
Abstract
Background:
Advance care planning enables individuals to define goals and preferences for future medical care. Despite advances in research and the production of tools and methods for advance care planning, uncertainty remains regarding whether and which interventions support intended outcomes for patients. This lack of clarity is occurring despite high financial investment into advance care planning research through grant funding, relative to other palliative care areas.
Aim:
To utilise published reviews to explore the efficacy of current advance care planning interventions, including how they are evaluated, and whether they achieve their intended outcomes for adults living with an advanced illness.
Design:
Meta-review of reviews.
Data sources:
Five electronic databases (PubMed, CINAHL, EMBASE, Medline and PsychINFO) were searched for reviews published between 2015 and 2025. Quality of reviews was assessed by the AMSTAR-2 tool.
Results:
Thirty-nine reviews were included. Fifteen reviews evidenced significantly decreased hospital utilisation in line with patient’s preferences following advance care planning. Fourteen reviews evidenced significant increases in patients receiving care consistent with their goals, and 12 evidenced significant increases in patients documenting their preferences. Evidence on the impact of advance care planning on decisional conflict was mixed.
Conclusions:
This review highlights where advance care planning interventions significantly impact outcomes defining successful advance care planning. The existence of a range of interventions can accommodate preferences of patients or families regarding how to receive and engage with their options. This heterogeneity is, however, a challenge for synthesising research data to understand the impact of interventions and inform practice.
Advance care planning, through legal documentation and various interventions, aims to identify a patients preferences for future care.
Existing academic literature has debated the effectiveness of advance care planning in meeting patients goals of care and aimed to define outcomes of successful advance care planning.
Fourteen reviews evidenced significant increases in patients receiving care consistent with their goals following advance care planning interventions.
Twelve reviews evidenced significant increases in patients documenting their preferences following advance care planning, and eight evidenced increased congruence between patients documented wishes and surrogate reports of wishes.
Evidence on the impact of advance care planning on decisional conflict was mixed: eight reviews evidenced decreased decisional conflict, while five illustrated no effect.
This meta-review evidences that different advance care planning intervention types impact patient outcomes to varying degrees.
The importance of endorsing person-centred advance care planning is highlighted, recognising that specific interventions may better suit some patients and their preferences and goals for care, over others.
Importantly, advance care planning was scarcely evidenced to have a detrimental impact on any patient outcomes.
Introduction
Advance care planning is ‘a process that supports adults at any age or stage of health in understanding and sharing their personal values, life goals and preferences regarding future medical care’, as defined by a multi-disciplinary Delphi panel. 1 In its earlier stages, advance care planning was narrowly defined as stating written preferences via legal documentation (such as advance directives and living wills). 2 Although legal documentation of wishes remain important for many patients today, advance care planning has evolved into a holistic process over the life course that is ‘a process of preparing patients and surrogate decision-makers for communication and medical decision-making’. 3 Advance care planning takes many forms including, advance directives, ‘do not attempt cardiopulmonary resuscitation’ orders, conversations using supportive tools (such as Recommended Summary Plan for Emergency Care and Treatment (ReSPECT) forms), goals of care conversations and decision making tools.
As the breadth of interventions has expanded, researchers and clinicians have emphasised the lack of standardised outcomes relating to advance care planning. 4 In 2017, a Delphi panel of international experts identified outcomes that define successful advance care planning. 4 The resulting framework’s outcome domains included an assessment of process (e.g. readiness to engage and prognostic awareness), resulting actions (e.g. communication with surrogates and healthcare professionals and documenting preferences) and outcomes relating to quality of care (e.g. receiving care consistent with goals and satisfaction) and health care (e.g. hospital admissions and place of death). 4 The introduction of standardised outcomes aimed to develop a shared understanding of successful advance care planning, enabling comparison of findings across research and clinical initiatives.
The level of research funding allocated to advance care planning, is testament to its perceived value and importance. In 2025, a refreshed list of priorities for palliative and end of life care research was published, following James Lind Alliance Priority Setting Partnership methodology. 5 Exploring the barriers to people’s wishes being acted upon with regards to care and treatment remained a high priority 10 years on from its identification as a research priority in a previous Priority Setting Partnership in 2015.5,6 However, advance care planning’s efficacy and evidence base have been debated. A recent editorial by Morrison et al. 7 questioned whether advance care planning achieves its desired outcomes, highlighting the potential gap between hypothetical scenarios and decision-making in practice. This has sparked conversations throughout the field, where there remains disagreement about the efficacy of advance care planning in clinical practice.8,9
However, it is important to consider the literature base in the context of the relatively recent standardisation of outcomes defining successful advance care planning. 4 Therefore, the current meta-review aims to consolidate and convey the vast literature within this field, to evaluate interventions within the context of defined advance care planning outcomes.
Aim
This meta-review aimed to utilise published reviews to explore current advance care planning interventions, including how they are evaluated, and their efficacy in achieving their intended outcomes for adults living with an advanced illness.
Research questions were:
RQ1: How is the efficacy of current advance care planning interventions evaluated? (i.e. through which outcome measures and/or methods?)
RQ2: What is the efficacy of advance care planning interventions: do current evaluations suggest that advance care planning is achieving its intended outcomes?
RQ3: Do the above results differ by population?
Methods
Study design
A meta-review (systematic review of reviews) was conducted. This approach was selected to provide a summary of evidence from a number of reviews including the combination of different interventions and outcomes, 10 in a field where there are many existing important reviews. The protocol for this meta-review is registered on PROSPERO (ID: CRD42023449467) and is reported adhering to the PRISMA 2020 reporting guidelines 11 (Supplemental Material 1).
Eligibility criteria
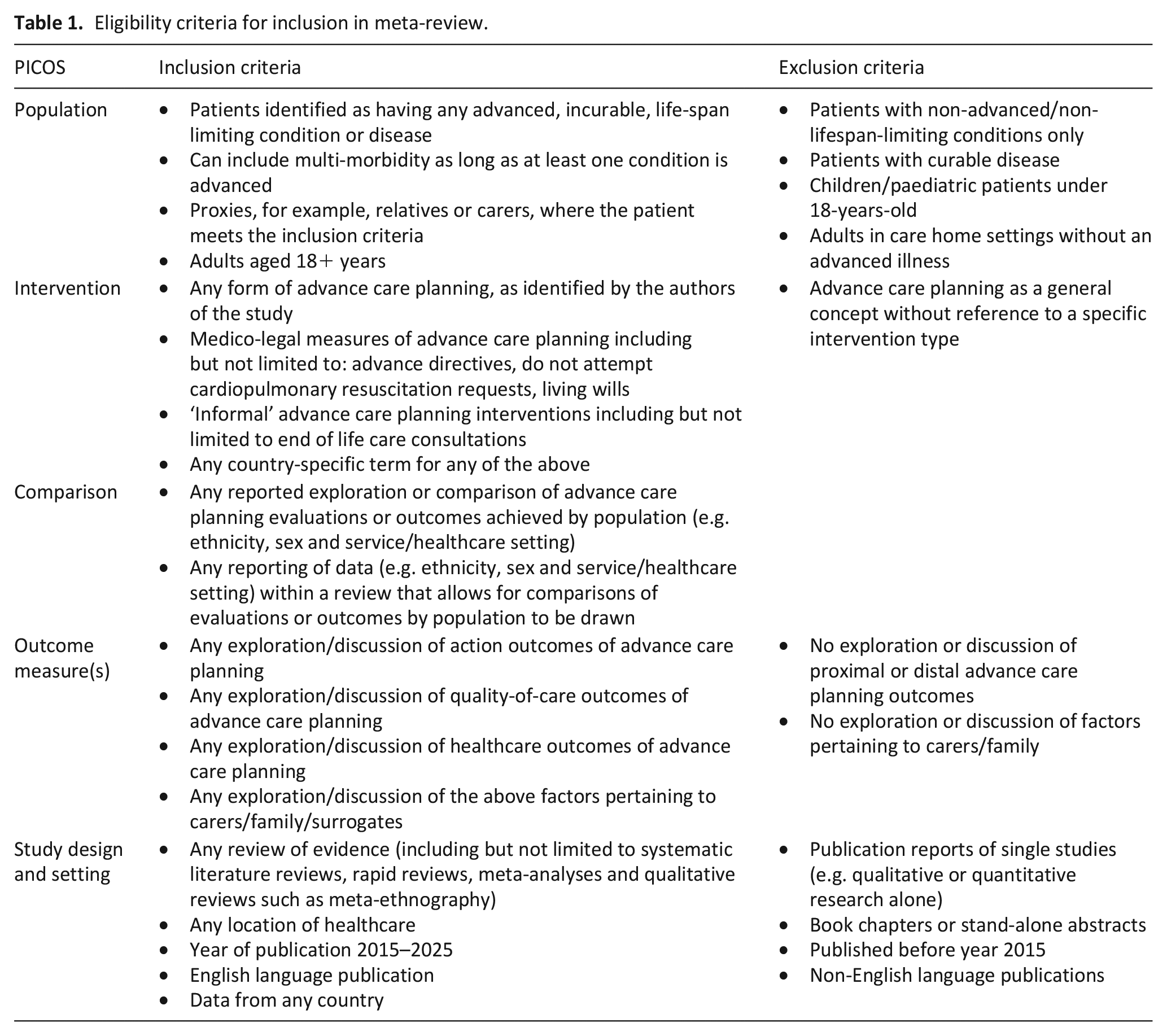
Full eligibility criteria are outlined in Table 1. Although advance care planning can be useful for all patients, this review focussed on patients with advanced disease due to the high perceived importance of advance care planning for this group: namely, the relationship and communication with healthcare professionals, conversations with family and anxiety and/or depression surrounding advance care planning are likely to be substantially different for patients with advanced illness.2,12 Criteria relating to advanced disease were purposefully broad and inclusive to maximise transferability; we included reviews reporting on patients with any advanced, life-limiting illness. This included frailty with or without a co-morbid condition.
Eligibility criteria for inclusion in meta-review.
Information sources
Searches were carried out in January 2025. Five electronic databases (PubMed, CINAHL, EMBASE, Medline and PsychINFO) were searched using a comprehensive search strategy of Medical Subject Headings and keywords. The full search strategy was based on previous work by the authors. 13 and can be found in Supplemental Material 2. Search terms covered heterogeneous terminology for advance care planning interventions, terms outlining palliative and end of life care and review types. Manual searching of relevant journals (Palliative Medicine; BMJ Supportive and Palliative Care and BMC Palliative Care), and secondary searches of eligible retrieved reviews reference lists were also carried out in January 2025.
Selection and data collection process
Articles retrieved from searches were imported into EndNote reference management software and deduplicated. Articles were title screened for initial eligibility, before progressing to abstract and subsequent full-text screening. This process was done collaboratively, with one author (JC) screening all papers, which were all second screened by another member of the team (NR, CSG, GH and BH). Any discrepancies were resolved through discussion.
Data were extracted into a pre-designed form in excel, extracting review information, participant information, intervention type and information on action, quality of care and healthcare outcome data. Data extraction of full texts was conducted independently by two researchers (JC, NR, CSG, GH and BH). Output was compared and combined.
Data items and outcomes
Outcomes considered in this meta-review stem from a Delphi-panel consensus on ‘Outcomes That Define Successful Advance Care Planning’. 4 This Delphi-study identified overarching advance care planning outcome domains into an organising framework; after consultation with Patient and Public Involvement (PPI) representatives and thorough exploration of the literature, three outcome domains to explore in this meta-review were selected.
As outlined in the Delphi-study, 4 Action outcomes ‘measure an individual’s completion of specific components of advance care planning such as discussion or documentation of a surrogate or medical preferences’. Quality of care outcomes ‘measure the impact of advance care planning on quality of care’, and Health care outcomes ‘measure the impact of advance care planning on health outcomes, such as health status and health care utilisation’. We did not consider Process outcomes in this review, as they aim to specify how or why an effect or relationship occurs, which is outside the scope of this review.
Risk of bias
Risk of bias assessment was carried out utilising the AMSTAR 2 tool: designed to evaluate quality of systematic reviews containing either randomised control trials or non-randomised studies. 14 Assessment was done independently by two members of the research team (JC and NR). Each of the 16 AMSTAR-2 domains was considered and scored ‘yes’, ‘partial yes’, ‘no’ or ‘not applicable’. An overall quality rating of ‘high’, ‘medium’, ‘low’ or ‘critically low’ was assigned, after considering the individual scores for each domain, including scoring of the critical statements identified within the tool. Furthermore, to examine the potential for bias introduced via individual studies being reported in more than one eligible review, the Corrected Covered Area (CCA) was calculated and is reported in the results of this meta-review. 15
Synthesis methods
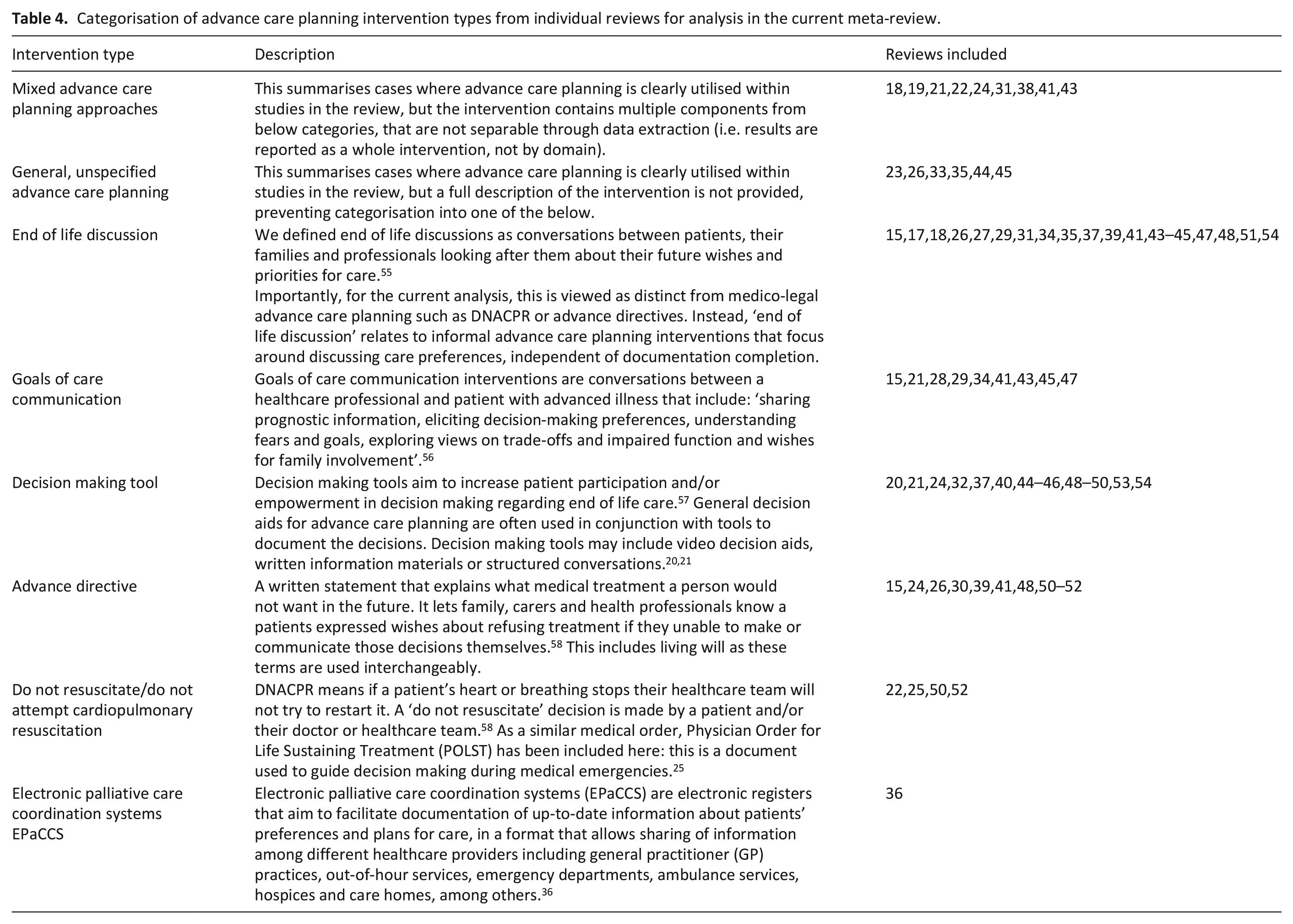
Given that this is a global review, considerable heterogeneity was found between intervention terms. Therefore, interventions were categorised based on the descriptions provided in individual reviews. Data extracted for each outcome domain was tabulated across the extracted advance care planning intervention categories. A separate table was developed for each outcome domain (i.e. action outcomes, quality of care outcomes and healthcare outcomes). These included whether the described advance care planning intervention showed a significant increase, decrease or no effect on the outcome, as reported in each paper. Where outcomes had considerable numbers of reviews associated with them, they were explored further via narrative summary. Data was visualised using R software.
Patient and public involvement
Two Patient and public involvement contributors supported this review (OS and KS). They were involved from conceptualisation of the review including protocol development. Key input included developing search terms, supporting full text screening, reviewing analysis, determining routes for dissemination, contributing to steering group meetings and support in developing conference posters.
Results
Study selection
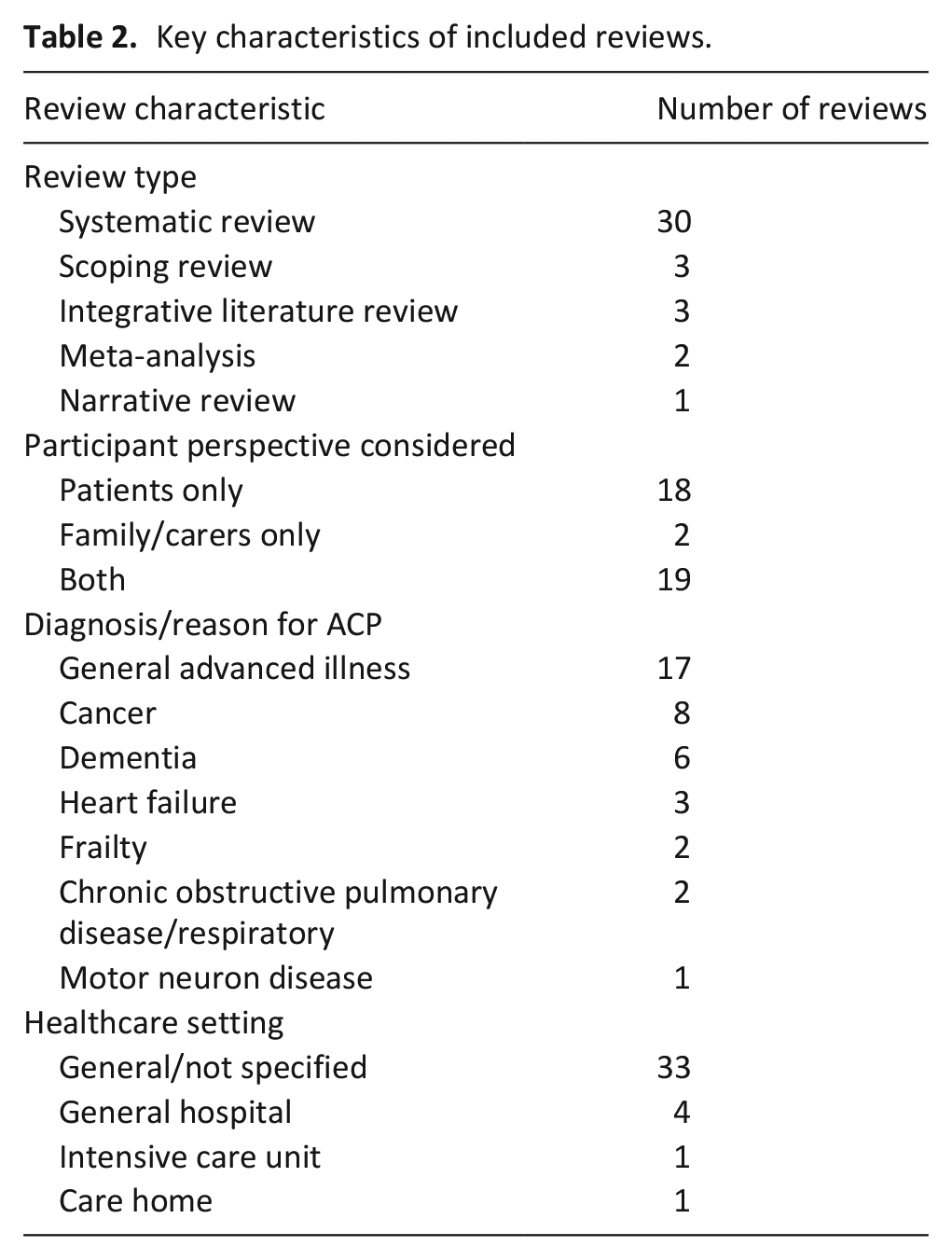
Of the 1551 records identified via database and grey literature searches, 39 were eligible for inclusion in the final review. These 39 reviews reported on 754 individual studies. A Corrected Calculated Area of 0.08 was calculated, indicating a low risk of bias of individual studies appearing in more than one review. 16 Key characteristics of included reviews can be seen in Table 2. Full study characteristics can be seen in Supplemental Material 3. Age was scarcely reported in individual reviews, but all considered adults aged 18 years or over. Gender and ethnicity data were rarely reported by individual reviews so cannot be reported here. The full screening process can be seen in Figure 1. 11
Key characteristics of included reviews.
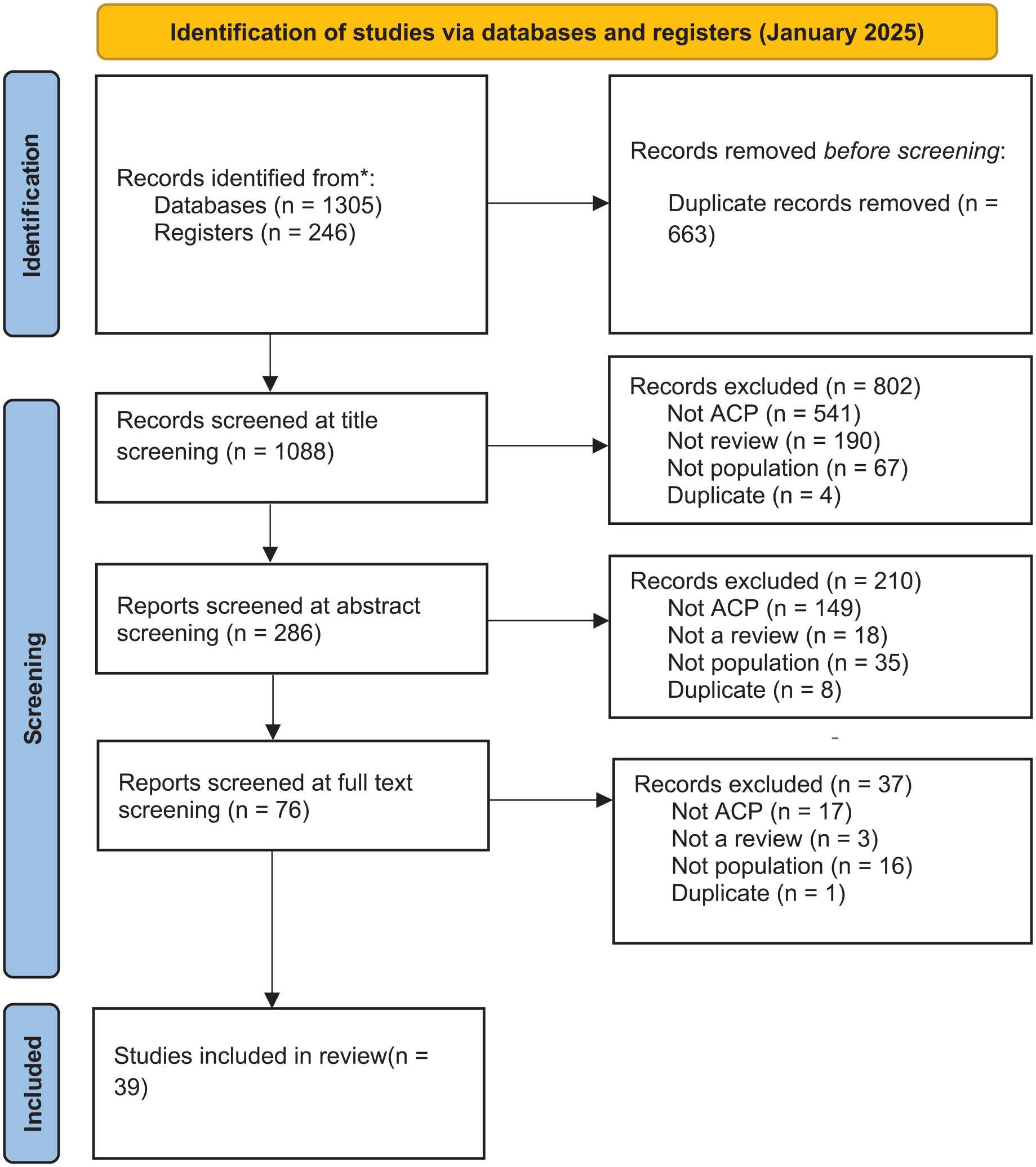
PRISMA 2020 flow diagram for new systematic reviews which included searches of databases and registers only.
Risk of bias in studies
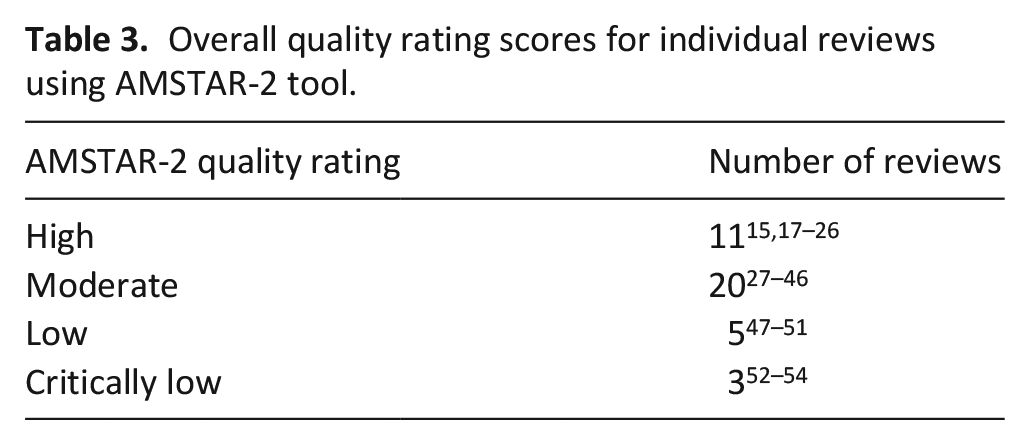
The AMSTAR-2 tool was used to assess quality of individual reviews: full reporting of final scores can be found in Tables 3 and 4.
Overall quality rating scores for individual reviews using AMSTAR-2 tool.
Categorisation of advance care planning intervention types from individual reviews for analysis in the current meta-review.
Healthcare outcomes
Thirty-one reviews considered at least one healthcare outcome (Figure 2).
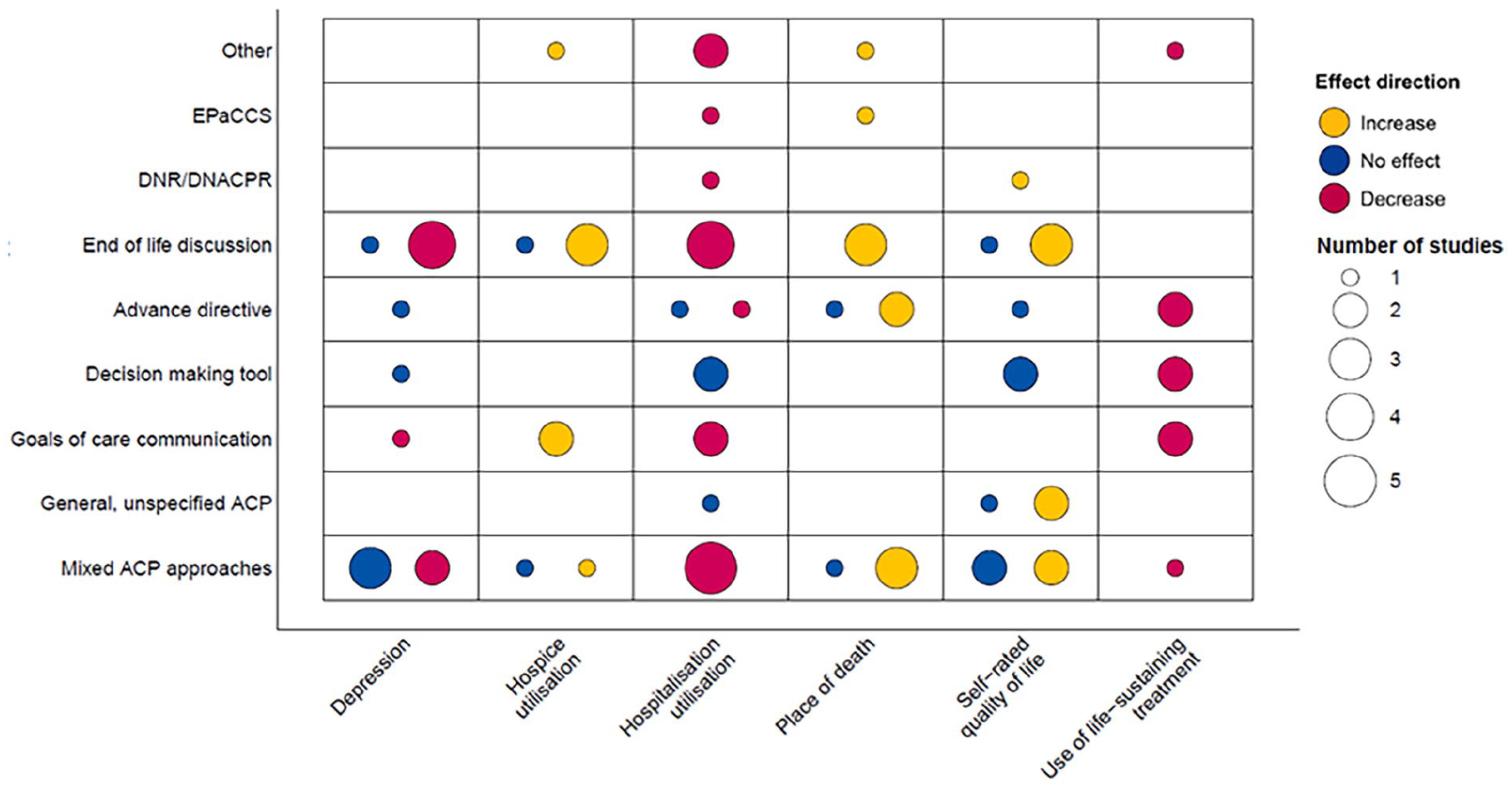
Evidence evaluating effect direction of advance care planning interventions on key healthcare outcomes.
Depression
Seven reviews evidenced a significant decrease in patients depression following advance care planning.15,22,28,31,37,51,54 Of these, one was low quality and one critically low.51,54 Decreased depression in intervention groups was not exclusive to patients; one review evidenced significant carer-reported decreases in patient depression, 51 and three reported significant decreases in carers self-rated depression and anxiety.31,37 Within these seven reviews, two reported a decrease in depression following interventions with mixed advance care planning approaches,22,31 four following end of life discussions,15,37,51,54 and one following a goals of care communication intervention. 28
However, six reviews reported interventions having no effect on patients self-reported depression.20,21,27,38,40,43 This was evidenced in three reviews considering interventions with mixed advance care planning approaches,21,38,43 one advance directive, 20 one end of life discussion intervention, 27 and one decision making tool. 40 Of these six reviews, two were high quality20,21 and four were moderate.27,38,40,43
Self-rated quality of life
Eight reviews evidenced a significant increase in patients self-rated quality of life following advance care planning.15,18,22,23,26,34,51,52 Of these, five were high quality.15,18,22,23,26 Three reviews looked at patients with dementia, reporting that end of life discussion-based interventions resulted in significant increases in self-reported quality of life.15,34,51 One of these reviews also highlighted increased quality of life for carers of patients with dementia. 51 One review reported increase quality of life following an advance directive, 52 two following mixed advance care planning approaches,18,22 and two following general, unspecified advance care planning.23,26
However, five reviews reported no effect between intervention and control groups for self-rated quality of life,20,21,38,43,49 and two reported mixed evidence.26,52 Of these, three were high quality, two moderate, one low and one critically low. One review reporting mixed evidence considered frail patients, where the impact of advance care planning on quality of life was inconsistent across several quality of life scale measurements. 26
Hospital utilisation
Fifteen reviews evidenced a significant decrease in hospitalisation following advance care planning intervention.15,18,19,21,22,24,25,34,36,38,41,43,50 –52 Seven were high quality,15,18,19,21,22,24,25 two low,50,51 one critically low. 52 Three reviews considered patients with cancer, finding advance care planning resulted in higher proportion of home care versus hospitalisation, 24 significant reductions on hospital admissions in the last 30 days of life, 41 and that communication-based interventions had higher odds of reducing hospitalisation than documentation-based interventions. 19
Four reviews considered the impact of advance care planning documentation on hospital utilisation for people with dementia. Results indicated that advance directives increased home care. End of life discussions and goals of care communication resulted in briefer hospital stays, and all interventions contributed to decreased hospital admission.15,34,50,51
In reviews with patients with mixed diagnoses, Vranas 25 evidenced across eight observational studies that treatment limitations on Physician Orders for Life Sustaining Treatment (POLST) are associated with reduced hospitalisation. Leniz 36 reported a significant decrease in hospitalisation for patients who completed an Electronic palliative care coordination systems (EPaCCS) intervention.
A further four reviews reported no effect of advance care planning interventions on hospitalisation for patients with cancer, frailty or mixed diagnoses.26,30,32,49
Use of life sustaining treatment
Eight reviews evidenced significant decreases in the use of life sustaining treatment in line with patients preferences, across six intervention categories spanning both discussion-based and documentation-based advance care planning.19,24,25,28,32,45,50,52 All reported significant decreases in receipt of aggressive treatment options in line with expressed preferences, with three explicitly highlighting increased preferences for comfort-based care.25,28,52 One review was rated as critically low quality. 52 This finding spanned a range of diagnoses, including cancer,19,24,28 dementia, 50 and COPD. 45
Hospice utilisation
Seven reviews evidenced significant increases in hospice utilisation following interventions with mixed advance care planning approaches, 18 Goals of Care Communication interventions,28,41 end of life care discussions34,44 and Physician Orders for Life Sustaining Treatment (POLST). 25 Of these, two were high quality18,25 and the remaining four were moderate.28,34,41,44 Two reviews considered the impact of goals of care communication for patients with cancer, reporting significant increases in hospice admission 41 and discharge from hospital into hospice 28 corresponding with patients wishes. This increase in hospice admission was evident across other diseases, including heart failure 18 and dementia. 34
A further two reviews reported no effect of interventions with mixed advance care planning approaches and end of life care discussions on hospice utilisation.19,29
Place of death
Ten reviews evidenced significant increases in concordance between preferred and actual place of death after interventions with mixed advance care planning approaches,31,38,41 Electronic palliative care coordination systems (EPaCCS), 36 advance directives,15,30 end of life care discussions,18,29,59 and Physician Orders for Life Sustaining Treatment (POLST). 25 Importantly, all reviews were high or moderate quality. Three reviews highlighted that more patients died at home (in accordance with their preferences) following advance care planning,30,31,41 with a further two reviews reporting that advance care planning supported patients to die outside of hospital, as preferred.18,25 This significant increase in congruence for place of death following advance care planning was evident for several diseases, including frailty, 31 cancer,30,41 dementia 16 and heart failure.18,29
Two reviews reported no effect of interventions with mixed advance care planning approaches 21 or living wills 52 on congruence in place of death. One was high quality 21 and one critically low. 52
Quality of care outcomes
Thirty-one reviews considered at least one quality of care outcome (Figure 3).
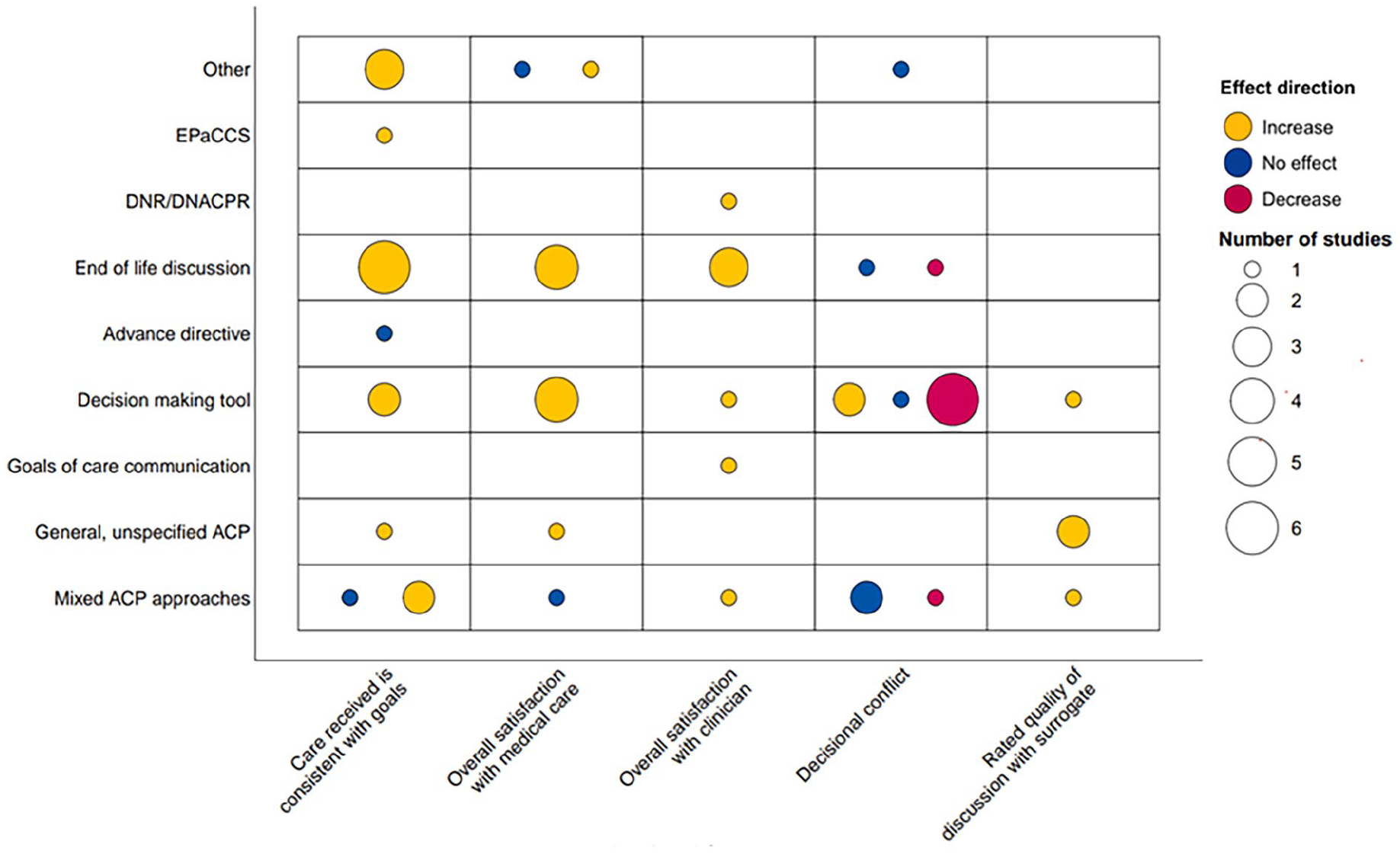
Evidence evaluating effect direction of advance care planning interventions on key quality of care outcomes.
Care received is consistent with goals
Fifteen reviews evidenced increased concordance between preferred and actual care following interventions with mixed advance care planning approaches,21,22, end of life consultations,15,29,31,34,45,54 decision making tools,40,50 EPaCCS, 36 general, unspecified advance care planning, 44 and interventions categorised as ‘other’.18,42,53 Of these 15, only one was low quality. 50 and one critically low. 53 Three reviews considered patients with dementia, reporting that end of life discussions and decision-making tools increased adherence to patients care goals, due to wishes becoming known.16,34,50 One review highlighted that EPaCCS resulted in an increase from 55% to 79% of patients with general advanced illness receiving their desired care. 36
Two additional reviews reported no effect of interventions on concordance between preferred and actual care.24,38 One was critically low quality. 54
Overall satisfaction with medical care
Ten reviews evidenced increased satisfaction with medical care overall after engaging with advance care planning interventions.15,18,23,27,34,40,43,45,46,49 Three were high quality,15,18,23 one low 49 and the remaining moderate. For patients with dementia, carer satisfaction was often used as a proxy, indicating increased carer satisfaction with medical care following end of life discussions15,27,34 and a decision making tool. 46 Significant increases in patient satisfaction with medical care following advance care planning interventions were also seen for patients with heart failure18,23 and COPD or respiratory diseases. 45
Two reviews reported no effect of advance care planning interventions on patient or carer satisfaction with medical care.20,22 Both were rated as high quality reviews.
Overall satisfaction with clinician
Seven reviews evidenced increased overall satisfaction with clinicians following ACP interventions.17,21,22,28,37,49,54 The quality of these were mixed: four high quality,17,21,22,37 one moderate, 28 one low, 49 and one critically low. 54 Two reviews investigating decision making for people with general diagnoses (i.e. patients diagnosed with an advanced illness that is not specified by the review the data is extracted from), and GOCC interventions for patients with cancer reported both patient and carer-reported increases in satisfaction with clinician following the intervention.28,49 A further two reviews considering end of life discussions reported significant increases in satisfaction with clinician, due to increased trust and reported quality of conversations.17,54
Decisional conflict
Evidence outlining the impact of advance care planning on decisional conflict is mixed. Decisional conflict is personal uncertainty about which option to choose. Eight reviews reported decreased decisional conflict (i.e. increased decisional confidence) following ACP.21,24,27,32,37,46,48,54 Six of these eight reviews considered decision making interventions.24,37,46,48,54 Four reviews reported significant decreases in decisional conflict as reported via the Decision Conflict Scale.27,32,46,48
However, five reviews evidenced no effect on decisional conflict for interventions with mixed advance care planning approaches,38,43 end of life discussions,33,35 and a decision making tool. 49 Four of the five reviews were moderate quality, with one rated as low. 49 All five reviews considered patients with general or mixed diagnoses. A further two reviews reported a significant increase in decisional conflict20,50: one high quality 20 and one low quality. 50 In one, patients with cancer reported more uncertainty following an educational video intervention, 20 with the other reporting increased carer-reported decisional conflict for patients with dementia, following implementation of a decision making tool. 50
Action outcomes
Thirty reviews considered at least one action outcome (Figure 4).
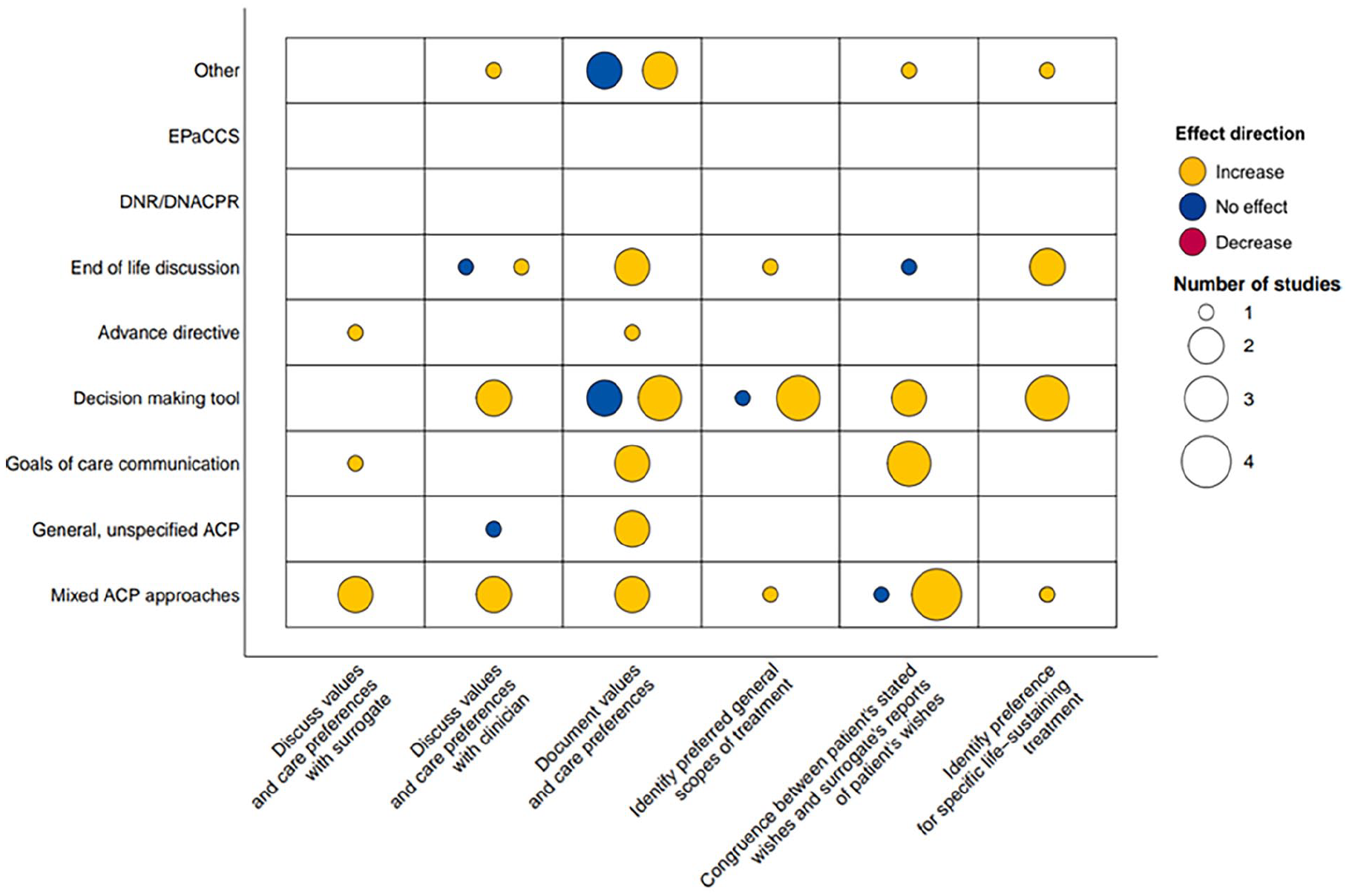
Evidence evaluating effect direction of advance care planning interventions on key action outcomes.
Discuss values and care preferences with clinicians
Six reviews evidenced a significant increase in patients discussing values and care preferences with clinicians following interventions with mixed advance care planning approaches,31,38 end of life discussion 45 decision making interventions45,48 and one intervention categorised as ‘other’. 20 Evidence highlighted significant increases in willingness to discuss preferences for patients with COPD, 45 in addition to significant increases in reported end of life conversations post-intervention.20,31,38,48
A further two reviews reported no effect of general advance care planning interventions or end of life discussions on rates of discussion of values and care preferences with clinicians.17,35 One review reported only 19% of collated studies evidenced a significant increase in discussion rates, despite increased documentation. 17
Document values and care preferences
Twelve reviews evidenced significant increases in documentation of patients values and care preferences following advance care planning intervention.21,22,26,28,34,35,40,43 –45,48,53 Six of these reviews reported significant increases in advance directive completion as documentation of patients’ preference, resulting from interventions with mixed advance care planning approaches, 22 decision making tools,40,44 a goals of care communication intervention 43 and one general, unspecified ACP intervention. 26 One high quality review reported 20 RCT’s evidenced significant increases in documentation of care preferences, 21 and another moderate quality review reported on 15 studies evidencing increased documentation of preferences for patients with dementia residing in nursing homes. 34
However, two of these reviews (one low quality 48 and one critically low 53 ) presented mixed evidence, whereby some individual studies within the reviews reported significant increases, and some reported no effects of the advance care planning intervention on documentation of care preferences.48,53 A further two reviews reported no effect of a decision making tool and an intervention categorised as ‘other’.27,49
Congruence between patients stated wishes and surrogate’s reports of patients wishes
Eight reviews evidenced increased congruence between patients’ wishes and surrogate reports of these wishes following interventions with mixed advance care planning approaches,21,22,38,43 goals of care communication29,37,47 and a decision making tool. 48 Notably, one of these reviews (moderate quality) reported a meta-analysis of 17 studies indicating a significant increase in congruence following shared decision-making. 37 Two of these reviews considered specific disease groups, namely patients with cancer and heart failure, both finding that the intervention group demonstrated significantly higher congruence than the control group.29,47
Two further reviews reported no significant differences between intervention and control groups regarding patient-surrogate congruence, for interventions with mixed advance care planning approaches and end of life discussions.18,35 One was high quality, 18 the other moderate. 35
Identify preference for specific life-sustaining treatment (e.g. CPR, etc.)
Six reviews evidenced significant increases in patients identifying preferences for life-sustaining treatments following interventions with mixed advance care planning approaches, 22 video interventions,20,32,44 and end of life discussions.27,47 Two of these reviews considered patients with cancer, reporting a significant increase in patients identification of their preferences surrounding life-sustaining treatment, even when these preferences were to opt-out of treatment.20,47
However, one of the six reviews reported mixed evidence regarding patients with dementia 27 – this was rated moderate quality. Although some studies reported that the intervention group were more likely to identify preferred life-sustaining treatment options, including carers preferences, this was not a significant difference. 27
Differences in ACP between populations
This research aimed to explore whether advance care planning interventions and outcomes differed by population. However, data on the population considered was rarely reported within individual reviews: only two reviews offered population-based comparisons of advance care planning.47,53 One reported that men were less likely to engage in discussion-based advance care planning interventions, and were therefore more likely to receive aggressive treatment as their preferences were unknown. 47
Both drew comparisons by ethnicity: one stated that minoritised ethnic groups were less likely to discuss their care preferences with a clinician, 53 and the other outlined that compared to white patients (in the USA) who preferred aggressive end of life care, black patients were less likely to have these preferences met. 47
Discussion
This meta-review consolidated the vast literature examining the efficacy of current advance care planning interventions, including how interventions are evaluated (i.e. through which outcomes), and whether current evaluations suggest that advance care planning is achieving its intended outcomes.
Healthcare outcomes
Fifteen reviews evidenced significantly decreased hospital utilisation in line with patients’ preferences following advance care planning. This is consistent with previous evidence demonstrating low advance care planning rates (7% of patients studied) among patients re-admitted to hospital within 30 days before death. 60 Further, evidence has shown the impact of advance care planning on specific elements of hospitalisation; such that it can decrease ICU admission. 61 Further, six reviews highlighted significant increases in hospice utilisation, in line with patients preferences, following advance care planning. This supports previous evidence that advance care planning reduces hospitalisation and increases hospice use. 62 Decreased hospitalisation has been evidenced to impact costs associated with palliative care, through reducing emergency and unplanned admissions, thus saving costs for the patient and healthcare systems.63,64
Evidence regarding impact on patients’ wellbeing was mixed; but no advance care planning interventions were found to increase depression or negatively impact wellbeing. Eight reviews evidenced significant decreases in self-reported depression following advance care planning, but six reported no effect. Six reviews suggested increased quality of life, but five reported no effect. Although evidence consistently demonstrates a high prevalence of mental ill-health towards the end of life, there is a lack of consistency in measurement scales and definitions for these outcomes.65,66 Therefore, these conflicting findings may be explained by documented heterogeneity in definition and measurement of depression and quality of life, 67 resulting in fewer high quality meta-analyses.
Nine reviews indicated significant increases in patients dying in their preferred place of death following advance directives, end of life discussions and advance care planning generally. This supports previous evidence suggesting that over three quarters of patients who documented a preferred place of death during advance care planning died in their preferred location. 68 Largely, data highlights preference for dying outside of hospital, which is congruent with many patients actual place of death.59,69
Quality of care outcomes
Fourteen reviews evidenced that advance care planning significantly increased patients receiving care that was consistent with their goals. This outcome is central to successful advance care planning, as a Delphi study outlined the ‘goal of advance care planning is to help ensure that people receive medical care that is consistent with their values, goals and preferences’. 1 However, goal-concordant care is difficult to measure, with little guidance in how to do so. Evidence has suggested methodological weaknesses in studies assessing this outcome with non-reproducible research using poorly defined concepts. 70 This calls for research to utilise standardised measurement tools or outlining reproducible methods for retrospective chart reviews to produce robust data regarding goal-concordant care.
Eight reviews reported decreased decisional conflict (i.e. increased decisional confidence) following advance care planning, with four measuring this via the Decision Conflict Scale. This supports previous evidence that advance care planning can improve decisional conflict in both patients and surrogates.71,72 However, five reviews evidenced no effect on decisional conflict following advance care planning. A further two reviews reported a significant increase in decisional conflict. Some disparity in evidence may be due to the confounding factor of readiness: evidence has demonstrated that advance care planning may decrease decisional conflict where patients/surrogates are ready to engage. 73
Action outcomes
Twelve reviews evidenced significant increases in documentation of patients values and care preferences following interventions. Six of these reviews reported significant increases in advance directive completion as documentation of patients’ preference. However, previous evidence has highlighted that many patients with completed legal forms/orders do not have accompanying documented explanatory discussions. 74 In addition, many forms are not easily accessible: both to patient populations (i.e. language accessibility, health literacy or access to services providing advance care planning), and to medical professionals (i.e. sharing of completed advance care plans across services). 74 Consequently, recommendations have been made for ensuring high quality advance care planning documentation when developing interventions. 75
Evidence gaps and directions for future research
High levels of missing data and heterogeneity in demographic reporting, meant it was not possible to complete our planned analyses regarding differences in advance care planning efficacy for different populations. Standardising the reporting of demographic data and bolstering attempts to reduce missing data could enable the efficacy of advance care planning interventions across identities such as gender, ethnicity, country and age group and intersections between these characteristics to be explored, which could generate important insights.
Further, although this meta-review explores the efficacy of advance care planning interventions broadly, it does not explore the mechanisms and contextual factors behind observed effects. As recommended within previous research, it may be beneficial to explore the intrapersonal, interpersonal and socio-environmental interactions of essential stakeholders in advance care planning. 76
Limitations
Globally, there is a plethora of advance care planning interventions. Although many incorporate similar approaches, there are numerous small-scale interventions that have unique names or elements, that are not widely known. For an intervention to be evaluated within the current review, it must have been previously included in a peer-reviewed systematic review. Therefore, it is likely that some advance care planning interventions may not be fully represented within this review. However, we undertook extensive searches leading to the inclusion of 754 individual studies across 39 reviews, representing a wide body of literature.
Furthermore, due to the continuing evolution of advance care planning and research methods investigating it, existing research and data is heterogeneous. This is apparent in intervention names and terminology pertaining to outcomes.38,77 Therefore, despite best efforts to develop an informed, piloted search strategy, it is possible that this vast heterogeneity may lead to unintentionally excluded literature. To avoid incorrect exclusion of literature identified via electronic searches, we erred on the side of inclusion throughout the screening process: where language used in titles was ambiguous, the literature progressed to abstract screening stage for more thorough screening.
Finally, the ‘Process domain’ outcomes outlined in the Delphi study framework that guided the format of the outcomes discussed in the current meta-review was excluded. 4 This was because constructs within this domain (i.e. behaviour change and perceptions) were reported in individual reviews less frequently, and more heterogeneously than action, outcome and quality of care domains. Therefore, process outcomes were excluded to increase consistency in data extraction and reporting. However, analysis of these outcomes may provide useful insight if assessed in future research.
Conclusions
There are a wide range of advance care planning interventions, with a range of aims and levels of success in facilitating care aligned with the wishes of patients and families. Unfortunately, the process of exploring and documenting wishes is not always enough to enable end of life experiences that are congruent with preferences: this can be influenced by many factors beyond advance care planning such as availability of resources (e.g. hospice beds), the ability to manage symptoms in different settings and capacity of informal carers.
However, advance care planning, in various forms has been linked to positive or neutral impacts on different aspects of end of life care and experience; very little evidence that advance care planning has a detrimental effect was found in studies reviewed. The existence of a vast range of interventions and outcomes can accommodate different preferences of patients or families with regards to how to receive and engage with their options. This heterogeneity is, however, a challenge for synthesising research data to understand the impact of interventions and inform practice.
This review is the first (to the best of the authors knowledge) to take a systematic approach to exploring the aims and impacts of advance care planning using an accepted framework 4 and represents a step forward in consolidating the growing and extensive body of evidence around advance care planning towards the end of life.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163251344428 – Supplemental material for Evaluating outcomes of advance care planning interventions for adults living with advanced illness and people close to them: A systematic meta-review
Supplemental material, sj-docx-1-pmj-10.1177_02692163251344428 for Evaluating outcomes of advance care planning interventions for adults living with advanced illness and people close to them: A systematic meta-review by Jodie Crooks, Noura Rizk, Charlotte Simpson-Greene, Gina Hopwood, Owen Smith, Kathy Seddon and Briony Hudson in Palliative Medicine
Supplemental Material
sj-docx-2-pmj-10.1177_02692163251344428 – Supplemental material for Evaluating outcomes of advance care planning interventions for adults living with advanced illness and people close to them: A systematic meta-review
Supplemental material, sj-docx-2-pmj-10.1177_02692163251344428 for Evaluating outcomes of advance care planning interventions for adults living with advanced illness and people close to them: A systematic meta-review by Jodie Crooks, Noura Rizk, Charlotte Simpson-Greene, Gina Hopwood, Owen Smith, Kathy Seddon and Briony Hudson in Palliative Medicine
Footnotes
Author contributions
NR, JC and BH conceptualised the review. All authors designed the protocol. JC and NR conducted searches. JC, NR, BH, CSG, GH, KS and OS screened search output for eligibility. JC, NR, CSG and BH extracted data. JC, NR and BH synthesised data. CSG developed visualisation of data and figures. JC and NR led on writing the manuscript; all authors reviewed.
Data availability statement
All data is available in Supplemental Material 3.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. BH, JC, NR, GH and CSG are employed by Marie Curie.
Ethical approval and consent to participate
No ethical approval was sought due to the nature of the review.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.