.
It is important to anticipate and address practical challenges when conducting group meetings, as strictly following the original plans is often unrealistic and may compromise the quality of recommendations. These challenges, often underreported in the literature, can persist even after pilot meetings due to multiple tasks, time constraints, practical complexities and real-world uncertainties. Such issues are particularly evident during the recommendation listing, clarification, voting and ranking stages. Cultural considerations are also essential when applying the nominal group technique. In societies where interruptions are avoided as a sign of respect and politeness, allocating sufficient time for group meetings, particularly during the recommendation listing and clarification stages, and using it efficiently is vital. Prior arrangements to accommodate participants’ communication styles can help ensure they fully express their recommendations.
Although time-consuming, in-depth analysis of meeting transcripts, particularly discussions during recommendation listing and clarification, using an interpretive qualitative approach is highly recommended for future studies. This approach allows for reflection on the group meeting process and the researcher’s role and can address practical challenges encountered during the process. It provides deeper insights into the context and rationale behind participant-generated recommendations, refining them for better applicability. To assess if the original consensus has changed, the final list of refined recommendations should be presented to participants for review, with the possibility of re-ranking the recommendations.
Conclusion
The nominal group technique serves various research purposes and has significant potential to advance palliative care research and other fields. While methodologically structured, it remains flexible and can be adapted to specific research objectives or participant needs. Drawing from its theoretical foundations and practical applications in palliative care, we provide methodological reflections and identify key challenges: the absence of pilot meetings, neglecting practical challenges in conducting group meetings, insufficient attention to cultural factors and underutilisation of valuable data generated during meetings. These issues can undermine research rigour and the quality of recommendations. We also offer suggestions to address these methodological challenges to strengthen the application of the nominal group technique, including culturally appropriate approaches. This paper will support the development of more contextually relevant and implementable recommendations.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163251368974 – Supplemental material for Methodological reflections to support good practice in using nominal group techniques: Insights from applications in palliative care studies
Supplemental material, sj-docx-1-pmj-10.1177_02692163251368974 for Methodological reflections to support good practice in using nominal group techniques: Insights from applications in palliative care studies by Hui-Ju Liang, Qian Xiong and Nancy Preston in Palliative Medicine
Footnotes
Author contributions
H-JL, NP and QX contributed to the conceptualisation of the paper. H-JL drafted and revised the manuscript. All authors reviewed and approved the final version for submission.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethics approval
This is a research methodology and methods paper, and no specific or detailed participant information is reported. The example study presented in the article was approved by the National Cheng Kung University Hospital Institutional Review Board (Ref: A-ER-111-193) and Lancaster University Faculty of Health and Medicine Research Ethics Committee (Ref: FHM-2022-0972-ExRev-1).
Data management and sharing
There is no data.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.