
Abstract
Background:
During advance care planning, individuals can benefit from the support of a healthcare professional to navigate the intricacies of decision-making. There are specific roles to be played at each level of the process. Evidence is lacking about how professionals understand their role when conducting advance care planning conversations.
Aim:
To explore how professionals perceive, define and describe their role when conducting advance care planning conversations.
Design:
We conducted this exploratory cross-sectional study in Switzerland from November 2019 to June 2020 by using semi-structured interviews, which were transcribed and thematically analysed with an inductive approach.
Participants:
Fourteen professionals having received a training on advance care planning in Switzerland.
Results:
We identified three themes: (1) role typology; (2) individual-centred and (3) professional-centred aspects related to role ascription. Roles that professionals undertake were aggregated in two overarching categories, ‘facilitators’ and ‘counsellors’, according to whether they prioritise individual’s capacity to decide for themselves or their need to receive guidance towards a particular decision. In practice, roles fluctuate between these categories, according to the individuals (to what extent they are informed and eager to engage in autonomous decisions, their communication capacity and desires) or the professional (main profession and involvement in the person’s care plan).
Conclusions:
Advance care planning requires professionals to be very adaptable and flexible in order to identify the role that they can play in each situation. Training needs to take into consideration this complexity and address it explicitly.
One of the specificities of advance care planning resides in the fact that individuals receive the support of a third party to help them navigate the intricacies of decision-making
The role of leading advance care planning conversations is a critical element of the process and requiring particular competences
Many professionals identify the need to clarify their own role within advance care planning and associate this to a barrier in practicing and implementing advance care planning
Findings show how professionals who conduct advance care planning conversations perceive, define and describe their role during advance care planning (what can be identified as ‘role self-ascription’)
Role shifts dynamically between two categories, ‘facilitators’ and ‘counsellors’, showing that role borders are permeable and that professionals juggle with a dual attitude
Certain professions were considered more competent to conduct advance care planning, such as being a clinician or a medical specialist
Advance care planning training needs to take into consideration that professionals are required to be very adaptable and flexible throughout the process in order to identify the role that they can invest in each situation
Background
Advance care planning enables individuals to make health-related decisions in anticipation of a situation in which they would be incapable of doing so spontaneously. 1 During advance care planning, people receive information about potential health trajectories and treatment options, identify values that are relevant for defining goals of care and what medical outcomes might or might not be acceptable, and often record their results and decisions for future care. 1 Evidence compiled by systematic reviews highlights several positive effects of advance care planning, particularly in the context of terminal illness, such as reducing hospitalisation, increasing use of palliative services, increasing concordance between actual care and people’s care wishes, and decreasing use of life-sustaining treatment that would drastically lower quality of life.2,3 Other reviews suggest shortcomings in the practice. 4 Studies show that outcomes of advance care planning are influenced by legislations, institutional policies and cultural factors 5 as well by numerous barriers, such as lack of training and time to conduct conversations, 6 its inadequate implementation (e.g. offering it too late). 7
While advance care planning programmes exist in which patients are only provided with decision aids and complete the process by themselves, in most cases, advance care planning relies on a healthcare professional who supports patients to understand, explore and make decisions. 5 Recognising the complexity and life-and-death implications of the decisions made during this process, healthcare professionals need to be trained to be able to conduct advance care planning conversations. 1 Internationally, these trainings can be designed only narrowly for professionals with clinical duties, mainly doctors 8 and nurses, 9 as well as interdisciplinary, open to any professionals working in the healthcare domain, such as social workers. 10 Certain programmes invest only in non-healthcare or clinical professionals, called ‘patient navigators’. 11 No guidance is given as to the background of professionals, except to the fact that they should be ‘trained’. 1
There are specific roles to be played at each moment of advance care planning, that is, when initiating or conducting it, as well as when documenting preferences. The European Association for Palliative Care 1 identified six ‘recommended roles and tasks’ that reflect this complexity: adopting a person-centred approach; having the necessary skills and being open to talk about diagnosis, prognosis, death and dying; providing individuals with clear and coherent information; possibility for non-physician facilitators to be involved in advance care planning; possibility of it being initiated in and outside of health-care settings; involving health-care providers to discuss diagnosis, prognosis, medical options. Specific studies have also looked more in depth into the issue of advance care planning professional roles. Most often, they conjugate roles and responsibilities according to the main profession of the person conducting advance care planning: nurses, 12 physicians, 13 allied health professionals, 14 care assistants, 15 social workers, 16 chaplains. 17
Throughout the literature, the role of leading advance care planning conversations is identified as a critical element of the process and requiring particular competences. As Carr et al. 18 showed, self-efficacy is statistically associated with an increased number of conducted conversations, while knowledge isn’t; this shows that practices and engagement are modelled by what facilitators think about themselves. Despite existing guidance, several studies point out the fact that many professionals identify the need to clarify their own role within advance care planning and associate this to a barrier in practicing and implementing it.6,19,20 This highlights the evermore relevance of looking into how professionals understand their roles and how these conceptions are being constructed (e.g. during training but also with experience),
Aim
Our aim was to explore how professionals who conduct advance care planning conversations perceive, define and describe their role during advance care planning (what can be identified as ‘role self-ascription’). Our focus has been exclusively on the act of conducting advance care planning, and not connected to other activities such as teaching or awareness raising.
Methods
Study design
We conducted an exploratory cross-sectional study 21 in Switzerland from November 2019 to June 2020 using semi-structured interviews.
Setting
In Switzerland, the legal adoption of binding ‘advance directives’ in 2013 created an impetus for the development of advance care planning 22 and several regional initiatives for implementation and training of professionals, especially in Zurich, 23 Lausanne,24,25 and Geneva. 26 The training is offered to ‘health and social work professionals, holding a university degree, or physicians with experience in communication with patients’. 27 Concretely, participants have come from the following backgrounds: nurses, physicians, social workers, medical secretaries, health sociologists, psychologists, chaplains, death doulas.
Participant population
Inclusion criteria consisted of (i) having received a formal training in Switzerland in the past 10 years for conducting advance care planning, (ii) having conducted at least one advance care planning conversation in Switzerland, (iii) in a Swiss national language (French, German, Italian).
Participant sampling
A purposeful sampling strategy was used. Participants were identified initially by online research of registered professionals conducting advance care planning in Switzerland, who were all (n = 13) contacted by email. Given the low number of those who accepted to participate (n = 10), more were identified among those who did training in the Lausanne area and having done at least one advance care planning conversation since (n = 8).
Participants received written and verbal information via e-mail; those interested to participate were asked to sign an informed consent form.
Data collection
We employed semi-structured interviews as a resource to access participants’ own understandings and formulations about roles. Interviews were conducted in French and German by native speakers, took place via telephone and virtually (due to COVID-19 restrictions), and were audio-recorded. Interviews in French were transcribed verbatim and those in German were transcribed directly in French. The interview guide was developed by ACS (see Supplemental Material 1). It gathered basic sociodemographic information and explored the participant’s advance care planning training and current practice, their perceptions about advance care planning and their role within it, and practices, challenges and resources related to communicating with beneficiaries during advance care planning. Participants were invited to open share their experiences and perceptions, without referring to hypothesis or expected results. It was initially tested on two individuals (not included in the sample), after which minor modifications were done.
Data analysis
Interview data was analysed with reflexive thematic analysis.28,29 Initially, ACS (a health sociologist) read the transcripts repeatedly to develop a broad sense of perceptions that facilitators have about their role. Two conversations were inductively coded by the three authors (ACS, MB, a palliative care psychologist and researcher and ERT a medical doctor specialised in geriatrics), independently and in parallel. Codes were assigned to sentences or paragraphs containing several sentences. The team compared and reviewed the codes. This stage was extremely useful in identifying aspects from the interview that relate to how facilitators perceive and experience their roles. We found that establishing a certain level of coherence at this stage was essential, particularly given our different disciplines. Then, ACS conducted an initial inductive descriptive coding of the whole data. ACS subsequently identified and grouped similar codes into broad themes, which she then then differentiated into sub-themes when relevant (i.e. when the theme contained too diverse aspects). Themes were not mutually exclusive of each other and could occur in tandem. Driven by the way in which participants talked about the topic, the themes revolved around two dimensions: (i) what are the roles of facilitators and how they are expressed or made manifest (Table 1), and (ii) the aspects that led to or characterised these roles (Tables 2 and 3). As such, the themes were ‘conceptualised as patterns of shared meaning, organised a central concept’. 29
Characteristics of study participants.

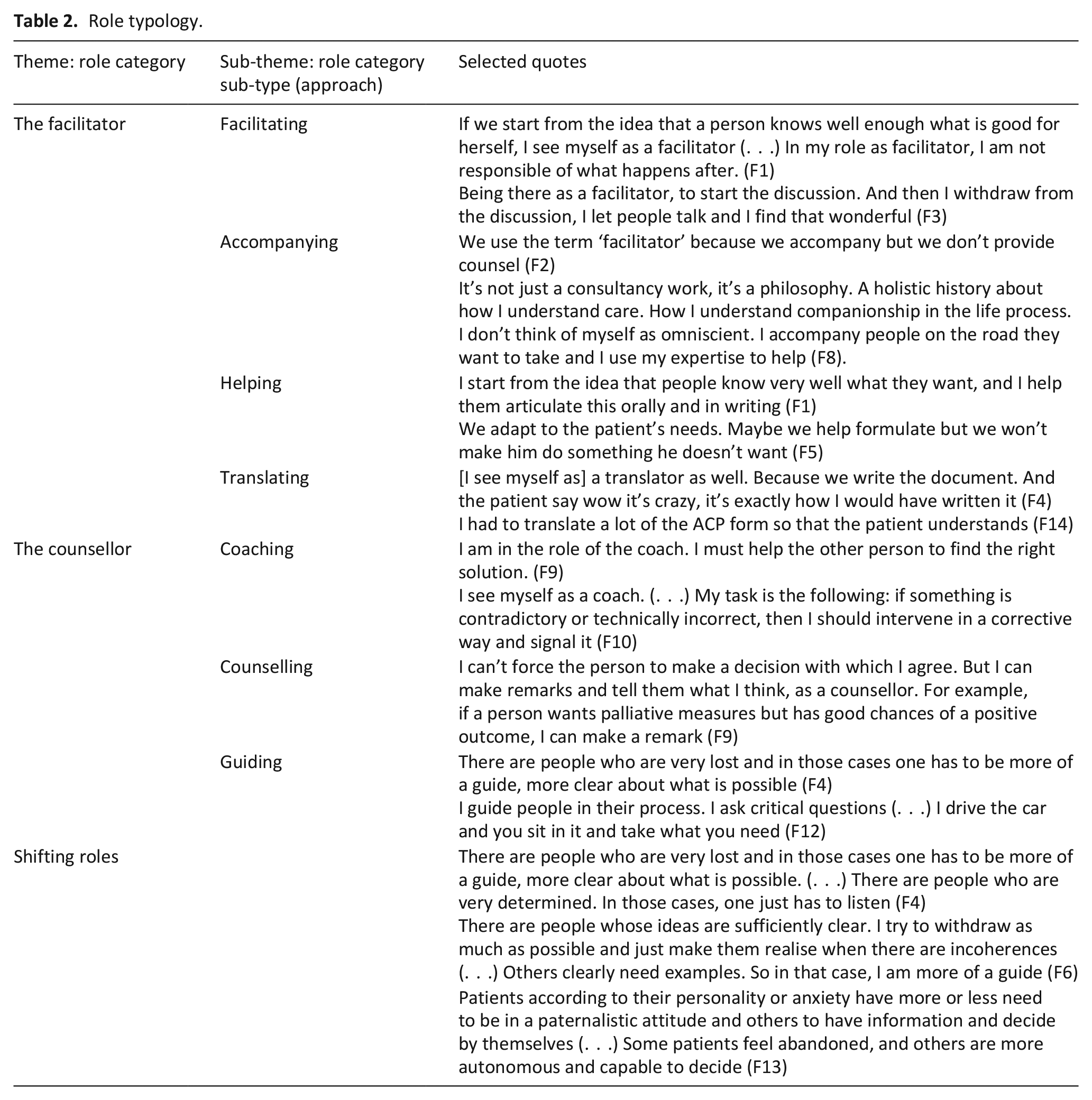
Role typology.
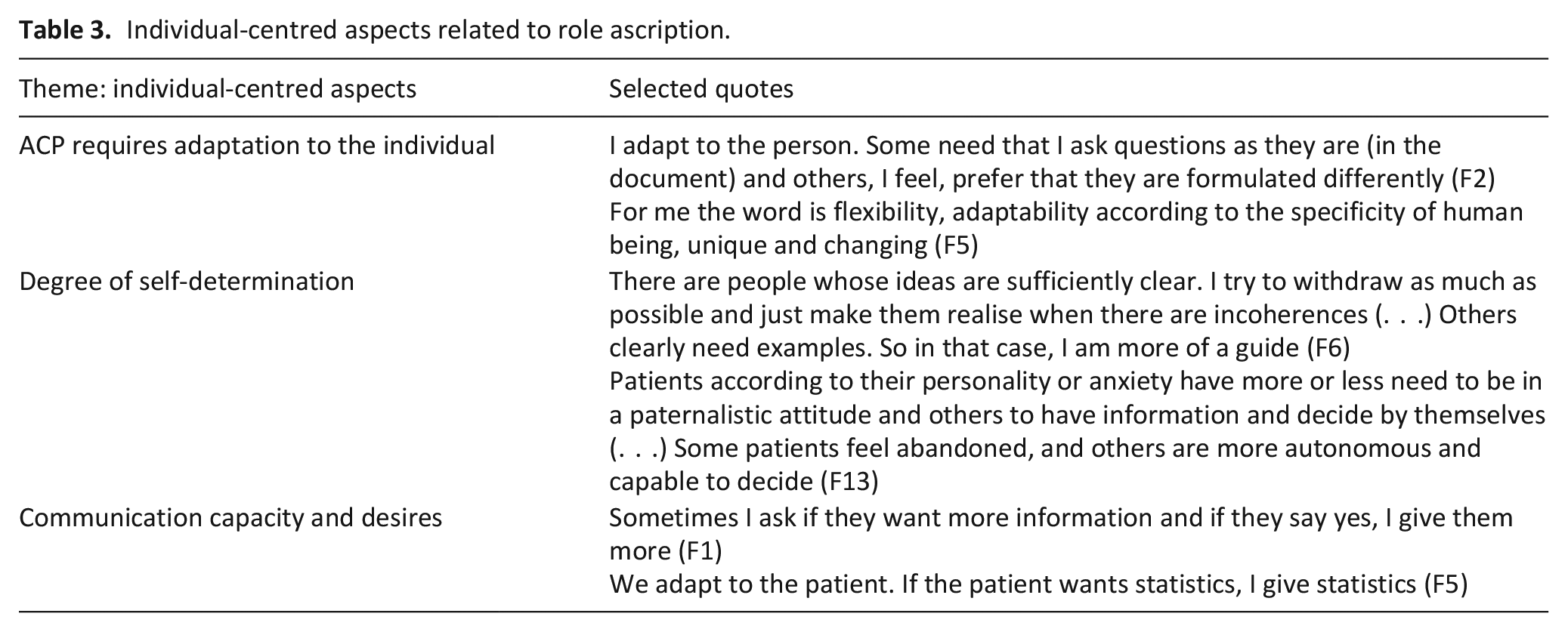
Individual-centred aspects related to role ascription.
A final coding book containing all the codes, themes and subthemes was created by ACS. Final interpretation of themes and subthemes was developed by ACS and validated with MB, RJJ (an ethicist and palliative care physician) and ERT. Throughout the process, only information relevant to the objective of the study was coded and interpreted. Coding, theme and subtheme development and interpretation was done in French. The themes, sub-themes and quotations used in this paper were translated from French to English by ACS. We adhered to the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist, 30 that we adapted to the specificities of our methodology, 29 to ensure comprehensive and transparent reporting.
We follow the structural symbolic interactionism approach, developed at the convergence of two different way of understanding professional roles.31,32 Structuralists understand roles as essentially fixed positions embedded in the social structure, while symbolic interactionists consider roles as negotiated understandings between individuals and relying on subjective perceptions, therefore always potentially fluctuating. The structural symbolic interactionism approach recognises that professional roles do tend to become institutionalised and that this imposes structural constraints upon them. However, in analysing professional roles, it also recognises the significance of role meaning and perception which influences how roles are enacted and how identity is created.31,32 This led our analysis to closely consider how facilitators translate their understanding of what advance care planning requires (the institutional frame) into a stance and set of actual activities (their roles). We refer to ‘role self-ascription’ to recognise the fact that roles are not (solely) those conveyed by the training but are something that professionals build themselves and develop in consideration to their own practice.
Results
Of 18 identified participants, 14 agreed to participate. They reflect four different professions, both clinical and non-clinical, participated to the study. Table 1 details their characteristics.
Interviews lasted 49 min (mean).
We identified three themes: (1) role typology; (2) individual-centred and (3) professional-centred aspects related to role ascription. All themes and sub-themes are detailed in Tables 2 to 4.
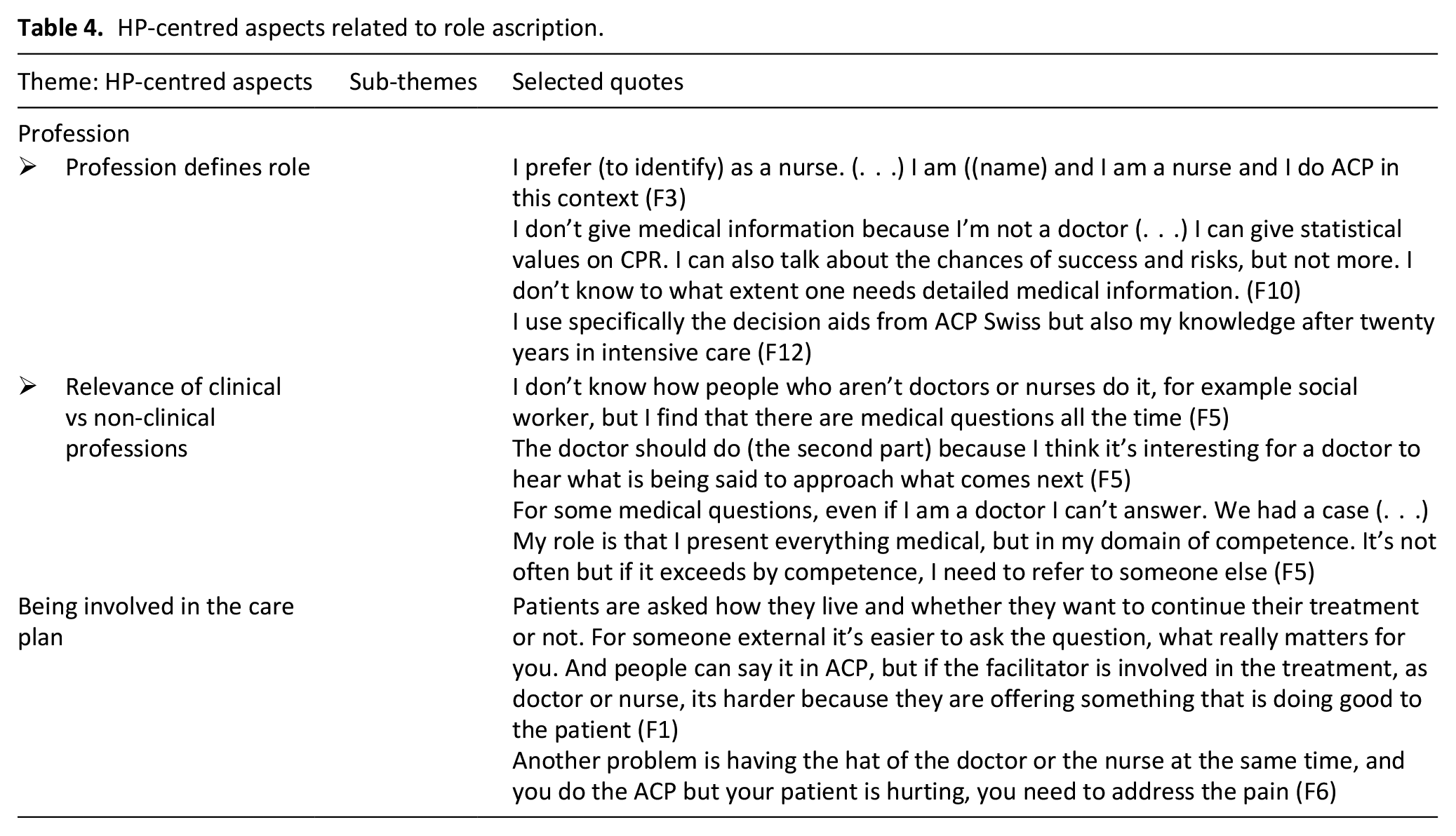
HP-centred aspects related to role ascription.
Theme 1: Role typology
Participants referred to a variety of roles and often to a combination of roles. We identified two overarching role categories: facilitators and counsellors (Table 2), each defined through particular approaches (sub-types) in terms of how communication takes place with patients. The names of the categories were derived from the sub-type that englobed the others.
‘Facilitators’ bestow a complete focus on individual’s autonomy in decision making; they understand their mission as being to empower people to engage in decision-making by offering neutral and complete information and respecting their decisions (‘it’s a philosophy. A holistic history about how I understand care. How I understand companionship in the life process. I don’t think of myself as omniscient. I
‘Counsellors’ recognise their mission as being more directive than that of the facilitator; they give selective information relative to the medical situations and interventions in a way that is considered as relevant for the person, and inform people of what is medically indicated or not (‘I must help the other person to find the right solution’, F9). The counsellor role was also described as related to constructive questioning of individual’s decisions when these don’t reflect their preferences or when they refer to medically irrelevant acts. Keywords associated to this role category comprise of ‘to counsel’, ‘to guide’, ‘to support’, ‘to coach’, ‘to consult’.
This typology is, however, conceptual, since all but one participant referred to endorsing roles from both categories and being, at times, ‘facilitators’, and at others, ‘counsellors’, according to the situation. For example, one participant said, when describing her role, that ‘There are people who are very lost and in those cases one has to be more of a guide, more clear about what is possible. (. . .) There are people who are very determined. In those cases, one just has to listen’ (F4). This highlighted the dynamic of the situation and the adaptability that advance care planning professionals need to show when endorsing their role to certain factors (that are explored as theme 2 and 3).
Theme 2: Individual-centred aspects related to role ascription
Professionals referred to the fact that their role fluctuates according to the individual (Table 4).
Generic adaptability to the needs of the person was a pre-requisite mentioned by several participants (‘I adapt to the person. Some need that I ask questions as they are (in the document) and others, I feel, prefer that they are formulated differently, F2). Two other aspects in particular were noted. Firstly, the person’s personal ‘degree of self-determination’, that is, to what extent they understand their health situation, have reflected about medical options, and have already made choices. People who have already positioned themselves and are knowledgeable about medical technology and their health situation don’t require much advice but rather a support to translate and transcribe wishes, while those who are less knowledgeable and undecided or haven’t thought of the subject require more active guidance and counselling (‘There are people whose ideas are sufficiently clear. I try to withdraw as much as possible and just make them realise when there are incoherences (. . .) Others clearly need examples. So in that case, I am more of a guide’, F6). Second, the professional’s role was also dependent on the person’s ‘communication capacity and desires’, that is to what extent they welcomed and requested certain information, as well as their ability to process it (‘We adapt to the patient. If the patient wants statistics, I give statistics’, F5).
Theme 3: Professional-centred aspects related to role ascription
Professionals also referred to intrinsic aspects that define their role (Table 4).
Participants referred to their ‘main profession’ as bearing weigh on their role. For some, their clinical defined their role during the advance care planning, as they drew on knowledge and attitude particular to that profession (‘I prefer (to identify) as a nurse. (. . .) I am ((name)) and I am a nurse and I do ACP in this context’, F3). One participant found that not being a clinician might impact the role in advance care planning, for example about what information they can (or cannot) give to the person (‘I don’t know how people who aren’t doctors or nurses do it, for example social worker, but I find that there are medical questions all the time’, F5). Certain professions were considered more competent to conduct advance care planning, such as being a clinician or a medical specialist. Another aspect was related to ‘being involved in the care plan’ of the person. Here, participants noted the challenges of ‘double hatting’ (being the patient’s treating doctor and doing an advance care planning with them): individuals might be less adamant to refuse treatments that facilitators suggest, and facilitators need to prioritise symptom management, which might be disruptive for advance care planning.
Discussion
Main findings
This study provides evidence about how professionals self-ascribe their role within advance care planning discussions by exploring accounts of how they perceive, define and describe it. Participants provided rich accounts of their stance, which confirms that professionals feel the need to better define their roles within the process.6,19,20
What this study adds?
Our findings highlight that roles fluctuate according to various dimensions but can be aggregated in two overarching categories, ‘facilitators’ and ‘counsellors’. ‘Facilitators’ consider people as experts and knowledgeable about what is relevant or not in terms of medical risk-taking, whereas ‘counsellors’ undertake a more custodial role, and design information and explanations in a way that explicitly describes what is medically relevant. While facilitators put the onus on autonomous decision-making (prioritising the person’s right to document their choice independent of medical indications), counsellors focus more on informed decision-making (prioritising the person’s need to receive information that is personalised and a clear explanation of what is medically indicated).
This dual polarisation is by far not representative for most participants, who rather referred to their role shifting dynamically between these two categories, showing that role borders are permeable and that they juggle with a dual attitude. Role ascription is anchored in what the individuals themselves make relevant as needing, as well as in the identity and position of the professional themselves. Professions were deemed important to the point to which some participants didn’t initially acknowledge endorsing another advance care planning -specific role than that of their clinical professions. Professionals who do advance care planning with their patients experience certain challenges in maintaining their role (and continuing advance care planning) when patients had symptoms in need of tending. All this shows that competences and stances from main professions overflow the role of professionals. This begs the question of to what extent certain desirable competences for advance care planning professionals are found within specific professions, and, more globally, of the place of communication as professional competence. 33 For example, prior evidence shows that some of the barriers encountered by professionals concern the fear of depriving patients of hope by way of presenting options, 34 which is a core skill for initiating end-of-life discussions. While a call has been made for advance care planning research to focus more on the ‘diversities and variations between people’, it is implicit that there is equally a need to address how facilitators face diversity and adapt to it. 35
Role fluctuation can be challenging, since it requires a lot of adaptation and flexibility. Role boundaries are permeable, with specific practices or activities being conjugated in a way that tend more towards one role than another. It also means that professionals don’t have a unique professional identity associated to advance care planning, which might make their experience more complex.
Implications for practice
Thinking about role specificity is the only way to identify appropriate resources for professionals. Training can directly address the issue of role ascription and the link between original profession and advance care planning role. Ibarra and Obodaru 36 highlight, to this regard, the importance of the concept of ‘liminality’, that is, the experience of role transition, or rather when a person feel ‘betwixt and between’ roles. Ibarra and Obodaru argue that liminal experiences can be more or less institutionalised, and, in particular, that under-institutional liminal experiences are subjectively more challenging for individuals (because they have less guidance and support) but have a greater potential for identity growth (since they allow more room for individual agency and creativity). More research is necessary to explore dimensions such as shifting from professional roles to ACP roles as well as shifting between the typologised ACP roles.
Strengths and limitations
This study explores how professionals self-ascribe roles during advance care planning discussions, a topic that has been under-researched. Its strengths reside in the diversity of participants (clinicians and one non-clinician), and in the inductive approach used for data analysis, that allowed to be faithful to participants’ experience. This study also has limitations. Firstly, a greater number of participants would have allowed to reach a more granular analysis. Indeed, role flexibility generates a diversity of patterns in which participants would experience and understand their roles. Furthermore, we only captured participants’ subjective point of view, but we acknowledge that a more naturalistic approach would be more informative (e.g. relying on recorded advance care planning conversations) to develop an understanding of role dynamics. Only one of the participants was not a clinician. Since profession seems to be an important factor in role ascription, important questions related to the relevance of the clinical background are eschewed. Finally, the sample size of healthcare professions other than nursing (4/14) is too small to generalise with confidence. However, given that ACP is overwhelmingly done by nurses in the jurisdiction from which the participants were drawn, this somewhat mitigates the concern.
Conclusions
Roles that professionals undertake during advance care planning encounters can be aggregated in two overarching categories, ‘facilitators’ and ‘counsellors’, according to whether they prioritise autonomous decision-making or informed decision-making. In practice, however, roles fluctuate between these two categories, according to individual-related aspects (to what extent the person is informed and eager to engage in autonomous decisions, and what their communication capacity and desires are) or professional-related aspects (their clinical or non-clinical profession and their involvement in the individual’s care plan). This means that advance care planning requires professionals to be very adaptable and flexible throughout the process in order to identify the role that they can invest in each situation. Additionally, our results also show that the professionals themselves distinguish between the roles of facilitator and counsellor, which has ethical implications in terms of responsibility. Training and further research need to take into consideration this complexity and address it explicitly.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163251331168 – Supplemental material for Role self-ascription of professionals conducting advance care planning conversations: A thematic analysis
Supplemental material, sj-docx-1-pmj-10.1177_02692163251331168 for Role self-ascription of professionals conducting advance care planning conversations: A thematic analysis by Anca-Cristina Sterie, Mathieu Bernard, Ralf J Jox and Eve Rubli Truchard in Palliative Medicine
Footnotes
Acknowledgements
We thank the study participants for sharing their experiences and the team of the Service of palliative and supportive care and of the Chair of geriatric palliative care of the Lausanne University Hospital for their support before, during and after the piloting of this study.
Consent and data sharing
All participants provided oral and written informed consent.
Data availability
Transcripts may be available from the first author upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: For this study ACS was awarded the Käthe Zingg-Schwichtenberg fund of the Swiss Academy of Medical Sciences.
Ethical approval
Ethical approval was received from the regional Ethics Committee (2020-01922).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.