
Abstract
Background:
Nurses can be involved in interventions that they perceive as hastening death. These interventions may intentionally cause death, as in the case of assisted dying or result in death as an unintended consequence, such as when life-sustaining treatment is withdrawn. There is increasing evidence regarding nurses’ experiences of providing care in these separate contexts. However, it remains less clear whether parallels exist in experiences across various acts that nurses might consider death hastening.
Aim:
To synthesise qualitative research findings on the lived experiences of nurses when involved with acts that may be perceived as death hastening.
Design:
A qualitative evidence synthesis utilising thematic synthesis.
Data sources:
An initial search of CINHAL, PsychInfo and Medline was undertaken in December 2022 and updated in August 2024. Papers were quality assessed using the Joanna Briggs Institute Critical Appraisal Checklist for Qualitative Research.
Results:
Twenty-three papers were included in the review. An overarching theme linked to the emotional labour required to provide care was developed. Three sub-themes influence emotional labour: (1) experiencing personal and professional conflicts, (2) the provision of ‘normal(ised)’ care and (3) perceptions of palliative care as a proxy for hastening death.
Conclusions:
This synthesis demonstrates that nurses experience significant emotional labour across acts that may be perceived as death hastening. The level of emotional labour is influenced by nurses’ uncertainty of the ethical and moral status of these interventions and navigating these uncertainties alongside colleagues, patients and those important to them during care delivery.
Keywords
Nurses deliver care for patients and those important to them across acts that may intentionally or potentially hasten death, navigating this care within the boundaries of healthcare systems and professional regulation.
The increase in permissive legislation relating to assisted dying is challenging healthcare professionals to consider how an assisted death sits alongside accepted or ‘traditional’ healthcare practices at the end of life.
Providing care in these situations can be challenging and requires emotional labour to navigate.
This review allows recognition of how the emotional labour involved in providing care, and its subsequent impact, is often better recognised within assisted dying than for other acts that may be perceived as death hastening.
The ‘normalising’ of care, and consequently dying, within acts that may be perceived as hastening death limits the recognition of the emotional labour required for nurses to provide care in these circumstances.
When supporting a patient through an assisted death, nurses focus on optimising the experience for the patient, whereas in other acts that may hasten death, nurses’ primary focus is on the experience of those present with the patient.
The impact on nurses’ emotional well-being due to the expectation to engage in significant emotional labour, in all care that may be perceived as death hastening, should be considered in daily practice, policy and organisational structure.
The provision of emotional support should be considered for nurses when involved in the delivery of care that may hasten death, either through intentional acts (an assisted death) or unintended consequence of the care.
Normalising care that may be perceived as death-hastening can impact nurses’ feelings of agency within care delivery and may need to be considered in jurisdictions with permissive assisted dying legislation as these practices embed within organisations.
Background
An increasing number of countries permit assisted dying, an act that intentionally hastens a patient’s death. Other acts within healthcare have the potential to hasten death, although are not used with this intention. Examples of such care might be the use of sedation or the withdrawal of life-sustaining treatment.1,2 On a clinical, conceptual, and philosophical level, what encompasses ‘hastened death’ remains poorly defined with no internationally agreed terminology. 3 Clinicians identify complex physical and moral issues that occur when attempting to define what may constitute an act with the potential to hasten death (see Table 1). Acts that ‘hasten death’ are often seen as solely voluntary euthanasia and physician assisted dying. 4 However, acts of care, which are relatively common in palliative care, such as withdrawal of life-sustaining treatment and the use of sedation may also be perceived as death hastening. 5 For some people with a desire to hasten their death, the choice to voluntarily stop eating and drinking may be taken 6 and can often be considered as a natural form of dying. 7 Healthcare professionals may continue to have an active role in supporting patients who make this choice and not intervene in halting the dying process. 8
Definitions.
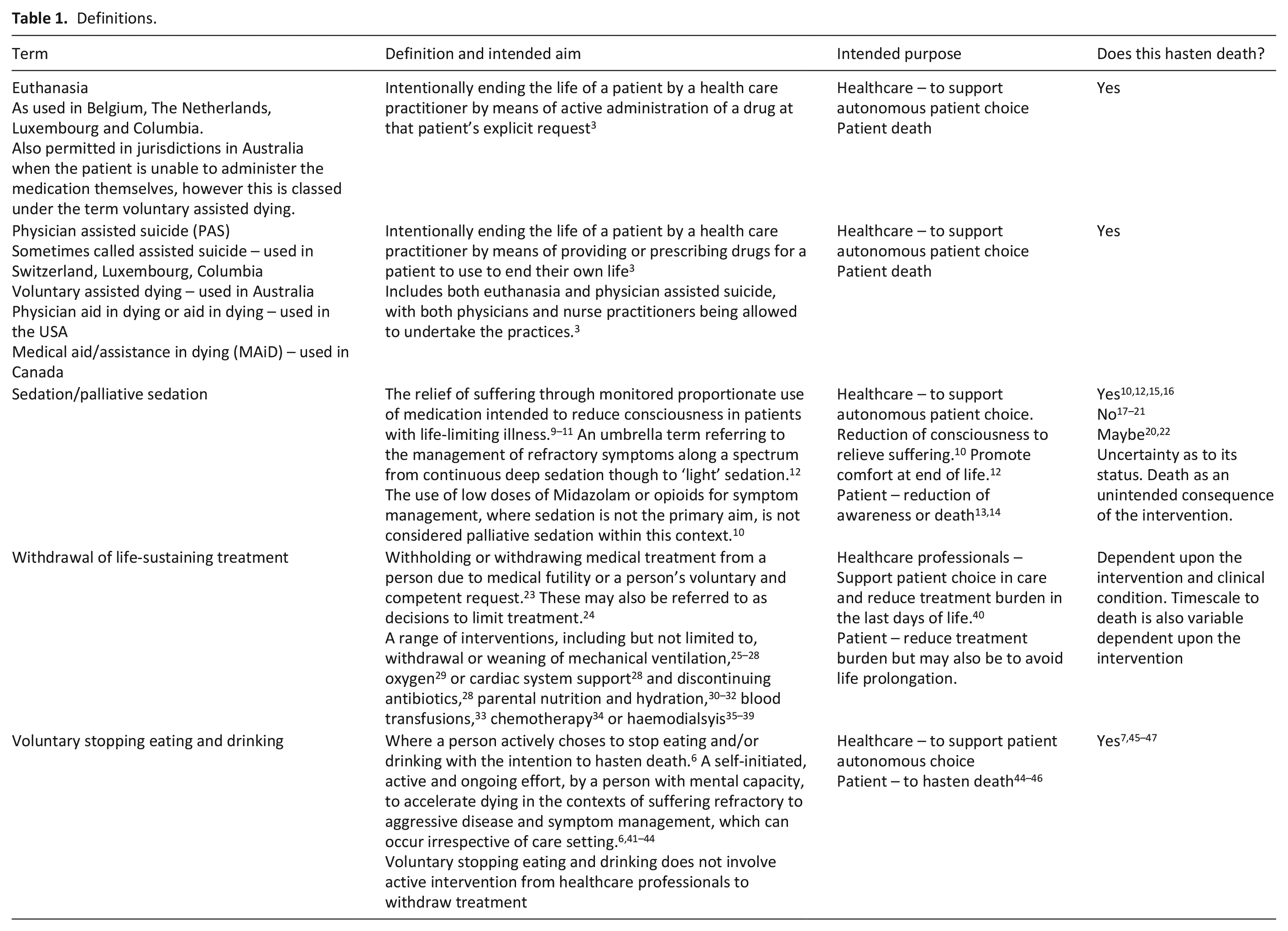
The complexity in defining these care acts also links to their ethical status. Primarily whether death, in this context, is an intended or unintended consequence or side effect of the act for the healthcare professional5,48 –56 Although it is recognised within legal and ethical frameworks where these differ from assisted death, 57 it can be difficult to delineate the intentions of patients and healthcare professionals within existing frameworks. 15 There may also be a disconnect between doctors’ and nurses’ perceptions of acts that hold the potential to hasten death,58 –65 with nurses more likely to experience internal conflict and increased uncertainty about the nature of these interventions.15,22,62 This uncertainty is more marked within the use of sedation than other interventions.9,66 Whilst attempts are made within the literature to decrease the ambiguity that nurses feel about whether care may hasten death, it is also recognised that this originates primarily from physician authored papers. The focus on ‘educating’ nurses to help them gain moral clarity may serve to further marginalise their concerns about these acts. 67
The term ‘experience’ can often be used without explanation as to what it may refer to. 68 Experience can be considered as an active ‘intersubjective, social and political’ process that people enter through in order to create meaning. 69 A relational understanding and expectations of the nurse-patient relationship defines the nurse’s experience, yet their experiences are commonly amalgamated with other healthcare professionals, most specifically physicians. Nurses identify their role as unique within the healthcare team. The frequency and intimacy of patient contact, seeing themselves as a patient advocate, and coordinating care to support patients to navigate the healthcare system are all cited as specifically defining their role in palliative care.70,71 The dynamics with the wider healthcare team are also considered as potentially impacting how care delivery is experienced.70,71 Both nurses and physicians feel that nurses are well placed to identify suffering and establish if symptoms are poorly managed or whether further treatment may be futile.22,72 However, the level of involvement nurses have in decision-making is noted as an important factor that impacts upon the quality of their experience delivering care; often primarily influenced by the physician. 72 Nurses being required to undertake care they perceive not in the patient’s best interest or where they feel they are witnessing unnecessary and iatrogenic suffering can result in moral injury. 73 While there appears to be some issues in common for all healthcare professionals, synthesising research that solely considers nurses will allow a greater understanding of their own nuanced experiences.
This review aims to synthesise evidence across acts that nurses may perceive as death hastening to yield new knowledge of the experience of providing care that may or will hasten death. Understanding where, or if, comparable experiences exist could help develop knowledge related to the practical, ethical and moral complexities nurses report when providing care at the end of life. Finally, this review aims to amplify the nursing voice within this complex and often divisive topic.
Review question
What can be learnt from synthesising qualitative research findings on the lived experiences of nurses when involved with acts that may be perceived as death hastening?
Methodology/methods
A qualitative evidence synthesis was undertaken utilising thematic synthesis, as described by Thomas and Harden. 74 The research question considers experience, as such a focus on primary qualitative research, which is supported by this approach, is most appropriate. Thematic synthesis is valuable when the research question aims to gain a deeper understanding of an unknown issue, rather than theory generation. Thomas and Harden 74 state that, within this form of synthesis, it may not be possible, or required, to locate all available evidence. However, the strategy focusses on ensuring that no new research would alter the ‘conceptual synthesis’. 74 Reverse and forward citation checking and reviewing recent documents published in the author’s country were included in the search strategy. This process stopped when there was agreement across authors that the results were conceptually rich. Analysis and synthesis were undertaken using the three-step approach. 74
Coding text
Developing descriptive themes
Generating analytical themes.
The review exists within a social constructivist paradigm, where individuals’ experiences of the world shape understanding and meaning-making. 75 This recognises the overt importance of the social context of the research and the influence of positionality within the analysis. This evidence synthesis is reported in line with the enhanced transparency in reporting the synthesis of qualitative research (ENTREQ) checklist. 76
Search strategy
The search strategy and subsequent inclusion/exclusion criteria were developed using SPIDER. 77 SPIDER was utilised to facilitate a search that considers experience across interventions. To increase the sensitivity of the search strategy, the research design was not specified within the search terms. The lead author (VA) ran initial searches in December 2022 and updated in August 2024 using the Cumulative Index to Nursing and Allied Health Literature (CINAHL), PsycINFO, and MEDLINE databases. The search strategy was developed alongside a Lancaster University subject specialist librarian using Medical Subject Heading (MeSH) terms and database specific linked suggested terms and was tested against two known papers. The search terms are identified in Table 2 and results were obtained by linking searches with the Boolean operator AND.
Search terms.
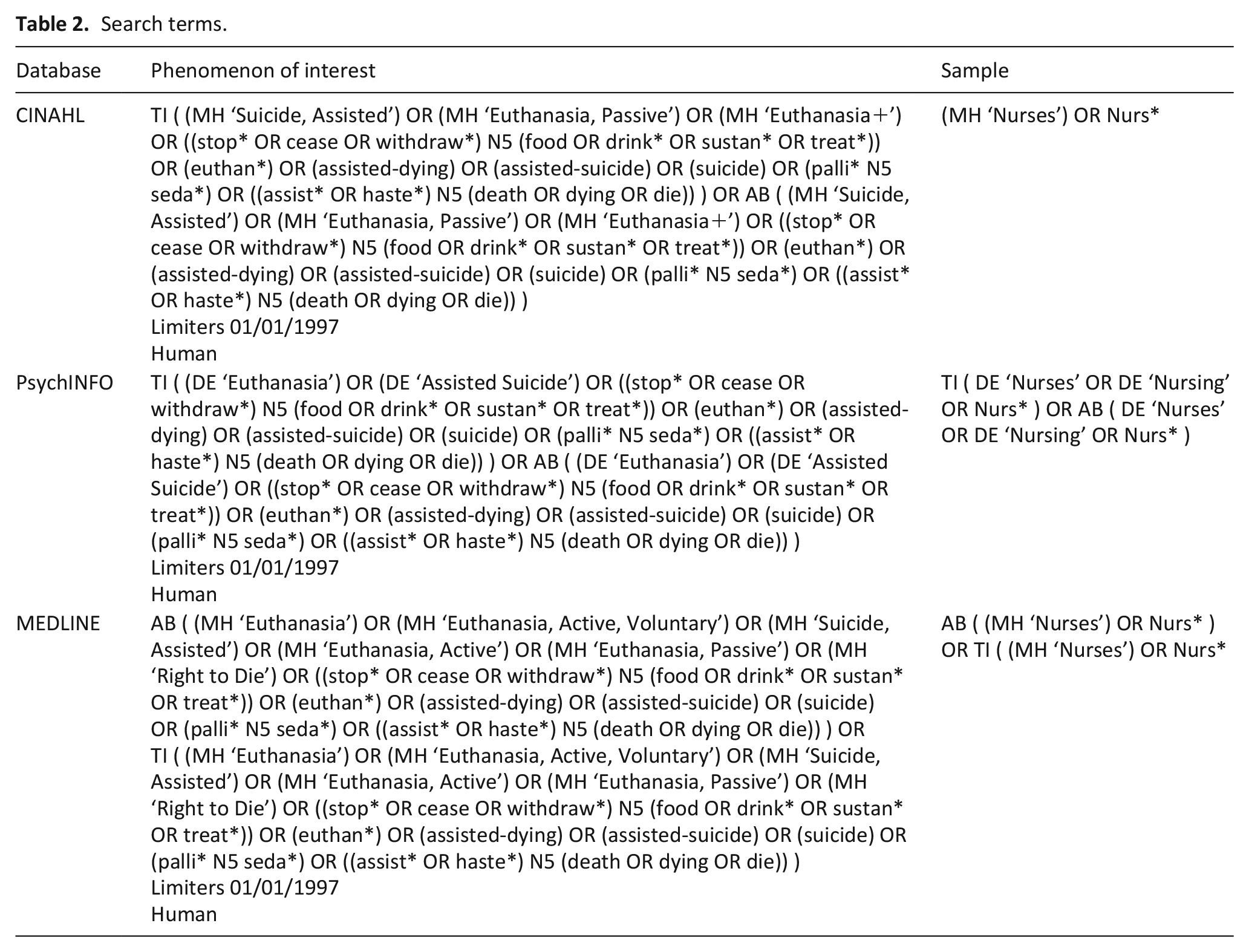
A manual search was undertaken through citation checking of reference lists and forward tracking of citations within included studies to ensure no papers had been omitted. A selection of reference lists of legalisation and policy documents local to the author were also reviewed, although this process did not add any further papers.
Inclusion/exclusion criteria
The inclusion/exclusion criteria are given in Table 3.
Inclusion/exclusion criteria.
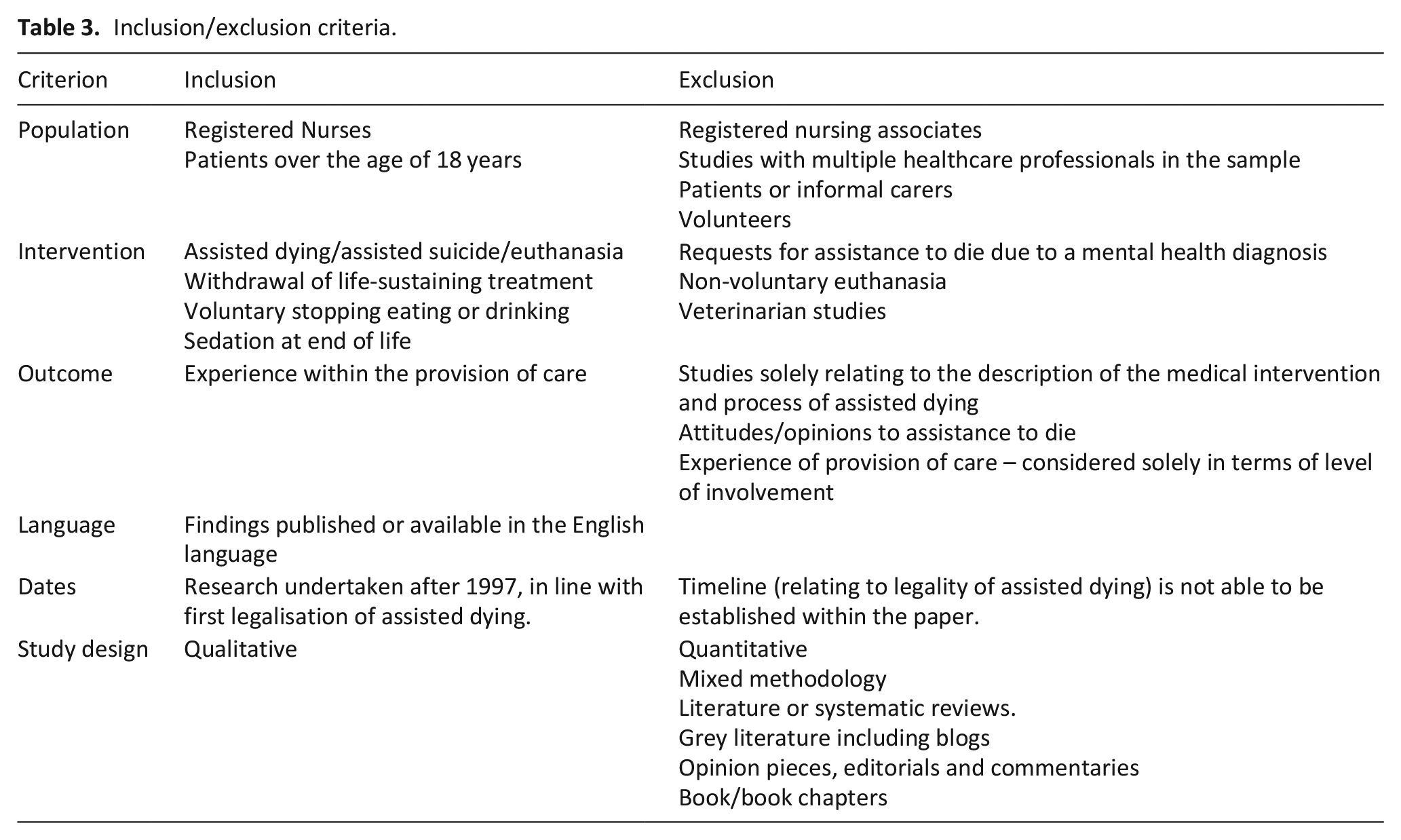
The papers’ titles were initially evaluated against the inclusion criteria. Abstracts and full text papers were read if they appeared to meet the inclusion criteria following the title search. All included papers were then re-read to ensure their appropriate inclusion. A second reviewer (JM) blind-reviewed 10% of titles (360 out of 3600 papers) from the initial search against the inclusion criteria. The process was undertaken utilising Rayann® and the decisions were blinded until both reviewers had completed the evaluation process. Decision-making relating to the application of the inclusion criteria was discussed and recommendations were made to provide rigour to the process. An example of this was how the concept of experience was understood by both reviewers as this was central to the review process. There was consensus on which papers should be included.
Data extraction, appraisal and synthesis
Data were extracted using a tool developed from the work of Noyes, 78 supporting the extraction of large amounts of narrative data verbatim from the research. The tool was modified to include data relating to the review question, including the legality of assisted dying. The second reviewer (JM) undertook data extraction on 10% of the included papers (3 of 23) to clarity check the tool and protocol for appropriate data extraction. Uncertainty was resolved through initial discussion and changes made to the extraction tool to capture necessary data. The studies were quality assessed alongside data extraction 79 using the Joanna Briggs Institute quality appraisal tool. 80 No papers were excluded based upon this assessment, although data quality was considered reflexively during the synthesis, in keeping with the method. 74
Coding and theme development were undertaken inductively. Analytical themes were developed following the identification of cross cutting, comparative and parallel descriptive themes. 81 A hybrid approach to coding was undertaken using both Nvivo® for descriptive themes and moving to pen/paper for the development of analytical themes. Reflexivity is fundamental in the development of a rigorous thematic synthesis and therefore regular discussions and reflections with the supervisory team (NP and LM) were undertaken.
Findings
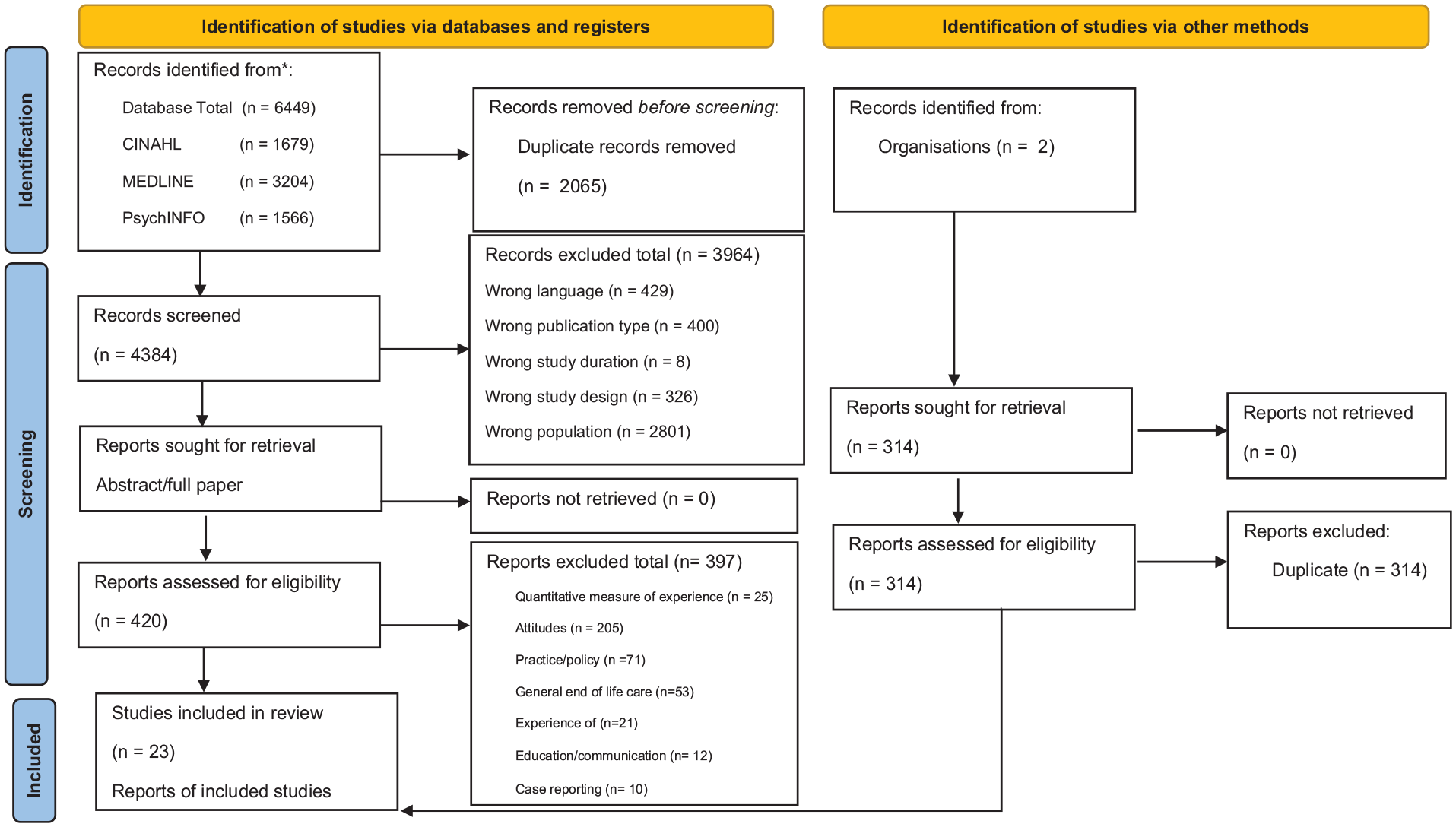
From 4384 papers assessed for eligibility, a total of 23 papers were identified relating to nurses’ experience of acts that may potentially hasten dying (see PRISMA Figure 1). Thirteen relate to assisted dying including six from Canada, five from Belgium and two from the USA. These papers are from areas with permissive assisted dying legislature with the exception of De Bal et al., 94 Dierckx de Casterle et al., 95 Schwarz 103 and Volker. 104 Three papers consider sedation, these are from Canada, the UK and the Netherlands and seven consider withdrawal of life-sustaining treatment all in jurisdictions without permissive assisted dying legislature at the time of the study. All papers relating to withdrawal of life-sustaining treatment were based in intensive care settings. No papers considering voluntary stopping eating and drinking met the inclusion criteria. Table 4 provides a summary of included papers.
PRISMA.
Summary of included papers.
Within this synthesis, the term ‘other acts that may hasten death’ is used to represent withdrawal of life-sustaining treatment and sedation. The term ‘assisted dying’ has been chosen to encompass interventions across physician assisted suicide, euthanasia and MAiD. This is used as a neutral, umbrella term for acts undertaken with the active intention of inducing death, in keeping with suggested international convention.3,105,106
An overarching theme, the emotional labour of care was developed with three subthemes that influence the experience of delivering care and subsequent levels emotional labour involved. The sub themes are (1) experiencing personal and professional conflicts, (2) the provision of ‘normal(ised)’ care and (3) perceptions of palliative care as a proxy for hastening death. Table 5 identifies how the papers are represented within the themes.
Themes.
The emotional labour of care
The emotional labour associated with nurses’ involvement in care that may hasten death is an overarching theme within the studies. Emotional labour is defined as ‘the management of feeling to create a publicly observable facial and bodily display’ (p. 7) 107 . It is an active process where behaviours develop in line with social expectations of professional roles. Emotions can be suppressed and outwardly expressed emotions and behaviours can be performative depending upon situational expectations, 107 which is seen consistently within the studies. Overall, nurses identify a requirement to understand, navigate and conform to expected behaviours, when involved with all acts that may hasten death, which requires emotional labour. Opinion varies amongst nurses in the studies about what behaviours may be appropriate, including showing emotions during care delivery. When involved in the withdrawal of life-sustaining treatment, nurses feel showing emotions publicly can be appropriate 85 although they also described needing to hide these from the wider team.86,87 When caring for people having an assisted death, any outward physical emotional response is generally removed from any public view.94,96,97 Within palliative sedation, nurses frequently describe situations they find challenging linked to witnessing suffering, though the expression of emotion is not considered.
Across interventions, nurses report involvement in care impacting both positively82,86,92 –94,97,98,100,102 and negatively82,84,87 –90,92 –94,97 –100,102 on them. Experiences perceived as negative are reported as impacting nurses’ personal lives with examples of them ‘taking it home with you’.86,88 –90,94,98,100 Within all acts, nurses discuss emotional detachment as a useful strategy to manage emotional labour,86,87,90,95,96,98 although some do not routinely use this in practice.94,100
As professionals nurses’ sympathy extended to their patients, but a certain emotional distance was maintained. Many nurses underlined the importance of psychologically releasing the patient’s request. Not all nurses succeeded in maintaining this emotional distance. . . . . .Non-palliative care nurses in particular took their experiences home after their shift
94
p 596
Instead, nurses commonly feel required to regulate negative emotions while providing patient care in order to manage their own well-being.87,88,94 –97,100 Across all acts, emotional labour is reported to diminish as nurses gain experience with providing care, both through desensitisation to witnessing dying and through the development of clinical skills.83 –85,89,92,96 –98,100,101
The intensity and level of emotional labour required are consistently considered by nurses as linked to a desire to help when witnessing suffering. Nurses specifically report that iatrogenic suffering increases the emotional labour required to provide compassionate care82,84,86 –88,93,98 –100 and was also considered as motivation for involvement within assisted dying.93,98,100
That first experience troubled me. Not because of the experience itself, but because of all the previous events that could have ended much better if MAID had been available before. I have images of people I have accompanied in painful end-of-life situations (P17). We do MAID, it is not painful. There is pain, but there is much less pain and suffering compared to someone slowly dying for two or 3 days with pulmonary complications (P31).
98
p. 1638
Nurses who decline to be involved in assisted dying due to moral objection (conscientious objection) also report aspects of care that generate emotional labour. The requirement to deliver care for a patient knowing they wish to have an assisted death or providing care for other patients when an assisted death is occurring are reported as burdensome.93,100 The position as ‘conscientious objector’ also makes them feel vulnerable, with support depending upon individual manager’s stance rather than organisational policy.93,99 The lack of organisational support leads nurses to feel they must self-regulate emotional responses due to the uncertainty of the reactions of team members. As such, active involvement in assisting dying cannot be considered as the sole cause of emotional labour in these cases.
Experiencing personal and professional conflicts
This theme can be summarised as elements that cause personal and professional conflict, which affects the levels of emotional labour required to provide patient care. Conflict occurs when nurses, to meet professional expectations, are required to work beyond perceived professional or moral boundaries. The professional obligations nurses feel towards patients mean they will offer support irrespective of moral tensions that may occur.86,90,93 –95,97,102,103 This was consistently observed across all acts that may hasten death.
Conflicts experienced by nurses are, most commonly, linked to interprofessional tension and are a significant consideration in all studies. Most notable for nurses is the sense that their input is not valued and their role in clinical decision-making is not recognised within the healthcare system.82,84,86 –90,94,97 Nurses describe themselves, within the healthcare team, as closest to patients and therefore best placed to accurately represent the patient’s wishes and clinical condition to others.84,86 –88,94,95,97,102 There was agreement, within other acts that may hasten death, that nurses will often find themeslves alone in navigating the consequences of these decisions with patients and families.83,84,86,87,90,91,94 The quote from the Australian paper illustrates the consequent challenge for nurses to (re)present decisions that they may disagree with and deliver care they feel not to be in the patient’s best interest. Essentially becoming the representative of the plan of care on behalf of the healthcare systems.
When the doctors sought to withdraw/withhold treatment, the participants expressed that they were often dissatisfied with the management of the situation. The most clearly articulated complaint was that whilst the doctors excluded nurses from the decision making and formulation of the management plan, once a decision is made to forego medical treatment the nurse is left to manage the dying process. ‘‘The mind your business and I’ll make the decision, then they make their decision or have the family make the decision . . . and then leave you to deal with it. . . they do it all the time . . . . . ’’.
86
p. 218
To reduce emotional labour nurses need to feel supported by the clinical team and a shared philosophy of care is considered important.82,83,86,92,94,95,98 –100. When mentioned, nurses feel that policy, no matter what that may be, is supportive as it legitimises the nurses’ actions and is perceived as constructing safe professional boundaries.85,87,91,94,96,99 Within other acts that may hasten death, a policy is more likely to be replaced by clinical guidelines causing ambiguity, with nurses describing feeling ‘caught’ between guidelines and individual physicians’ stance.86,91,97 Within assisted dying, tensions are reported as manifesting at an organisational level where nurses report a lack of input on structural and policy decisions.
Nurses, however sometimes found themselves trying to assist in a MAiD procedure with no practice guidelines in their places of work. This created uncertainty in their practice, particularly when nurses remained the primary caregivers of patients contemplating or undergoing MAiD
99
p. 14
However, this was only observed when considering legislative changes through MAiD100,102 and may be representative of the seniority of the nurses involved in this study. Overall, the requirement to deliver care that juxtaposes their professional or personal viewpoint can leave nurses feeling disempowered, which adds to their emotional labour.
The provision of ‘normal(ised)’ care
This theme reflects the perception that withdrawal of life-sustaining treatment and sedation are considered part of ‘normal’ healthcare, whereas assisted dying is perceived as something ‘other’. The term ‘normal(ised)’ is used to represent nurses’ perceptions that other acts that may hasten death, whilst not part of a ‘natural’ dying process, are accepted as part of ‘normal’ dying86,88 –90. Assisted dying is considered as a significant event, and a non-standard, unnatural death,92,93,95,97,98,100 with nurses using terms such as ‘murder’ and ‘killing’ irrespective of their moral position.
A reflective process was described by Donna: It was something really big for me when I saw the death certificate, it was this overwhelming feeling like, oh my gosh, I killed him. Because I think I truly believed that knowing his situation, and his. . . sort of isolation, that had I not been open to the conversation, had I not helped him access the information, that he probably would have never been able to access the MAiD services. . . . . . .
93
p. 516
Being the cause of death was not a significant narrative within other acts that may hasten death. McMillen 89 is the only example where nurses consider whether their actions were the cause of the patient’s death.
When asked if they played any part in the actual decision one participant replied: ‘‘No, and I don’t think I’d ever want to either because at the end of the day it’s somebody’s father, brother, mother whatever. No amount of money in the world could ever get me to make that decision I don’t think and I don’t know how they (the consultants) sleep at night sometimes.’’ (Nurse 3)
89
p. 254
Within this theme, there is a shared narrative about the point of death being controlled. Within other acts that may hasten death, this relates to healthcare-led interventions that nurses report undertaking to deliver compassionate care. Examples include delaying withdrawing life-sustaining treatment to wait for family members to be present and administration of sedation in response to perceptions of suffering.82 –86,89,103 This control extends to nurses attempting to de-medicalise the experience of dying to optimise the experience for patients and those important to them. This links to the concept of an aesthetic death 90 with examples including controlling the bedside environment, ensuring relatives have time with the person and titrating medication based upon the needs of those witnessing the dying process.85,86,90,91 Within assisted dying this manifested as nurses advocating for their patient’s choice and prioritising the patient within their caseload.93,99,100 For an assisted death, the point of death is invariably driven and controlled by the patient.92,100,103 This ‘othering’ of death within assisted dying is, perhaps, linked to control of the timing of death being situated outside of healthcare. A shift that is disruptive to the established or expected relationship between patients and healthcare professionals.
Perceptions of palliative care as a proxy for hastening death
Within this theme, the perception that palliative care provision can be seen as a proxy for hastening death is presented. In some cases, nurses perceive other acts that may hasten death as both physically and emotionally commensurate with an assisted death, and express this through implicit and explicit communication.83,84,88,89,94,97,100,103,104 For example, Denier et al. 97 describe how some nurses consider sedation and assisted dying on a spectrum of interventions. Although not directly expressed, this is suggested through nurses’ concern about their own practices, such as ensuring sedation is used judiciously and anxiety if death is prolonged.82,103,104 Nurses use phrases such as ‘active dying’ and ‘very, very terminal agitation’ as a justification to use sedation for intractable symptoms 83 or offering sedation as an alternative choice when assisted dying is requested. 94
Nurses also feel required to navigate the consideration that the public may view palliative care as offering a means to hasten death.87,88,97,104 In cases of sedation, nurses report family members consider that hospices and palliative care teams become involved with the direct intention to shorten life.83,84 Nurses report shock when faced with requests to hasten death83,108 and feel responsible for addressing what they see as an ill-informed view. They describe wanting to be clear that palliative care interventions will not hasten death. 94 However, the uncertainty some nurses express about the nature of these interventions, means this response can be incongruent with their personal view.
All of the nurses expressed uncertainty that palliative sedation could or would lead to the death of the patient and they repeatably reflected on this possibility. They all reported experiencing anxiety at some time about such an outcome, but all maintained the position of wanting what was deemed “best for the patient” at that time.
83
p. 152
These responses, therefore, may be a performative action that nurses feel required to undertake as part of the ‘nursing role’.
Nurses identify difficulty in establishing an ‘acceptable’ moral line that connects their external position with their internal stance,87,88,93,94,103 which requires significant emotional labour. Nurses suggest a hesitancy to openly state the opinion that death may be hastened through the actions of healthcare professionals.
There seems to be a discrepancy between the criterion on life expectancy in the guideline and nurses’ views, where nurses appear to prefer a more limited life expectancy than the guideline. This may be related to nurses’ concerns that sedation might hasten death
84
p. 160
As such, nurses may use innuendo and metaphor to help them navigate this ‘acceptable line’ with others, speaking to a shared implicit understanding around these interventions.82,94,103,104 In some cases, in countries where assisted dying was illegal, nurses used innuendo to give covert advice relating to medication use where a desire to die had been expressed. 104
While the term “overdose” was never used, it still was something that was understood as an “option” that the patient would have if they felt it was necessary
104
p. 45
Open discussions about the intention to hasten death are only reported in the assisted dying literature and legalisation of assisted dying is reported as facilitating more open discussions about care and reducing feelings of powerlessness for nurses.94,97,101,102 Overall, this theme reflects the complexity that nurses report navigating care that may hasten death and how nurses feel compelled, despite uncertainty, to present a narrative that interventions undertaken as part of routine palliative care do not hasten death.
Discussion
Main findings
Synthesis across acts of care that may, or intends to, hasten death has highlighted new parallels in experience for nurses. The emotional labour required to provide care is intensified by tensions created by nurses’ uncertainty as to whether the care they deliver may hasten death. Perhaps most significant is the recognition that supporting intentionally hastened death does not create distinctive challenges for nurses when compared to acts often provided within established palliative care. Actually, the synthesis appears to suggest the reverse. The normalisation of dying with medical intervention normalises the high levels of emotional labour needed to provide care. This challenges a narrative that, for nurses, involvement in assisted dying may feel distinct from involvement in established palliative care practices.
What this study adds?
The findings within this synthesis build upon earlier reviews, which consider these interventions individually. These reviews describe the emotional impact on nurses, including tensions trying to navigate family and doctor interactions 71 and the need to regulate emotions to deliver care. 19 This review adds to the wide and often contradictory findings reported when healthcare professionals are overtly asked about attitudes towards, and experiences within, assisted dying.109 –112
To address the review question, the data is understood through the lens of ethics of care. Care at the end of life is embedded with ethical and moral entanglements, and within the review, nurses consistently report ethical tensions linked to existent systemic powers. Ethics of care allows consideration of moral agency as embedded within interpersonal relationships. As such, decision-making is relationally oriented, directed towards care provision for others and understood through the interdependencies of relational responsibility bound within institutions.113 –115 Nurses’ experience, in this context, is created through engagement with the life of the patient, the embodied physical and emotional spaces that nurses are placed within and who nurses spend time with during care delivery.71,116 –118 Within the assisted dying literature, the predominately important relationship for nurses was between them and the patient and optimising the experience for the person dying.97,101 Whereas for other acts that may hasten death, nurses consider those with the patient as most important and place focus on optimising their experience of dying.85,86,90 This difference is perhaps influenced by the ability of the patient to engage with care decisions. Within other acts that may hasten death, patients are more likely to be semi-comatosed or in a medically induced coma and therefore conversations will be focussed upon those at the bedside. The intention for the nurses is to support families in creating a positive lasting impression of dying for those with the patient119,120 and linking to the provision of an ‘aesthetic’ death. However, this seemingly engenders the performative language and actions identified in the review, where the intention to communicate complex ethical decision-making is undertaken in ways to avoid misinterpretation.
The ‘spaciotemporal and bodily proximity’ of nurses with patients can make them uniquely placed to understand the patient’s needs, which nurses also reported within the review,70,117 yet ‘institutional space’ is needed to support their involvement in decision-making. 113 ‘Institutional space’, in this context, refers to a philosophical space that supports nurses to utilise their skills and recognises the unique roles different healthcare professionals have in providing holistic care. Within assisted dying, nurses appear to be given ‘institutional space’, seeing themselves as taking a more proactive role in leading care,117,121 and as such feelings of disempowerment were not commonly reported. ‘Institutional space’ here provides a culture of support to actively advocate for patients, allowing nurses to influence the structures they worked within, reflective of their clinical experience.122,123 More commonly, nurses involved in acts that potentially hasten death reference a lack of agency in care and a culture of ‘getting on with it’ 86 adding to the emotional labour required. It is also important to recognise that the formal practical and emotional support for nurses reported as embedded within assisted dying services, are not reflected across other interventions that may hasten death. This is despite positive associations between self-compassion and the provision of compassionate care. 124
Nurses ‘proximity’ can also increase the emotional labour involved providing in care. 125 Witnessing suffering is perceived as an expected aspect of the nurse’s role, required to be managed silently. 126 This links to a hegemonic and gendered expectation that nurses engage more in emotional labour in comparison to other healthcare professionals. 127 The parallels within emotional labour noted in the review occur as nurses routinely place more value on the well-being of others than their own. Whilst the expectation to regulate emotions can also explain a commonality of moral and emotional dissonance identified within the review, which appears distinct to nursing literature. Doctors, for example, have been shown to often lack the social ‘permission’ to show emotion with colleagues when caring for critically unwell patients through the professional expectation of their role 128 and describe experience centred through their own emotions rather than linked to patient experiences. 129 As such, it is suggested that this form of emotional expression and subsequent emotional labour sits within a nursing space and feminised expectations of the nursing role.
The concept of normal(ised) care identified within this synthesis has significance for future developments in policy. Nurses do not currently see assisted dying as part of normal healthcare. 130 It is significant to recognise that nurses consider controlling the dying process, through the care they deliver, as part of routine end-of-life care. However, when patients seek to control the point of their own death, nurses have difficulty seeing this as part of standard care. Using the term normal(ised) acknowledges that care at the end of life is often medicalised care influenced by factors within healthcare control. As such, no death considered in this review is considered natural or normal dying; it must only be considered normal within institutional healthcare. 131 Nurses describe ownership to manipulate the care environment, undertaken in an attempt to (re)create a ‘natural’ or ‘normal’ death, 132 which is valued and seen as part of compassionate nursing care.118,133,134 However, considering nurses’ feelings of disempowerment in decision-making, 135 influencing the environment offers nurses a means of control and the knowledge of providing this aesthetic death is seen as an opportunity to reduce the emotional labour required to provide care.
When acts that may be considered as death hastening are subsumed into general nursing processes, the emotional labour to provide this care is not well recognised. Yet, this is incongruous with the subsequent emotional impact nurses report and is a significant tension this review highlights. As palliative care navigates through local, national and international paradigmatic shifts, due to increasing jurisdictions with assisted dying legislature, understanding the impact of delivering this care is vital. This review adds a nurse’s perspective to this discussion and emphasises the significant parallels in the experiences of nurses across care that may hasten death that may have previously been viewed as distinct.
Strengths and limitations of the study
This review is the first synthesis considering the experiences of nurses across acts that intentionally and potentially hasten death. As such, this review serves to amplify nurses’ voices and, in some ways, attempts to address the subjugation of the value nurses bring to patient outcomes and experience, an aspect identified within the studies. The review takes a structured reflexive approach; therefore, offers one interpretation of the data. However, the use of a second reviewer throughout the iterative review process and the active engagement of the supervisory team adds rigour to the review findings.
The review highlights the paucity of evidence relating to nurse experience, which may also limit its transferability. There is a lack of research relating to the withdrawal of life-sustaining treatment outside of the intensive care unit and sedation outside of the hospice setting. Despite the inclusion of voluntary stopping eating and drinking, there was no evidence considering nurse’s experience in this area. A focus on these acts outside of ‘traditional’ settings would aid the development of a richer evidence base reflective of the places and people that deliver this care. This review must also be seen within the social context. The review can only present a Western-centric view of this topic, considering the geographical spread of the research, the diversity of participants and the role of nurses in these locations. This is a significant area for future development.
Conclusion
Synthesising experience across acts that intentionally or potentially hasten death draws parallels between experiences previously viewed as distinct. Nurses are grappling with the complexities of understanding their roles and position with the wider team when providing care that may intentionally or potentially hasten death. Uncertainty relating to whether interventions may hasten death and a lack of agency within care delivery increases the emotional labour involved in providing care. The impact of iatrogenic suffering and the recognition that physical and emotional time is not dedicated to supporting nurses within normal(ised) care has significance for nurse wellbeing. From a nurse’s perspective, there may be more in common in the experience of providing care in these contexts than previously recognised.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.