
Abstract
Background:
Advance care planning aims to ensure that care received during serious and chronic illness is consistent with the person’s values, preferences and goals. However, less than 40% of people with dementia undertake advance care planning internationally.
Aim:
This study aims to describe the perspectives of people with dementia and their carers on advance care planning and end-of-life care.
Design:
Systematic review and thematic synthesis of qualitative studies.
Data sources:
Electronic databases were searched from inception to July 2018.
Results:
From 84 studies involving 389 people with dementia and 1864 carers, five themes were identified: avoiding dehumanising treatment and care (remaining connected, delaying institutionalisation, rejecting the burdens of futile treatment); confronting emotionally difficult conversations (signifying death, unpreparedness to face impending cognitive decline, locked into a pathway); navigating existential tensions (accepting inevitable incapacity and death, fear of being responsible for cause of death, alleviating decisional responsibility); defining personal autonomy (struggling with unknown preferences, depending on carer advocacy, justifying treatments for health deteriorations); and lacking confidence in healthcare settings (distrusting clinicians’ mastery and knowledge, making uninformed choices, deprived of hospice access and support at end of life).
Conclusion:
People with dementia and their carers felt uncertain in making treatment decisions in the context of advance care planning and end-of-life care. Advance care planning strategies that attend to people’s uncertainty in decision-making may help to empower people with dementia and carers and strengthen person-centred care in this context.
Advance care planning (ACP) supports people to consider and communicate their current and future treatment goals. However, only up to 40% of people with dementia undertake ACP worldwide.
People with dementia receive sub-optimal care at end of life, including overly aggressive treatments, low rates of palliative care referrals and poor pain and symptom management.
People with dementia and their carers felt uncertain in making decisions in the context of ACP and end-of-life care.
People with dementia and their carers had to confront emotionally difficult conversations and navigate existential tensions during ACP; while also feeling a sense of distrust and a lack of confidence in the information and support available to them in healthcare settings.
Carers needed to overcome uncertainty if the person with dementia had not previously expressed their preferences; they felt adhering to the ACP preferences of the person with dementia would make them responsible for the person’s death; or they experienced disagreement with clinicians when advocating for the preferences of the person with dementia.
Health professionals who are involved in ACP and end-of-life care in dementia should demonstrate empathy and aim to facilitate acceptance of the inevitable cognitive decline and death in dementia and provide an understanding of the decisions that may need to be made along the trajectory of dementia.
Future ACP strategies should attend to potential uncertainties that may arise when carers are attempting to adhere to the person with dementia’s ACP preferences at end of life.
Introduction
The increasing prevalence of dementia is an international public health priority, affecting an estimated 47 million people globally, and is expected to nearly triple in prevalence by 2050. 1 Dementia is a progressive and terminal illness, characterised by impaired memory, thinking, reasoning and communication. For people with dementia, the ability to make decisions, plan for the future and perform daily self-care ultimately deteriorates as the disease progresses. 2 Because of this, caregiving for people with dementia can be emotionally challenging, particularly when facing decisions about the person’s future medical care,3,4 such as whether to consent to life-sustaining treatments. 5
Advance care planning (ACP) supports people to consider and communicate their future treatment preferences in the context of their own goals and values. It is an ongoing process in which a person may need to appoint a substitute decision-maker and document their preferences for care in an advance care directive or advance care plan. 6 The goal of ACP is to ensure that people receive treatment and care consistent with their goals, values and preferences during serious and chronic illness. 7 Yet ACP is estimated to occur with only 3%–39%8–10 of people with dementia internationally. People with dementia receive sub-optimal care at end of life, 11 including overly aggressive treatments, low palliative care referrals 12 and poor pain and symptom management. 13 Moreover, although people with dementia and their carers believe ACP is relevant to people with dementia and it should be completed early in the illness trajectory,14,15 they may not feel comfortable discussing ACP because of fear of future cognitive decline.16,17
Qualitative research methods are used to elicit the attitudes and beliefs of participants to generate in-depth and nuanced insight into their perspectives.18,19 A systematic review and synthesis of qualitative studies can bring together data across different populations and contexts, beyond a single primary study. This allows a more comprehensive understanding to inform clinical practice regarding ACP and end-of-life care in dementia that accords with their values and preferences.20,21 This study aims to describe the perspectives of people with dementia and their carers concerning ACP and end-of-life care in dementia, which may inform strategies that will maximise quality of care and quality of life outcomes in this vulnerable population.
Methods
We followed the Enhancing Transparency of Reporting the Synthesis of Qualitative Research (ENTREQ) framework 21 and used thematic synthesis as described by Thomas and Harden. 20 Thematic synthesis is used to formalise the identification and development of themes from multiple primary studies and subsequently enabled the development of a comprehensive conceptual framework for this study that can explain the experiences and perceptions of people with dementia and their carers.
Data sources and searches
The search strategies are provided in Supplementary Table S1. We searched MEDLINE, Embase, PsycINFO and CINAHL from database inception to 6 July 2018. Google Scholar, PubMed and reference lists of relevant articles were also searched. Two reviewers (M.S. and O.C.) independently screened the search results, initially by title and abstract, then the full texts of potentially relevant studies for eligibility. Studies that did not meet the inclusion criteria were excluded.
Selection criteria
Qualitative studies were eligible if they reported the experiences of people with dementia and carers and perspectives of ACP and end-of-life care in dementia. Study participants had to include adults aged 18 years or older diagnosed with dementia of any type or stage in the illness trajectory, and/or carers (i.e. family member, friend or other appointed substitute decision-maker) who provided unpaid care and support to a person with dementia. Studies across all care settings were eligible for inclusion. ACP was defined as any intervention aimed at supporting people to consider and communicate their current and future treatment goals in the context of their own preferences and values. End-of-life care was defined as any treatment or care around death or the dying process. Studies involving mixed methods (including surveys) or process evaluation that reported qualitative data were included if qualitative data could be extracted. Studies were excluded if they exclusively examined euthanasia or ‘assisted suicide’, or reported only quantitative data. We also excluded non-English articles to minimise misinterpretation of any linguistic and cultural nuances.
Quality assessment
We assessed each primary study for comprehensiveness of reporting, which can provide details for readers to assess the trustworthiness and transferability of study findings. We used an adapted consolidated criteria for reporting qualitative health research (COREQ) 22 framework, which included criteria specific to the research team, study methods, study setting, analysis and interpretations. Two reviewers (M.S. and O.C.) independently assessed each study and resolved discrepancies through discussion.
Data analysis
Consistent with thematic synthesis guidelines, 20 participant quotations and text under the results/findings or conclusion/discussion sections were imported for each article into HyperRESEARCH (ResearchWare Inc. version 3.7.5; 2015) software. One investigator (M.S.) performed line-by-line coding of the findings from studies generated by the database search, conceptualised the data and inductively identified concepts. Text was then coded into existing concepts or a new concept was created as required (M.S. and O.C). Similar concepts were grouped into themes and subthemes. Conceptual links among themes were identified (M.S. and O.C.) to extend the findings offered by the primary studies and develop an analytical thematic schema. To ensure that coding captured all relevant issues and reflected the primary data, researcher triangulation was used, in which two reviewers (M.S. and O.C.) independently reviewed the preliminary themes and analytical framework, and discussed the addition or revision of themes with all the authors.
Results
Literature search
From 2653 articles identified in the search, we included 81 articles involving at least 389 people with dementia and 1864 carers from 14 countries (Figure 1). Two studies did not report the number of participants. The age of people with dementia ranged from 46 to 95 years, while carers’ ages ranged from 18 to 95 years. The characteristics of the included studies are summarised in Table 1, with the details of each study provided in Supplementary Materials (Supplementary Table S2). The included studies were published from 1996 to 2018. Fifty (60%) studies reported the stage of dementia, with advanced stage being most commonly reported (75%). Of the 76 studies involving carers, 62 reported on the carer’s relationship to the person with dementia, which included spouse/partner (56 studies), child (57 studies), grandchild (9 studies), sibling (13 studies) and other (29 studies).
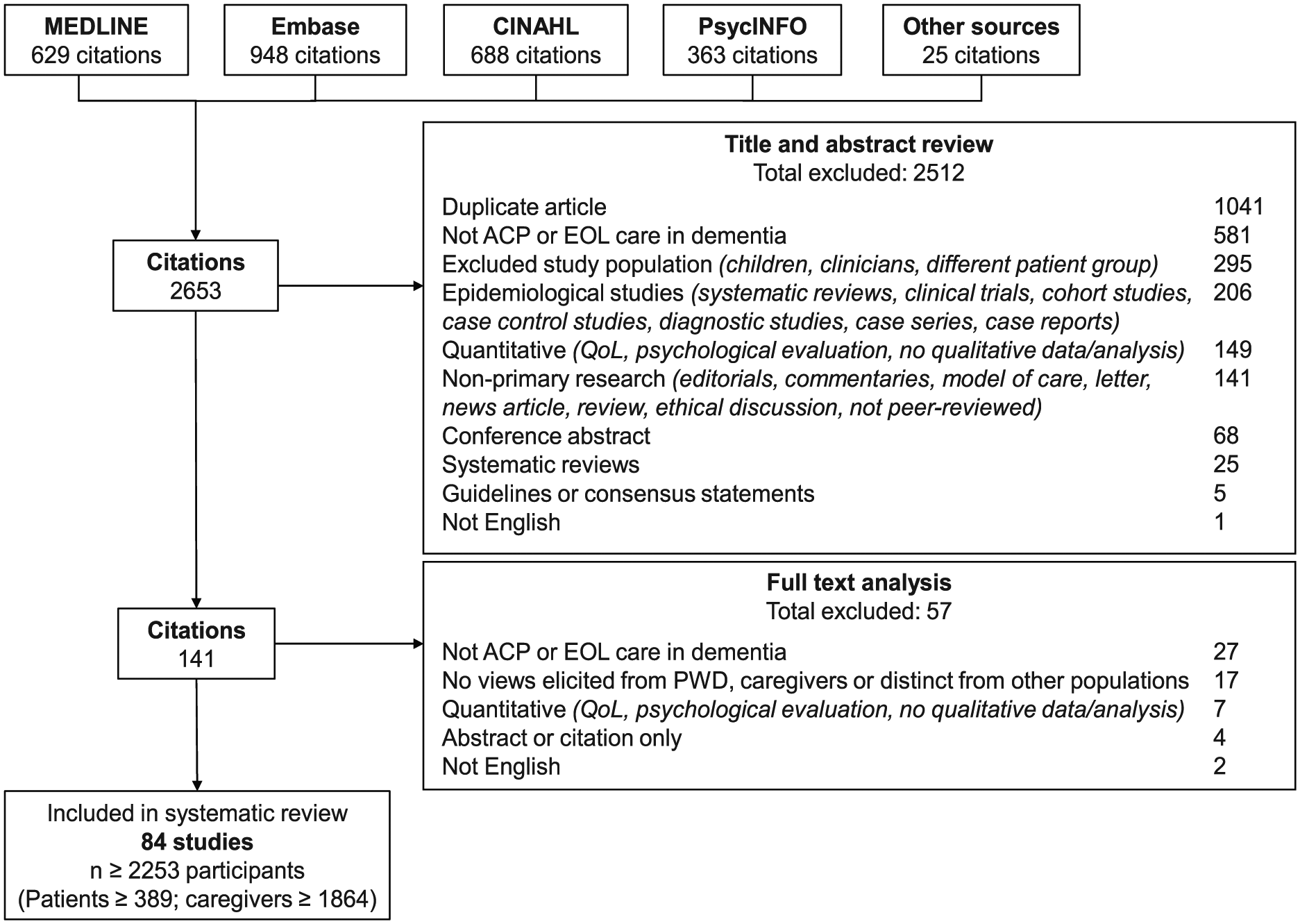
Search results.
Characteristics of included studies (N = 84).
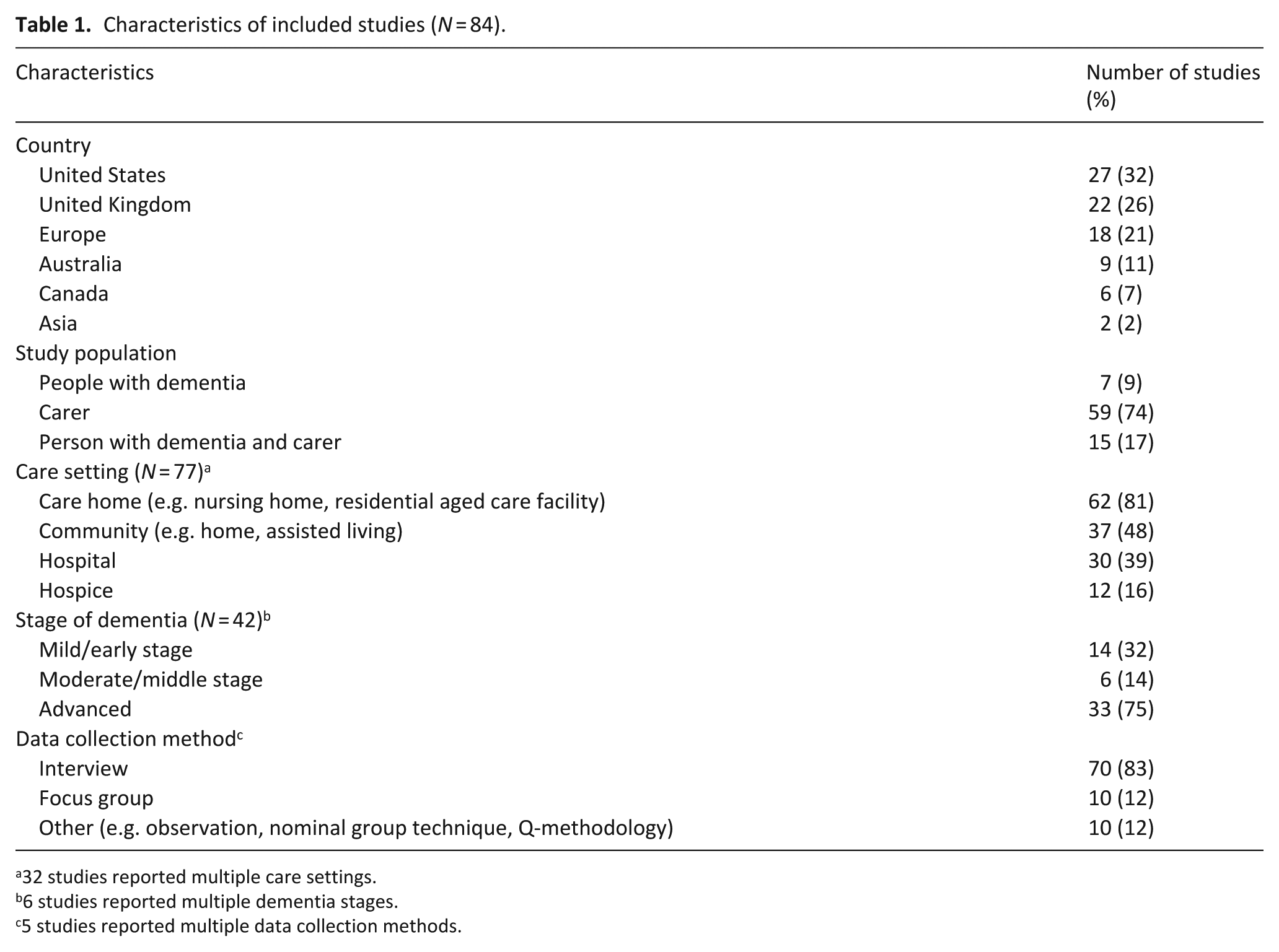
32 studies reported multiple care settings.
6 studies reported multiple dementia stages.
5 studies reported multiple data collection methods.
Comprehensiveness of reporting
The comprehensiveness of reporting was variable, with studies reporting 2 to 22 of the 34 items included in the framework for assessing the reporting of qualitative studies (Table 2). The sampling strategy was described in 53 (65%) studies. Theoretical or data saturation, 19 whereby subsequent data collection identified few or no novel concepts, was reported in 18 (22%) studies. Member checking, whereby participant feedback is obtained for preliminary findings, was reported in five (6%) studies, while the number of data coders (e.g. investigator triangulation used in data analysis) was reported in 57 (70%) of studies.
Comprehensiveness of reporting in included studies.
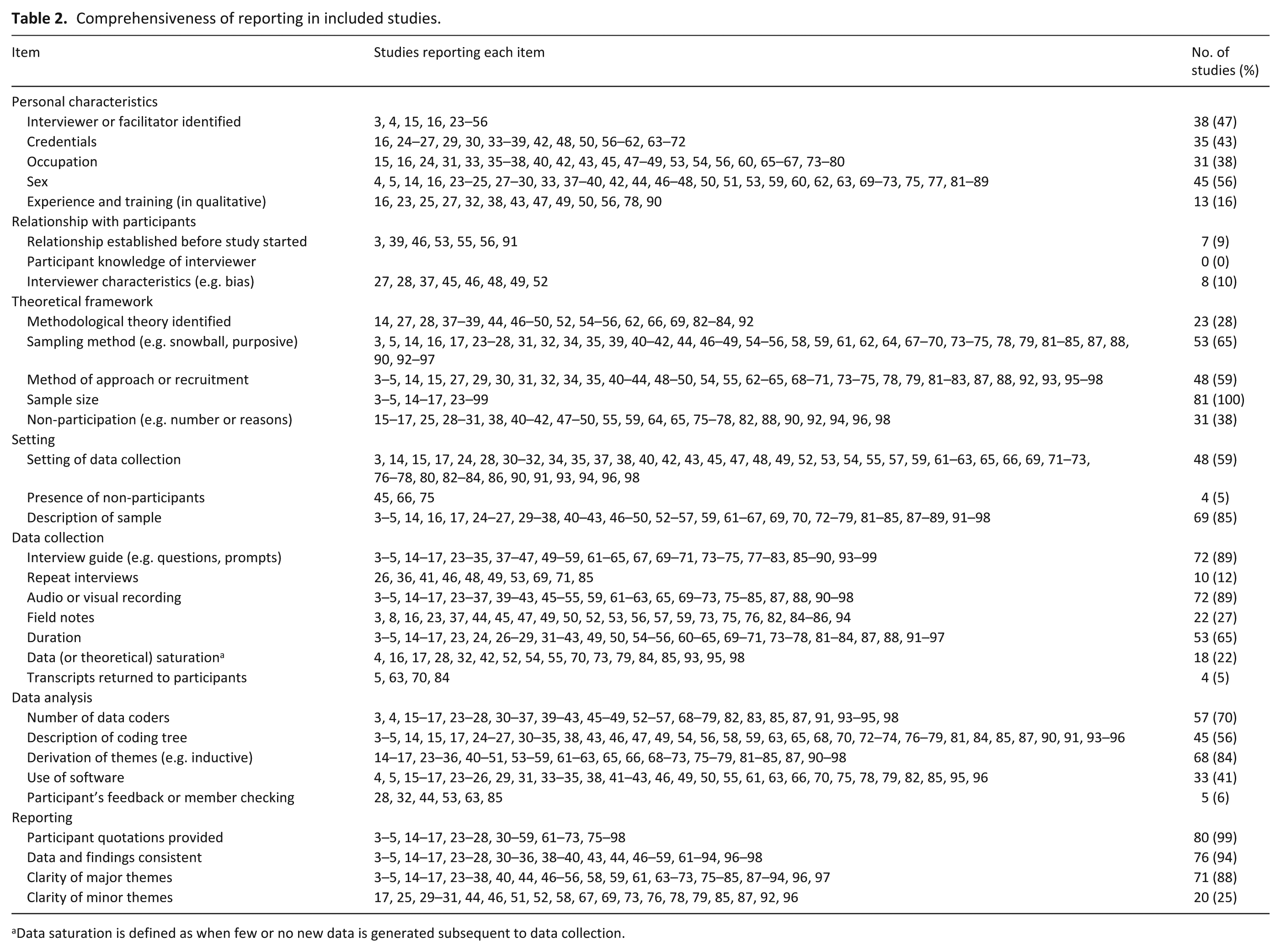
Data saturation is defined as when few or no new data is generated subsequent to data collection.
Synthesis
We identified five themes: avoiding dehumanising treatment and care, confronting emotionally difficult conversations, navigating existential tensions, defining personal autonomy and lacking confidence in healthcare settings. These are detailed in the following section. The themes were relevant to both people with dementia and carers unless specified otherwise. Selected quotations to illustrate each theme are provided in Table 3. Conceptual links among themes are presented in Figure 2.
Illustrative quotations by theme.
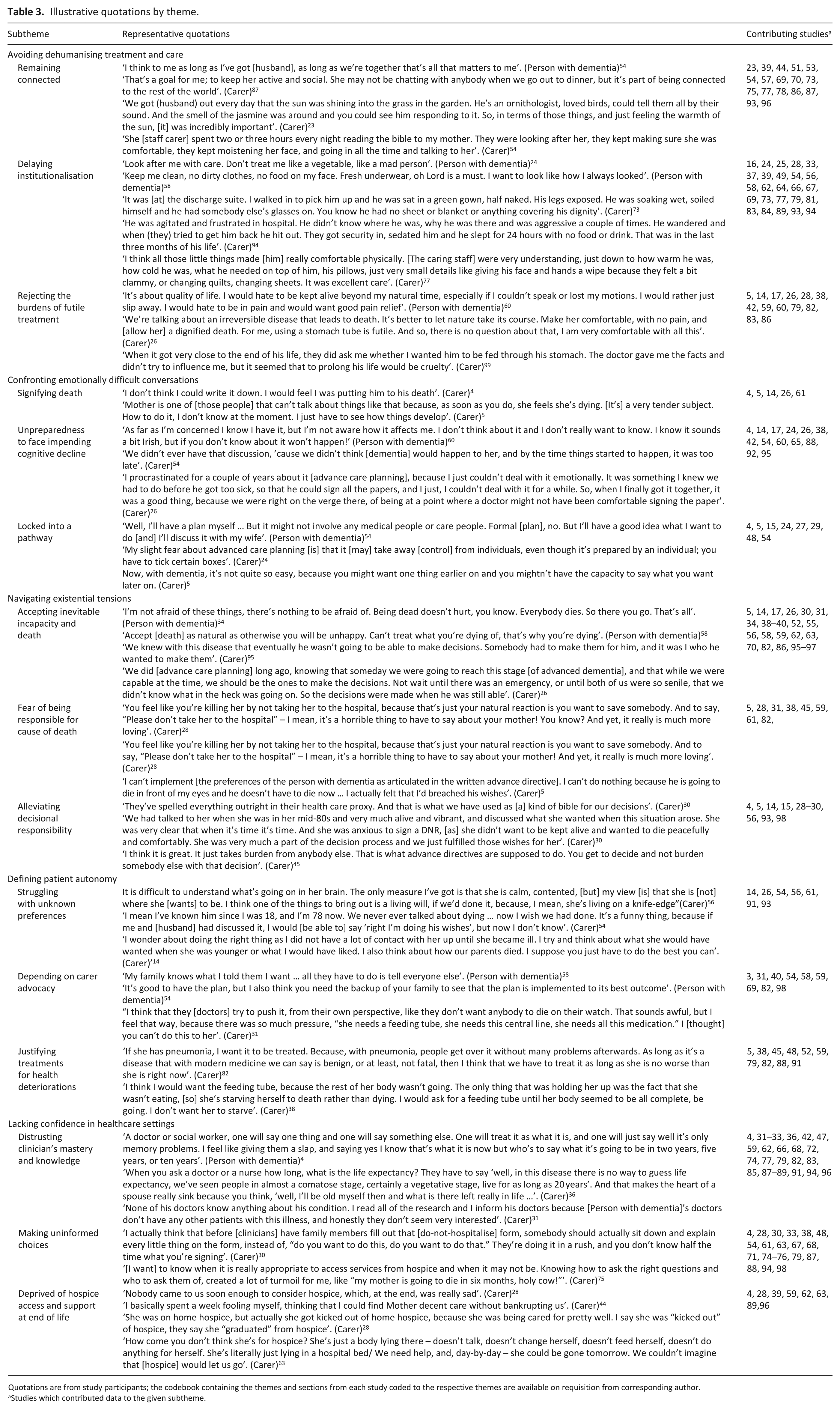
Quotations are from study participants; the codebook containing the themes and sections from each study coded to the respective themes are available on requisition from corresponding author.
Studies which contributed data to the given subtheme.
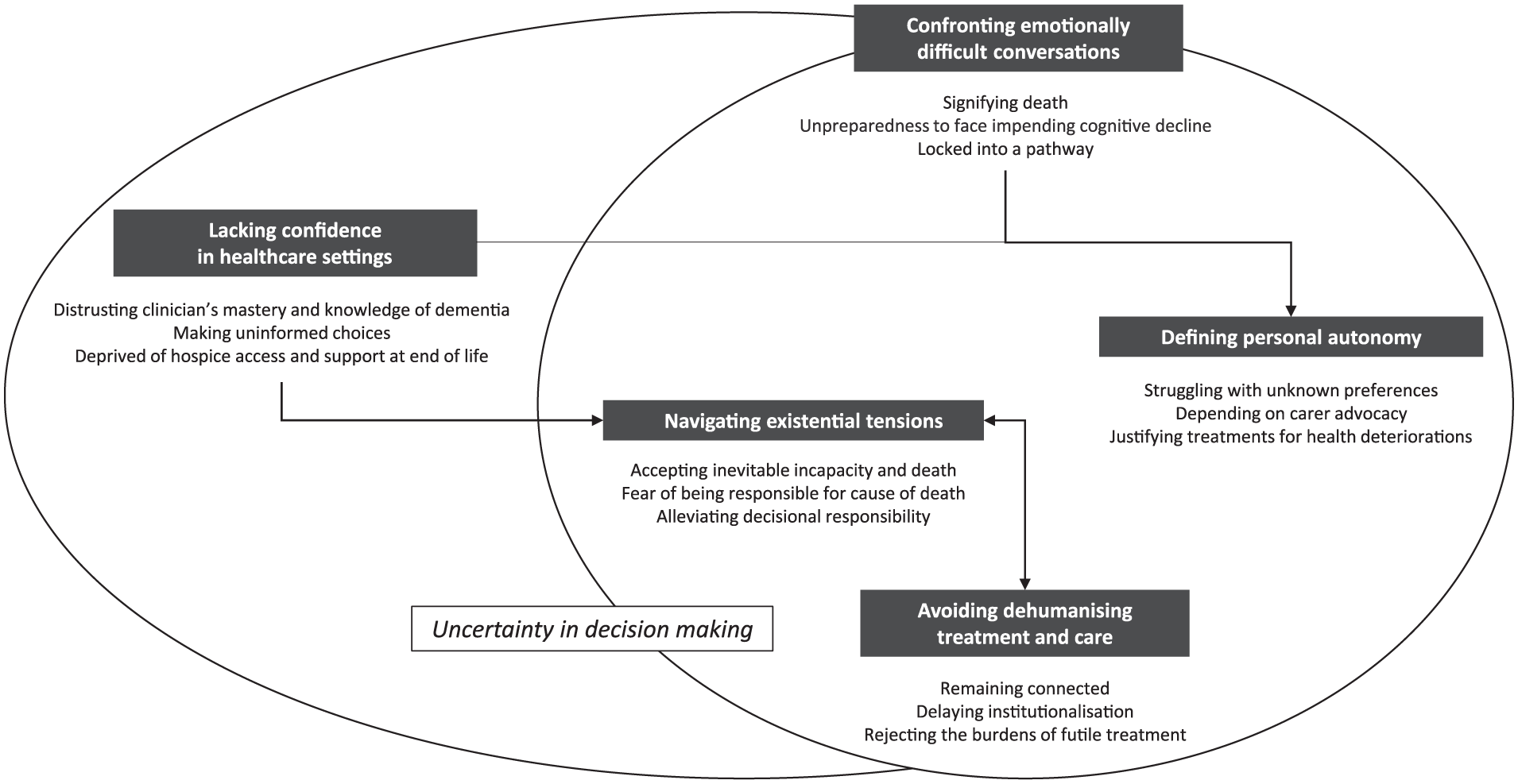
Thematic schema of people with dementia and carer’s perspectives of ACP and end-of-life care. For people with dementia and their carers, ACP and end-of-life care was characterised by a sense of uncertainty in decision-making. ACP required some to confront emotionally difficult conversations and some carers felt unprepared in the act of adhering to ACP preferences and making end-of-life decisions on behalf of the person with dementia. In addition, a lack of confidence in healthcare settings contributed to carer uncertainty while they navigated existential tensions nearing death. To overcome these challenges, people with dementia and their carers expressed needs and conditions to avoid dehumanising treatment and care.
Avoiding dehumanising treatment and care
Remaining connected
Nearing death, people with dementia and their carers highlighted a need for social, sensory and spiritual engagement consistent with a ‘normal life’ 57 without dementia. One person with dementia described spiritual engagement as attending to the ‘true self’ 23 who has a meaningful existence after memory, communication and emotional expression have diminished. As dementia was seen to ‘take away’ 73 the person they once knew, carers believed it was important that the person with dementia continue to participate in recreational activities, spend time with family and be treated as an individual with a unique personality. For instance, one carer felt it was important that her husband be surrounded by his own belongings while living in a nursing home. Some carers reflected on how having nursing staff physically present and verbally communicative with their dying relative, even when the person with dementia could no longer communicate, had inspired their trust and relieved anxiety.
Delaying institutionalisation
Some carers were upset because they perceived treatment and care delivered in nursing facilities or hospitals had ‘robbed’ 24 the person with dementia of dignity at end of life. Some carers felt ACP preferences had been deliberately ignored by care staff or were not prioritised within these services because all people with dementia were seen to be treated the same ‘based on institutionalised care practices’. 25 In the absence of knowing what the person with dementia would have preferred and because of a perception that institutionalised care would result in undignified care, some carers decided to keep the person with dementia at home as long as possible or endeavoured to provide care themselves (such as dressing and showering), to avoid ‘humiliating’ 81 acts of care. People with dementia and carers regarded dignified care within institutions as having preferences known and adhered to by health professionals, maintaining a respectable physical appearance, having privacy, being clothed, having hygiene maintained, being comfortable, being able to use the toilet and being free of fear and pain.
Rejecting the burdens of futile treatment
Some carers who had participated in ACP perceived dementia as a terminal condition and focused on promoting a ‘good death’ 58 in line with the preferences of the person with dementia only. Other carers reflected on circumstances in which they believed aggressive treatment caused only prolonged suffering and, thus, were preferring ‘to let nature take its course’ 26 – to have a ‘natural death without machines’. 59 In contrast, some carers who had not participated in ACP struggled to understand dementia’s dying trajectory and felt obliged to treat what could be treated (e.g. pneumonia, urinary tract infection, loss of swallowing), even in the advanced stages.
Confronting emotionally difficult conversations
Signifying death
Some carers felt unable to discuss ACP and end-of-life issues with the person with dementia as they were concerned it would cause the person with dementia to ‘feel [they were] dying’. 5 Some were reluctant to set goals or document ACP preferences (such as to refuse resuscitation) because they felt such a process was too harsh or inhumane and might be perceived as ‘putting [the person with dementia] to [their] death’. 4
Unpreparedness to face impending cognitive decline
Some people with dementia and their carers made an active decision not to participate in ACP, as they found the progressive and inevitable cognitive deterioration associated with dementia too ‘frightening’ 60 to think about in advance. Some felt there was ‘no real urgency’ 4 for ACP and avoided the discussion until the timing felt right. One carer reflected that they had ‘procrastinated for years’ 26 to avoid ACP until the person with dementia was ‘right on the verge’ of losing the ability to communicate. Other carers regretted that they had not completed ACP earlier because they felt the person with dementia’s illness had advanced too far for them to be able to participate in the decision-making process.
Locked into a pathway
Some people with dementia and carers feared that completing ACP documentation may be overly binding and lock the person with dementia into a ‘static and immutable’ 27 contract. ACP documents were perceived by some to be a barrier to autonomy and they expressed concern that they were just ‘tick[ing] certain boxes’ 24 on a pathway predefined by health professionals. Thus, some preferred to make informal advance care plans, believing that substitute decision-makers would more accurately communicate the preferences of the person with dementia at end of life. In contrast, some carers and people with dementia who had participated in ACP felt reassured because they perceived ACP documentation could be revised later if the preferences of the person with dementia changed.
Navigating existential tensions
Accepting inevitable incapacity and death
People with dementia and their carers who were more accepting of the progressive, ‘irreversible’ 82 and terminal nature of dementia appeared better able to engage in ACP discussions than those who felt unprepared to face these issues. ACP assisted some carers to confront fears of losing their loved one by preparing them for death and by enabling them to feel more comfortable making end-of-life treatment decisions regarding resuscitation and artificial nourishment. Some carers believed that a lack of communication with health professionals implicitly reinforced beliefs among people with dementia and/or their carers that death should remain unspoken. Thus, they felt having supportive health professionals who encouraged discussions of death was integral to reaching this acceptance.
Fear of being responsible for cause of death
Even when ACP had occurred, some carers were deeply conflicted when called upon to make end-of-life decisions. The main source of difficulty appeared to be operationalising goals for comfort into actions, such as denying hospitalisation or withholding nutrition or fluids, because such actions would effectively ‘cause’ 61 the death of their loved one. Thus, once carers realised that adhering to the operationalisation of the ACP preferences of the person with dementia would lead to the person’s death, they became less able to follow the preferences as they felt responsible for ‘killing’ 28 the person with dementia. This proved too overwhelming for some and led them to ignore the preferences of the person with dementia against life-sustaining treatments in order to preserve their own peace of mind and maintain a clear ‘conscience’.
Alleviating decisional responsibility
ACP helped some carers to overcome the perceived guilt and ‘burden’ 29 that they believed they would have otherwise experienced during end-of-life decision-making; this was particularly notable among carers who were adhering to ACP preferences of the person with dementia to forego life-sustaining treatments. Nonetheless, carers expressed a need to frame decision-making from the perspective of the person with dementia, such that documented advance care plans became ‘a bible’ 30 for decision-making and that their responsibility was simply to ‘implement [decisions]’ 98 or to ‘fulfil [the person with dementia’s] wishes’. 30
Defining personal autonomy
Struggling with unknown preferences
Carers were confronted by a ‘moral dilemma’ 93 or ‘quandary’ 26 when a medical decision was required and an advance care plan had not been made. Under these circumstances, carers relied on their knowledge and sense of who the person was before the onset of dementia to make treatment and care decisions. However, some carers found these decisions were accompanied by feelings of ambivalence and guilt and left them to hope that they were doing the ‘right thing’ 14 for the person with dementia. Such circumstances appeared easier for spousal carers who felt that being ‘married so many years’ 26 to the person with dementia led to an implicit understanding of their preferences; but more difficult for carers who had shared less frequent contact, such as children or extended relatives.
Depending on carer advocacy
Even when an advance care plan had been documented, some people with dementia expected their carers to be present during medical decisions, to protect and enforce their end-of-life preferences. Similarly, some carers felt it was their duty to ensure that the preferences of the person with dementia were adhered to. For example, such carers believed doctors were more focused on ‘meeting targets’ 3 and ensuring that nobody would ‘die on their watch’. 31 Thus, they anticipated that they might ‘have to fight the doctors’ 59 to prevent unwanted interventions, such as inserting a feeding tube or central line. One carer felt they had failed to advocate for the person with dementia because they had been ‘pressured’ 31 by doctors to consent to the use of life-sustaining treatments, despite knowing this was in conflict with the person’s ACP preferences.
Justifying treatments for health deteriorations
Even when ACP had occurred, some carers felt they needed to ‘breach’ the preferences of the person with dementia to withhold life-prolonging treatments, in order to save them from a ‘premature’ death. Carers who perceived health events, such as colds, bone fractures, pneumonia and dysphagia, as ‘curable’ with ‘modern medicine’, appeared to discount the life-threatening nature of such episodes in dementia. Rather, they perceived treatments involving minor surgery, antibiotics and feeding tubes as low risk and likely to return the person with dementia back to their previous state of health.
Lacking confidence in healthcare settings
Distrusting clinician’s mastery and knowledge of dementia
Some carers perceived a degree of ‘medical uncertainty’ among healthcare providers, leading them to feel frustrated and lose trust in healthcare providers. Such carers reflected on perceived inaccuracy at the point of diagnosis or when seeking advice about prognosis and/or treatment options for the person with dementia. In addition, some believed that physicians had purposefully disengaged from the person with dementia and their carers in conversations about ACP because they lacked confidence in making clinical judgements and the ACP process. Others felt that healthcare providers had actively ‘ignored’ 74 the carer’s concerns about the cognitive deterioration of the person with dementia and their inability to obtain a firm diagnosis was a barrier to them being able to plan for the future. Nonetheless, some carers looked to healthcare providers as the ‘specialists’ 32 of dementia and some carers chose not to ‘question [clinicians] decisions or actions about care’. 62
Making uninformed choices
Some carers who had completed ACP on behalf of a non-competent person with dementia felt that they had not made the best advance care plan, as they had not been given enough time or received enough support from clinicians to explore all options. One carer reflected that they could have ‘come up with a better plan’ 75 had they been better informed of the course of dementia and treatment options at the time and one carer who had completed a ‘Do-Not-Hospitalise’ form reflected that it had been completed in a rush and that they ‘[didn’t] know … what [they were] signing’. 30 Both people with dementia and carers expressed a need for ‘better education’ around the course of dementia and medical decisions they were likely to face to enable them to participate meaningfully in ACP, such as ‘what a feeding tube is [and] what a DNR [do not resuscitate] is …’, 33 and for communication to be ongoing and revisited to allow time to digest the relevant information.
Deprived of access to hospice care and support at end of life
Overall, carers were disappointed by difficulties they experienced ‘getting through the front lines’ 28 and accessing hospice and support when the person with dementia was approaching end of life, which they believed was a result of limited care options, high costs of services and inconsistent/lack of communication from health providers. Some carers felt ‘cheated’ 28 because the person with dementia was not offered hospice until it was too late to consider or benefit from the care. For others who had accessed hospice, some later became overwhelmed when the person with dementia was discharged or ‘kicked out of hospice’ 28 despite being considered ‘terminal’ but ‘not dying fast enough’ 63 to qualify for hospice care. Thus, carers believed the provision and duration of hospice access was inadequate in dementia and some questioned the appropriateness of using an ‘end-of-life care’ model in dementia given its unpredictable disease trajectory.
Discussion
People with dementia and their carers felt uncertain in making treatment decisions in the context of ACP and end-of-life care. They had to confront emotionally difficult conversations and navigate existential tensions during ACP; while also feeling a sense of distrust and a lack of confidence in the clinical information and support available to them in healthcare settings. Because of this, some were reluctant to discuss ACP preferences as they felt that ACP signified impending death; were unprepared to face the inevitable cognitive deterioration; or feared that by completing an advance care plan, they would be locked into a predefined pathway for care. In addition, carers needed to overcome uncertainty in decision-making if the person with dementia had not previously expressed their preferences; they felt adhering to the ACP preferences of the person with dementia would make them responsible for the person’s death; or they experienced disagreement with clinicians when advocating for the preferences of the person with dementia. Overall, people with dementia and their carers appeared more willing and prepared to undertake ACP if they were more accepting of the progressive, irreversible and terminal nature of dementia, and viewed ACP as a flexible and ongoing discussion with supportive healthcare providers.
Our review found that even when ACP documentation had been completed, some carers felt unprepared for making end-of-life decisions for the person with dementia. For some, this may have resulted from insufficient consideration of the types of decisions typically encountered through the dementia illness trajectory. It also acknowledges that uncertainty may be inevitable in some contexts of dementia and substitute decision-makers may require some ‘leeway’ when adhering to ACP preferences. 100 In our study, some carers struggled with decisions to refuse or restrict interventions, because they felt a level of personal responsibility for the death of the person with dementia. In addition, some felt they had breached the ACP preference of the person with dementia to refuse life-sustaining treatments when health complications arose that they perceived as curable. Nonetheless, some carers, who viewed themselves as only a messenger for the preferences of the person with dementia, expressed relief because they felt they had been spared from having to make otherwise burdensome end-of-life decisions.
The challenges to achieving person-centred care for people with advanced dementia, particularly in institutionalised settings, have been well described in the literature spanning different healthcare settings. 101 People with dementia and carers perceive a lack of personalised care, inclusion or choice in healthcare decisions and health professionals missing opportunities to enhance physical and psychological comfort.102,103 The themes identified in this review, such as avoiding dehumanising treatment and care and defining personal autonomy, similarly emphasise person-centred care as a central goal and priority of dementia care. For example, in this review, people with dementia and their carers expressed a need to maintain a connection to a ‘normal life’ and regarded dignified care as having preferences known and adhered to by health professionals. However, some carers experienced difficulties collaborating and communicating with health professionals, such as obtaining accurate information about prognosis or treatment options for the person with dementia or accessing hospice services or support at end of life.
While ACP has potential benefits for people with dementia and carers, implementing systems and structures to support ACP in dementia is complex. One challenge is that in dementia, cognition and decision-making capacity deteriorate and, in some situations, result in a lack of ability to understand the concepts involved in ACP.24,104,105 In addition, the preferences specified by a person during ACP may not cover all care decisions or daily care activities in advanced dementia, whereby a person’s ability to communicate needs is restricted, both by their own communication impairments (e.g. loss of speech) and by the health professional’s ability to assess and recognise the person’s needs and symptoms. Furthermore, the diagnosis of dementia may only occur years after the disease has begun,94,106 leaving decision-making responsibility up to a substitute decision-maker if the person is unable to participate themselves. Our new thematic schema of the perspectives of people with dementia and carers on ACP and end-of-life care draws attention to several key challenges: carers’ distrust in clinicians’ ability to provide accurate diagnosis and advice about the prognosis of dementia; difficulties facing and accepting cognitive decline and approaching death; uncertainties in defining and adhering to ACP preferences of the person with dementia; and barriers in accessing hospice and support at end of life. Our synthesis also highlights carers’ beliefs that using an ‘end-of-life care’ model in dementia is problematic given the dimensions of uncertainty experienced by carers across the illness trajectory.
Our review reflects findings from previous studies examining perspectives on ACP and end-of-life care among people with other chronic and progressive illnesses such as chronic kidney disease, chronic obstructive pulmonary disease and cardiac failure. Studies among these populations have also documented perceptions that ACP signifies death 107 or that completing an advance care plan may be overly binding. 108 Frustration about being unable to obtain a clear prognosis and access palliative care services has also been reported. 109 In addition, ACP and end-of-life decision-making can require negotiation with existential tensions when deciding to commence or continue with life-sustaining treatment. 110 Similarly, our review identified that some people with dementia and their carers found ACP emotionally difficult, distrusted clinicians’ ability to diagnose and prognosticate in dementia, and felt deprived of palliative care services. Moreover, carers needed to overcome existential concerns in dementia, particularly when the person with dementia lost capacity to make decisions for themselves.
Strengths and limitations
In this review, we conducted a comprehensive search and independent assessment of study reporting; and synthesised data from different healthcare contexts where people with dementia are likely to undertake ACP (such as care home, community, hospital and hospice) to develop a new and comprehensive thematic framework. However, there are some potential limitations. Only one in five of the included studies reported whether data saturation was reached, which questions whether subsequent data collection would have identified additional or novel concepts in those studies. In addition, less than one-third of the studies included people with dementia, and this may reflect the challenges of involving people with dementia in qualitative studies, 111 and the need to address these. Additional concepts regarding the perspectives of people with dementia on ACP and end-of-life care may have been identified if there had been a greater number of qualitative studies including people with dementia. We excluded articles that were not published in English and the majority of studies were from high-income English-speaking countries; thus, the transferability of the findings beyond these settings and populations is unclear. Nonetheless, the analytical themes offer a high-level conceptual framework regarding ACP and end-of-life care that may be applicable across different contexts.
Implications for policy, future practice and research
In ACP and end-of-life care in dementia, we suggest that health professionals demonstrate empathy and attend to people’s uncertainty in decision-making. Models of ACP that appear to lock individuals into a pathway, or do not facilitate acceptance of the natural course of dementia, that is, the cognitive decline and eventual mortality, may fail to elicit healthcare preferences before the person with dementia loses capacity. Thus, strategies to improve clinicians’ mastery and knowledge of palliative and dementia care, with respect to discussions about prognosis and treatment and care options available now and in the future, are essential to increasing confidence among people with dementia and their carers as they navigate the healthcare system. Moreover, consistent with past recommendations, 100 future ACP strategies should focus on preparing substitute decision-makers for potential uncertainties that may arise ‘in-the-moment’ when adhering to the person with dementia’s ACP preferences and plan for some leeway in these circumstances.
We suggest future research aims to further describe the perspectives of people with dementia on ACP and to consider addressing the challenges of conducting qualitative interviews with people experiencing varying levels of cognitive decline. Strategies to optimise participation of people with dementia in such research may include scheduling interviews with people when they are usually most alert during the day; being flexible in communication style and restructuring questions if they are not understood initially; and supplementing interviews with other qualitative techniques, such as observation.112,113 Furthermore, in general medical settings, ACP has previously been shown to improve the likelihood that preferences will be known and adhered to at end of life and reduce stress, anxiety and depression among surviving relatives. 114 However, similar high-quality studies of ACP have not yet been conducted in people with dementia 115 and thus future randomised controlled trials of ACP are needed to further understand the impact of ACP on people with dementia and their carers.
Conclusion
For people with dementia and their carers, the experience of ACP and end-of-life care was characterised by a sense of uncertainty in decision-making. ACP required some to confront emotionally difficult conversations and some carers felt unprepared in being able to adhere to ACP preferences and make end-of-life decisions on behalf of the person with dementia. We suggest health professionals demonstrate empathy and aim to facilitate acceptance of the inevitable cognitive decline and death in dementia and provide an understanding of the decisions that may need to be made along the trajectory of dementia. In addition, future ACP strategies should attend to potential uncertainties that may arise when carers are attempting to adhere to the person with dementia’s ACP preferences at end of life.
Supplemental Material
809571_supp_mat – Supplemental material for Perspectives of people with dementia and carers on advance care planning and end-of-life care: A systematic review and thematic synthesis of qualitative studies
Supplemental material, 809571_supp_mat for Perspectives of people with dementia and carers on advance care planning and end-of-life care: A systematic review and thematic synthesis of qualitative studies by Marcus Sellars, Olivia Chung, Linda Nolte, Allison Tong, Dimity Pond, Deirdre Fetherstonhaugh, Fran McInerney, Craig Sinclair and Karen M Detering in Palliative Medicine
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work received financial support from the Australian Government Department of Health National Palliative Care Program.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.