
Abstract
Background:
Despite the increasing prevalence of dementia, persons with dementia often receive suboptimal care near the end of life. In many countries, specialized end-of-life support is offered by hospice. During the transitions to end-of-life care, caregivers play a crucial role in the decision-making and care provision for the persons with dementia. However, caregivers’ experiences regarding the initial entry to hospice have not been comprehensively assessed in the dementia context.
Aim:
To synthesize qualitative evidence on the caregiver-reported barriers and facilitators to hospice enrollment for persons with dementia.
Design:
Systematic review and thematic synthesis
Data sources:
We conducted a systematic literature search across PubMed, CINAHL, Embase, PsycINFO, and Scopus. We considered articles published between 2009 and 2024 that contained qualitative data on hospice entry collected from dementia caregivers.
Results:
Twenty-two articles met our study eligibility criteria. Five themes were identified: (a) caregivers’ observation and perception of severe stage dementia, (b) whether hospice was the right choice for persons with dementia, (c) burden due to the practical aspects of caregiving, (d) emotions and perception about death and hospice, and (e) guidance and access to hospice. These five themes encompassed 11 facilitators and 15 barriers.
Conclusions:
Dementia caregivers experience intrapersonal, interpersonal, emotional, logistical, and physical challenges in ensuring quality end-of-life support for their loved one (e.g. limited understanding of end-stage dementia, gatekeeping providers, and family conflicts). The unique needs of caregivers caring for a seriously ill family member with dementia are not being fully addressed by the current available services and policies.
Dementia is now among the leading causes of death worldwide, which calls for specialized support at the end of life.
While significant numbers of persons with dementia have high palliative needs, hospice entry may not be guaranteed for all patients who seek it due to strict admission criteria or late referrals.
As persons with dementia experience significant decline in functional and cognitive abilities near death, family caregivers are often involved in end-of-life decision-making and care coordination.
Our findings highlight the uniqueness of dementia in the context of hospice due to the unpredictable and/or prolonged nature of its end-of-life trajectory.
Caregivers of persons with dementia experience a variety of emotional, physical, logistical, intrapersonal, and interpersonal challenges as they consider or pursue hospice for their family member.
Hospice care models, whether operated under certain eligibility criteria or primarily driven by professionals’ referrals, commonly focus on time-based prognosis of the person with dementia, which does not correspond with how caregivers perceive end-of-life caregiving in severe dementia.
Integrating a need-based approach to hospice enrollment by regularly assessing caregivers’ burden and their openness to palliative approaches could help better tailor hospice entry for persons with dementia and their families, including end-of-life care, symptom management, and respite.
Further research into the specific contexts and available resources that support hospice transition for persons with dementia is warranted to improve the provision of quality end-of-life care for this population.
Introduction
Dementia is a progressive and terminal illness associated with structural and functional impairments and high symptom burden, especially near death. The World Health Organization estimates more than 55 million persons with dementia worldwide and its impact on society is expanding rapidly. 1 The United Kingdom’s Office for National Statistics reported that death caused by dementia comprises approximately 12.5% of all deaths in England and Wales in 2019. 2 Similarly, in the United States, Alzheimer’s disease was the seventh leading cause of death in 2022. 3 Such global trends underscore the need for specialized end-of-life support for persons with dementia.
Hospice upholds the values of compassion and dignity for terminally ill individuals, 4 attending to the physical, spiritual, social, and psychological needs of the patient and their families.5,6 Although commonly operating under this philosophy, there are cross-national differences in hospice regarding its setting, access, and finance. For instance, hospice in the United States is most commonly offered at home 7 ; to be funded by the Medicare Hospice Benefit, patients must forgo curative treatments. While many hospitals have affiliated hospice teams, there are also stand-alone organizations dedicated exclusively for hospice. In the United Kingdom, hospice services substantially rely on charitable donations, 5 and are commonly provided in the patients’ residence or inpatient units. 8 Hospice in the Netherlands, for example, can be provided within specialized palliative care units in nursing homes.9,10 To encompass the global variations of hospice care models, in this paper, we define hospice as a specialized form of palliative care oriented toward the end of life, provided across all care settings—private residences, nursing homes, senior living communities, or inpatient units.
For persons with dementia and their families, hospice can achieve desired outcomes such as care satisfaction, less unmet needs, and better quality of dying.11,12 Nonetheless, hospice is not guaranteed for everyone who wants it, and each country has its own enrollment protocol. In the United States, the Centers for Medicare and Medicaid Services outline certain admission criteria. For instance, persons with dementia must show stage 7 on the Functional Assessment Staging Scale (severe dementia) and have conditions such as aspiration pneumonia, decubitus ulcers, or constant weight loss. 13 Although dementia-related conditions are indeed leading diagnoses for hospice enrollment in the United States, 7 a hospice model built upon strict criteria leads to challenges such as live discharge and recertification. 14 In other countries, specialist palliative care services may be available at end of life outside specified eligibility. Yet, referrals from healthcare professionals are still required and could be initiated very late. 15
For persons with dementia, caregivers, namely families or friends providing unpaid care for the individual, 16 play a crucial role near death. Due to the patients’ cognitive and functional decline, caregivers often engage in care planning as proxies and coordinate day-to-day care for their loved one. Kumar et al. 17 reported that dementia caregivers provide an average of 64.5 h of care per week at the end of life, nearly twice the time spent by those caring for patients with cancer. This intensive involvement suggests that caregivers can offer valuable insights into the provision of hospice for persons with dementia.
In the dementia literature, previous reviews synthesized evidence surrounding advanced care planning and caregivers’ hospice experiences.18,19 Regarding potential transitions to hospice, Murali et al. 20 recently reviewed the predictors and interventions facilitating these transitional processes for persons with dementia. However, despite the crucial role of dementia caregivers at the end of life, no review has particularly focused on synthesizing the caregivers’ narratives, emotions, and attitudes as they consider or encounter hospice. Therefore, our research question was: What is the current evidence on caregiver-reported barriers and facilitators to hospice enrollment for persons with dementia? Conducting a qualitative systematic review can bring together caregivers’ lived experiences across different settings and contexts. 21 As such, we aimed to identify, evaluate, and synthesize qualitative evidence on what they reported as making it difficult or easier for persons with dementia to enter hospice.
Methods
This review adhered to the ENTREQ (enhancing transparency in reporting the synthesis of qualitative research) framework as a reporting guideline (Supplemental Table 1). 21
Search strategy and databases
We collaborated with an academic librarian at the University of Pennsylvania to determine the search databases and strategies. We included databases (i.e. PubMed, Cumulative Index to Nursing and Allied Health Literature (CINAHL), PsycINFO, Embase, and Scopus) that captured a broad range of scholarship from different disciplinary perspectives (e.g. biomedicine, psychology, nursing, global health). For the search, we combined terms related to dementia, caregiver, hospice, and qualitative data (Table 1). Keywords and controlled vocabulary, along with the synonyms and entry terms of the keywords defined by each database, were included. Because our focus was specifically on the end-of-life context, palliative care was not included in the search as it covers a broad scope of care regardless of the stage of a serious illness. Truncations were applied where appropriate. The list of terms was combined utilizing Boolean operators (AND, OR). We filtered the search by language (English) and article type (peer-reviewed journal where applicable). Since dementia-related policies, initiatives, and practices have significantly evolved throughout time worldwide,22 –24 we restricted the publication search to the past 15 years (2009–2024) to reflect the recent health and societal parameters. We conducted the search on May 9th, 2024.
Search strategies.
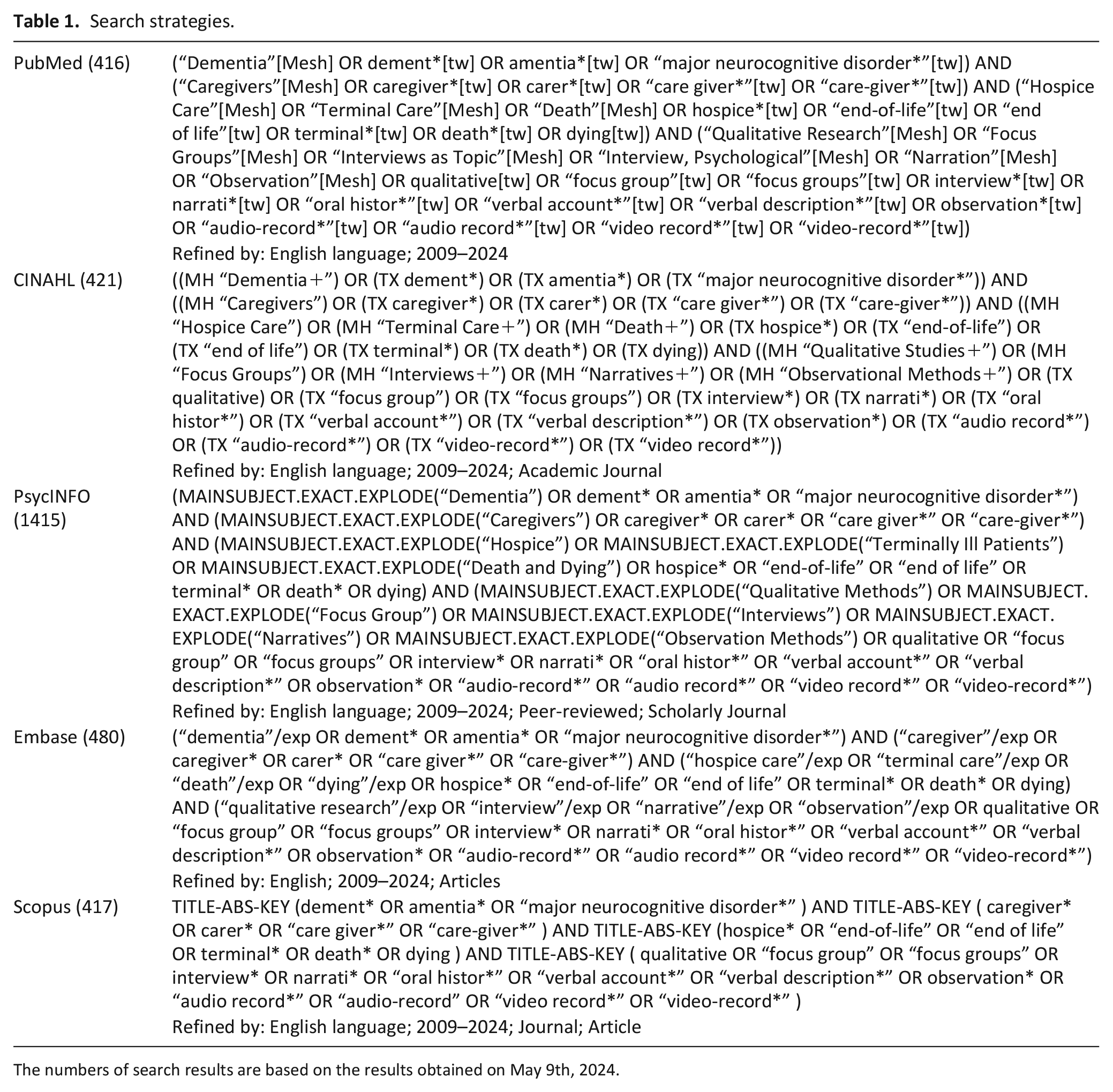
The numbers of search results are based on the results obtained on May 9th, 2024.
Study screening and selection
Articles were imported into Covidence for screening. 25 Based on our review’s eligibility criteria (Table 2), all titles and abstracts were screened by the first author (OO). Hospice enrollment was defined as the initial phase of entering hospice. We considered this term to be more specific than hospice utilization, which covers the entire hospice episode, or hospice access, which emphasizes the physical and environmental aspects of approaching hospice services. Caregiver-reported barriers and facilitators were defined as factors that caregivers perceive as making it either more difficult or easier for persons with dementia to enter hospice.
Eligibility criteria.
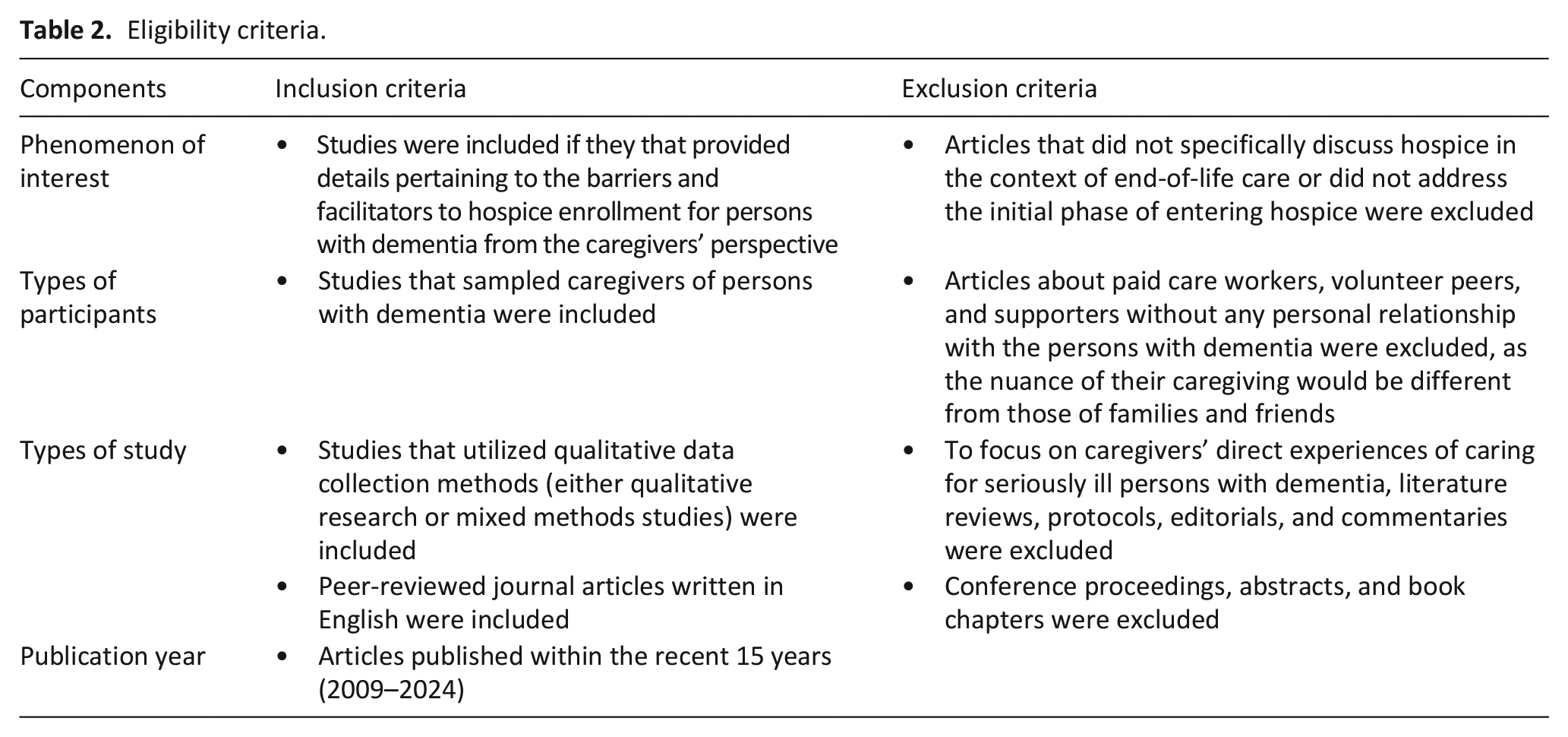
For abstracts that were considered potentially relevant, their full papers were retrieved. The first author (OO) reviewed the full text and, if there was uncertainty regarding a study’s eligibility, two authors (OO and GD) discussed it until reaching agreement. References from the included studies were also examined to identify additional articles that met our criteria but were not retrieved by the search strategy.
Quality appraisal
As we included both qualitative and mixed methods studies, we used the Mixed Methods Appraisal Tool to evaluate the overall methodological rigor. 26 This tool includes two screening and five design-specific questions. Considering each item and the overall impression of the article, its quality was categorized into high, moderate, and low. Quality appraisal was initially conducted by the first author (OO); coauthors reviewed the results. All articles were included in this review to gain a comprehensive understanding of our phenomenon of interest and ensure caregivers from diverse settings and contexts were represented. 27
Data extraction
From each study, the following data were extracted: geographic area (country), research study aspects (study aims, design, setting, and theoretical framework), methods (sampling procedures, data collection, and data analysis methods) as reported by the authors, sample characteristics, strategies to achieve trustworthiness, and key findings. Data were summarized into a table of evidence.
Data synthesis
Thematic synthesis was conducted to synthesize qualitative data. 28 Thematic synthesis is a primary method for synthesizing qualitative evidence 21 ; its advantages lie in its transparent steps and the closeness to the data. 28 Generated findings aim to directly inform future interventions, policies, and practice, 29 which aligns with the intended implications of this review.
Full texts of the included articles were uploaded into the ATLAS.ti software. 30 Data from each article’s results and Supplemental Materials (if relevant) were extracted for synthesis. Following the inductive approach described by Thomas and Harden, 28 the first author (OO) used line-by-line coding to generate in vivo codes for each relevant sentence. This included both participants’ quotes and the authors’ interpretation. The codes were then compared; new codes were created to capture collective meanings (descriptive themes). Finally, abstract themes were identified to infer barriers and facilitators to hospice enrollment (analytical themes). This was an iterative process through which the materials were revisited to ensure the codes sufficiently captured their content and that the analytical themes were abstract enough to offer practical implications. 28 Two authors (OO and GD) regularly met to refine codes and themes. We also engaged in peer debriefing including other coauthors (CMU and LM). Given the qualitative nature of our review, we documented a reflexivity statement to assess how our backgrounds may impact the meaning-making process of this synthesis (Supplemental Table 2).
Results
The search strategy yielded 3149 articles (Figure 1). After removing duplicates, 1917 remained. The full text was reviewed for 150 studies, where 22 were eligible. Their references did not add any additional eligible articles.
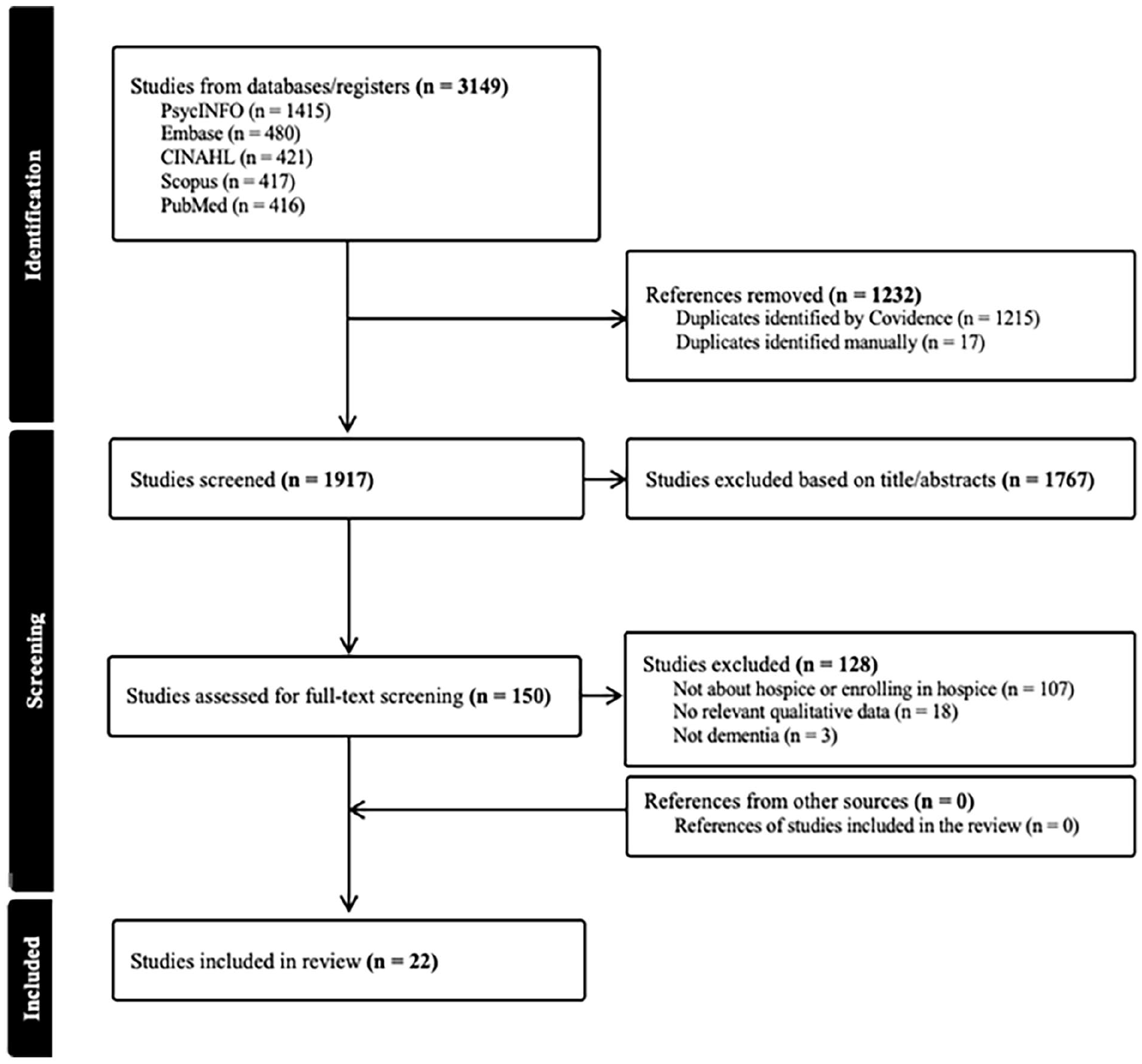
Literature screening process.
Study characteristics
Of the 22 articles, 16 were from the United States31 –46 and three were from the United Kingdom (Table 3).47 –49 The remaining 3 were from the Netherlands, 10 Israel, 50 and Germany. 51 Eighteen studies were qualitative,31 –35,37 –42,44,45,47 –51 and four were classified as mixed methods studies10,36,43,46; the number of caregivers in each study’s qualitative data ranged from 4 34 to 85. 51 Eight studies recruited samples from community settings,10,32,33,35,38,48,50,51 while others utilized various settings combined (n = 8),34,37,40 –42,46,47,49 outpatient (n = 3),31,36,43 and inpatient settings (n = 1). 39 Five articles focused on a specific diagnosis: Lewy body dementia (n = 2),32,33 sporadic Creutzfeldt-Jakob disease (n = 2),36,43 and Alzheimer’s disease and/or Parkinson’s disease (n = 1). 42
Table of evidence.
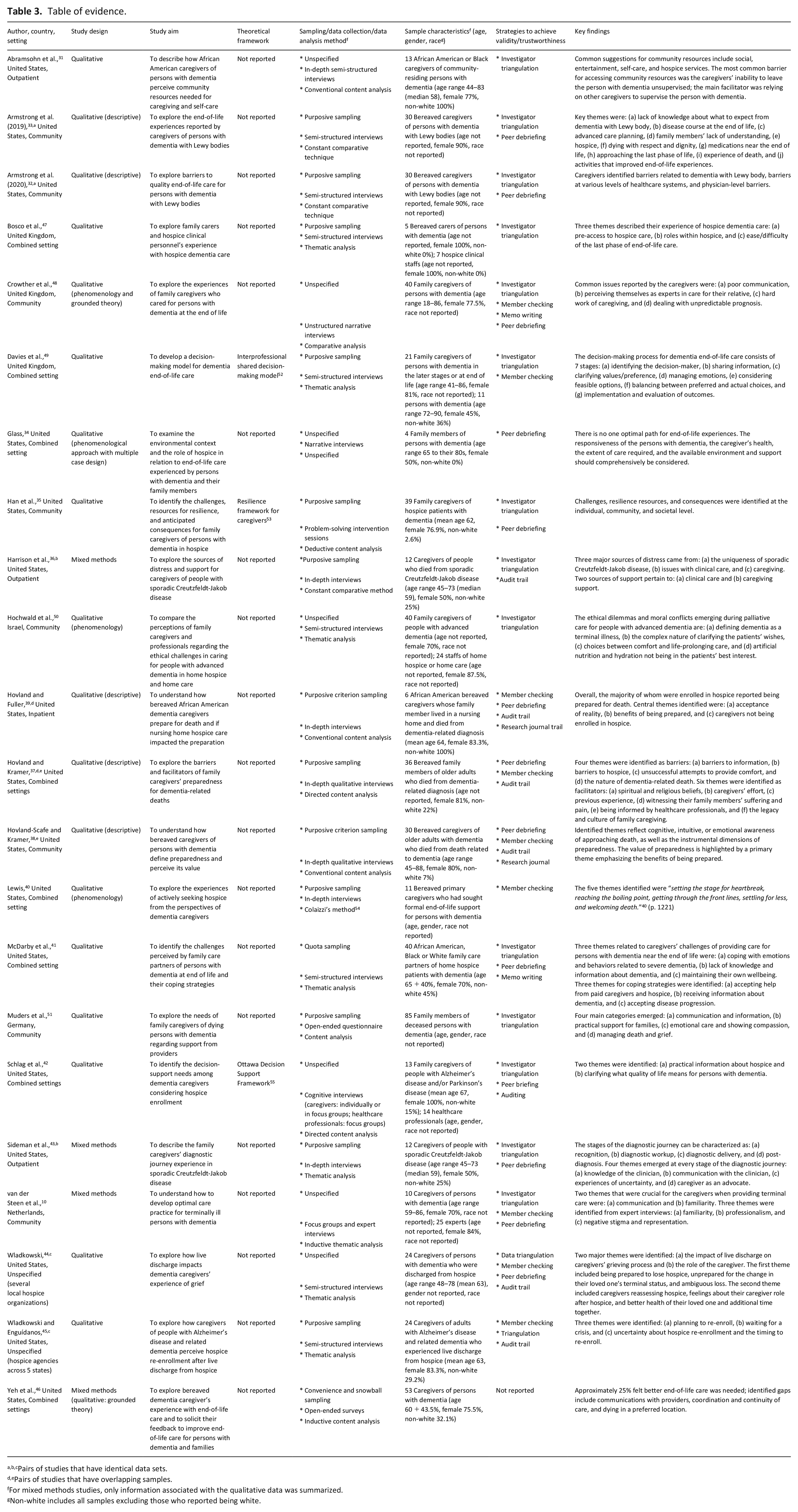
Pairs of studies that have identical data sets.
Pairs of studies that have overlapping samples.
For mixed methods studies, only information associated with the qualitative data was summarized.
Non-white includes all samples excluding those who reported being white.
Ten articles reported specific approaches: qualitative descriptive (n = 5),32,33,37 –39 phenomenology (n = 3),34,40,50 and grounded theory (n = 1). 46 Crowther et al. 48 reported adopting both phenomenology and grounded theory. Three studies used a theoretical framework,35,42,49 including the interprofessional shared decision-making model, 52 resilience framework for caregivers, 53 and the Ottawa Decision Support framework. 55 Approximately half (n = 9) reported using semi-structured interviews to collect data.31 –33,41,44,45,47,49,50 For data analysis, the majority used either thematic analysis (n = 8)10,41,43 –45,47,49,50 or content analysis (n = 8).31,35,37 –39,42,46,51 Investigator triangulation (n = 14)10,31 –33,35,36,41 –43,47 –51 and peer debriefing (n = 13)10,32 –35,37 –39,41 –44,48 were most commonly used to achieve trustworthiness.
Methodological quality
Most studies were high quality, with two studies rated as moderate,37,48 and four as low quality (Supplemental Tables 3 and 4).34,36,43,46 Ten studies did not specifically state their approach and only referred to their study as qualitative.10,31,35,41,42,44,45,47,49,51 Nonetheless, articles were deemed high quality if they provided sufficient details about data collection and analysis methods and offered quotes to justify themes, showing a coherent link between the collected data, analysis, and interpretation. 21 Moderate-quality articles either reported the use of directed content analysis without presenting a theoretical framework or theory to guide the initial coding scheme 37 or described the use of grounded theory but did not generate any theories from the data. 48 Reasons for risk of bias in the low-quality articles included: (a) showing no integration between qualitative and quantitative components, resulting in the study being a multi-method study instead of mixed methods,36,43,46 and (b) not providing any details on how the qualitative data were coded and analyzed. 34
Synthesis of findings
Thematic synthesis yielded 647 codes, which were grouped into 26 descriptive themes comprising 15 barriers and 11 facilitators (Supplemental Table 5); five analytic themes emerged. We mapped these five themes onto our key concepts: caregivers, persons with dementia, and hospice (Figure 2).
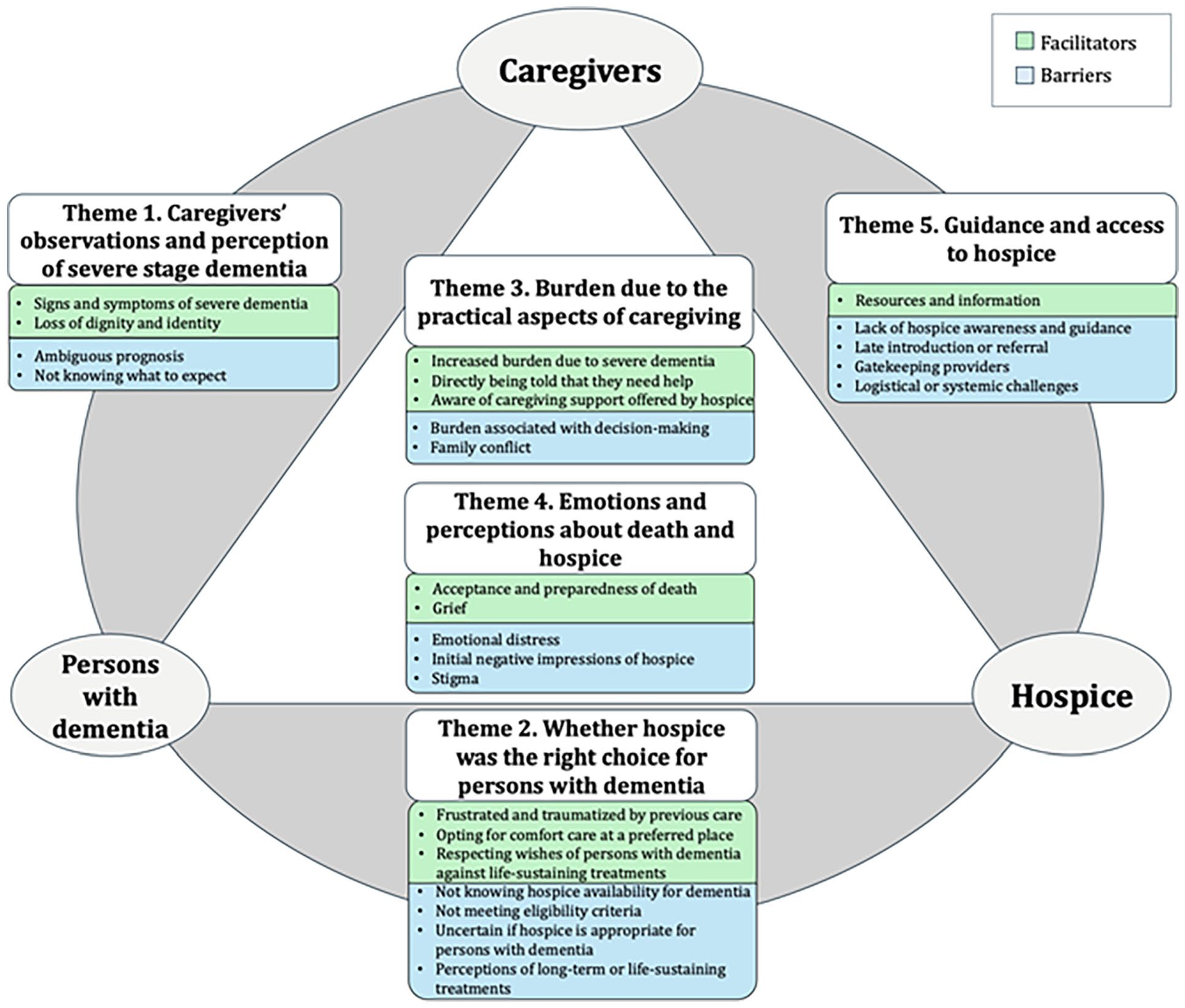
Themes and subthemes regarding caregiver-reported barriers and facilitators to hospice enrollment for persons with dementia.
Theme 1. Caregivers’ observations and perception of severe stage dementia
Specific aspects of severe dementia, as perceived and observed by the caregivers, impacted their pursuit of hospice.32 –35,37,40 –47,50 Two facilitators and two barriers were identified.
The first facilitator encompassed the signs and symptoms of severe dementia that prompted caregivers to recognize the approaching death of the person with dementia and the need for hospice. These included: being bed-bound and unable to perform independent activities,34,40,44,45 unsafe behaviors,40,41,47 difficulty swallowing or breathing,34,40 loss of appetite and speech,37,40,41 changes in mentality,34,40 use of catheter and stool incontinence, 34 clammy skin, 37 sleeping a lot, 37 and increased risk of pneumonia. 34 The second facilitator was caregivers perceiving the individual as losing dignity and identity. During this phase of progressive health deterioration, caregivers reported that their loved ones were “disappearing slowly” 37 (p. 68) and some refused to believe that the person was still their loved one. 50 They also described this stage as “a body lying there” 44 (p. 54) with “no real joy, really, in anything anymore” 40 (p. 1225) and being “worthless, empty, full of suffering and pain.” 50 (p. 1235)
However, the ambiguous prognosis of dementia was a main barrier to hospice enrollment.32,34,35,37,42,44,45 One caregiver described end of life as a “murky term” for persons with dementia: “I view hospice as end-of-life care. But what constitutes end of life? Certainly my mother’s at the end of her life, but how long are you going to drag this out for?” 44 (p. 56) Such ambiguity was also found among those without clear signs of death37,42,45: “you would have never even have had any indication that she was going to die . . . laying in the bed together sharing a salad, and siiinnggging. . .I thought for sure when I left the hospital . . . I was going to bring her home the next morning.” 37 (p. 64)
The second barrier was about caregivers lacking understanding of dementia’s end-of-life progression, not knowing what to expect.32,33,37,40,42,46 Many were unsure how close the end of life was,32,33,37,40,42 with some not believing that dementia can be terminal. 40 They often reported having no end-of-life conversation with providers,32,33,37,42,46 leaving them uncertain what to do next.32,42,46 End of life had to be clearly explained 46 : “Probably at least addressing and saying that, you know, this is terminal, and these are the types of things that we have to talk about or think about.” 33 (p. 4) One caregiver who cared for her mother and sister wished for guidance on the course of dementia before imminent death to “already know what’s next.” 42 (p. 816) Interestingly, for rapidly progressing disorders such as sporadic Creutzfeldt-Jakob disease, receiving the diagnosis itself enabled caregivers to receive information about hospice. 43
Theme 2. Whether hospice was the right choice for persons with dementia
Caregivers considered the fit between persons with dementia and hospice,32 –38,40 –42,44,45,47,50,51 revealing three facilitators and four barriers. The first facilitator was caregivers being frustrated or traumatized by their loved ones’ care, ranging from long-term care to aggressive life-sustaining treatments.32,34,38,40,44,47,50 They felt the hospital was not a caring place that met end-of-life needs and resisted hospitalization: “[My sister] called the doctor and said, ‘what can we do to have my mother never go to the hospital again?’” 40 (p. 1227) Some caregivers worried that their loved ones were humiliated being institutionalized40,44: “if she could see herself, she would be mortified.” 40 (p. 1225) This led to the second facilitator, which was opting for comfort and wanting their loved one to die at a preferred place34,40,42,44,47,50: “So, every meal he would get a white pile, a green pile, and a brown pile. So one day he said to me, ‘Boy, I sure wish I could have toast again!. . .’ And I just said, ‘You know, I don’t care! Give him toast! This is crazy the way we are treating him.’” 40 (p. 1226)
The third facilitator was caregivers wanting to respect their loved ones’ wishes against life-prolonging treatment: “We knew that she wanted to stay at home for as long as possible, she didn’t really want to be in a nursing home and she had agreed to a do not resuscitate form when the GP had spoken to her about that.” 47 (p. 8) These caregivers knew their loved one’s preferences for end-of-life care before dementia progressed to the point where they could not communicate. Advanced care planning, advanced directives, or previous discussions facilitated such awareness and ensured that the decisions aligned with the patients’ preferences.40,47
In contrast, not being aware that hospice is available for persons with dementia served as a barrier.35,40,47 For instance, a caregiver caring for their mother-in-law mentioned, “For the last- just under a year of her life, she had to go into a care facility nursing home because she wasn’t safe to be on her own. . .and I never realized that the hospice actually took patients that had dementia.” 47 (p. 9) When considering end-of-life care for persons with dementia, caregivers wanted to better understand dementia, its progression and symptoms, the functional and physiological changes near death, when to consider hospice for persons with dementia, dementia-related care that would be discontinued in hospice, and the meaning of quality of life in dementia.37,41,42,51
Not meeting hospice eligibility was the second barrier among caregivers who sought hospice.32,36,37,40,44,45,47 Reasons included not meeting “all of the criteria,” 32 (p. 733) “could still feed herself,” 37 (p. 63) and “wasn’t in the dying phase.” 47 (p. 7) One caregiver whose doctor declined to certify their mother for hospice reported: “there’s really nothing wrong with her. . .I mean she’s been at 72, 70 [pounds] for like over a year. . . She doesn’t have any particularly life-threatening issues.” 45 (p. 1376) Many also did not understand why their loved one was not qualified for hospice.32,40,44 Caregivers of people with sporadic Creutzfeldt-Jakob disease reported that, in some cases, hospice delayed enrollment as they did not understand how rapidly their loved ones’ condition would deteriorate. 36 Among those who eventually did enter hospice, many complained about the waiting periods and repeated rejections.32,44 A husband who cared for his wife for 5 years felt that the eligibility period for hospice was inadequate: “six months [for hospice], I think was the term she used and I’ve heard some people say three months and that certainly is not adequate. It should be longer.” 34 (p. 32)
The third barrier was the caregivers’ uncertainty regarding whether hospice is the right care model for persons with dementia. Such uncertainty was more evident among those who had experienced hospice discharge, thus being skeptical about the utility of hospice if they cannot maintain eligibility.44,45 These caregivers wanted to wait for a clear indication of “fall[ing] off another cliff.” 45 (p. 1377) to consider hospice enrollment: “I think we have to initiate it [hospice] if we see that there’s a degradation in his quality of life, or some event. It will be a 911 call that probably means that he could be in hospice, which is sort of silly, but that’s what it’s going to have to take.” 45 (p. 1376) Conflicted feelings toward hospice was described as, “wanting support, but not too much support that would improve the individual’s condition.” 44 (p. 56)
The final barrier was caregivers’ perceptions of long-term or life-sustaining treatment.32,33,42,50 Some caregivers believed that quality of life would be maintained through high-quality usual care that integrates symptom management and extends longevity. 42 Caregivers wanted to “keep him alive” 50 (p. 1234) and “keep their brain going as much as they can.” 33 (p. 8) Some were concerned that discontinuing medications for comorbidities may increase their loved one’s suffering. 42 Religious caregivers expressed having no control over withdrawing current treatment: “it is not for us to decide.” 50 (p. 1235)
Theme 3. Burden due to the practical aspects of caregiving
The practical burden of end-of-life caregiving had a profound impact on hospice enrollment,10,32 –36,40,42,45,47,50 shaping three facilitators and two barriers. Increased caregiving burden itself was a key facilitator40,42,45: “her physical needs definitely increased. . .the psychosocial and spiritual. . .needs all increased as she became kind of sicker.” 45 (p. 1377) Financial burden was also described as “horrendous.” 40 (p. 1225) during this stage. The second facilitator was being directly told by others that they needed more help and should consider hospice.32,34,36 One caregiver reported that, after recurrent visits to the emergency room, one doctor sat with them and said, “You’ve got to bring in a team. There is such a thing called hospice.” 36 (p. 32) The third facilitator was caregivers understanding practical and financial benefits hospice could offer to the caregivers.32,42 One female caregiver, who cared for her mother with her sister, described caregiver support as “the differences in choosing just the usual care vs the hospice.” 42 (p. 817)
However, burdensome end-of-life decision-making was a barrier preventing persons with dementia from entering hospice sooner.32,33,35,40,42,47,50 Caregivers often had to make quick decisions,32,42 feeling overwhelmed and fatigued to remember all the information.32,33,42,47 Even in situations where families had pre-planned end-of-life care, they reported feeling a sense of “spiraling out of control.” 40 (p. 1227) Some caregivers even avoided confronting the dilemma between life-prolonging care and comfort care. 50 Family conflicts were the second barrier,32 –34,40,42 which involved other family members being against hospice, in denial, or lacking understanding of their loved one’s condition.32 –34
Theme 4. Emotions and perceptions about death and hospice
Caregivers’ feelings and perceptions regarding the potential death of persons with dementia and hospice heavily influenced hospice enrollment.31 –34,36,37,39 –41,44 –47,49,50 Two facilitators and four barriers were identified.
A key facilitator was caregivers accepting that “the end is near” 45 (p. 1377) and being prepared.34,39,40,45 A 76-year-old caregiver who cared for her sibling for 5 years reported, “I think once he started going down and I could see it, he was gonna die. I knew it. . .” 39 (p. 137) Even when the caregivers knew that their decisions may result in their loved ones’ death, they felt that they would have to “live with that” 40 (p. 1226) and “be firm in the choice.” 47 (p. 11) The second emotion-related facilitator was grief. Caregivers quoted “I’ve said goodbye many years ago,” 50 (p. 1235) and “I know my wife is gone now, but she’s still here.” 34 (p. 34) Caregivers anticipated that enrolling in hospice would give them time to “grieve together as a family.” 44 (p. 54)
In contrast, emotional distress, such as being in denial, not being ready, fear, and guilt, served as a barrier delaying hospice enrollment.32 –34,37,39,40,44 –46,49,50 One 74-year-old spouse caregiver reported: “While we was getting ready to do hospice, but I was still praying on it, I hadn’t signed any papers yet. . .he was going to go through it, and we was going to talk about it more. . .I was in denial to believe that he was dying.” 39 (p. 139) These emotions were evident even when their loved one was “in front of you laying in a hospital bed, unable to walk anymore” 40 (p. 1226) and “ha[d] no dignified quality of life.” 44 (p. 53) Some were afraid of hospice resulting in their loved ones’ death 33 : “The fear of losing him is the hardest thing, nothing else is difficult. . . and I’ll do everything in my capability to keep him alive.” 50 (p. 1235) Others feared upsetting their loved one by bringing up hospice, as the individual either did not prefer or was afraid of hospice.32,33,49 Guilt was described as “You feel like you’re killing her by not taking her to the hospital, because that’s just your natural reaction is you want to save somebody.” 40 (p. 1227)
Initial negative impressions of hospice were also a barrier.32,36 For instance, a caregiver stated, “I wasn’t pleased with the intake person. It—I really didn’t get any sense of, uh, compassion or sincerity,” 32 (suppl 3) and decided not to pursue hospice. Another caregiver was frustrated with the hospice organization’s lack of understanding of sporadic Creutzfeldt-Jakob disease, resulting in switching institutions. 36
Finally, stigma was a key barrier—associated with both hospice itself and accepting help from others.31 –33,41,45 Some perceived hospice as a place “where a person goes to die,” 41 (p. 1791) associating it with “hate,” 31 (p. 5) being “cruel,” 32 (suppl 3) and “false sense of her end.” 45 (p. 1378) A 62-year-old female caregiver stated, “I didn’t want them to think that I didn’t want to take care of my mom.” 41 (p. 1790)
Theme 5. Guidance and access to hospice
The final theme relates to caregivers’ experience with receiving guidance and access to hospice10,31 –34,36 –43,45 –48,51; one facilitator and four barriers were identified. Many resources, including the internet,33,37,41 print materials,33,40 books,33,37 support communities,36,43 information seminars, 37 movies, 37 daycare centers, 47 and clinics, 36 acted as facilitators that helped caregivers learn about hospice and death in dementia. Caregivers also heard about hospice or received support from family friends, both with or without medical expertise,34,37,40,41 as well as healthcare professionals (e.g. doctors, nurses, social workers) and ancillary staff.33,36,37,39 –41,43,45 Some referred to their past experiences with death or dementia to guide their decision-making.37,41,42 Information about hospice that was or would have been useful included: services offered by hospice, both in general and outpatient-specific; its flow and medications; financial costs and insurance coverage; the appropriate timing for considering enrollment; and the possibility of re-enrollment.31 –33,42,45,46,51 Physicians or social workers using specific scenarios to illustrate the optimal timing for hospice,34,36 along with having other medical team members validate the patients’ current medical condition, 33 were also reported to be helpful.
Nevertheless, not knowing what hospice was or that it was an option for their loved one was a major barrier31 –33,40,46,47: “Nobody mentioned the word hospice. Nobody ever said it would be a good idea to look into that now too.” 32 (p. 734) Even when some caregivers expressed concerns about life-prolonging care, they were not informed about other alternatives. 40 Caregivers also noted that physicians and nurses themselves sometimes lacked hospice awareness.32,33,40 Many did not receive sufficient guidance,32,33,36,40,42,46 with caregivers saying that they were “‘self-navigating’ through the medical system” 40 (p. 1227) without having “anyone to reach out to” 42 (p. 817) and feeling “abandoned” 36 (p. 27): “When I talked with Hospice she just said to me, ‘You need to make that decision soon and it’s up—you know, we can’t help you with that.’” 32 (suppl 3) Misconceptions about hospice were also reported—believing that hospice and visiting nurses are the same, 32 or assuming that one must live at home to qualify for hospice. 40
Late introduction or referral to hospice was the second barrier,32,33,37,38,40,51 with many reporting that hospice was mentioned days or a few weeks before death37,38,40: “hopefully they would have been able to provide some. . . stuff. . .but they didn’t have a chance to do it. . . they should have brought in hospice for me earlier. . .” 37 (p. 63)
Gatekeeping healthcare professionals were also a common barrier.32,33,37,40,43,47,48 Even though caregivers “begged them to get her to the hospice several times,” 47 (p. 7) they felt that “they [physicians] really didn’t listen.” 40 (p. 1226) One caregiver continuously asked to be referred to a specialty clinic but was refused: “It wouldn’t have changed the diagnosis, but it would have changed his end of life in terms of how we would have had conversations and knowing where we were headed.” 43 (p. 287) Some doctors, neurologists, nurses, and nursing home staffs did not recommend hospice,32,33,37,40 believing it was too early: “I think they thought I was giving up on him or I didn’t want to give him a chance.” 37 (p. 63)
Logistical or systemic challenges in accessing hospice emerged as the final barrier.10,32,36 –38,46,47,51 Logistical issues included hospitals being the default option in emergencies (e.g. falls) 47 or situations requiring physical transfers to access hospice. 10 System-related obstacles included a shortage of available beds, 47 inability to consult hospice staff, 32 lack of access to outpatient hospice services, 51 absence of opportunities to document advanced directives, 36 or transfers being delayed.32,37,38 Poor care coordination also delayed hospice enrollment,32,46 such as having a “mix-up at the doctor’s office.” 32 (supp1 3)
Discussion
Main findings
Five themes identified from this thematic synthesis emphasize an interplay among caregivers, persons with dementia, and hospice. Hence, involving hospice to provide quality end-of-life care for persons with dementia entails the need to adopt a dementia-specific lens to hospice entry and acknowledge the crucial role dementia caregivers play near death.
In hospice, terminal stage is often defined as having a life expectancy of 6 months or less. 13 However, as persons with dementia are often referred to hospice very late,37,38,40 identifying potential hospice candidates based on time-based prognoses may not be practical for this population. It also does not align with how dementia caregivers recognized terminality in their loved ones. Many felt they had already lost their loved one due to severe symptoms of dementia,37,40 experiencing pre-death grief.34,50 Dignity was perceived to be lost and many caregivers felt that their loved one would rather benefit from comfort care.40,44 Nonetheless, the ambiguous end-of-life trajectory of dementia functioned as a barrier to hospice entry. Hospice models operating under strict eligibility criteria like the United States did not deem certain individuals as terminal.32,36 In other healthcare systems, such as the United Kingdom, where provider referrals were vital for entering hospice, some consultants did not recognize the patient as being in the dying phase, even when they eventually passed away a few days later. 47 There are indeed measurements used to help assess end of life in dementia, such as the Functional Assessment Staging Scale, which is used to determine hospice eligibility in the United States, 13 or the Clinical Frailty Scale, which is often used in the United Kingdom or Canada to predict mortality. 56 Nonetheless, Browne et al. 57 highlighted limitations of these tools in capturing the complexities across end-of-life trajectories in dementia. Hospice care models—whether driven by strict admission criteria or providers’ referrals—substantially focusing on time-based prognoses can create a discrepancy between the needs of dementia caregivers and the actual circumstances under which hospice can be offered.
We also found that healthcare providers, including physicians, nurses, and social workers, acted as both facilitators and barriers to hospice enrollment. In some cases, they informed caregivers about such services and guided them through decision-making processes. 36 In other cases, they declined to certify the person with dementia without clear explanation or did not recommend hospice,32,37 sometimes resulting in caregivers feeling ignored. 40 There were clearly circumstances where policy, financial, or practical realities constrained providers from making hospice available. For instance, if hospice is provided in a separate unit, some providers might have deemed the patient too ill to survive the transport. 48 When hospice is heavily supported by charitable donations like the United Kingdom, lack of funding may impact bed availability. 47 In addition to these real-world limitations, inconsistencies in how providers assessed end of life in dementia stem from the unpredictable and/or long-lasting nature of dementia-related symptoms and uncertain timing of hospice referrals. Instead of solely focusing on the disease characteristics, need-based approaches incorporating regular assessments of the caregivers’ burden and their openness to palliative approaches could be beneficial. In our included studies, dementia caregivers reported increased burden near death due to their loved ones’ severe condition.42,45 Yet, we found that engaging in conversations about their situations enabled healthcare professionals to identify unmet needs and explore available resources like hospice. 36 Hence, this additional attention to families’ needs by the providers could help hospice entry be better tailored for persons with dementia.
For caregivers living with persons with dementia, alleviating burden associated with constant caregiving was a clear benefit. 42 Nonetheless, the ambiguous end-of-life trajectory of dementia sometimes led to others wanting to wait for their loved ones to begin experiencing health crises or acute episodes before they would start considering hospice. 45 This highlights that hospice decision-making in the dementia context is often reactive in nature. In many cases, the decision-making process also resulted in moral dilemmas, such as debating between longevity-focused care and comfort or pursuing hospice despite their loved one being afraid of it. This left caregivers unable to decide or delaying enrollment.32,50 Previous reviews have documented caregivers’ difficulties in making decisions on behalf of persons with dementia,58,59 and our study findings add to these challenges. Such findings urge the need for strategies to help dementia caregivers navigate end-of-life decision-making, often shaped by reactive choices during critical moments and intertwined with moral uncertainty. Proactive approaches, such as advanced directives or early end-of-life discussions with their loved ones, were reported to be helpful.40,47 Hence, involving patients in these discussions early in the disease trajectory, either actively or passively, may alleviate some caregiver burden associated with end-of-life decision-making.
Many caregivers were dissatisfied with their loved ones’ hospitalization, feeling that standard care did not meet end-of-life needs and only provoked trauma.38,40,44 Even so, some still wanted to maintain treatment for non-dementia comorbidities or dementia-related care unavailable in hospice.32,42 Wishes against hospice and palliative approaches should also be respected; yet we also found the need to examine more closely whether such resistance to hospice is based on an informed decision. For instance, some caregivers perceived negative stigma or held misconceptions about hospice,32,41 while others demonstrated negative initial impressions toward hospice that deterred them from pursuing it. 32 Such findings highlight the need to ensure that caregivers’ decisions about end-of-life care are well-informed and not influenced by stigma, misconceptions, or generalized beliefs.
We also identified an ongoing need to address the lack of awareness regarding hospice being available for persons with dementia.35,47 Caregivers learned about hospice not only from providers but also from the internet, daycare centers, seminars, and pamphlets.33,37,40,47 Other previous studies have similarly demonstrated the potential of utilizing social media and online support groups to promote public health knowledge.60,61 Organizations and systems can leverage these informal channels to disseminate knowledge on the terminal nature of dementia and its hospice eligibility, which could be more accessible and convenient to caregivers.
Finally, many persons with dementia receive care in nursing homes or long-term care facilities. 62 Yet, few of our included studies recruited from these settings.39,42 In cases where hospice is provided in a separate specialized unit within a nursing home requiring patient transfer, van der Steen et al. reported that the familiar environment with on-site care and established relationships with the staff led caregivers to question the need for such a transfer. The authors ultimately suggested integrating palliative approaches into regular nursing home units by training mobile teams with expertise in both dementia and palliative care. 10 However, in other healthcare contexts, such as the United States, where hospice is not restricted to certain settings, 7 it is still underutilized among nursing home residents with dementia. 63 Further research is needed to understand whether hospice transitions are supported differently when they occur within the same setting, compared to those that involve physical transfers, such as across different inpatient units or from hospitals to home.
What this study adds
There are cross-national variations in the hospice care models, whether they operate under strict eligibility criteria or depend heavily on providers’ referrals. Yet, possibly stemming from the lack of financial and workforce resources, the models commonly focus on time-based terminality and clinical prognosis. For dementia caregivers, this creates a gap between their perception of end-of-life caregiving for severe dementia and the practical reality for receiving resources that could alleviate their burden and offer comfort to their loved one. Applying a dementia-specific lens to the hospice entry phase, while considering caregivers’ needs and openness to palliative approaches, would be beneficial. Moreover, hospice discussions were often reactive, prompted by health crises in persons with dementia. Understanding the unique context that leads to hospice transition during these critical moments would add further insights into facilitating hospice entry for this population. Finally, since challenges may still arise post hospice entry, understanding how dementia caregivers describe their transition to hospice could help identify actionable support that can facilitate the shift to end-of-life care.
Strengths and limitations
To our knowledge, this is the first study to synthesize qualitative findings to understand what influences hospice entry for persons with dementia from caregivers’ perspectives. We generated dementia-specific themes, highlighting the uniqueness of dementia in hospice. However, due to resource constraints, there are some limitations impacting our methodological rigor, such as the absence of a pre-registered review protocol and the involvement of a single author in the literature screening and quality appraisal. We also excluded gray literature, including dissertations and conference proceedings, which could have added insights to our review. Furthermore, we did not exclude articles that were appraised as low quality, which may introduce bias. 64 Finally, the coding was initially conducted by one author and further refined through discussions with coauthors. While this method has been used in previous qualitative syntheses,58,65,66 additional insights might have been missed.
Conclusion
Caregivers play a pivotal role in managing care and advocating for persons with dementia toward the end of life. However, hospice for persons with dementia is often based on a time-limited prognosis, which may not fully reflect the complex nature of severe dementia and the caregivers’ needs. Tailoring hospice entry to better address the uniqueness of dementia requires ongoing discourse, but it will be imperative to improve end-of-life care for persons with dementia and their families.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163251353013 – Supplemental material for Caregiver-reported barriers and facilitators to hospice enrollment for persons with dementia: A systematic review of qualitative evidence
Supplemental material, sj-docx-1-pmj-10.1177_02692163251353013 for Caregiver-reported barriers and facilitators to hospice enrollment for persons with dementia: A systematic review of qualitative evidence by Oonjee Oh, Connie M Ulrich, Lauren Massimo and George Demiris in Palliative Medicine
Footnotes
Acknowledgements
We thank Carlos I. Rodriguez from Holman Biotech Commons at the University of Pennsylvania for his thorough and insightful consultation on the study’s search strategy.
Data sharing
The full search strategy for this review is available within the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics and consent
This study did not require ethical approval or informed consent as it involved only secondary analyses of published empirical data.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.