
Abstract
Background:
Legacy building interventions are used in pediatric healthcare settings to help families cope with difficult healthcare experiences and typically reserved for intentional use at or near the end of a child’s life. However, little is known about how bereaved families perceive the concept of legacy that these practices are meant to address. Emerging research challenges the view of legacy as a standardized, handheld keepsake item but rather as a summation of qualities and experiences that affect those left behind. Therefore, more research is needed.
Aim:
To explore the legacy perceptions and experiences of bereaved parents/caregivers in an effort to inform legacy-oriented interventions in pediatric palliative care.
Design:
In this qualitative, phenomenological study grounded in social constructionist epistemology, bereaved parent/caregivers completed a semi-structured interview about their legacy perceptions and experiences. The interviews were audio-recorded, transcribed, and analyzed using an inductive, open coding approach grounded in psychological phenomenology.
Setting/participants:
Participants were parents/caregivers and one adult sibling of children (ages 6 months–18 years) that died between 2000 and 2018 at a children’s hospital in the Southeastern United States and spoke English as their primary language.
Results:
Sixteen parents/caregivers and one adult sibling were interviewed. Participants’ responses converged across three themes: (1) definitions of legacy, including traits and characteristics, impacts on others, and the child’s enduring presence; (2) manifestations of legacy, such as tangible items, experiences, traditions, and rituals, and altruism; and (3) factors perceived to affect legacy experiences, including characteristics of the child’s death and one’s personal grief process.
Conclusion:
Bereaved parents/caregivers define and experience their child’s legacy in ways and manifestations that conflict with current legacy building interventions used in pediatric healthcare settings. Thus, an immediate shift from standardized legacy-oriented care to individualized assessment and intervention is needed to provide high-quality patient- and family-centered pediatric palliative care.
Legacy building interventions are provided in most pediatric healthcare settings to help families cope with difficult healthcare experiences, typically the end of a child’s life.
These interventions often take the form of arts-based projects like plaster hand molds or painted handprints created at the time of a child’s death or immediately afterwards; little research has evaluated the effect of these interventions.
However, the legacy perceptions and experiences of bereaved parents/caregivers have yet to be explored, which compromises truly patient- and family-centered pediatric palliative care.
Bereaved parents/caregivers define legacy primarily as the child’s intangible qualities, shared experiences, and enduring impacts on the family and community.
Bereaved parents/caregivers do not refer to hand molds, handprints, or tangible keepsakes created in the hospital at the end of their child’s life as elements of their child’s legacy.
In addition, bereaved parents/caregivers describe their child’s legacy as targeted altruism efforts, rituals, or traditions that vary as a function of the child’s cause of death and the parent’s personal grief process.
Bereaved parents/caregivers define and experience their child’s legacy in ways and manifestations that conflict with current hospital-based legacy-oriented interventions.
These findings align with other recent studies on stakeholder perceptions of legacy, suggesting that current legacy building interventions are misnamed, and are instead the creation of keepsakes or mementos.
These findings necessitate a shift from standardized, tangible legacy-oriented interventions in healthcare settings to family-centered assessment and individualized care honoring a child and family’s unique personhood and history.
Background
The death of a child has significant and lasting effects on the physical and psychosocial wellbeing of parents/caregivers.1,2 In particular, bereaved parents/caregivers are understandably highly susceptible to psychological distress such as depressive symptoms, anxiety, and sleep disorders. 3 Perhaps related to these elements of distress, grieving parents report decreased psychological wellbeing and worsening social relationships which together can lead to poorer physical health and increased morbidity.2,4 As grief is known to be a subjective and personal experience, 5 and given the sensitivities needed to conduct research in this domain, 6 identifying effective grief support interventions is both challenging yet incredibly timely and necessary. 7
Legacy building interventions are arts-based techniques intended to help families cope with difficult healthcare experiences, including the impending loss of a child.8–10 Often, these legacy building interventions take the form of standardized, tangible creations like plaster hand molds, painted handprints, embossed footprints, or fingerprint jewelry made at or immediately after the time of death. This practice trend is still widespread today in 98% of children’s hospitals. 11 However, research evaluating the effects of these interventions on patient- and family-centered outcomes in pediatric end-of-life care is limited, in part due to insufficient understanding of legacy as a construct, intervention, and outcome.
Legacy research to date spans six continents and multiple cultural groups, primarily focusing on adult patients receiving palliative or end-of-life care.
10
However, emerging research suggests that these interventions could be feasible and beneficial for pediatric patients and their families independent of anticipated treatment or survival outcomes.10,11 Perceptions garnered from healthcare providers,
9
parent/caregivers of hospitalized children,
12
and pediatric patients ages 6–18 years
13
portray legacy as an individualized, experiential, relational, and transformative phenomenon. To this, a recent systematic review
10
reconceptualized legacy as:
. . .an enduring representation of the self – its qualities, experiences, effects, and relationships – built and bestowed across generations. Whether concrete or intangible, intentional, or serendipitous, legacies are avenues of connection, education, inspiration, or transformation (p. 13).
Accepting such a definition would require a paradigmatic shift in legacy-oriented intervention practices, moving from a procedural emphasis on tangible product provision to an emphasis on interpersonal experiences, relationships, and processes. In bereaved families especially, less is known about their legacy perceptions and experiences; although recent findings from parents who have experienced infant or perinatal loss 14 have provided confirmation of the definition above; Goldberg 14 found that infant or perinatal loss is also uniquely bounded by time, location, and development in ways that an older child’s death may not be. Therefore, additional research is necessary for developing legacy-oriented interventions that are truly evidence-informed.
Aims and objectives
The purpose of this study was to explore the legacy perceptions and experiences of bereaved parents/caregivers. With this information, providers can better understand and anticipate the legacy needs and experiences of this population and thus provide evidence-informed interventions and supports in pediatric palliative care.
Methods
This study involved inductive analytic analysis of in-depth interviews with bereaved parents/caregivers, informed by Moustakas’ psychological phenomenology. 15 Given the limited prior research on the legacy perceptions and experiences of bereaved parents/caregivers, the focus of this study was more on depth rather than breadth—characteristic of most qualitative approaches. Additionally, when investigating a phenomenon like legacy, which consists of concrete, relational, spiritual, and existential elements, Moustakas’ psychological phenomenology felt most appropriate. Blending insights from clinical therapies and Husserl’s 16 phenomenological philosophy, this approach to phenomenology offered a means for exploring both the essential structures and individual, perceptual differences of families navigating the death and legacy of a child.
Population
Eligibility criteria were: (1) primary parents/caregivers of children (aged 6 months–18 years) who died at the research site between January 2008 and December 2017, (2) spoke English as their first language, and (3) were over the age of 18 years. Exclusion criteria included those unwilling to provide consent to participate and non-English speaking. Additionally, families less than 24 months past their child’s death were not included in this study because they were still receiving mailed bereavement support from the hospital.
Sampling
Participants were recruited from a freestanding children’s hospital affiliated with an academic medical center in the Southeastern United States. This hospital serves a multi-state area with its level I trauma center, tertiary intensive care units, and more than 300 inpatient beds.
Recruitment
Eligible participants were identified through medical records and recruited through mailed letters that introduced the study. Participants who experienced the death of a child between 2008 and 2017 were selected due to the accessibility of the electronic medical records systems used during that time. The contact information of the principal investigator was provided within these letters, which was the avenue by which interested participants contacted and expressed their desire to participate. Providing study information by mail is consistent with what prior research has demonstrated about bereaved parent preference for research recruitment and participation. Grounded in patient- and family-centered care principles, every effort was made to extend choice and control to parents/caregivers who opted to participate.
Bereaved parents/caregivers were contacted between February 2020 and February 2021; participants for this study were recruited alongside a complementary study of parent/caregiver experiences of infant or perinatal loss. 14 The study team contacted all interested participants to discuss the study, answer questions, check eligibility, and complete the consent form. Once consent was completed, arrangements for an interview were made. All participants were offered the choice of location and medium of interview (in-person or via telephone), acknowledging that some participants might find the topic difficult to discuss in person.
Data collection
In-depth, semi-structured, phenomenological interviews explored bereaved parents/caregivers’ legacy experiences and perceptions. The semi-structured nature of the interviews allowed for collection of rich data. Interviews were conducted by members of the research team, and were audio-recorded and transcribed verbatim. The interview guide was informed by Moustakas’ psychological phenomenology, 15 while also aligning with the authors’ previous work on legacy perceptions in different stakeholder populations.9,12–14 Interview questions focused on the participants’ definition of legacy, their thoughts and feelings elicited by the word, and experiences in their lives that led them to define legacy in this way. Additionally, participants responded to questions about the sources of their legacy perceptions, and their experiences of their child’s legacy before, during, and after death. These interviews lasted between 30 and 150 min (M = 79 min), depending on what the participant chose to share.
Analysis
Interview recordings were transcribed verbatim, cross-checked, and then independently coded by two members of the research team using an inductive analytic approach developed from Moustakas’ psychological phenomenology (see Figure 1). 17 Analyzing in this way helped ensure interpretations were as fully grounded in participants’ thoughts, feelings, and experiences as possible, without imposing “a priori” researcher- or practitioner-driven frameworks.
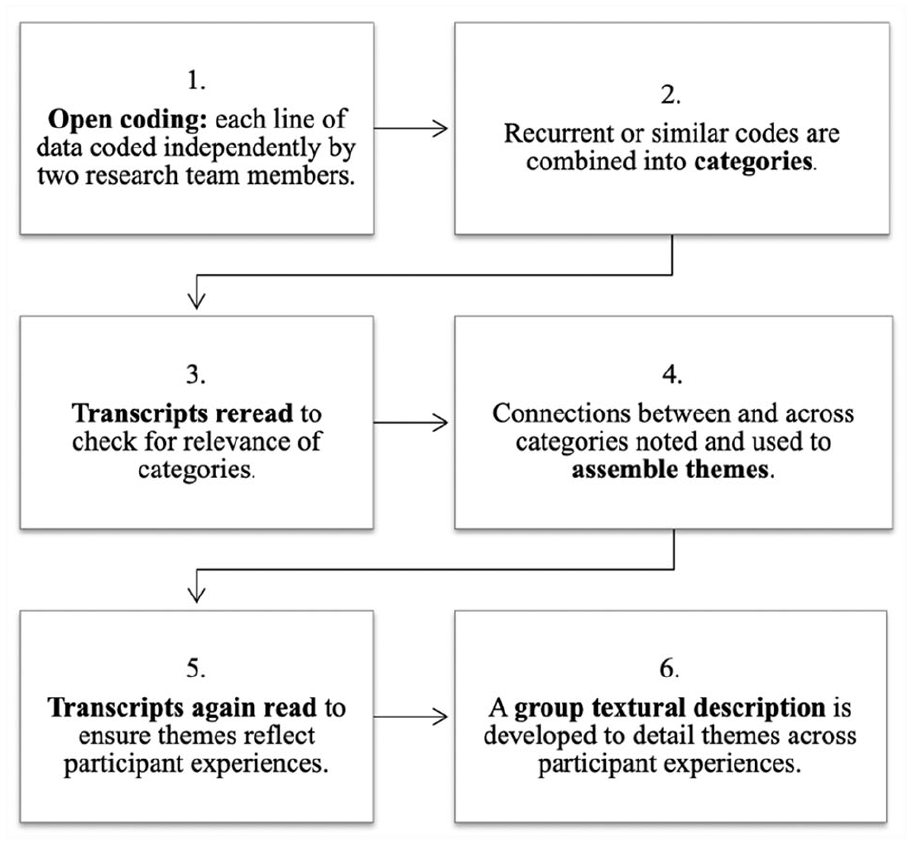
Data analysis procedures.
Ethical considerations
Full approval was obtained from the Vanderbilt University and Medical Center Institutional Review Board in January 2020 (protocol 171121), and all participants provided written consent for participation. Due to the sensitive subject matter of this study, the research team prioritized ethical considerations in the study design and conduct. For instance, in line with previous reports from bereaved parents, a non-invasive, opt-in approach to recruitment was used to avoid any possibility of coercion.18–21 Additionally, to mitigate undue discomfort and acknowledge the different types and intensities of grief that participants may be experiencing, each was able to choose their preferred medium and location for the study interview session. 14 All participants were able to receive information about the bereavement services at the research site should they need additional support. Finally, in line with best grief support and legacy building practices, each participant received a hand-written, individualized thank you note honoring their participation in the study and their willingness to share their child’s story and legacy with the research team.14,18,22
Results
Sample
Although more than 700 letters were mailed to eligible participants, 350 of these were returned to sender. Twenty-eight families contacted the research team in response to receiving the letter; of those, twelve decided not to participate (citing either lack of time or feeling emotionally unready to participate). Sixteen parents/caregivers and one adult sibling participated chose to participate and completed the study procedures (see Table 1). More than 70% of participants were mothers, and the majority experienced their child’s death in an intensive care unit (64.7%) due to a traumatic injury (35.3%), congenital condition (29.4%) or chronic illness (23.5%; Table 1).
Participant demographics.
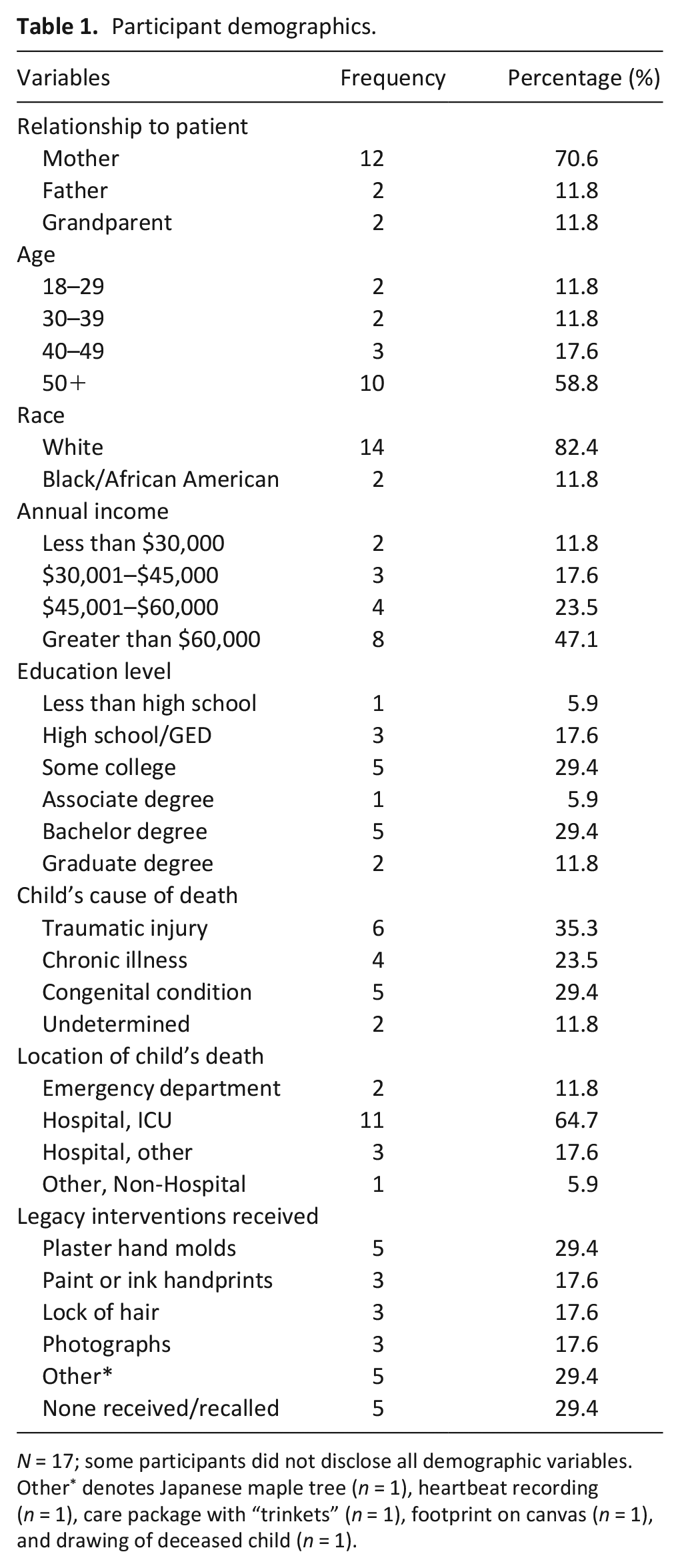
N = 17; some participants did not disclose all demographic variables. Other* denotes Japanese maple tree (n = 1), heartbeat recording (n = 1), care package with “trinkets” (n = 1), footprint on canvas (n = 1), and drawing of deceased child (n = 1).
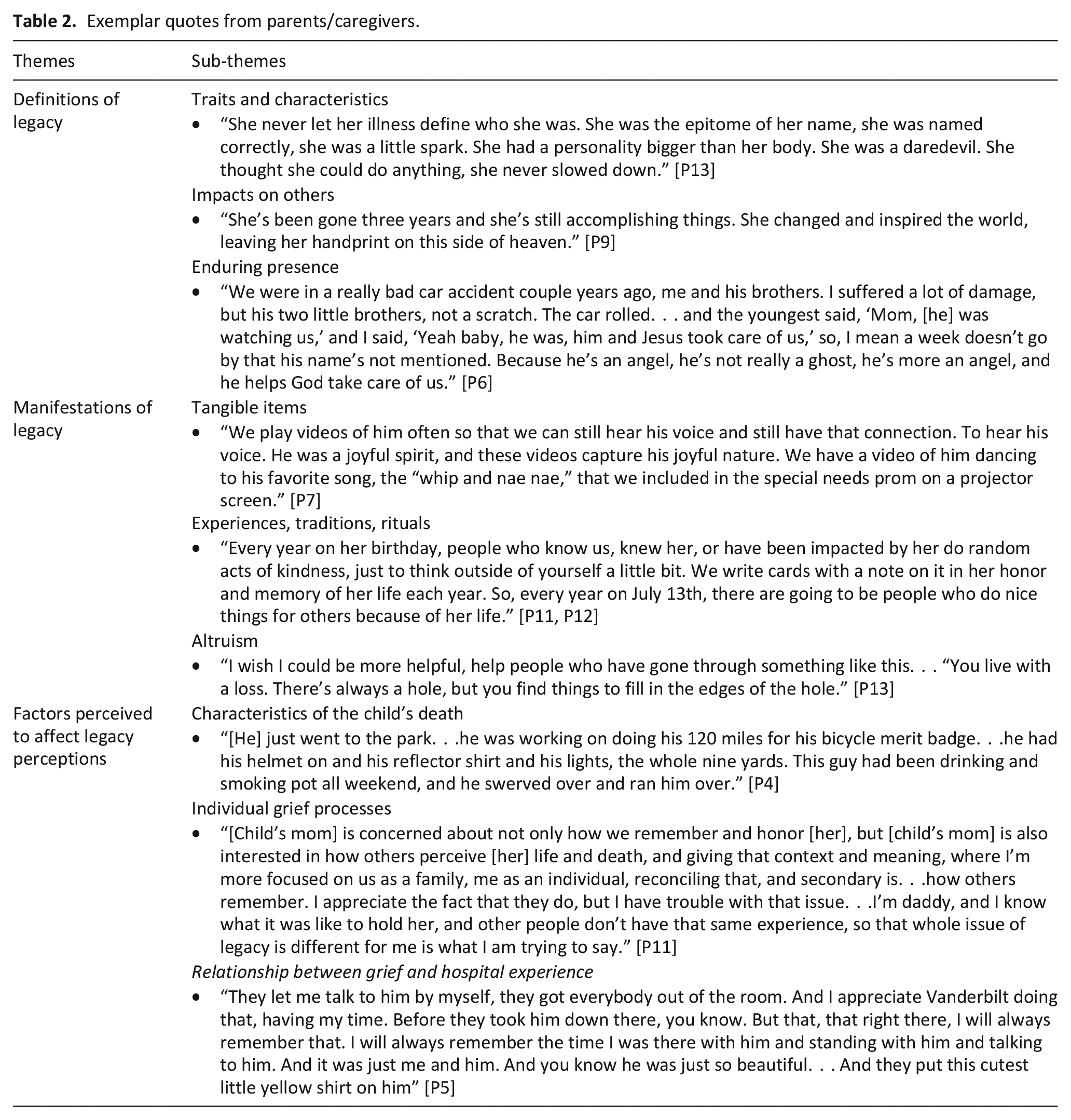
Participants described their legacy experiences and perceptions across three themes (Table 2): (1) definitions of legacy, (2) manifestations of legacy, and (3) factors perceived to affect legacy experiences.
Exemplar quotes from parents/caregivers.
Definitions of legacy
Several participants remarked on having only minimally considered the concept of legacy prior to their child’s death. These were often depersonalized references to “basketball stars or singers” (P5), “famous actors” (P1), or the “Star Wars” films (P2). However, once their child died, the word carried new relevance and meaning as a sum of their child’s unique traits and characteristics, the impacts they had on others, and their enduring presence.
Traits and characteristics
Participants described their children as “the most wonderful child you could ever meet” (P15), someone with a “strong sense of justice and kindness to others” (P16), “vibrant,” “meaningful, beautiful,” “happy,” “humble, caring, loving, and healthy” (P10)—each a reflection of the traits and characteristics they exemplified in life. One father who lost his teen daughter suddenly to unknown causes, reflected:
She was remarkable. . . loved everyone, could make friends with anyone. . . one of the one’s that could light up a room. . . make people laugh. A smart kid. . . and really sweet to everybody and really caring. . . selfless. . . even when she was young (P10).
Some shared how their child’s illness or condition contributed to their legacy, as one mother reflected, “had she not had Down Syndrome or a congenital heart defect, she wouldn’t have been able to create the legacy that she has left behind” (P9). Legacies were also connected to their child’s interests, hobbies, and accomplishments; one participant proudly shared his son’s accomplishments as a rising eagle scout, whereas another spoke often of her daughter’s involvement in local theater productions despite her chronic health conditions (P13).
Impacts on others
Multiple participants described legacy as a “lasting impression” (P16), “a continuation of history” (P17), and the elements of their child’s life that have subsequently motivated them to “do things differently or think differently because of having known her” (P8). One mother elaborated on her infant’s legacy sharing:
Her life has meaning and purpose and impact. . . she accomplished everything that she needed to. . . thinking about her legacy is realizing that. It was complete because of the parts of her that live on, because of the impact she had (P8).
Similarly, one father shared how his daughter’s life with special needs encouraged others to be more inclusive:
[She is] . . .continuing to effect people even though she is gone. She was able to reach a lot of people with the message of salvation through her life and death. It’s not something everybody does, but it is a very important part of our journey (P13).
Unprompted, all participants chose to reflect on their child’s lasting effects in their family and community as elements of their legacy.
Enduring presence
No matter their magnitude, legacies were described as transcending the bounds of life and death, as both a spiritual presence and enduring spirit. Participants reflected on feeling their child “watching over this hot mess of a family” (P6), providing comfort for surviving family members as if “part of her is still here. . .we feel her presence so much” (P16). One father reported, “I don’t feel bad about [remodeling her old bedroom]. I don’t need to go into her room to remember her because she’s all over the place, everywhere else” (P8). All participants described some belief in the continued presence of their child, though in different forms, with the insistence that “just because someone dies, doesn’t mean they’re gone” (P13).
Manifestations of legacy
Participants also offered examples of how their child’s legacy can manifest, or be represented, through tangible items; experiences, traditions, and rituals; and altruism.
Tangible items
Some participants described their child’s legacy through tangible items such as “tee ball trophies” (P10), initials written on personal belongings, handprints, memorial tattoos, and even a Japanese maple tree. One mother described putting “‘diva’ on her tombstone because she was the ultimate diva” (P13), while another spoke to “keeping [her son] alive” (P16) through photos and videos. Several referenced organ donation as a key component of their child’s legacy, recognizing the feeling that their child could “live on not just in our hearts but in a tangible sense” (P14) by “saving four lives and giving sight to two” (P7). None of the participants mentioned or discussed hospital-created plaster hand molds or painted handprints as elements of their child’s legacy, though these were recorded in the participant demographics survey.
Experiences, traditions, and rituals
Participants described charity events, honor walks, and remembrance events as manifestations of their child’s legacy. One mother reported:
My son loved to dance, and his life opened a door for others with special needs to enjoy something that he loved through the creation of this special needs prom. This event makes me feel good knowing my son’s life mattered to others. That they were here, and they were somebody, and they mattered (P7).
Multiple participants also mentioned experiences or rituals planned each year to honor their deceased child; one father and son duo noted how their family comes together on her birthday to visit her grave (P1, P2). Releasing balloons, posting pictures on social media, and “drinking milkshakes for breakfast” (P4) were also described as ways of representing and preserving the child’s legacy.
Altruism
Many participants shared how their child’s legacy served as inspiration “to do good,” and a “calling to do more, to be more” (P9). Altruism, “paying it forward,” or “doing anything you can to make a difference” (P7) helped several participants honor and carry on their child’s legacy. One mother whose son died by drowning expressed interest in creating a program to teach swim safety, to “save somebody else’s life” (P12). Another mother created a foundation in her child’s honor to fund research on congenital heart disease and Down Syndrome, reflecting “I feel like I get to continue on her legacy” (P9). Others created scholarships, gave endowments, coordinated hospital toy drives, and volunteered to help others as ways of representing the impact and inspiration their child’s legacy left behind.
Some participants described how the experience of losing a child has helped them channel their grief into serving others, because “that’s part of that process, that’s part of his legacy, and it’s not something you can leave out” (P7). Others described their child’s legacy as the motivation for participating in this study:
I understand how it feels to lose a child to various health problems. I don’t understand a lot of other things in this life, but I understand that. And I understand all of the different emotions. So that’s why I wanted to participate in this study thinking maybe down the road it will help somebody else (P14).
Though not always through formal organizations or events, many participants remarked on supporting or serving others as an important expression of their child’s legacy.
Factors perceived to affect legacy perceptions
Several participants identified how their child’s healthcare experiences, the characteristics of their death, and their own personal grief process shaped their legacy perceptions and experiences.
Healthcare experiences
Participants described how their child’s healthcare experiences, both positive and negative, impacted their perceptions of legacy. Some shared having “wonderful” (P6) experiences in the hospital marked by kindness, respect, and clear communication from providers and staff. One mother of an infant with a cardiac condition reported:
Everybody did such a wonderful job of reassuring us that she was not just a statistic and that she really did make an impact on their life as well. Child life was an angel to us. The nurse asked how I wanted to decorate her room and bed each day, it meant a lot to us being able to decorate her door. I still felt like I was able to care for her. I felt loved. Supported. Seen (P9).
Another participant shared how much it meant to her to bathe her child after death without feeling rushed by the team (P13), with others similarly recalling feeling “touched by the displays of care and concerns” as each one of their child’s medical providers “took time out of their busy day to come say goodbye” (P11, P12). These experiences of individualized and intentional care appeared to contribute to positive and dignified memories of their child’s last moments.
However, other families reported negative healthcare experiences at the end of their child’s life and identified how these moments influenced their perceptions of and engagement with their child’s legacy. As one pair of parents/caregivers shared:
[We] shut out a lot of things, other things become a blur, so that even a kind gesture to honor the legacy of a lost child such as a handprint can somehow get blurred into the background and is not as meaningful, so that’s an important part of honoring legacy (P11,12).
They also discussed challenges with staff communication, waiting hours for updates on their child’s condition, and how these embedded unwanted memories in their child’s legacy. They shared longing for a different set of memories around the end of their child’s life, and availability of support services delivered with a “high degree of empathy” (P12).
Characteristics of the child’s death
Especially in cases of traumatic death, participants intentionally framed their child’s legacy through positive shared experiences rather than the last moments of life. One mother who witnessed her son’s drowning, stated:
I think about the good stuff. I don’t even want to think about the time he was in the hospital. I think about the time when I was pregnant, when he walked for the first time, and came into my room every morning to tell me he loved me (P5).
One father described how his daughter’s unexpected and unknown cause of death complicates her legacy, leaving him sometimes focused on a perceived lack of police response rather than more peaceful memories (P1).
Conversely, participants who lost their child to chronic illness or congenital conditions described opportunities to build and honor their child’s legacy prior to death. One mother whose daughter died of a chronic cardiac condition recalled how, although unable to participate in sports, she turned to the arts to cope and build her legacy: “She never let her illness define who she was. She was very active in theater and in band. Everybody knew her. She was the epitome of her name; she was a little spark” (P13).
Individual grief process
Different grief responses were observed to shape participants’ engagement with and perceptions about their child’s legacy. For one mother who lost her child to a heart condition:
. . .the grieving process has been very different for [my husband] and I. I just want to talk about her, I want to say her name, anytime I hear anybody say her name I light up, and I am so grateful to be part of the Down Syndrome community. And my husband is too, it’s just really hard for him to see little blonde-headed girls with Down Syndrome. It just makes him retreat (P9).
Another caregiver shared, “trying to turn grief outward in a way, that’s how his mom dealt with it. Whereas, as our counselor said, I dealt with it like a storm cloud” (P11, P12). These differences were also described among siblings and extended family members:
Last Christmas [my mom] was writing the Christmas newsletter about the other grandkids and joked about putting ‘[Daughter] is still at Evergreen’ on the bottom - which is the cemetery where we buried her - but I knew people wouldn’t understand the joke. Most people don’t think our jokes are funny, but it’s part of the way we cope (P13).
In reflecting on the concept of legacy, one pair of participants defined legacy as “the individual and family process of healing and recovery from loss” (P11, P12), further illustrating the perceived relationship.
Discussion
Main findings
Participants described legacy as a compilation of their child’s unique traits and characteristics, the impacts they made on their families and communities, and their enduring presence beyond death. They saw their child’s legacy manifest in personal relationships, lasting traditions or rituals, memories of shared experiences, feelings of both love and grief, and even organ donation. Additionally, participants identified their child’s healthcare experiences, cause of death, and their own grief processes as factors shaping their beliefs about and engagement with their child’s legacy.
These findings align closely with recent research,3,9,10,12–14 articulating legacy as a representation of one’s intra- and interpersonal characteristics that endures after death and continues to impact those left behind. As Boles and Jones 10 note that legacy can be represented in “concrete or intangible, intentional or serendipitous” (p. 13) ways, bereaved parents/caregivers in this study primarily detailed facets of legacy that cannot be held or touched, but rather remembered and shared. This complicates the capacity for healthcare providers and support staff to sufficiently and meaningfully represent the child’s legacy in the standardized, tangible mediums of legacy building intervention practices that are currently in widespread use. 11 Although these items may serve a purpose in some cases as a memento or keepsake, it appears that these are not a component of what parents in this study described as their child’s legacy. This was also consistent with the perceptions of parents/caregivers who experienced perinatal or infant loss. 14
Results from this study highlight legacy as a process or experience rather than a product; perhaps a more appropriate name for plaster hand molds and other standardized activities is “mementos” or “keepsakes” as they fail to meet parents/caregivers’ legacy perceptions and needs. Instead of viewing or presenting legacy as these tangible products given to families at or near end of life, providers should instead recognize the traits, relationships, and shared experiences of the child and family as the integral elements of a legacy. With more attention to legacy in this vein, individualized pediatric palliative and end-of-life care may better buffer the interrelationship of the child’s healthcare experiences, mechanism of death, and parental grief as described by participants in this study and others. 14 Assessments of legacy needs should give priority to the quality of the child and family’s healthcare experience while providing meaningful opportunities to bolster family presence and engagement. Whether allowing family participation in elements of care, extended family visitation, making space for family private time or routines, or facilitated experiences such as going outside or visiting with a pet, all are legacy interventions as described by participants in this study.
Legacy, according to participants in this study, is in the expression and sharing of a child’s personhood and memories through experiential or artistic mediums across all domains of care. Providers should be proactively assessing and supporting families as they make transitions from the time of diagnosis onward. This can be done with simple prompts such as “Tell me a little about [child’s name],” or “What do we need to know about [child’s name] to take the best possible care of them?” In addition, active listening to families’ responses can help the team gather a sense of the child’s defining relationships, traits, and experiences that can be incorporated into keepsake creation and truly legacy-oriented interventions and supports.
Notably, some participants found therapeutic value in their involvement in this study; some shared that it had been several years since someone had said their child’s name, and that they appreciated having protected time to reflect on and describe their child’s legacy. As one set of parents shared:
Thank you for giving us the opportunity to share our hearts too, we appreciate this. . . even this small act ties into all that the hospital has done to honor [child’s name]’s legacy, it really matters that eight years later, you would call us and be interested in our opinion (P11, P12).
Perhaps, then, the genuine investment of time, energy, and emotional support as families share their stories of life, love, and loss may also be a feasible and meaningful opportunity to recognize and perpetuate children’s legacies—and something accomplishable within the scope of pediatric palliative and bereavement care.
What this study adds?
This study contributes first-hand insights into legacy as it is experienced by bereaved parents/caregivers which necessitates a shift from standardized, tangible legacy-oriented interventions in hospital- and home-based end-of-life care settings to family-centered assessment and individualized care that honors a child’s unique personhood and history.
Strengths and limitations
Exploring perceptions from the perspectives of bereaved parents themselves, using an in-depth phenomenological approach and an inductive, open coding scheme yielded more insightful data than any previously available. However, these were drawn from a singular healthcare institution and participants were somewhat homogeneous in terms of race and socioeconomic status. Future research should employ multi-site study design and recruit minority and marginalized populations to assess legacy perceptions across diverse groups and broaden current understandings.
Conclusion
Participants in this study described their child’s legacy in ways that both resonated with and challenged current clinical conceptions of legacy interventions in healthcare settings. By assessing and attending to the individuality of pediatric patients and families, clinicians can facilitate legacy experiences that prioritize subjective components of grief like adaptive coping and continued healing. When these results are considered alongside the legacy perceptions of pediatric healthcare providers, 9 parents/caregivers of hospitalized children, 12 and pediatric patients themselves, 13 reconceptualizing legacy becomes necessary, specifically as a shift away from tangible product to a therapeutic process.
Footnotes
Author contributions
Ms. Jones recruited participants; led data collection, analysis, and interpretation; drafted the initial manuscript; reviewed and revised the manuscript; and approved the final manuscript as submitted. Ms. Albanese participated in data collection, analysis, and interpretations; drafted the initial manuscript. Dr. Boles conceptualized and designed the study; recruited participants; supervised and participated in data collection, analysis, and interpretations; critically reviewed and revised the manuscript; and approved the final manuscript as submitted.
Data availability statement
Due to the small sample size and high risk of breach of confidentiality, data from this study are not available.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
Full IRB review and approval was obtained from the research site in January 2020 (protocol 171121), and all participants provided written consent for participation.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.