
Abstract
Background:
The palliative care evidence base has grown substantially in recent years with the benefits, barriers, and facilitators of care delivery well established across many settings and contexts.
Aim:
We aimed to rigorously and systematically delineate the trends, themes, and scope of the top 100 papers aided by bibliometrics to map the field of palliative care science and identify future directions for the field.
Design:
We conducted a bibliometric analysis in accordance with the BIBLIO checklist for reporting the bibliometric reviews.
Data source:
Employing a comprehensive search string we examined the Scopus online database from inception to December 14th, 2024, to identify and retrieve pertinent publications. Extracted data included year of publication, number of citations and other metrics, authorship, and study design, among others.
Results:
Total citations for the 100 most cited articles ranged from 5083 to 419. Most articles originated from the US (43%), United Kingdom (16%), and Canada (15%). Overall, 83 different first authors and 87 senior authors contributed; about half first authors and 32% of senior authors were women. Forty-two different journals published the articles. Key themes were end-of-life care, palliative care integration within different medical sub-specialties (e.g. oncology, respiratory disease), clinical tool development and validation, and symptom management.
Conclusion:
Our findings provide a comprehensive map of the palliative care scientific landscape with key implications for future research, clinical practice, and policy. These results can be used to mitigate scientific disparities in author representation, ensure appropriate evidence use across international contexts, and empower high-quality evidence-based palliative care advocacy.
Keywords
The palliative care evidence base has grown substantially over the past few decades
Palliative care benefits, barriers, and facilitators for patients and care partners are well documented
In the global health context, research is predominantly disseminated by authors and institutions in high-income countries
Research in palliative care is largely driven by contributions originating from high-income countries, despite the nonnegligible need for palliative care observed in low and middle-income countries, characterized by limited access to essential care
Female scientists remain significantly underrepresented in both lead and senior authorship positions in palliative care research, mirroring existing broader gender disparities in other medical fields
Highly cited studies in palliative care extend beyond end-of-life care, encompassing chronic disease management, symptom control, and psychological implications of chronic illnesses
Future research can leverage this analysis to bridge disparities in palliative care science relevant to authorship, gender, country of origin, and area of investigation
Clinicians working across countries should recognize the inherent biases of knowledge sourced in high-income countries and adapt existing evidence to local and contextual needs
Palliative care advocates can use this “map of science” to readily identify and equip themselves with high-quality science when engaging policy and health leaders
Introduction
While the specialty of palliative care originally emerged from the British hospice movement, its core principles are now widely recognized as applicable across a broad spectrum of chronic and life-limiting diseases.1,2 Since the World Health Assembly unanimously included palliative care as a core component of comprehensive healthcare and universal health coverage in 2014, 3 palliative care science has advanced methodology development and refinement; needs assessments; and service design and delivery innovations at national, regional, and international levels.4–10 The recognition of palliative care as an evidence-based medical subspecialty over the last decades has, indeed, catalyzed a surge in research activity within the field, 11 driving the growth of a rapidly evolving body of knowledge. 12 This growing scientific foundation plays a pivotal role in shaping policy agendas, influencing funding choices, and directing the development of services and targeted interventions. 13 However, fundamental issues in the access to palliative care still persist—73 million people worldwide are estimated to have serious health-related suffering amenable to palliative care, but still nearly 90% of the global palliative care needs remain unmet. More interestingly, almost 80% of the unmet palliative care needs are found in low- and middle-income countries (LMIC) and, while the World Health Organization (WHO) asserts that palliative care should be universally accessible, 14 recent research efforts have underlined critical differences in care access depending on the geopolitical situation, socioeconomic conditions, and cultural differences.15,16
Citation analyses have long been employed to map research contributions and identify prevailing trends. 17 When integrated with bibliometric analyses, these statistical methods facilitate a more precise definition of the scope, advancements, methodologies and authorship characteristics within specific research domains. Additionally, they enable the evaluation of extensive quantities of bibliometric data derived from global scientific outputs, thus offering interesting insights into their contents and methodology. 17 With the purpose of better delineating specific aspects of the palliative care landscape, a growing number of bibliometric analyses are currently available in the literature18–24—spanning several different topics such as spiritual care, 25 nutritional therapy, 26 non-invasive ventilation, 27 the interplay between the COVID-19 pandemics, and palliative care,28,29 end-of-life care, 30 research methodology, 13 palliative care in oncology, 31 and perinatal and pediatric palliative care.32,33
While bibliometric analyses delineating the trending topics in global and regional palliative care research are found in literature, a bibliometric analysis to identify the most influential articles in the field of palliative care has not been conducted yet. Therefore, in this study, we systematically evaluated the predominant research themes within palliative care scientific production. To prioritize a health equity lens, we focused analysis and discussion on country, author, and gender representation to assess whether relevant gaps (e.g. gender imbalances) explored in other fields, 34 existed in palliative care as well. We speculate that—by systematically exploring and understanding these inequities—the present investigation may help raise awareness of gender imbalances and therefore inform national and global policies. Furthermore, by mapping the most cited articles, we strive to provide a practical tool for both navigating high-quality science, and offering a deeper understanding of palliative care research trends, which can help bridge persistent gaps in authorship, gender representation, and geographical origin, ultimately fostering a more equitable and inclusive global discourse.
Material and methods
Search strategy and database selection
The methodology used in this study follows the approaches previously described in other bibliometric studies 35 and conforms to the BIBLIO checklist for reporting the bibliometric reviews of the biomedical literature (Supplemental Material, Supplemental Table 1). 36 Aided by a comprehensive search string that included terms such as “palliative care,” “palliative medicine,” “supportive care,” “life-limiting,” and “life-threatening,” one investigator (J.D.U.) searched the Scopus online database (www.scopus.com) to retrieve the search hits (Supplemental Material S1, Search string). The Boolean operators “OR,” “AND” were used to combine the search terms and enhance search precision. There were no exclusions based on language or year of publication. Both data access and download were performed on December 14th, 2024.
Data retrieval and charting
We exported literature data as a Microsoft Excel (.xlsx) worksheet. Duplicate publications were removed using EndNote X9 (Clarivate Analytics). The remaining search results were organized by total citations number; articles were then ranked from the most cited to least, and subsequently initially screened for potential retrieval and inclusion at title and abstract levels by two independent investigators (A.B. and S.C.). Inclusion criteria were: (i) original research (i.e. either studies reporting original data or publications not presenting original data including—but not limited to—guidelines and expert consensus documents, narrative and/or systematic reviews, meta-analyses, commentaries, letters, and editorials) having either adult or pediatric patients as the study population; (ii) focused on patients, relatives, caregivers, and/or healthcare providers; (iii) within the field of palliative care. In instances of disagreement, a third senior investigator (J.D.U.) was consulted. Following this preliminary assessment, a further careful examination of full-text articles was performed by A.B. and S.C. to finalize the selection of the 100 most cited studies, by total number of citations, in the field of palliative care.
Next, for each of the 100 identified articles, we used SciVal (www.scival.com) to collect the Field-Weighted Citation Impact (FWCI) for each article. The FWCI is a metric that compares the actual publication to the expected number of citations based on the actual citations of similar publications—therefore, a larger FWCI corresponds to a higher citation impact. Similar publications are defined by publication year, type, and subject area. Of note, the FWCI was not available for publications prior to 1995.
Data extraction
The following pertinent information which fulfilled research requirements was systematically extracted from the retrieved studies: (i) year of publication; (ii) total number of citations; (iii) title; (iv) first author; (v) senior author (i.e. last author); (vi) study design; (vii) corresponding author’s country; (viii) gender of the first and senior (i.e. last) author; (ix) publishing journal; and (x) FWCI.
The gender of first and senior author was determined by querying authors’ first names in the Genderize database (available at: https://genderize.io). 37 For authors whose first names were not found in the Genderize database, the gender was identified by a manual internet search, including consultation of authors’ professional website, photographs of the authors, and references to them by male or female pronouns. 38
Additionally, we calculated journal metrics (i.e. impact factor [IF] and quartile)—as sourced from the Journal Citation Reports™ 2023 (Clarivate Analytics)—alongside citation density (i.e. total number of citations divided by the number of years each work had been published) 39 for each of the retrieved articles and cumulative citations (i.e. the sum of the citations of the articles published by the same journal) for each journal. Lastly, articles were then manually classified by topic following screening of both their abstract and full text. Both investigators (A.B. and S.C.) independently classified articles based on their main topic. Subsequently, through mutual comparison and discussion—also involving a senior investigator if needed (F.M.)—a final consensus on articles classification was reached, to define a reasonable and coherent number of topics to delineate the scope of palliative care scientific output. In cases of articles encompassing more than one topic, the most prominent and significative one was chosen for inclusion in the final analysis.
Results
Our search string yielded a total of 7238 documents in the Scopus database (from inception until December 14th, 2024). Following the download of search results, the data were exported into a Microsoft Excel (.xlsx) file, and duplicate records were removed. The remaining results were then systematically reorganized in descending order of total citation count. The first 100 most cited studies that satisfied the inclusion criteria (i)–(iii) were selected for inclusion and subsequent bibliometric analyses. The key features of the first 25 most cited studies are summarized in Table 1, while a comprehensive overview of the 100 most cited articles in palliative care is presented in the Supplemental Material, Supplemental Table 2.
Top 25 most cited articles in palliative care.
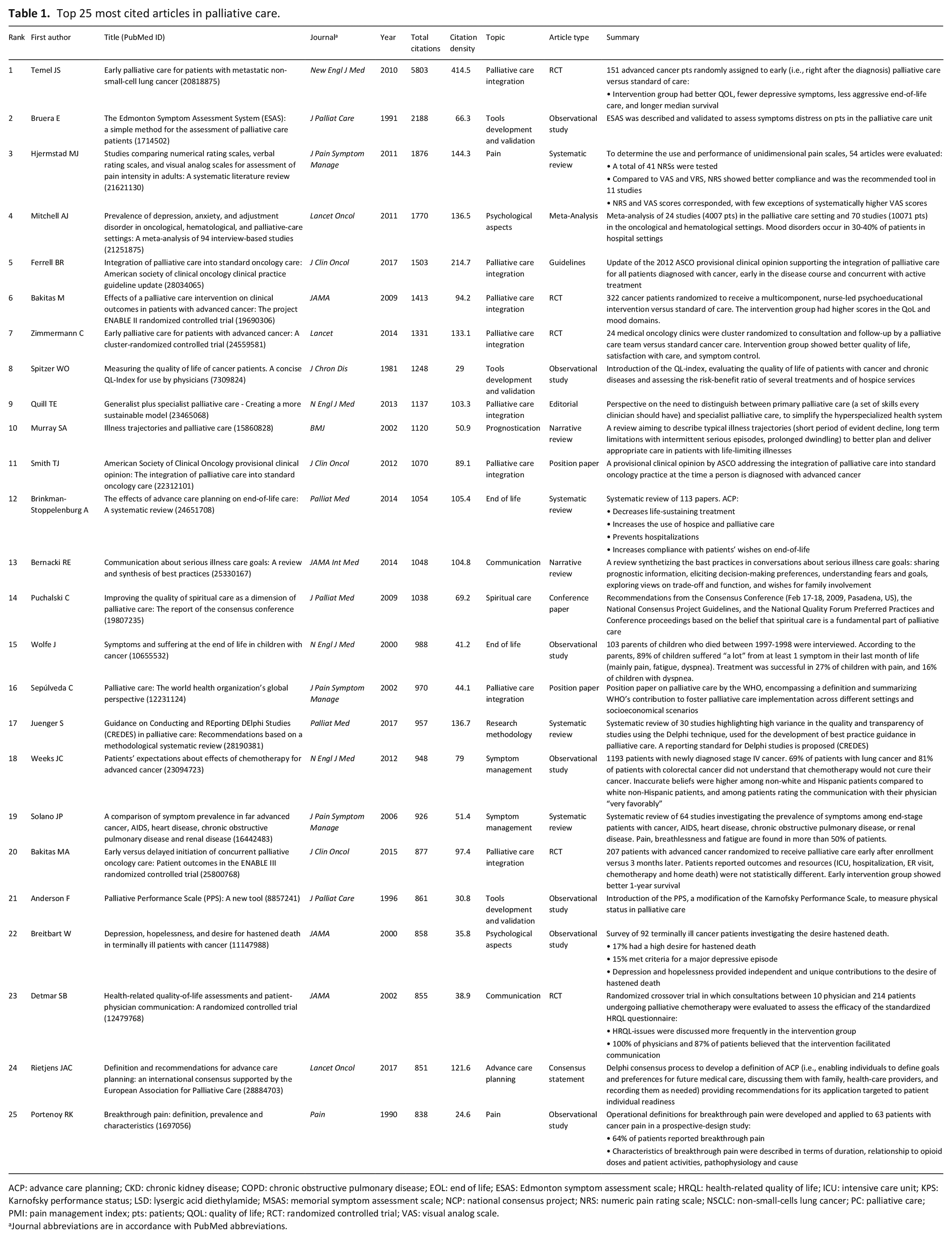
ACP: advance care planning; CKD: chronic kidney disease; COPD: chronic obstructive pulmonary disease; EOL: end of life; ESAS: Edmonton symptom assessment scale; HRQL: health-related quality of life; ICU: intensive care unit; KPS: Karnofsky performance status; LSD: lysergic acid diethylamide; MSAS: memorial symptom assessment scale; NCP: national consensus project; NRS: numeric pain rating scale; NSCLC: non-small-cells lung cancer; PC: palliative care; PMI: pain management index; pts: patients; QOL: quality of life; RCT: randomized controlled trial; VAS: visual analog scale.
Journal abbreviations are in accordance with PubMed abbreviations.
Citation analysis
The total number of citations of the 100 most cited articles ranged from 5803 to 419. All these articles were published between 1981 and 2020, with most of them (n = 44) being published between 2000 and 2009 (Supplemental Material, Supplemental Figure 1). The citation density ranged from 414.5 to 13.6. The FWCI, available only for articles published after 1995, ranged from 196.64 to 1.75. The article “Early palliative care for patients with metastatic non-small-cell lung cancer” by Temel et al. 40 had the highest total citation count, citation density and FWCI. Table 2 features a comparative analysis of the top 10 studies, ranked by citation density, total number of citations, and FWCI, respectively.
Most cited journals with total number of citations, number of published articles, impact factor (IF), and quartiles.
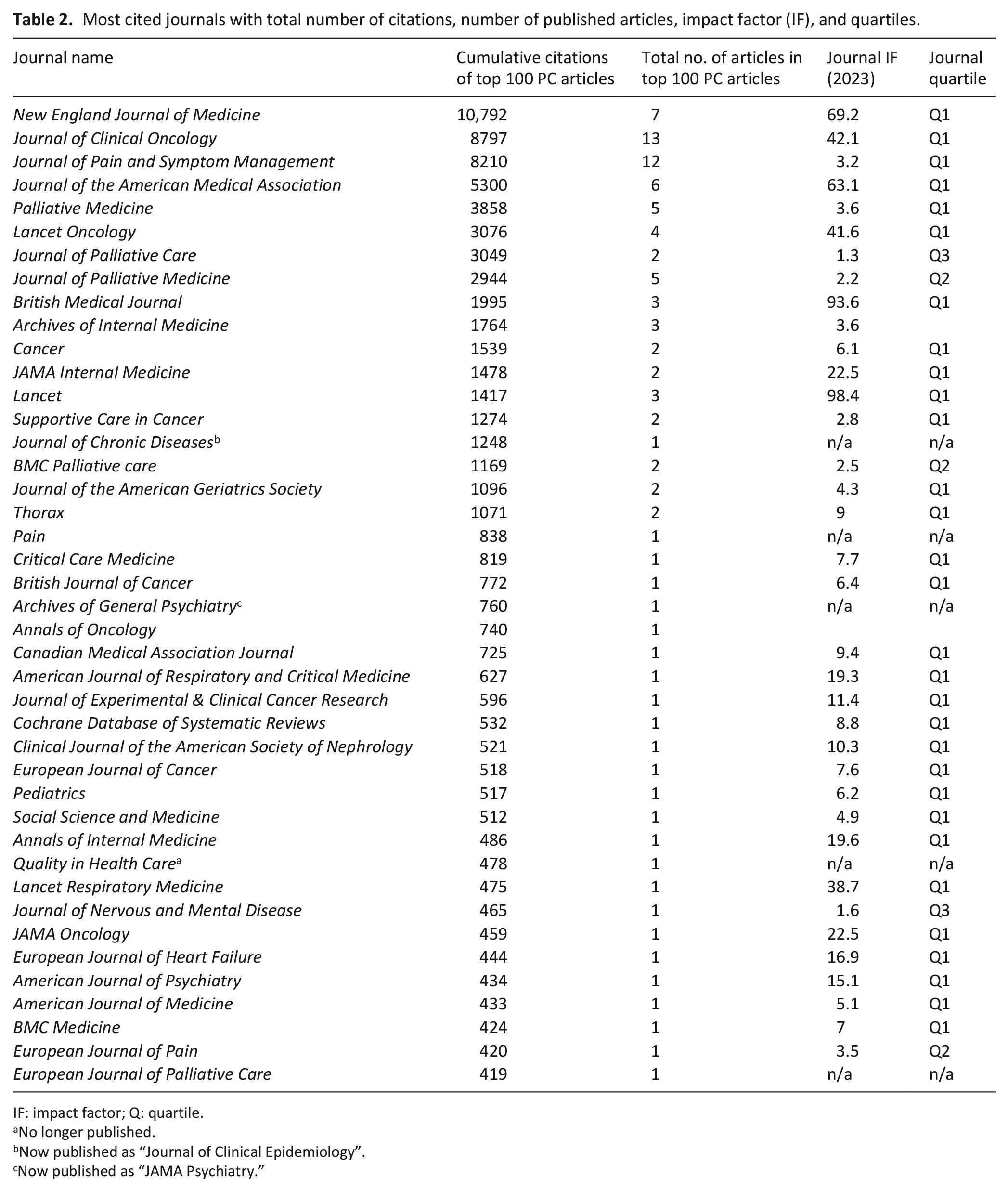
IF: impact factor; Q: quartile.
No longer published.
Now published as “Journal of Clinical Epidemiology”.
Now published as “JAMA Psychiatry.”
Journal analysis
The 100 most cited articles by total number of citations were published by 42 different journals (Table 3). The Journal of Clinical Oncology published the largest number of these (31%), followed by the Journal of Pain and Symptom Management (29%), and the New England Journal of Medicine (17%), as shown in Figure 1(a). In terms of cumulative citations, the New England Journal of Medicine led with a total of 10,792 citations, followed by the Journal of Clinical Oncology (n = 8797) and the Journal of Pain and Symptom Management (n = 8210), as shown in Figure 1(b).
Top 10 articles with highest citation/year rank.
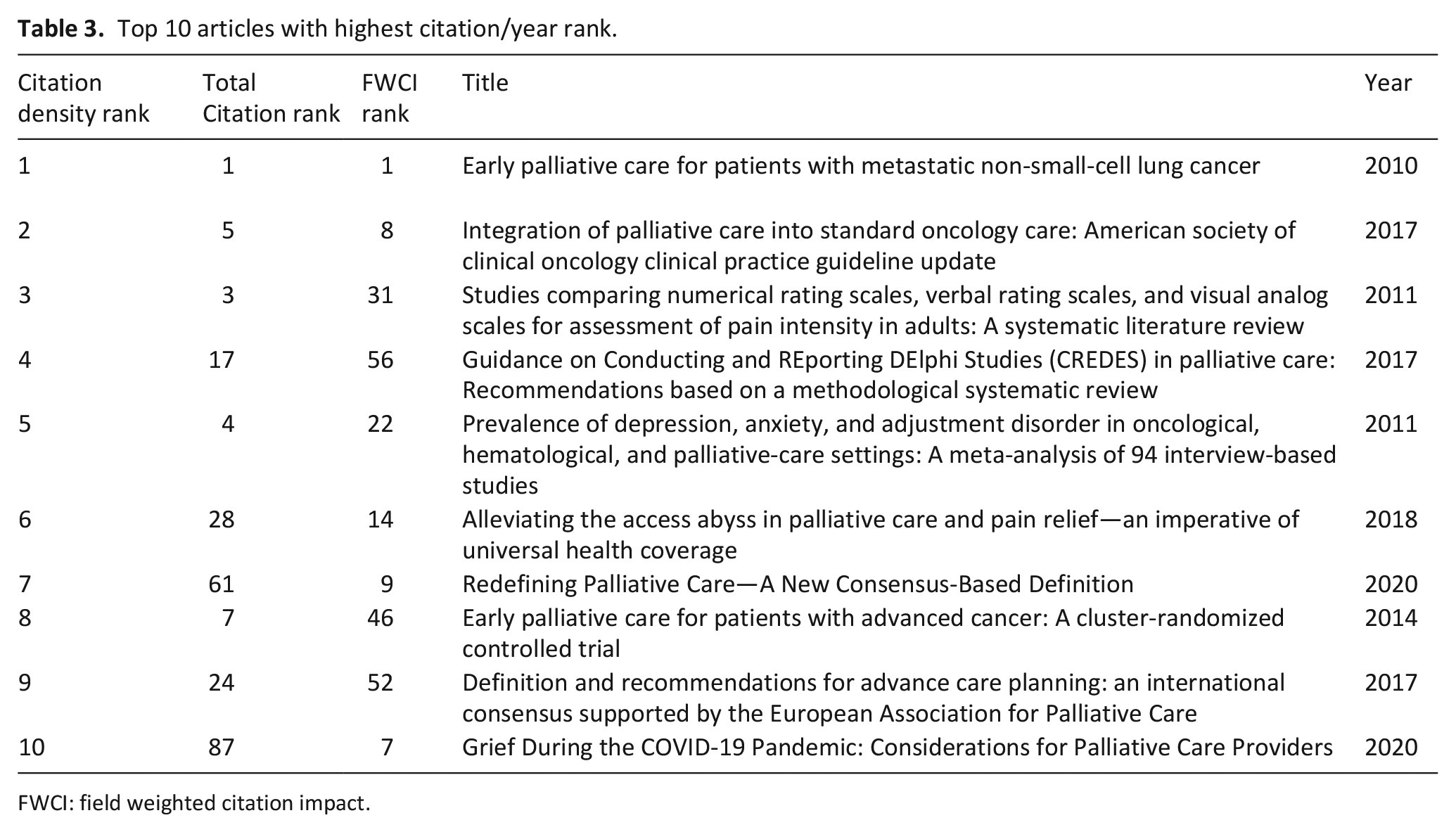
FWCI: field weighted citation impact.
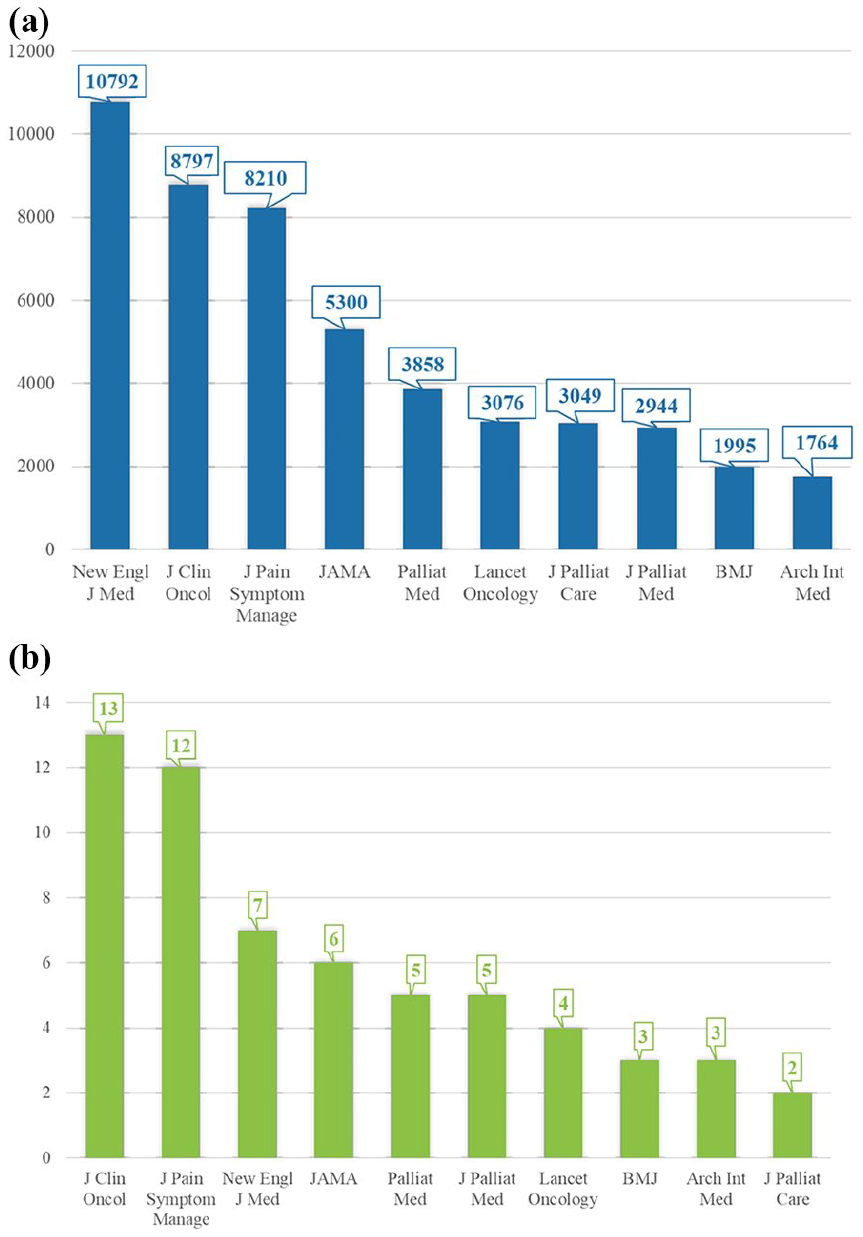
(a) Rank of the top 10 most cited journals, by their respective cumulative citation number, led by the New England Journal of Medicine and (b) rank of the top 10 most cited journals and by their respective cumulative publications number, led by the Journal of Clinical Oncology.
Authorship and countries analysis
Eighty-three different first authors contributed to the 100 most cited articles by total citation in palliative care. Among them, 12 authors (14%) had more than one publication, with one author credited with three publications and another author with five publications. Regarding senior authorship, a total of 87 senior authors were identified. Eight of them contributed to more than one publication, with Harlos M and Higginson IJ being the most prolific, with three articles each as last author. Overall, 47 papers (47%) were authored by a female first author, and female first authors accounted for almost half (44%) of the total number of first authors (37/83). Conversely, only one-third (34%) of the 100 most influential articles in palliative care were authored by a female senior author, with male senior authors accounting for the majority of senior authorship (68%, 59/87; Supplemental Material, Supplemental Figure 2).
According to the corresponding author affiliation, the articles originated from 15 different countries. The number of articles grouped by country of origin was led by the USA with 43 manuscripts, followed by the UK (n = 16) and Canada (n = 15). Other countries with more than one article among the 100 most cited included Australia (n = 3), Germany (n = 4), Italy (n = 2), the Netherlands (n = 6), Norway (n = 2), and Switzerland (n = 3; Supplemental Material, Supplemental Figure 3). The retrieved articles originated from 76 different institutions. Dana-Farber Cancer Institute and King’s College were the two most prominent, each contributing with six publications, while Massachusetts General Hospital, and University of Manitoba ranked second, both contributing with four publications each.
Study types
According to the study type, articles were classified into position papers/guidelines/consensus statements (n = 20), intervention studies (n = 21—of which, 15 were randomized controlled trials [RCT]), observational studies (n = 31), narrative reviews (n = 8), systematic reviews (n = 13), and meta-analyses (n = 4; Figure 2).
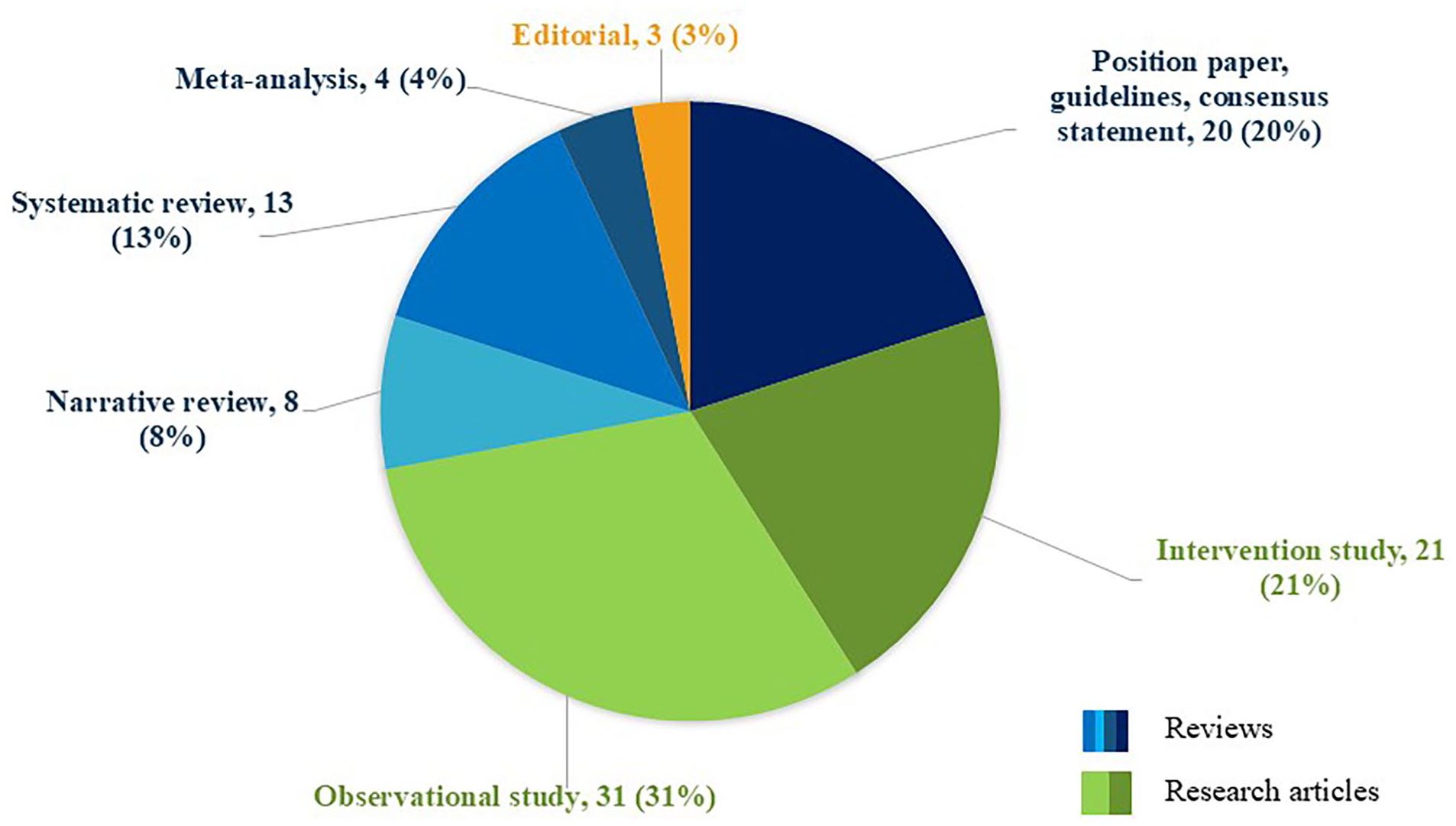
Study design distribution of the 100 most influential articles in palliative care (study design, number of articles, and percent).
Topic and subject distribution
The most frequently addressed topic among the articles was end-of-life care, with 20 papers. The second most common topics were the integration of palliative care within various medical specialties (n = 18), followed by themes such as the development and validation of clinical tools such as questionnaires and scales (n = 10), and psychological aspects of chronic and life-limiting illnesses (n = 9). Topics distribution is detailed in Figure 3.

Overview of the topics of the100 most influential articles (topic, number of articles, and percent). The category “Others” includes: palliative care effectiveness, cost analysis, research methodology, advance care planning, shared decision making, public health analysis, unmet needs, healthcare professional training, quality of life, COVID-19, palliative care definition.
The majority of the retrieved studies were set within the context of palliative and hospice care (n = 45). However, a substantial number of studies evaluated the delivery and integration of palliative care within other medical sub-specialties. Specifically, oncology emerged as the predominant specialty (n = 33), followed by respiratory (n = 4), psychiatry (n = 3), neurology (n = 2), pediatrics (n = 2), nephrology (n = 1), and cardiology (n = 1).
Discussion
Main findings of the study
The present bibliometric analysis aimed to provide a practical guide for navigating the current landscape of palliative care research, offering a comprehensive understanding of its prevailing trends. Notably, we found significant disparities in terms of country representation—with high-income countries dominating the palliative care research landscape—as well as ongoing gender inequities. Our analysis builds on these findings to help bridge persistent gaps in authorship, gender representation, and geographical diversity, ultimately fostering a more equitable and inclusive global discourse. As such, more than a decade since the World Health Assembly passed resolution 67.19 that identified palliative care as a core component of comprehensive healthcare and universal health coverage, 3 insufficient progress has been made in expanding access to palliative care at national, regional, and global levels. 41 Given these ongoing disparities, this analysis offers a robust and clear mapping of palliative care science to drive continued improvements and bridge worsening divides in palliative care access.
What this study adds?
The great citation impact of articles emphasizing the integration of early palliative care across nononcological, chronic diseases and focusing instead on the assessment of symptom and pain severity—critical elements in optimizing patient care and quality of life—underscores a shift in the palliative care field toward proactive models of care that are reflected in global efforts to improve quality of life and symptom control across different patient populations. Stemming from Temel’s foundational study, early palliative care integration has been increasingly explored as a model for nononcological chronic and life-limiting conditions, such as chronic obstructive pulmonary disease, 42 and heart failure. 43 However, its effectiveness on improving quality of life in these populations remains an area of active debate. A recent systematic review by Mós and Reis-Pina 44 explored this issue and found that early palliative care integration did not produce any statistical difference in quality of life for patients with heart failure, end stage liver disease, idiopathic lung fibrosis, chronic obstructive pulmonary disease, and HIV. Nevertheless, early palliative care integration demonstrated measurable benefits, including pain and fatigue reduction in patients with heart failure, symptom distress reduction in patients with HIV, and decreased anxiety and depression in patients with stroke. It also fosters the integration of advance care planning in chronic obstructive pulmonary disease populations, and leads to longer time to first readmission and days alive outside of the hospital for patients with end stage liver disease. 44 This highlights the nuanced impact of early palliative care across different disease trajectories and the existing critical gap, which call for the development of tailored interventions to address the unique needs of nononcological patients, refining palliative care models in a patient-centered fashion.
While it is important to recognize that citation counts “per se” do not inherently validate the scientific merit of a publication, a high citation count may serve as a clear indicator of an article’s visibility and influence within the scientific community.17,45 Consistent with previous bibliometric analyses,45,46 in our investigation we also compared citation density and FWCI to total citation counts for the first 10 articles with the highest citation density. While most of the most cited articles were published in the decade 2000–2009, the top 10 articles ranked by citation density are all recent (i.e. published between 2010 and 2020) with the oldest article published in 2010. 40 The increase in citation density by decade likely reflects global advancements in access to scientific literature, particularly through the widespread availability of electronic articles, digital journals, and online scientific database repositories. 45 Furthermore, the observed increase in citation density may be attributed to the growing recognition of palliative care as an essential element in the multimodal management of chronic and life-limiting illnesses. This is also supported by recent guidelines and position papers advocating for the early integration of palliative care and recognizing its significant benefits on patient outcomes.47,48
The New England Journal of Medicine ranked highest in cumulative citations (n = 10,792), surpassing the Journal of Clinical Oncology (n = 8797), despite publishing only half as many articles (13 vs 7 articles, respectively). In this regard, high IF journals (such as the New England Journal of Medicine, with an IF of 96.2) are attractive to authors who seek to maximize the visibility and citation potential of their work, thus perpetuating a cycle in which highly cited articles maintain the journal’s elevated IF. This phenomenon is known as Bradford’s law and has been described in previous bibliometric analysis studies. 49 However, the concentration of citations in high IF general medical journals present a structural challenge for palliative care researchers. While these journals maximize research visibility, they may not prioritize highly specialized palliative care studies, potentially limiting the dissemination of critical advancements. Given the cross-disciplinary nature of palliative care, restricted diffusion of key findings could hinder the adoption of practice-shaping interventions across medical specialties. Additionally, researchers publishing in dedicated palliative care journals may face disadvantages in citation-based metrics, leading to the underrepresentation of essential yet specialized research in top-tier publications. To address this limitation, policy makers and funding bodies should explore alternatives to traditional metrics (e.g. FWCI, societal impact of research) to ensure that palliative care research receives the recognition and resources necessary to drive meaningful progresses in the field.
To gain an in-depth comprehension of the palliative care scientific output, it is crucial to consider the literature’s country of origin. In the global health context, about 95% of available medical evidence emerges from high-income countries which represent a mere 15% of the global population. 50 Similar trends are seen across fields, including anesthesia, orthopedics, bariatric surgery, and otolaryngology.45,49,51–54 Our findings align with the aforementioned imbalances specific to palliative care science, with institutions from high-income countries (i.e. the United States) dominating the scientific landscape—aligning with the findings of previous bibliometric analyses.23,24,26 While this is likely due to the substantial financial resources allocated to health science research in the United States, 45 it is particularly problematic given that nearly 90% of global palliative care need is unmet and the majority of unrelieved health-related suffering that is amenable to palliative care exists in LMICs. 55 In fact, more than 80% of the 70 million people in need of palliative care—over 50 million people—live in LMICs with little or no access to controlled essential medicines (i.e. opioids) to alleviate symptomatic distress in serious illness and at the end of life. 8 Additionally, a previous bibliometric analysis showed that weak collaborations exists in palliative care research between LMICs and high-income countries, potentially further undermining LMICs visibility and palliative care access. 24
Prior analyses have shown that the inequities are not just in palliative care provision but also in the science that informs it.20,22 For instance, one bibliometric review showed that roughly 90% of the literature related to opioid medicines focused on opioid misuse and addiction (a well-noted crisis in high-income countries) 56 whereas only 10% focuses on the dearth of opioid access globally (a well-noted barrier to palliative care access in LMICs).9,57 Although the top-cited research in the current study is of the highest scientific quality and has inarguably shaped the field in all domains of practice, the disproportionate visibility of science from high-income countries inadvertently perpetuates palliative care divides that marginalize the world’s poorest populations.
The findings emerging from first author gender analysis align with previous evidence showing a growing representation of women in hospice and palliative care medicine. For instance, since 2014, women have constituted the majority of hospice and palliative care medicine fellowship graduates in the U.S., and 52% of program directors in 2019 were women. 58 In contrast, although palliative care research exhibits a much less pronounced gap, the senior authorship gender analysis reflects the well-documented underrepresentation of women in authorship found to happen in other scientific fields as well (e.g. critical care medicine, neuro-oncology and urology), further substantiating the persistent gender gap in several medical fields.38,59,60 In this regard, Vranas et al. 38 reported an overall prevalence of 31% and 19.5% of females as first and senior author, respectively, in the 40 most impactful critical care medicine journals. Similar findings—which suggested a higher representation of male authors in both first and senior authorship positions—were reported by Behmer Hansen et al. 59 in an analysis of the five most influential neuro-oncology journals, in which women accounted for 21% of first authors and 13.6% of senior authors. Likewise, Shukla et al. 60 observed a comparable trend in urological research, where an analysis of articles with a US correspondence address published in the two most impactful urology journals revealed that women constituted 15% of first authors and 10% of senior authors only. Our finding regarding the stark predominance of male senior authors—in line with what is reported for other medical fields—contrasts with the abovementioned findings highlighting a high rate of women holding leading positions in the academic palliative care field. 58 Contextualized within the broader context of gender disparity in science, the observed gender imbalance and the underrepresentation of LMIC-based research underscores how systemic barriers in scientific research may be present across geographic and gendered lines, reinforcing a cycle of limited visibility, and scientific influence. This calls for the urgent need for targeted efforts to promote gender and geographical equity and in research leadership and authorship.
Regarding key themes, although end-of-life care was the most frequent topic among the articles, it accounted for only 20% of the total. Other prominent themes included the integration of palliative care into the management of chronic and/or life-limiting diseases, the development and validation of clinical tools (e.g. scales and questionnaires), the psychological aspects of chronic and/or life-limiting illnesses, alongside symptom, and pain management. Altogether, these topics accounted for 48% of the 100 most cited articles, underscoring the wide scope of palliative care which extends beyond the sole end-of-life contexts. This finding also indirectly reflects the multifaceted role of palliative care in addressing psychological, physical, and spiritual needs across both early and late stages of chronic and/or life-limiting conditions. 25 These findings on scope and illness trajectory are particularly important for health system, public, and policy stakeholders who may limit palliative care utility to the end of life and are potentially uninformed about how palliative care integration across the serious illness continuum could improve relevant outcomes. Moreover, the distribution of the articles across various medical specialties (encompassing the fields of neurology, psychology and psychiatry, respiratory diseases, and cardiology) highlights the ever-expanding reach of palliative care, which has historically focused primarily on oncology and is now instead widely recognized as essential for managing patients’ suffering from a wide range of chronic and life-limiting conditions (e.g. dementia, chronic respiratory diseases, heart failure). However, this analysis constitutes a “snapshot” of the palliative care scientific output in a defined moment in time. It is reasonable to assume that emerging trends and novel paradigms—including the development of telehealth-based services to support patient and carers, 61 and the impact of artificial intelligence-based applications with related opportunities and ethical challenges62,63—may have been excluded from the analyzed topics and may, nevertheless, represent important future directions of research within the palliative care field over the coming years.
The findings of this analysis can do much to empower palliative care experts and allies with information regarding the most rigorous science to inform evidence-based advocacy efforts. Evidence-based advocacy is essential to improve practice, decrease disparities, and promote investments in palliative care capacity building, stigma reduction, and essential medicine access.64–66 With a clear understanding of publication trends, study areas of focus, and geographic origin, our study empowers advocates to readily identify scientific gaps to argue for enhanced research investments, particularly in LMICs where resources are severely constrained, and palliative care continues to seek validation at a national level. Building on our findings, the establishment of LMIC research consortia, open-access funding programs, and global mentorship initiatives for female researchers may represent critical steps toward narrowing the existing disparities and fostering more equitable participation in the palliative care global research landscape. Equipped with this map of the most influential science, advocates will be able to synthesize the most cited studies and merge key findings with their local priorities and sociopolitical narratives to promote locally effective policy and regulation.
Strengths and limitations of the study
While this bibliometric analysis of the 100 most cited articles in palliative care provides valuable insights into the scientific landscape of the field and encompasses among its strengths adherence to the BIBLIO checklist and dual-investigator screening, it is important to acknowledge several of its inherent limitations. Bibliometric analyses cannot replace systematic reviews or meta-analyses, which are designed to yield conclusive evidence for clinical decision-making in evidence-based medicine. 25 Additionally, a significant limitation of this analysis lies in the temporal disparities in citation patterns, as more recent publications inherently have had less time to accumulate citations compared to more dated works. To address this bias, we reported articles’ citation density and FWCI. While we acknowledge that these metrics may be subject to limitations, including potential bias introduced by self-citation, we believe that the diversity of authorship, and institutions represented contributed to milden the impact of this potential source of bias. Another potential source of bias is derived from reliance on a single database (i.e. Scopus)—a choice that, however, was imperative to systematically retrieve all the most important metrics—yet it may also have biased the attribution of authorship roles, as Scopus does not acknowledge the presence of co-first, co-last, and/or co-corresponding authors, and hindered the retrieval of publications from LMICs—which may have been published in non-indexed journals. Moreover, inaccuracies in gender determination, attributable to either the manual search or to the Genderize database intrinsic limitations, may be present. Lastly, we acknowledge that our results are a “snapshot” of literature at a point in time. As citation trends evolve, the findings of the present investigation are subject to evolve as well. Nevertheless, the present bibliometric analysis is systematically and rigorously constructed, thus allowing the delineation of a valuable and actionable roadmap for future research, policy, and clinical practice in palliative care.
Conclusions and future perspectives
In our bibliometric analysis of the 100 most cited articles in palliative care we found that the majority of the scientific output originated from the US, with a strong underrepresentation of LMICs—where the access to palliative care may play an even more important role. There are clear implications to ensure LMIC partnership and leadership in palliative care research endeavors. Additionally, while the gender gap in palliative care research appears to be less apparent compared to that observed in other medical fields (e.g. critical care medicine, neuro-oncology and urology), our findings emphasized the need for further targeted investigation aimed at achieving a more comprehensive characterization and understanding of the issue while amplifying the scientific contributions of women in the field. Overall, these findings provide a comprehensive map of the palliative care scientific landscape presenting key implications for future research, clinical practice (e.g. fostering early palliative care integration), and policy (e.g. by raising awareness on the existing gaps in palliative care access between high-income countries and LMICs). These results can be used to mitigate scientific disparities in author and country representation, ensure appropriate evidence use across international contexts, and empower high-quality evidence-based palliative care advocacy.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163251362560 – Supplemental material for Mapping the Science of palliative care: A bibliometric analysis of the top 100 cited articles
Supplemental material, sj-docx-1-pmj-10.1177_02692163251362560 for Mapping the Science of palliative care: A bibliometric analysis of the top 100 cited articles by Jacopo D’Andria Ursoleo, Alice Bottussi, Sandy Christiansen, Donald R Sullivan, Kelly C Vranas, William E Rosa and Fabrizio Monaco in Palliative Medicine
Footnotes
Acknowledgements
The authors would like to thank Enrica Piazza, MDs and Edoardo Mongardini, MDs (Vita-Salute San Raffaele University, School of Medicine) for their help in designing the Visual Abstract.
Authors’ contributions
Jacopo D’Andria Ursoleo: Conceptualization, Supervision, Study design, Investigation, Methodology, Writing – Original Draft, and Writing – Review & Editing. Alice Bottussi: Conceptualization, Investigation, Study design, Methodology, Data Curation, and Writing – Original Draft. Sandy Christiansen: Methodology, Investigation, Writing – Review & Editing. Donald R. Sullivan: Methodology, Investigation, Writing – Review & Editing. Kelly C. Vranas: Methodology, Investigation, Writing – Review & Editing. William E. Rosa: Supervision, Methodology, Investigation, Writing – Review & Editing. Fabrizio Monaco: Supervision, Investigation and Writing – Review & Editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Availability of data and materials
Further information is available from the corresponding authors upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.