
Abstract
Background:
Hope plays a pivotal role in enhancing the quality of life and coping strategies of individuals living with advanced diseases. The nature of the relationship between hope and prognostic awareness is unclear.
Aim:
To explore the experiences and meanings of hope and their association with prognostic awareness among people with advanced incurable diseases.
Design:
Qualitative phenomenological study using reflexive thematic analysis of semi-structured interviews.
Setting/participants:
Interviews with 24 participants aged 30–99 years with advanced incurable disease were conducted in hospices and hospitals in the Czech Republic.
Results:
We generated four distinct approaches to hope and prognostic awareness: Technical, Spiritual, Minimalist and Pragmatic. Each approach exhibited unique cognitive, emotional and behavioural dimensions of hope and prognostic awareness. The Technical and Minimalist approaches showed fluctuating hope influenced by medical updates, while the Spiritual and Pragmatic approaches demonstrated stable hope resilient to prognostic information.
Conclusions:
Recognizing these diverse hope approaches can guide tailored interventions in palliative care. Healthcare providers should adapt their communication strategies based on people’s predominant hope orientations to support effective coping and enhance end-of-life care outcomes. This study sheds light on how different individuals navigate hope amidst terminal illnesses, providing insights into the nuanced psychological and emotional dynamics that influence their coping mechanisms.
Maintaining hope enhances significantly quality of life, reduces depression and contributes to psycho-spiritual well-being in individuals with terminal illness.
Hope extends beyond the possibility of a cure, encompassing intangible inner experiences and acceptance of life and death.
It plays a critical role in discussions about prognosis, with prognostic awareness influencing how hope is maintained or redirected in the face of incurable diseases.
Hope in people with advanced incurable disease does not necessarily depend on prognostic information from health professionals.
We identified four distinct approaches to hope and prognostic awareness – Technical, Spiritual, Minimalist and Pragmatic – and explored how each approach influences patients’ experiences and responses to their prognosis.
Healthcare professionals should acknowledge different approaches to hope and prognostic awareness and tailor their communication and care strategies accordingly.
For people living with advanced incurable diseases who adopt the Technical approach, healthcare professionals need to provide detailed medical information and understand how even partial findings affect hope. For people with the Spiritual approach, focussing on spiritual support rather than detailed medical data is crucial. People with the Minimalist approach may need support from healthcare workers without extensive engagement in care planning. While people with Pragmatic approach may benefit from a focus on non-medical goals and daily routines.
Customizing care to fit each patient’s approach enhances trust and improves satisfaction in end-of-life care.
Background
Maintaining hope is perceived as a factor enhancing the quality of life, 1 diminishing depression,2,3 contributing to psycho-spiritual well-being, 4 and also an effective method of coping with terminal illness.5,6 Benzein et al. 7 investigated the meaning of the lived experience of hope in people living with cancer and concluded that hope as a dynamic phenomenon helps to maintain meaningful life and dignified death for people with incurable illnesses. Hope in the context of palliative care goes beyond the hope for a cure. People with incurable disease report on other aspects of hope, such as intangible inner experiences of hope 8 (inner peace, emotional resilience and acceptance) that are not connected to any object, or living in hope 7 which reflects acceptance and reconciliation with life and death.9,10
Hope has been identified as an essential element for people during discussions with healthcare professionals about the prognosis of their illness. 11 Prognostic awareness is the extent to which a person accurately understands the nature and likely course of their illness.12 –14 Although people facing incurable disease feel uncertainty, they express hopes about living a normal life as long as possible. 15 A systematic review focussed on factors associated with prognostic awareness found mixed results regarding the level of hope. 13 For some people with advanced disease, hope was maintained by truthfulness and straightforward discussion, whereas for others, avoiding specific details helped.11,16 Loučka et al. 17 found that hope can be sustained regardless of whether patients hold realistic or unrealistic illness expectations. According to Mathews et al., 18 accepting a negative prognosis can redirect hope to new targets beyond a cure. Further, hope can be seen as a coping mechanism when dealing with a negative prognosis. A phenomenological study found that some people facing negative prognostic information used a coping strategy of reframing to help them maintain hope. 19 Another coping mechanism is ‘open door prognosis’, where people request prognostic information but simultaneously want to maintain hope and optimism. 11
In this paper, we aimed to understand the experiences and meanings of hope and their association with prognostic awareness among people with advanced incurable diseases. Specifically, we posed a research question: What are the approaches of people with advanced incurable disease towards hope and prognostic awareness?
Methodology
Design
We framed this research within the phenomenological paradigm that enables us to explore meanings, values, feelings and concerns of individuals as they experience their everyday lives at the end of life.20 –22 We combined a descriptive phenomenological approach with a reflexive thematic analysis23,24 and reported the study according to the Reflexive Thematic Analysis Reporting Guidelines (RTARG). 25 This study was the first phase of the larger PATH project, which explores the relationship between prognostic awareness and hope. It was conducted at the Third Faculty of Medicine, Charles University and funded by the Czech Science Foundation.
Conceptual framework
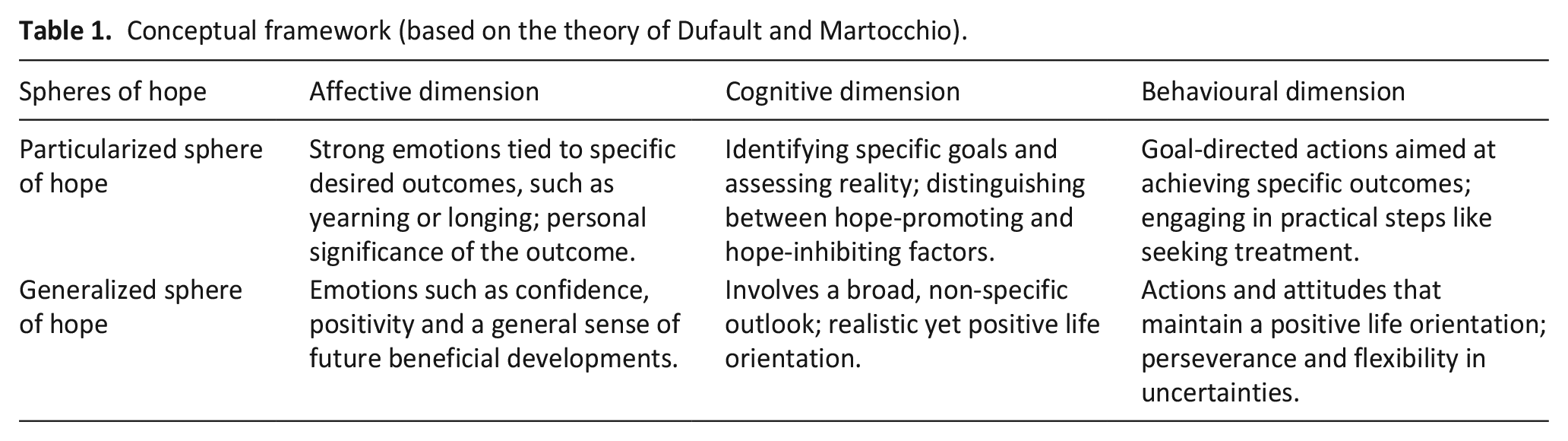
In this study we adopted a conceptual framework of hope based on the theory of Dufault and Martocchio. 26 They developed a complex multidimensional model of hope that has been widely cited and applied across various studies focussing on terminally ill patients.27,28 It includes two spheres of hope: (a) Generalized hope has a broad scope and is not connected with any particular object; it is rather a state of mind that provides inner flexibility and openness to life’s pitfalls. (b) Particularized hope is aimed at achieving specific goals that can be concrete or abstract in their nature. It helps individuals prioritize and affirm what matters most in life. We also included three dimensions of hope: affective, cognitive and behavioural (see Table 1).
Conceptual framework (based on the theory of Dufault and Martocchio).
Population
Adults with advanced incurable disease (assessed by their treating physician using the 6-month surprise question 21 ) treated in inpatient care (hospices or hospital) with decision-making capacity and willing to undergo an interview were considered eligible for the study.
Sample
Participants were selected purposively with the help of treating physicians at each site who identified eligible persons. Sample size was sufficient with regard to the concept of information power based on the specific aim of this study, the specificity of our sample, high quality interviewing and in-depth analysis of participants’ narrative. 29
Recruitment
Recruitment took place in the Czech Republic: in two inpatient hospices and one internal medicine department in the University hospital. Treating physicians provided eligible people with study information and forwarded information about potential participants to the researchers who then conducted interviews.
Data collection
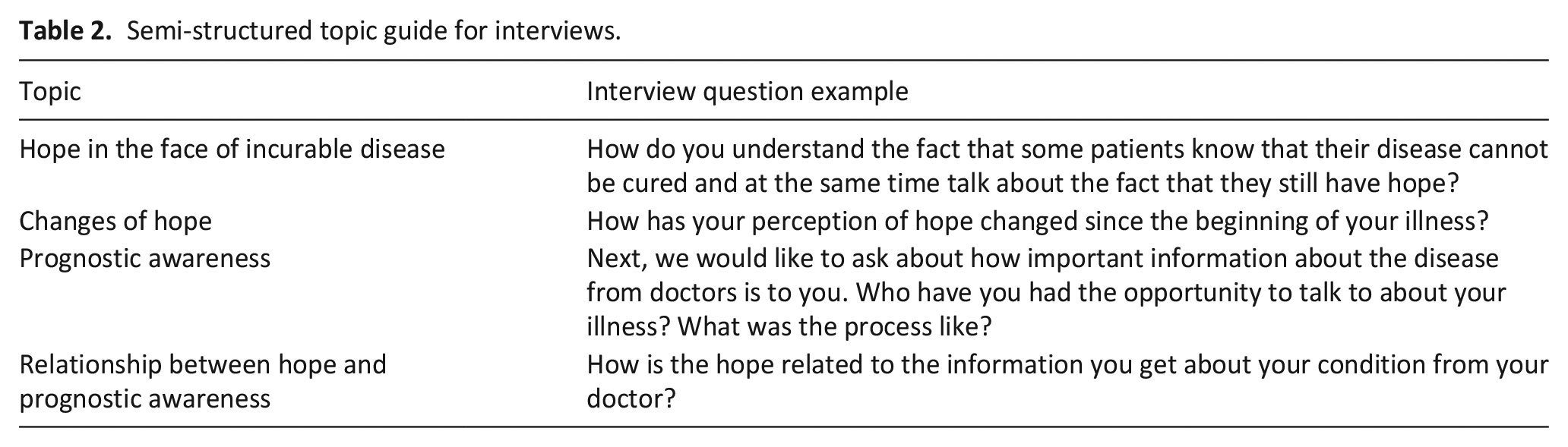
Interviews are a highly effective data collection method in phenomenological research, particularly for individuals receiving palliative care, as they facilitate a comprehensive exploration of participants’ lived experiences and subjective perspectives.22,23,30,31 We developed a semi-structured topic guide (see Table 2) according to the study aims, literature knowledge and expert discussions within the study team, consisting of researchers and clinicians in palliative medicine, psychology and sociology. Throughout the interview we asked probing follow-up questions in order to explore participants’ responses in depth. We also included one closed-ended question utilized in various research studies to assess the patients’ prognostic awareness32,33: ‘How would you define your current health status?’ (predefined answers: (a) relatively healthy, (b) ill, but not serious, (c) seriously ill but not terminal and (d) seriously ill and terminal).
Semi-structured topic guide for interviews.
We piloted the topic guide during the first three interviews; participants indicated an understanding of the questions; therefore, the interview guide was slightly adapted (we added one question that better led participants to talk about the subject of hope) and the interviews were included in the dataset. Interviews were conducted in person at the data collection sites by members of the research team (MJ, AH, ML, SV) who had experience with this method. All participants received information about the study and signed the informed consent. Ethical approval from the Research Ethics Committee of the Third Faculty of Medicine, Charles University was obtained on the 8 of June 2023 (Ref: PATH-01-2023).
The interviews were conducted between June and September 2023 and lasted 10–57 min. Immediately after the interviews, we removed the names of the participants and assigned codes to them. A trained research assistant transcribed verbatim anonymized audio recordings to maintain the authenticity of the speech, and two other assistants checked the accuracy of the transcription.
Data analysis
Data gathering and analysis were conducted simultaneously. In particular, we followed the procedures of reflexive thematic analysis by Braun and Clarke (2019, 2024).24,25 The process began with familiarization with the data, which consisted of listening to audio tapes and reading transcripts (AH, palliative care physician, and MJ, sociologist). We wrote reflections about individual stories for each transcript. Afterwards, an initial list of codes (containing both deductive and inductive codes) was generated by MJ after reading all stories and coding half of the transcripts. The list included both semantic and latent codes and was discussed with the research team. We applied collaborative coding where two researchers (MJ and AH) independently coded five transcripts in Atlas.ti software (version 7.5) and then compared their findings. Discrepancies were discussed with colleagues until reaching a consensus and agreeing how to approach the data. Two researchers (MJ, AH) systematically coded all interview transcripts using the list of codes. The continuous re-coding, discussing, writing reflections, using the conceptual framework table and working with data visualization (networks in Atlas.ti) helped us generate the themes. We named the themes collaboratively and generated interpretations of the final themes based on the data, our knowledge and experience in the field. During the whole process of analysis and interpretation of data, we followed the conceptual framework and phenomenological approach described above.
Analysis
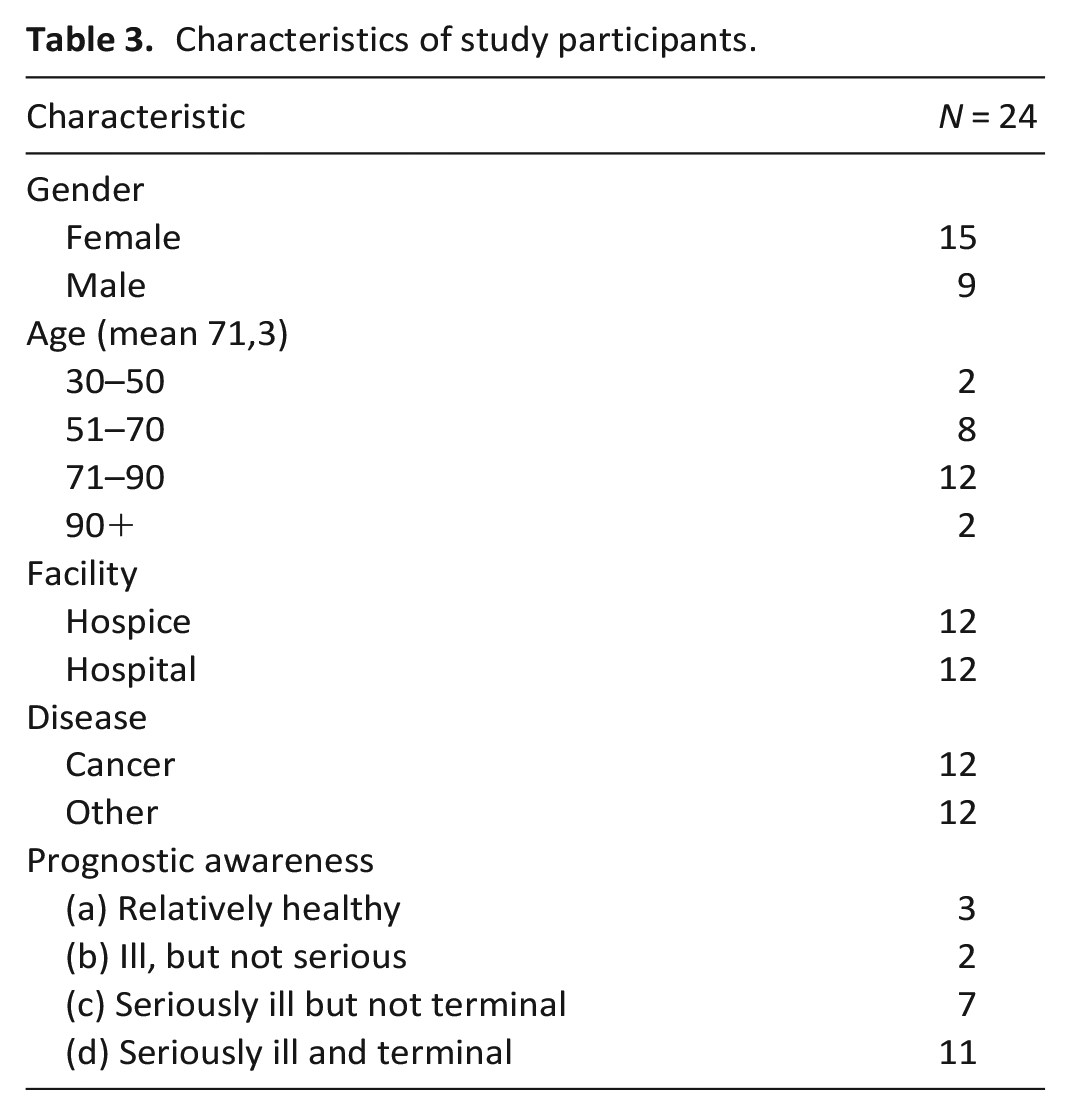
Altogether, we conducted 24 interviews with participants aged 30–99 years (15 women and 9 men). Half of the participants had been diagnosed with cancer (e.g. lung cancer, mesothelioma, colorectal cancer, pancreatic cancer, gastric cancer, ovarian cancer and a metastatic brain tumour). Other diagnoses included liver cirrhosis, Parkinson’s disease, pulmonary hypertension, geriatric frailty, COPD or renal failure (see Table 3).
Characteristics of study participants.
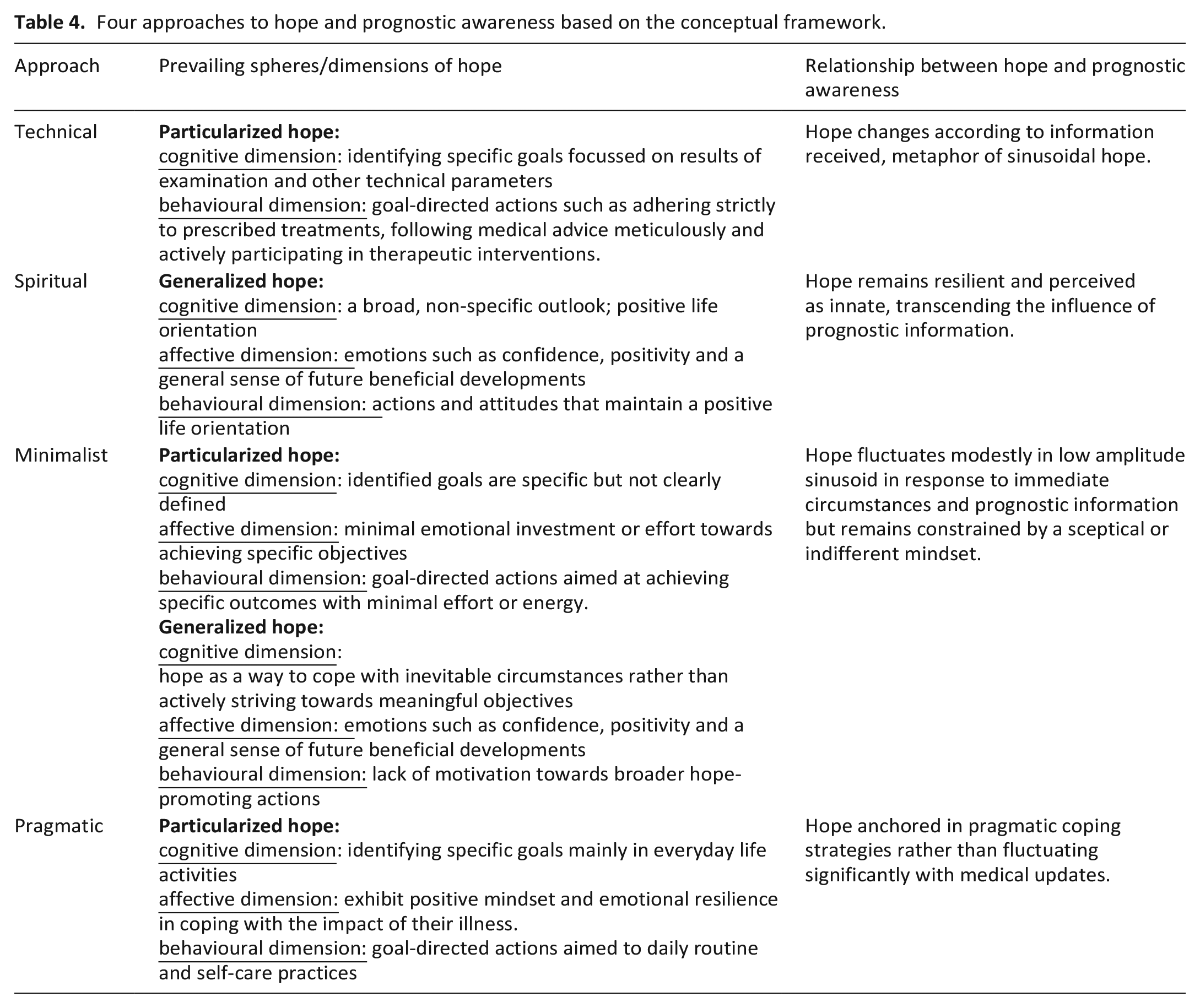
Based on our data, we generated four distinct types of approaches to hope and prognostic awareness among people with terminal illness: Technical, Spiritual, Minimalist and Pragmatic approach (see Table 4).
Four approaches to hope and prognostic awareness based on the conceptual framework.
Technical approach
People adopting the Technical approach exhibited a predominant focus on particularized hope, especially in terms of cognitive and behavioural dimensions.
I finally figured out that I need to be at least 80% healthy by the time I’m 60 and be able to function for the next ten years. (Interviewee 6)
Individuals holding the Technical approach perceived their illness with a practical mindset, seeking concrete, often technical solutions to address their health challenges. Although their immediate, well-defined goals were centred around specific treatments or medical outcomes, and they acknowledged the incurable nature of their illness, they still held a deep, underlying hope for a complete cure, despite knowing it was unlikely.
I kept thinking, well, it’s gonna be okay, it’s gonna be okay. And then they said no, no, it’s not gonna be okay: ‘If you hadn’t come today, you might not be out of bed tomorrow’. But the hope now is that I know there’s some partial progress and it’s getting better. It’s that wish, that belief that things will get right again. (Interviewee 24)
The search for technological solutions typical of this specific approach often led to a focus on partial results of laboratory or imaging tests. In relation to prognosis, people adopting the Technical approach preferred statistical data and used numerical expressions. The emphasis on objective test results was also linked to trust in the expertise of doctors or health professionals.
I feel hope, when the doctor comes, he says, ‘Here, we’ve made progress in this aspect. Overall, things are moving in the right direction, albeit slowly, but there is improvement. While there has been a slight setback in this area, it’s good, or it’s better by some measure. . . . I just have to trust them (the doctors), that they know what they’re doing and they’re doing it right. When I have that feeling and the numbers show it, that’s the hope. (Interviewee 24)
High information needs and proactive involvement in decision-making were related to this specific approach. Prognostic awareness was often high. These participants were aware of the severity and incurability of their disease. The unspoken hope of a complete cure is the driving force behind particular hopes, but the actual experience of hope is significantly influenced by the current results of subtests. The participants described the experience of hope, similarly, using a metaphor of a sinusoidal dependence on these outcomes:
That sinusoid of hope, depression, hope, depression, is unfortunately getting quite intense for me these last few months. (Interviewee 6) . . .of course, it’s a kind of a sinusoid, when you first hear the information. . . at first, you’re kind of freaked out, so you panic a little bit, and there are these phases where I learn something new, so I have to think about it for a while. . . . it’s a bit hard to take in at first, but after some of that thinking it’s like I’m at the stage where I understand what’s going on, I don’t know what situation I’m in, and I’m kind of at peace with the fact that there’s, there’s these possibilities, that it can just turn out good, it can turn out bad. (Interviewee 24)
In summary, the Technical approach to hope and prognostic awareness embodied a practical attitude to hope, focussing on concrete goals and technical solutions while drawing strength from the underlying hope to be cured completely. People with this approach used technical language and numbers to express their own experiences and their meanings. The hope varied according to the prognostic information.
Spiritual approach
This approach was characterized by a focus on generalised hope on the spiritual and existential level
34
. The hopes in this approach were not tied to specific outcomes or goals but rather to abstract concepts such as living in the present moment and embracing the essence of life itself, as one participant explained:
Well, I feel that hope is part of absolutely everything. It’s basically like breathing, yeah. (Interviewee 8)
For our participants with this approach, hope was found in the richness of the present moment, emphasizing the importance of cherishing each experience and connection. Rather than seeking tangible improvements or specific outcomes, they found relief in the simple joys of existence:
I was telling the oncology lady doctor, I could have walked more at that time, so I said: ‘Doctor, I’m going to the store now, I’m shopping, I’m totally happy’. She looked at me like that, she didn’t understand at all why I was happy when I have this disease. (Interviewee 22)
Trust in healthcare professionals transcended mere open communication. It reflected a belief in the expertise, compassion and empathy of medical caregivers:
What could health professionals do to strengthen that hope?
Do something that they might find hard to do. Really believe in the patient.
And believe him in what way?
Well, believe what he believes, what he says and what he thinks. . . . What he’s scared of like yeah. (Interviewee 8)
While people holding this approach may value communication, their coping strategies and decision making were more deeply anchored in faith and trust in healthcare professionals:
Well, the decision that I keep going, like I’m not giving up, and I’m just going to do everything that’s recommended to me by someone that I trust, I mean those doctors, it’s their job, they have records, so I go on, simply you don’t give up, well. (Interviewee 22)
Prognostic awareness varied among those participants, but their hope remained resilient, perceived as innate and invincible to prognostic information.
Do you feel it might take away someone’s hope if you tell them the truth about their medical condition?
No. It’s private, it’s just one’s own life. I mean it in the sense that we all have our own destiny, we all have our own karma. And either god is just gracious and sends us to the other world without talking to us about it, right, and we will experience it very gently, or he’s not gracious, or maybe he’s gracious too. . . but maybe he just needs something, so he solves it in different ways. (Interviewee 23)
In summary, the Spiritual approach to hope and prognostic awareness was characterized by a focus on generalized hope rooted in spiritual and existential levels, emphasizing abstract concepts like cherishing the present moment and embracing the essence of life. Despite varying levels of prognostic awareness, hope remained resilient and perceived as innate, transcending the influence of prognostic information.
Minimalist approach
The Minimalist approach was defined by a narrow and circumscribed outlook on hope. In terms of particularized hopes, people with this approach exhibited minimal emotional investment towards achieving specific objectives, displaying a sense of indifference. Similarly, regarding generalized hopes, they sometimes lacked motivation towards broader life goals or aspirations, demonstrating a passive or resigned attitude towards their pursuit. Their narrow view of things and brief responses to questions reflected a mindset characterized by scepticism.
What would you say hope is?
I don’t know, well. . . For now, keep going as long as you can. (Interviewee 10)
Well, there’s always hope.
And what would you say hope is, if there’s always hope, what would you say it is?
Well, I think one just has to believe in the better rather than the worse. (Interviewee 5)
Resignation expressed in this way was often related to a declared loss of hope for a complete cure. This led to a feeling of hopelessness. On closer examination, partial hopes emerged, but the overall reluctance to develop the theme of hope further referred to a loss of hope for recovery.
What do you hope for?
Well, I don’t hope for anything anymore, I’m just waiting for death, because there’s nothing else waiting for me.
And what keeps you going?
Well, what keeps me going is that I’m finally going to get out of the hospital, so I’m going to go to (town name), where they (my relatives) live. (Interviewee 19)
Partial hopes were often connected with family and independence. Moreover, hope was also tied to modest aspirations for improvement, although within the constraints of their narrow focus.
And speaking of hope, what do you hope for?
Well, I certainly hope that if I leave the hospital, I’ll walk on my own two feet and get better. And they won’t have to lead me by the hand.
Anything else you’re hoping for? Besides getting better?
Come on, it’s a lot to do with relationships, like home and stuff, that does a lot. (Interviewee 5)
People expressing this approach focussed more on personal acceptance and limited expectations rather than seeking reassurance or detailed communication from healthcare professionals. Thus, they indirectly reflected the Minimalist approach’s tendency to internalize struggles and maintain a self-reliant perspective on their medical situation:
The only way there can be hope is if the person is not terminally ill, they have some, they may have some things that can be healed, that’s what has hope. But when they are here in this hospice, they only give a definitive . . . . they have to be cancer patients and they have to have a definitive diagnosis of some kind, because they don’t treat in the hospice, they just wait in their own way for it to come and they take special care here, I am absolutely happy here because the nurses are helpful, which they can’t do in the hospital. . . (Interviewee 11) As the following illustrative quotations show, prognostic awareness varied among people with this approach, but the hope remained subdued and constrained by their narrow focus. And it’s just that everybody has this hope that they think they’re going to get cured, but they have to accept that if they’re told there’s a tumor on here, the tumor’s not going to shrink, it’s just going to progress. . . (Interviewee 11)
Some people want to know all the details of the examinations and their health condition and some people don’t want to know much. How about you, how much information do you need?
Well I don’t need to know everything. Who asks too much, learns too much. (Interviewee 2)
In summary, this approach is characterized by a modest outlook on hope. Although aspirations may be limited, participants adopting this approach found hope in enduring family ties, in the pursuit of modest improvements and in the ability to find contentment within the confines of their narrow focus.
Pragmatic approach
The Pragmatic approach was characterized by particularized hope mainly in affective and behavioural dimensions directed towards concrete everyday goals such as maintaining self-sufficiency, self-care or continuing leisure activities or hobbies. The outlook of people with this approach was grounded in realism, they found hope in the prospect of getting better and returning to a sense of normalcy or at least not getting worse, often centred around the comforts of home and the presence of family:
I’m a happy person, I look forward to every day, every moment. Yeah, and when my grandkids come to visit, they don’t live in town. So, I’m happy, I’m just in my element and I look forward to it so much always. Well, and the kids like yeah, I’m glad too yeah, because like I have them with me, yeah, I just know that, I’m just not alone. (Interviewee 1)
When I get help, it’s great.
So the nurses give you hope? Here, when they treat you well?
Yes, They do. (Interviewee 12)
Additionally, participants with this approach derived hope from the simple joys of the present moment, such as the companionship of a beloved pet or the routines of daily life:
Well, I hope that I’m going to be here as long as possible with the dog; I’ve got a three-year-old dog, so. I’d like to enjoy her. . . I guess that little bit of hope is definitely in everybody, but somebody believes more . . . But I think it’s more the kind of fanatical people who live by “I can do it because I have that hope”. I wouldn’t put it that way. (Interviewee 4)
Coping and managing are central themes for the individuals with the Pragmatic approach, reflecting their proactive approach to navigating their illness. They exhibited a strong determination to cope with challenges and manage their circumstances, refusing to succumb to despair:
No, I definitely don’t think about it every day. . . . It’s just the way it is and I live with it, yeah. Hoping it’ll get better or my back hurts, so maybe tomorrow it’ll get better. Yeah, I keep those little hopes alive, yeah. (Interviewee 15)
Refusing to admit defeat, they persevered with a sense of resilience and optimism, refusing to let their circumstances define them. Importantly, participants adhering this approach placed a strong emphasis on open communication with healthcare professionals, recognizing the importance of transparency and collaboration in managing their illness effectively:
I’m glad to know that diagnosis. To keep something from me is the hardest thing for me to handle. (Interviewee 16)
Prognostic awareness among those holding the Pragmatist approach was usually high and maintained stable regardless of the illness’s progression and medical information:
And do you think that hope is related to the information you get from the doctors?
I don’t know. You either have it in you, or you don’t.
So it doesn’t affect hope?
No, it doesn’t.
And how do you feel about hope?
If I didn’t have it, I probably wouldn’t be here. (Interviewee 12)
I have to think positive, and I want to, yeah, I still think that it’s going to be good, and I know it’s not going to be good, but I tell myself, it’ll be good. I’m breathing so far, so it’s great. Yeah, I’m not admitting it, well. (Interviewee 1)
In summary, this approach represented a pragmatic and determined attitude to hope and prognostic awareness, grounded in practical everyday life goals and a resilient spirit. The coping strategies of the participants holding this approach reflected a proactive, resilient mindset, characterized by a refusal to admit defeat and a strong emphasis on open communication and collaboration with healthcare professionals.
Discussion
Based on this phenomenological analysis, we identified four approaches to hope and prognostic awareness, characterized by distinct cognitive, behavioural and emotional patterns. These approaches are not fixed categories, as they can overlap, evolve over time and coexist within an individual. We did not find any differences among approaches regarding demographic variables or types of diagnosis which is in line with the outcomes of a review that did not find any relationship between hope and demographic and clinical variables. 35
We were particularly interested in the relationship between hope and prognostic awareness, and we found that only for some of these approaches does the hope change depending on the prognostic information. People taking the Spiritual and the Pragmatic approaches claim that their hope is stable and does not depend on external circumstances such as serious illness. The Pragmatic approach aligns with the concept of ‘living in hope’, which means reconciliation and comfort with life and death. 7 Accepting their life situation and prognosis can help people redirect their hopes and prepare well for the end of life in both practical and emotional ways.1,18
The Spiritual approach is in accordance with the version of hope as an essential, constant and enduring part of human existence. 25 Similarly, pre-intentional hope could be perceived as basic trust in the world or an existential feeling and is more likely to be connected with people with religious beliefs.26,27 Although this approach refers to spirituality, almost no participants mentioned religion or prayer as sources of hope. This is in accordance with the fact that the Czech Republic is among the least religious countries. 28
In contrast, for those who tend to follow the Technical and Minimalist approach, hope is a changing phenomenon and can oscillate between hopelessness and improvement over time depending on information from clinicians. According to a study focussed on the longitudinal dynamics of hope, despair and hopelessness, the nature of all three phenomena changed when the conditions changed. 36 Such findings correspond with the metaphor of the sinusoid of hope within the Technical approach.
The Minimalist approach does not refer to a resignation or lack of hope. This approach may emphasize the dynamic interplay between hope and hopelessness as described by Sachs et al. 37 which illustrates that hope acts as a coping mechanism against the existential threat of hopelessness, with acceptance of terminal prognosis fostering adaptive forms of hope. Conversely, hopelessness is described as a persistent, overwhelming state of mind. The Minimalist approach, while not equating to hopelessness, suggests that losing hope for a cure may result in a loss of generalized hopes, leading to a focus on particularized hopes accompanied by a narrowing of feelings and thinking where acceptance facilitates more specific and achievable forms of hope.
Our results align with the trinary conceptualization of prognostic awareness, 18 which categorizes patients as aware and accepting, aware and not accepting or truly unaware. While this framework captures key patterns, our findings reveal that hope can oscillate in some patients rather than fitting neatly into a static category, reflecting a more dynamic and fluid process.
Strengths and limitations
This study utilizes first-person narratives and provides authentic insights into the experience of hope in the context of terminal illness. The study benefits from a comprehensive perspective on the issues provided by the multidisciplinary research team. The inclusion of participants with various terminal illnesses beyond oncology broadens the scope of the study, enriching insights into hope across different medical conditions. Conducting interviews in both hospice and hospital settings allows for a contextualized examination of how hope is perceived and enacted within different care environments, enhancing the relevance and applicability of the findings.
Our study has several limitations that may influence the interpretation and applicability of its findings. The homogeneous Czech cultural background of the participants and the predominantly urban sample may have shaped the perspectives on hope and terminal illness presented in the study. Additionally, participants might have struggled to articulate their thoughts on the complex phenomenon of hope due to the nuanced distinctions between Czech terms ‘naděje’ (hope) and ‘doufat’ (to hope), which could have influenced the clarity and depth of the interview responses. These distinctions between hope as a noun and as a verb may have influenced how participants articulated their experiences of hope, potentially shaping their understanding of hope as either a static entity or a dynamic process, which in turn may have impacted the depth and clarity of their responses during the interviews. These contextual and linguistic factors should be considered when interpreting the findings.
Final considerations
This qualitative study offers valuable insights into the diverse experiences of hope among individuals with advanced incurable diseases. In clinical practice, understanding these nuanced approaches to hope can inform interventions and communication strategies for healthcare workers. People with the Technical approach require detailed information, but it is important for doctors to understand how even these partial medical findings can significantly influence their hope. On the contrary, for people with the Spiritual approach, it is not crucial to dissect medical findings in detail; rather, it is important to support their spiritual needs. In the case of the Minimalist approach, awareness that the person is not in deep despair or depression can help, focussing on supporting partial hopes and accepting that she may not be willing to engage in decision-making and care planning significantly. Conversely, planning care based on non-medical goals is appropriate for the Pragmatic approach. By tailoring communication styles and treatment recommendations to fit each individual’s approach to hope, healthcare workers can foster trust, enhance patient satisfaction and support better outcomes in end-of-life care settings.
Footnotes
Acknowledgements
We would like to thank Adéla Řežábková, Markéta Zindulková and Patricie Hanáková for their help with transcribing the interviews.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Czech Science Foundation (GACR), grant number 23-07747S.
Ethical approval
All participants received information about the study and signed an informed consent. Ethical approval from the Research Ethics Committee of the Third Faculty of Medicine, Charles University, was obtained on the 8 of June 2023 (Ref: PATH-01-2023).