
Abstract
Background:
To achieve benefits of person-centred outcome measures within routine children’s palliative care, implementation plans and the intended pathways to impact must be established.
Aim:
To develop a Theory of Change and Implementation Plan for sustained implementation of a novel person-centred outcome measure into routine hospital care for children with life-limiting conditions and to identify potential causal mechanisms.
Design:
Participatory workshops and a directed content analysis developed a Theory of Change. Framework analysis of workshop qualitative workshop data, supported by Normalisation Process Theory Informed an implementation plan.
Setting/participants:
Health and social care professionals and parent/carers were recruited to six online workshops through social media and networks.
Results:
Eight health and social care professionals and eight parents participated. The Theory of Change identified overall impact of improved care and quality of life, through improved identification of symptoms and concerns and improved communication between healthcare teams. However, for this to happen, education and training on the outcome measure, anticipated benefits, how to implement and use it are required. Logistical, resource and staffing barriers must be addressed, alongside the development of a detailed implementation plan. Analysis of workshop transcripts identified seven themes relating to the domains of Normalisation Process Theory: education and information needs, the importance of a tailored approach, stakeholder engagement and the role of champions, healthcare records and IT system support requirements, improved health outcomes, improved experience of care and evidence for service provision, development, evaluation and expansion
Conclusion:
Future work should pilot test the Theory of Change and Implementation Plan.
Keywords
Whilst person-centred outcome measures have been shown to improve the quality of care and patient outcomes in adult palliative care when successfully implemented into routine care, this has not been achieved for children and young people.
It is essential to identify the causal mechanisms underpinning implementation and normalisation processes through which a novel child and family-centred outcome measure may achieve its intended impact, through the perspectives of stakeholders.
A Theory of Change map was developed which explains the causal pathway for successful implementation of outcome measurement in children’s palliative care, including how short-term outcomes and long-term impacts may be achieved.
The use of Normalisation Process Theory enabled novel understanding of implementation and normalisation of person-centred outcome measures into routine care.
An implementation plan was developed to operationalise the strategies for implementation and normalisation of the C-POS:UK into routine care.
Theory of Change and Implementation Plan can be used to support the implementation of outcome measurement into routine care.
Health and social care professionals and parents both described great potential for person-centred outcome measures to have a significant positive impact on health outcomes and experience of care for children with life-limiting conditions and their families.
Future research should aim to assess the Theory of Change for transferability to support implementation and normalisation of person-centred outcome measures in routine care for children with life-limiting conditions in further contexts.
Background
Children and young people (hereafter ‘children’) with life-limiting and life-threatening conditions (hereafter ‘life-limiting’) experience burdensome symptoms and concerns requiring a holistic, person-centred approach.1,2
Person-Centred Outcome Measures are standardised questionnaires that assess effects of a health condition or treatment on patients, and/or their family. 3 They are usually self-completed or, when the patient is unable, proxy-completed.3,4 Their use can empower patients and families to raise concerns with clinicians, and support conversations and decision-making through shared language5,6; improving quality of care and outcomes.7,8 Despite a growing body of evidence on use and implementation of Person-Centred Outcome Measures in adult palliative care,3,4,9 –11 evidence to underpin their use and implementation for children with life-limiting conditions is limited.3,12 –14 Children with life-limiting conditions, their families and healthcare teams anticipate benefits of using such measures in care, 15 including strengthening health and social care professionals’ (hereafter ‘professionals’) understanding of what matters to patients and families, improved communication and collaboration between families and healthcare teams, improved communication and collaboration between professionals and standardised data collection and reporting. 15
The Children’s Palliative care Outcome Scale: UK version (C-POS:UK) project aims to develop,1,16 –23 validate23,24 and implement15,22,25,26 a novel child- and family-centred outcome measure for use in the care of children with life-limiting conditions in the UK. However, to realise the benefits of C-POS:UK in care, implementation must be carefully considered,9,11 including the causal pathway,9,11 and mechanisms to sustained implementation and normalised use.
This study aimed to develop a Theory of Change and Implementation Plan for sustained implementation of C-POS:UK into routine hospital care for children with life-limiting conditions and to identify potential causal mechanisms.
Methods
Research questions
RQ1: What is the Theory of Change underpinning C-POS:UK implementation?
RQ2: What are the potential causal mechanisms underpinning sustained C-POS:UK use?
Design
This observational study used a participatory Theory of Change approach 27 informed by the Medical Research Council Guidance for developing and evaluating complex interventions. 9 Theory of Change workshops were conducted, informed by evidence from a systematic review on implementing Person-Centred Outcome Measures in paediatric healthcare 25 and findings from interviews with stakeholders (including children with life-limiting conditions, their parents and siblings, health and social care professionals and planners of paediatric palliative care services). 15 The prototype visual Theory of Change was reviewed in consultation with a Young Person’s Advisory Group and study steering group to form a final Theory of Change Map. To identify the key mechanisms underpinning sustained use, a second phase of qualitative analysis was conducted informed by Normalisation Process Theory.28,29 The methods for developing the Theory of Change are detailed in Figure 1.
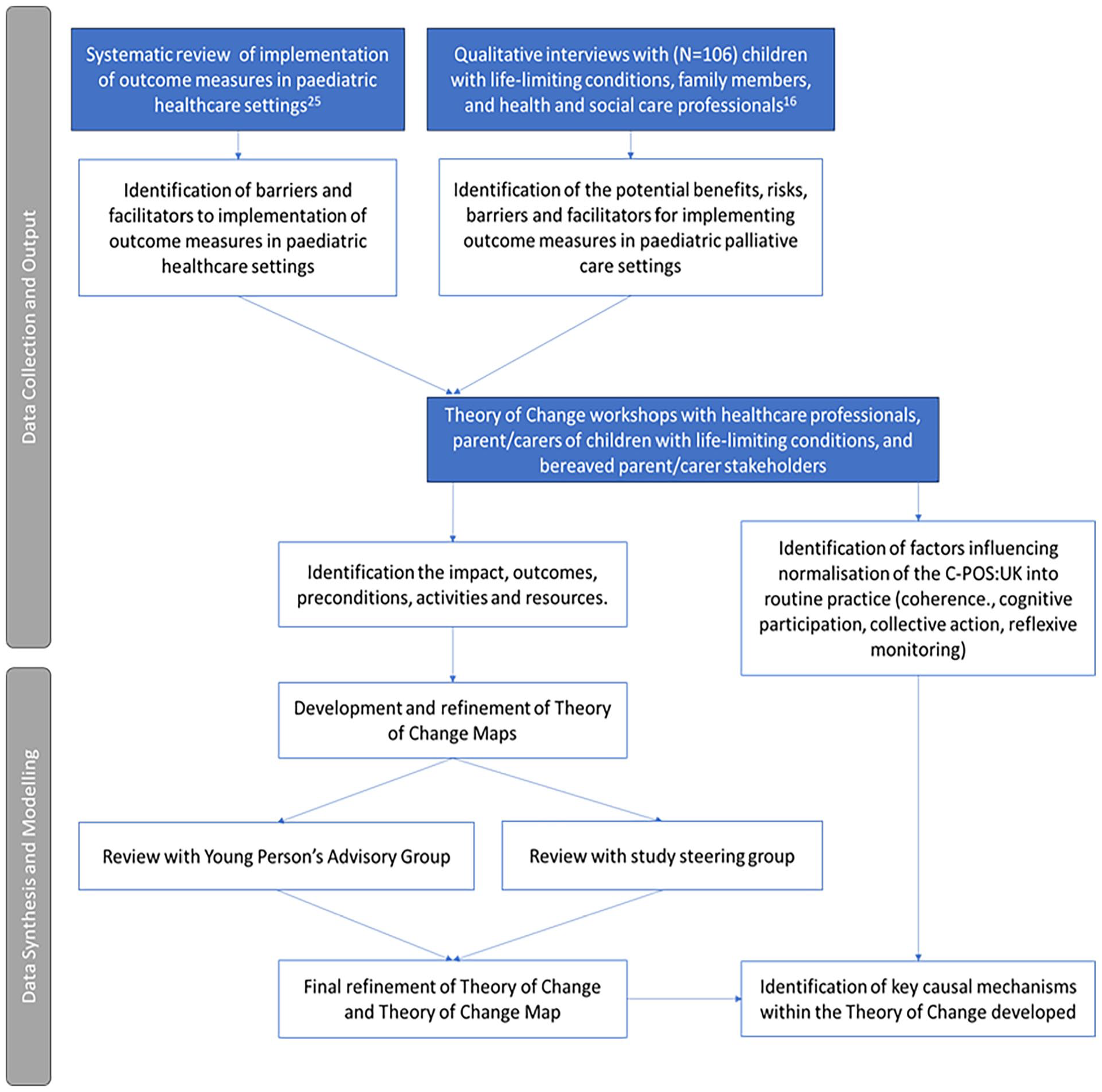
Diagram of information sources and synthesis process for developing the Theory of Change for the implementation of C-POS:UK.
The development of the Theory of Change is reported in line with Breuer et al.’s Theory of Change reporting checklist. 30 Patient and Public Involvement with the Young Person’s Advisory Group is reported as per the Guidance for Reporting Involvement of Patients and the Public (GRIPP2) short checklist. 31 The second phase of Framework analysis is reported in accordance with the consolidated criteria for reporting qualitative studies (COREQ). 32
Population
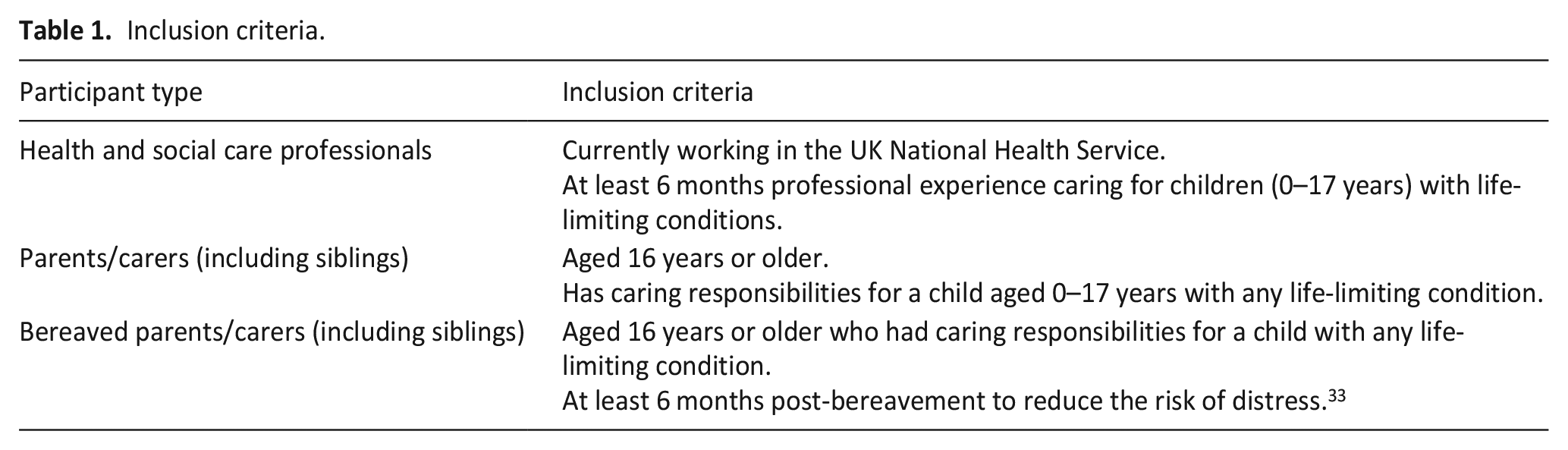
Inclusion criteria for participants are reported in Table 1.
Inclusion criteria.
Sampling and recruitment
Sampling was a combination of purposive (stakeholders targeted on the basis of being a parent/carer or bereaved parent/carer of a child with a life-limiting condition or being a professional working in the NHS caring for children with life-limiting conditions 34 ) and convenience (social media as this is useful to access ‘hard to reach’ or ‘hidden’ populations in health research35,36).
Study advertisements (developed with the steering group) were disseminated through social media, mailing lists of a paediatric palliative care professional association and a family support non-governmental organisation, and through the steering group’s networks. Stakeholders who responded were screened for eligibility by HS.
Data collection
Theory of Change workshops were held March–May 2023. Separate workshops were held for professionals, parents/carers and bereaved parents/carers to reduce the impact of power imbalances. 37 Workshops for professionals were conducted asynchronously, on the online platform Basecamp 38 providing discussion boards for participants to read and contribute in their own time. 39 Workshops for parents/carers and bereaved parents/carers were conducted on MS Teams in small groups whereby participants and facilitators could see each other and interact in real time both verbally and through the chat function. Two workshops were held for each stakeholder group and participants could choose to attend one or both workshops.
The workshop topic guide was developed using findings from a systematic review 25 and qualitative interview data 15 in collaboration with bereaved parent Patient and Public Involvement study members. The workshops followed a structured format informed by STRiDE guidance 40 with adaptations to support participation 37 that is, shorter small group workshops to better accommodate parent/carers balancing caring responsibilities and to provide greater privacy. ‘Live’ delivery enabled the research team to provide real time support if needed. Workshops were asynchronous for professionals to maximise engagement alongside clinical demands.
The Theory of Change development used ‘backwards outcome mapping’, identifying the impact/long-term goals of implementing C-POS:UK then working backward to medium and shorter-term outcomes, preconditions and activities/resources that may be required. 40 HS analysed the data to develop preliminary Theory of Change maps for each group which were presented for further discussion and refinement in the second workshops. The Young Person’s Advisory Group and steering group were consulted to further review the Theory of Change map and inform development of implementation strategies.
Data analysis and integration
Workshop audio-recordings, and forum discussion boards were transcribed verbatim and pseudonymised, then analysed by HS using directed content analysis. 41 A deductive coding framework was developed, informed by elements of Theory of Change.
The second phase of analysis applied a Framework analysis. 42 Transcripts were inductively coded42,43 by HS and IG using NVivo 12. Interpretation was performed by HS by mapping the data to the domains of Normalisation Process Theory.28,29 Themes were then mapped onto the Theory of Change map and an Implementation Plan developed, reported in line with Proctor et al.’s recommendations for specifying and reporting implementation strategies. 44
Findings were presented to the steering group (academics, researchers, advocates and professionals) to agree upon key strategies for the implementation plan. We also consulted a Young Person’s Advisory Group at a UK tertiary children’s hospital. 45 Members were aged 13–24 years, with chronic health conditions, their siblings and young people interested in a career in healthcare or research. An age-adapted version of the Theory of Change map was developed for the consultation workshop. Members of the group were asked to provide feedback on the map content (what the most important elements were, if anything was missing).
Ethical approvals and consent
Ethical approval was granted by King’s College London (HR/DP-22/23-33702). All participants provided written informed consent.
Results
Sample characteristics
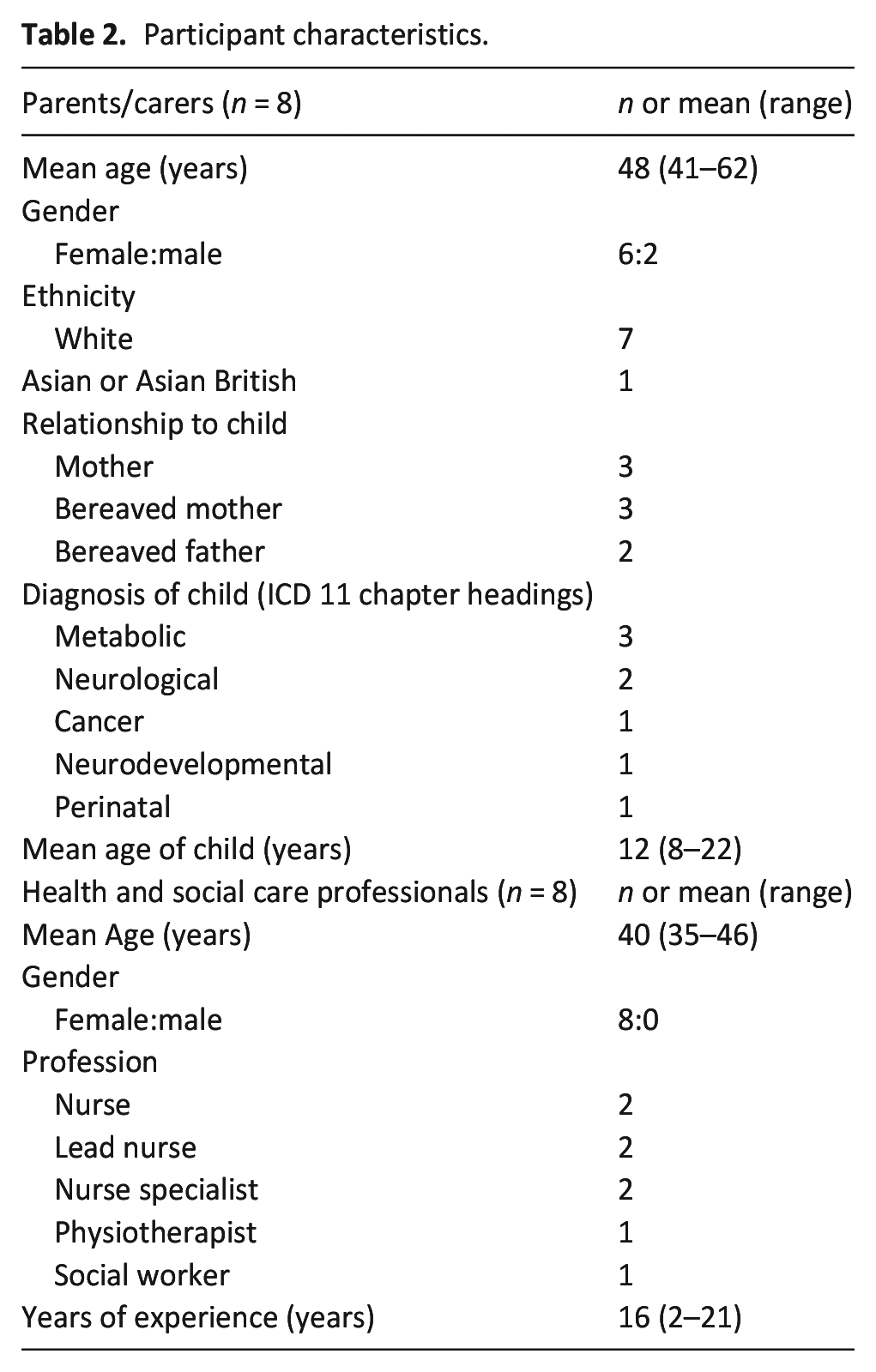
Six workshops were conducted with a total of 16 participants. Demographic characteristics are reported in Table 2.
Participant characteristics.
Theory of change for implementing C-POS:UK
The Theory of Change map is presented in Figure 2.
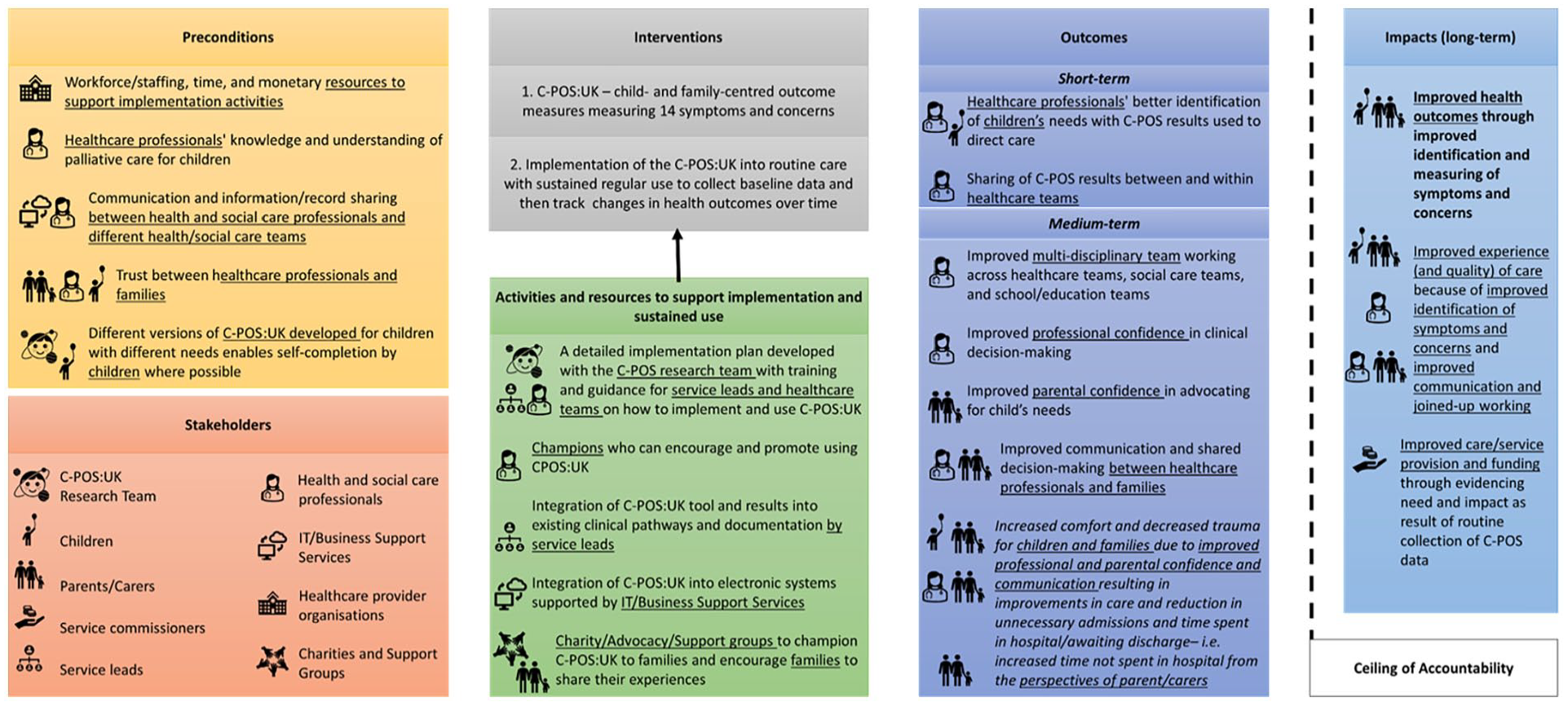
Theory of change map for implementation and routine use of the C-POS:UK into paediatric palliative care provided in UK National Health Service hospitals.
Impact
The anticipated long-term impact of implementing C-POS:UK was improved health outcomes due to better identification of symptoms and concerns. Professionals felt implementation of C-POS:UK would facilitate person-centred care and all participants reported that it could lead to improved experiences and quality of care. Professionals and parents suggested that the data collected from C-POS:UK could be used to evidence need and support service development/expansion at a commissioning level. Long-term impacts do however have a ceiling of accountability, due to other influencing factors.
Outcomes
Short-term outcomes
Short-term outcomes included improved identification of children’s needs due to integration of into routine care, including sharing of C-POS:UK results between services. This, however, requires integration into existing clinical workflows and infrastructure.
Medium-term outcomes
C-POS:UK could provide professionals an understanding of what was important to families, improving shared decision-making. Parents felt it would support them advocating for their child’s needs and lead to improved collaboration with professionals. Parents felt that C-POS:UK could provide evidence of the child’s ‘baseline’ or ‘normal’ symptoms, giving professionals more confidence in making the decision to discharge, even with complex symptoms. This may reduce unnecessary time spent in hospital, leading to improved quality-of-life.
Preconditions
Preconditions for successful implementation included adequate staffing, time, education/training needs and monetary resources. Parents reported that it is essential for all professionals (particularly those who are not paediatric palliative care specialists) to have an understanding of the speciality so that they have confidence to introduce and use the measure.
Electronic and paper-based versions of C-POS:UK are needed to accommodate differing needs and abilities of children, enabling them to self-report.
Parents felt that communication and information sharing between healthcare teams and services needed improvement before C-POS:UK was implemented (potentially though shared patient records), to avoid families having to re-complete C-POS:UK. A close, positive working relationship between families and professionals was identified as an important prerequisite.
Activities and resources
Professionals recognised that implementing C-POS:UK would bring challenges but identified mitigating resources and activities. These included carefully planned clinical pathways, and a robustly developed implementation plan detailing families’ requirement that it is used flexibly in response to changing needs and family preferences.
Professionals felt incorporating C-POS:UK into existing tools (e.g. Child and Young Person Advanced Care Planning tools, 46 Child and Family Wishes discussion tools 47 ) and incorporating guidance into existing documentation may achieve seamless integration. Prompts and reminders when C-POS:UK is first implemented may also support integration. Professionals identified the need for IT system/business support to enable C-POS:UK to be integrated into electronic systems. Parents felt it would be important to involve charity/advocacy/support groups to help champion C-POS:UK with families, explain its benefits and encourage use.
Review with study steering group
Twenty-four members attended the review meeting – 15 professionals (6 consultants, 7 nurses and 2 physiotherapists), 5 research team members and 4 clinical academics. To optimise implementation, attendees suggested the requirement to first get buy-in at an organisational level, then engage with service leads, then individual professionals and families. Attendees also recommended champions to encourage and promote C-POS:UK use. Training and education on how to implement and use C-POS:UK in practice was also identified as important, alongside ensuring C-POS:UK can be integrated into existing clinical pathways and systems.
Consultation with a Young Persons Advisory Group
Thirty-one young people (19 female and 12 male) aged 13–24 years attended an online meeting in July 2023. All members reported that the Theory of Change map was comprehensive. However, they stressed that C-POS:UK should be implemented and used flexibly to best enable children to self-report. Members also proposed that sharing of C-POS:UK data should go beyond the hospital setting to include other healthcare teams and teaching/education providers in the community.
Framework analysis main findings
Seven themes were identified across the four domains of Normalisation Process Theory: coherence, cognitive participation, collective action and reflexive monitoring to sustain implementation. The themes are described in the text below and Figure 3 shows themes mapped onto the Theory of Change.
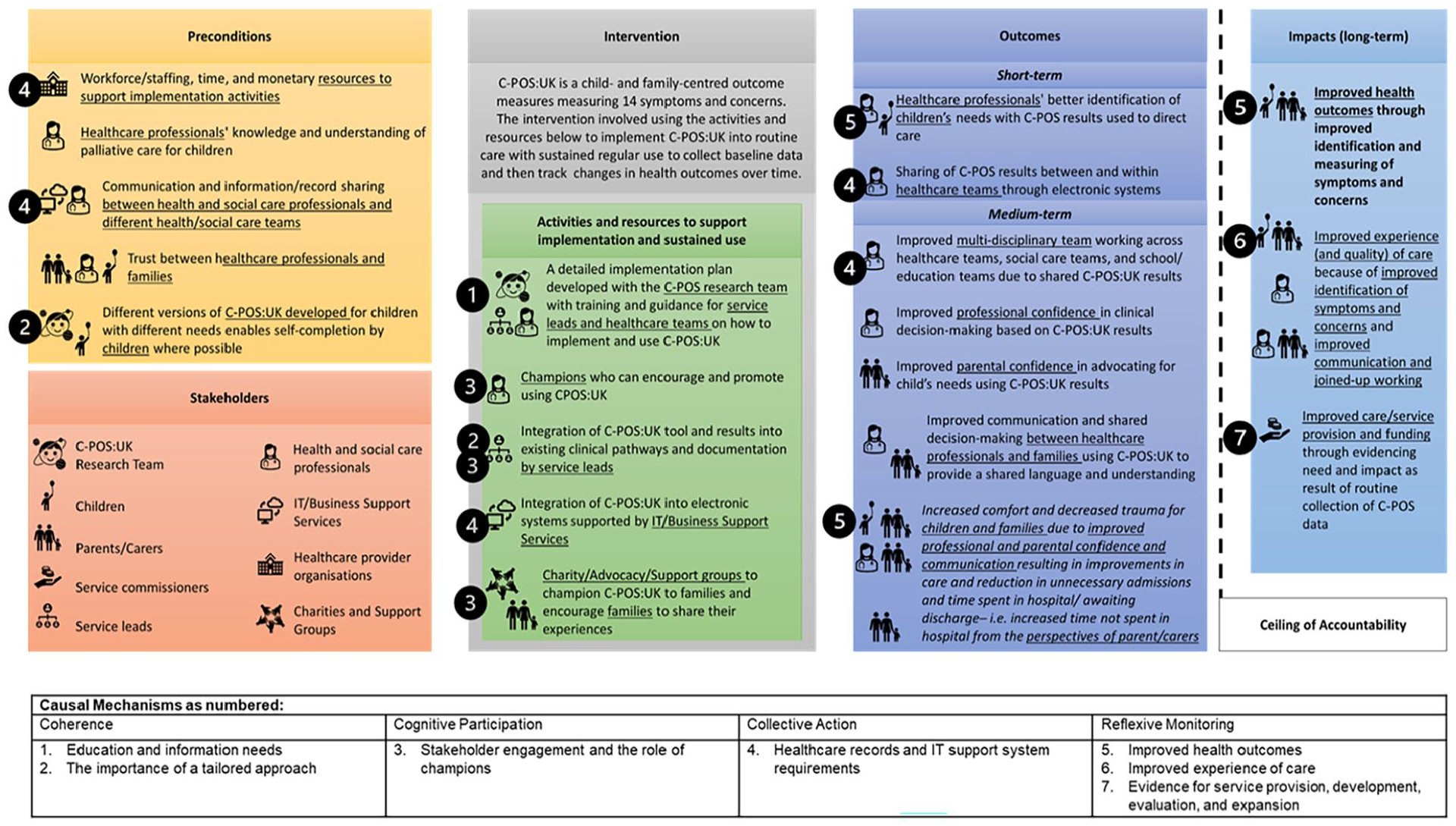
Theory of change map for implementing the C-POS:UK into routine paediatric palliative care within hospitals with key causal mechanisms underpinning implementation and normalisation mapped.
Coherence
Theme 1: Education and information needs
All participants discussed education and information needs. Professionals’ needs related to practical aspects, for example, understanding fit within existing clinical workflows and when/how it should be completed. Professionals proposed providing a plan for initial implementation and guidance for incorporation into existing documentation. Family needs related to understanding what C-POS:UK is and benefits of use.
All stakeholders need to know the purpose and importance of the C-POS. Clinicians and families need to know how to complete the C-POS. Clinicians need to know how to record the [completed C-POS results] on the electronic patient record. – HSCP10 Implementing change is always tricky but if a clear clinical pathway was implemented on how to do this it would be less challenging. – HSCP12 I think here it’s all about the why, so why are you asking people and what benefit is it going to have and I think that’s that needs to be really dealt with. – PARCAR8
Theme 2: Importance of a tailored approach
Professionals felt C-POS:UK could be used routinely during existing review meetings to support better identification of changing needs.
Ideally it would be used on a semi-regular basis (during annual reviews or other important meetings) in order to direct care appropriately in relation to changing outcomes. – HSCP9
However, both professionals and parents emphasised C-POS:UK should be used flexibly due to changing needs, with more frequent use if a child became unstable.
As we all know, each family is different [. . .] Mandating a frequency for completion is unlikely to be in keeping with the preferences of families and may actually be detrimental to their outcomes. – HSCP9
Some parents felt there was a specific professional they had a close relationship with that may be most appropriate to compete C-POS:UK with. The professional may be different for each family and may change over time.
for us that was definitely who we saw the most of erm and a real relationship was built up [. . .] because they were seeing you on a weekly basis whereas consultants you know could be every six months perhaps three but it’s over many years you do build a good relationship but it is a less week-on-week thing erm but as I say it that does seem to work differently everywhere in the country – PARCAR6
Parents and professionals also discussed the importance of having electronic and paper-based versions of C-POS:UK, for children with different needs or abilities.
and different ways of completing it you know [. . .] because he’s deaf but he can hear some stuff with something that was visual that he was able to rate or he could do it on an iPad. – PARCAR1
Cognitive participation
Theme 3: Stakeholder engagement and the role of champions
Professionals and parents highlighted the importance of engaging stakeholder groups and proposed identifying champions. Champions would likely be professionals who could drive implementation, educating and training other professionals on how C-POS:UK may support care provision, demonstrating its use with patients and families and providing prompts/reminders.
I think that by having professionals who are passionate and competent about the benefits of using the [outcome measure] to educate and train teams in use of it should help to address any barriers of reluctance in incorporating it into the core tools used with this service user group. – HSCP4
For parents, understanding why they were being asked to complete more paperwork was felt to be key to motivating families. Hearing the benefits from other parents and through family support groups were felt to be effective ways to develop a community around its use.
if they have another parent saying to them use this it is a lifesaver they will go for it [. . .] how it works and why it works well and sort of share our experiences about it – PARCAR9
Collective action
Theme 4: Healthcare records and IT support system requirements
Parents felt that C-POS:UK results could be kept as part of healthcare records or passports to facilitate sharing. However, professionals noted where services were not all using the same digital systems, this may complicate sharing of C-POS:UK results.
her folder had her symptom management plan, advanced care plan, um her standard care plan and her [Medication Administration Record] charts for all the different drugs she took and er escalation protocols for anything like dystonic episodes, etc. etc. It was all there in one place. Um so a tool like this in there would’ve been fantastic as well. – PARCAR3 Having shared records that all professionals that have consent to access can access as some providers are not even digital, communication is the key to everything being successful – HSCP12
Professionals recognised potential challenges to integrate C-POS:UK into online infrastructure, and the need for IT system support
Anything that requires the developers of the electronic patient record to make changes at the developers’ side [may be a challenge]. [. . .] We have identified an issue with another outcome measure which requires the [IT system] developer to make a change at their end; we have been asking for the change for several years. – HSCP10
Reflexive monitoring
Theme 5: Improved health outcomes
Professionals and parents felt implementation and regular use of C-POS:UK in care would support better identification and management of symptoms and concerns, leading to improved outcomes.
The ultimate goal would be to improve health outcomes of care by identifying what will make a positive impact on our patients and their families. – HSCP2 hopefully their wellbeing or comfort will have increased as a result of there being some measurable data to assess the situation against – PARCAR2
Theme 6: Improved experience of care
Professionals expected that C-POS:UK use would improve experiences of care by supporting a person-centred approach.
The measure will help us to identify outcomes that are important to children/young people and their families and working to improve those outcomes will almost certainly improve their care experience – HSCP9
Improved care experiences may be achieved through a shared understanding of what was most important to improve shared decision-making. Parents described how having data from C-POS:UK would support them to advocate for their child’s needs, and lead to greater collaboration between families and professionals.
yeah I think what this would do this would encourage that collaborative approach in care from the parent carers and from the clinicians which they all strive to do and in theory it should breakdown those barriers so there’s going to be no unnecessary confrontations which I think is going to be really cool actually – PARCAR8
Theme 7: Evidence for service provision, development, evaluation and expansion
The collection of routine, standardised data that was also seen as beneficial by both parents and professionals. Parents felt the availability of data would provide evidence of need and better enable children and families to access services and support.
I wonder if that connected or produce reports they could use, because I remember when we finally said yes we want to have carers at home at night because we are not sleep. It was a real big headache to get it all together and it was all the actual medical information and we again had to resort to our known nurses and the people that really know us that say that they’re exhausted and really need this help and [child’s] condition is really really really severe – PARCAR9
Professionals recognised the potential impact at a service or system level, as data could provide evidence of need to help direct development or expansion of services.
If effective the implementation could provide evidence for service development and expansion to ensure outcomes improve for patients and families – HSCP7
Implementation plan
From the Theory of Change workshops, review with the Young Person’s Advisory Group and study steering group, and analysis of the workshop transcripts, an implementation plan was developed. It is formed of strategies to achieve the potential key causal mechanisms identified. The plan was developed using Normalisation Process Theory to ensure both initial implementation and sustained use. The strategies reported in Table 3 can be used alongside the Theory of Change map to support implementation. To ensure greater specification and operationalisation, the strategies are reported in line with Proctor et al.’s recommendations for specifying and reporting implementation strategies 44 and drawing on Powell et al.’s compilation to ensure clarity and consistency in the naming of the strategies. 48
Implementation plan for Integration of C-POS:UK into routine paediatric palliative care with specification of implementation strategies.
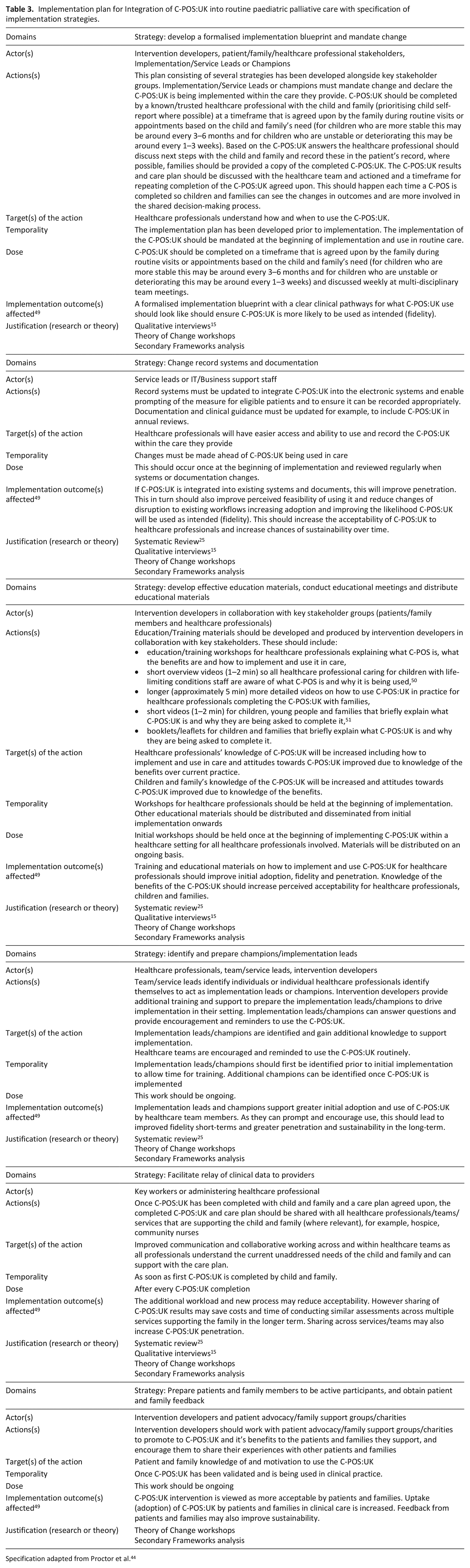
Specification adapted from Proctor et al. 44
Discussion
Main findings
Through using a Theory of Change approach, a causal pathway for the implementation of the novel C-POS:UK was developed and presented in a Theory of Change Map. Utilising Normalisation Process Theory to interpret the data enabled novel understanding of potential normalisation of C-POS:UK into sustained routine care. From this work an implementation plan was developed consisting of strategies to operationalise future implementation efforts.
The professional perspective enabled identification of important service/system level factors such as electronic system support and integration. The parent perspective prioritised individual/family level factors such as flexible use of C-POS:UK to accommodate changing needs throughout the child’s life.
The review with the steering group and consultation with the Young Person’s Advisory Group highlighted key elements of the Theory of Change that must be considered when C-POS:UK is implemented into routine care.
What this study adds?
Whilst many of the findings are in keeping with both the existing adult palliative care literature and findings from other paediatric care settings,3,7,8,25,52,53 this is the first time they have been identified in the context of paediatric palliative care. Considerations that are specific to this population and context relate to the importance of ensuring C-POS:UK is implemented in a way that enables children to self-report their own health outcomes and that it equally engages both the child and their family members. This must be carefully considered in relation to delivery mode, as well as how the results are shared and stored across services, including issues relating to data privacy. 16
As with all complex interventions, the implementation of the C-POS:UK is context-specific, and this Theory of Change has been developed for a specific healthcare context – paediatric palliative care provided in UK National Health Service hospitals. We recommend a similar method (i.e. Theory of Change) is applied in further care delivery settings such as community and hospice.
As far as we are aware, this is the first time that Theory of Change workshops have been conducted through multiple small group workshops and using a mix of synchronous and asynchronous methods. During the time-period in which the workshops were run, there were multiple strains on paediatric healthcare services in the UK including a scarlet fever outbreak and nursing and junior doctor strikes. This led us to take the decision to take an asynchronous approach to the professional workshops. This approach allowed professionals to engage in the workshops at a time that would work best for them.
For parents/carers, we ran synchronous workshops at different times and days (without the requirement to attend all workshops) which provided parents/carers greater opportunity to participate. The small groups also provided more privacy for parents/carers to share their experiences, compared to the larger groups more typical of traditional Theory of Change workshops. The small groups also enabled the research team to probe participants’ answers and suggestions, to better understand their thoughts and reasoning. This novel approach has advanced Theory of Change methodology, providing evidence that different modes of engagement can produce robust Theory of Change development and enable engagement with stakeholder groups who may otherwise have not been able to participate.
Whilst several methods for selecting implementation strategies have been proposed, 54 they typically rely on theory and/or existing research. However, there is very limited existing research into implementing an outcome measure into paediatric palliative care.15,25 As such this study took a stakeholder-driven approach, to identify key considerations for implementation that were developed into strategies. We found this approach feasible and our systematic reporting, could enable this approach to be replicated in future research to develop implementation strategies where there is limited evidence.
Strengths and limitations
The sample is a potential limitation of this study. Only a quarter of the parent/carer participants were fathers. This is in line with much of the existing paediatric palliative care research, where fathers are often underrepresented (mothers made up 75% of samples across 45 studies). 55 Additionally, the majority of the parent/carers were white British. This is a limitation as in the UK life-limiting conditions are more prevalent in children from Pakistani, Asian and Black backgrounds. 56 As such, there may be additional implementation considerations specific to those from ethnically diverse backgrounds. 57 Further work is required to meaningfully engage and involve children with life-limiting conditions and their family members from ethnically diverse backgrounds.58,59 Innovative child-friendly approaches may also need to be developed to further enable the participation of children.60,61 Reduced ability to probe in the asynchronous workshops was a limitation of the professional workshops meaning there may be additional considerations that could impact implementation that have not been identified.
Finally, due to lack of existing measures in practice, 62 implementation of C-POS:UK was presented in a hypothetical way to stakeholders. This work provides a theoretically informed explanation of how implementation of C-POS:UK may occur. Further work is needed to test the proposed causal pathways of the Theory of Change and Implementation Plan in practice through pilot and/or feasibility studies including addressing resource/logistical challenges.15,25
Conclusion
Using a participatory Theory of Change approach, a potential causal pathway and key mechanisms have been identified for implementation and normalisation of the novel C-POS:UK into hospital-based paediatric palliative care and an implementation plan has been developed. There is great potential for C-POS:UK to have a significant positive impact on the care provided to children with life-limiting conditions and their families.
Footnotes
Acknowledgements
We thank the European Research Council and the NIHR Applied Research Collaboration South London (NIHR ARC South London) at King’s College Hospital NHS Foundation Trust for the financial support needed to undertake this study. The Children’s Palliative care Outcome Scale (C-POS) Study Steering Group members are: AK Anderson, Jo Bayly, Lydia Bate (PPI), Myra Bluebond-Langner, Debbie Box, Katherine Bristowe, Rachel Burman, Lucy Coombes, Alan Craft, Fin Craig, Jonathan Downie, Julia Downing, Helena Dunbar, Bobbie Farsides, Sara Fovargue, Lorna Fraser, Jay Halbert, Julie Hall, Irene Higginson, Michelle Hills, Mevhibe Hocaoglu, Vanessa Holme, Gill Hughes, Jo Laddie, Angela Logun (PPI), Eve Malam, Steve Marshall, Andrina McCormack, Catriona McKeating, Lis Meates, Jane Morgan (PPI), Fliss Murtagh, Eve Namisango, Cheryl Norman, Sue Picton, Christina Ramsenthaler, Anna Roach, Ellen Smith, Michelle Ward and Mark Whiting.
Author contributions
Conception and design of the work: all authors. Data collection: HS, RH, IG, DB and CES. Transcription: HS, IG and DH. Data analysis: HS. Patient and Public Involvement: HS and IG. Interpretation of data: HS. Draft of paper: HS. Critical review and revision of article: all authors.
Data management and sharing
No data are available. Not applicable.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The C-POS study is supported by the European Research Council’s Horizon 2020 programme [Grant ID: 772635]; this article reflects only the author’s views, and the European Research Council is not liable for any use that may be made of the information contained therein. The C-POS study is supported by the National Institute for Health and Care Research (NIHR) Applied Research Collaboration South London (NIHR ARC South London) at King’s College Hospital NHS Foundation Trust. The views expressed are those of the author[s] and not necessarily those of the NIHR or the Department of Health and Social Care. Hannah Scott, King’s College London, is supported by the National Institute for Health and Care Research (NIHR) Applied Research Collaboration South London (NIHR ARC South London) at King’s College Hospital NHS Foundation Trust, through which their PhD is funded [Grant ID: NIHR-INF-2158]. The views expressed are those of the author[s] and not necessarily those of the NIHR or the Department of Health and Social Care. The funding bodies above did not have any role in the design of the study, collection, analysis, interpretation of data or writing of the manuscript.
Research ethics and patient consent
Ethical approval was granted by King’s College London Health Faculties (Purple) Research Ethics Subcommittee (HR/DP-22/23-33702). All participants provided written informed consent. Young Person’s Advisory Group representatives were providing patient and public involvement and so ethical approval was not required.