
Abstract
Background:
Paediatric end-of-life care is an important part of palliative care, and provides care and support for children in the last days, weeks, months or year of life. However, there is currently a picture of inconsistent and disjointed provision. Despite differences in delivery models across countries and cultures, healthcare professionals need to be able to support families through this difficult time. However, there is limited evidence to base high quality end-of-life care.
Aim:
To explore healthcare professionals’ experiences of delivering end-of-life care to infants, children and young people, their needs and the factors affecting access and implementation.
Design:
Qualitative study employing online focus groups, analysed using framework analysis.
Setting/participants:
Healthcare professionals who provided end-of-life care to infants, children and young people, across cancer centres and neonatal and paediatric intensive care units.
Results:
A total of 168 professionals from 13 tertiary hospitals participated in 23 focus groups. Three themes highlighted many barriers to delivering optimal care: (1) Professional perceptions of end-of-life care; (2) What we want to provide versus what we can and (3) Workforce and sustainability: Healthcare professional support. These illustrate professionals’ awareness and desire to deliver high-quality care, yet are constrained by a number of factors, suggesting the current system is not suitable.
Conclusions:
This study provides an in-depth exploration of paediatric end-of-life care, from those professionals working across the settings accounting for the majority of end-of-life care delivery. Many of these issues could be resolved by investment in: funding, time, education and support to enable delivery of increasingly complex end-of-life care.
Despite differences in delivery models of paediatric palliative care across countries and cultures, healthcare professionals need to be able to support families through this difficult time.
Paediatric palliative care is not adequately covered in professional training and healthcare professionals are lacking in confidence in delivery.
There is little research evidence on how to provide high quality end-of-life care for infants, children and young people.
Societal expectations, and perceived readiness on the part of parents and professionals, both impacted significantly on the [timeliness of] introduction of paediatric palliative care.
The environment is important for both families and professionals when their child is at end of life. Currently, not all settings have the necessary bereavement facilities available.
Formalised wellbeing support for healthcare professionals was often inaccessible and required investment.
There is an urgent need for improved formalised wellbeing services for professionals who provide paediatric end-of-life care.
Investment in structured training and development surrounding end-of-life care, particularly, facilitating end-of-life care conversations are necessary to help build upon confidence levels and encourage a joint approach to providing this care.
Bereavement facilities and support services for families must be made available to ensure all families are offered choices surrounding location of care and bereavement support.
Background
Despite the marked improvement in infant and child mortality over recent decades, more than seven million infants and children still die worldwide every year. 1 These infants and children should receive high quality palliative care defined as ‘an active and total approach to care, beginning from diagnosis or recognition and continuing throughout the child’s life and death’. 2 End-of-life care is an important part of palliative care, and provides care and support for children and their families in the last days, weeks, months or year of life.3,4
The number of paediatric palliative care services that contribute to end-of-life care for children is increasing worldwide.5,6 However, availability and access differ across countries. Whilst there are improvements in provision, the ways in which this type of care is organised are often still inconsistent and incoherent, with little evaluation of this care.7,8 As per the rest of the world, in the United Kingdom, there is a similar picture of inconsistent and disjointed provision.2,9,10 Despite differences in delivery models across countries and cultures, healthcare professionals need to be able to support families through this difficult time. This should be a common key component of palliative and end-of-life care, whatever the setting. However, evidence has shown paediatric palliative care may not be adequately covered in professional training 11 and professionals have been described as lacking confidence in delivering aspects of this care. 12
To standardise and improve children’s end-of-life care in England, the National Institute for Health and Care Excellence (NICE) 13 developed clinical guidance in 2016 9 and in 2017 set six clinical standards. However, the guidance are based upon low quality evidence, often from North America, with elements not applicable to the United Kingdom-based healthcare system. 10 A subsequent survey conducted in the United Kingdom 14 found palliative care referral occurred late or did not occur at all, due to its negative connotations. 15 All of which raises implications for quality of care and potential impacts on families as further evidence is necessary to better understand professionals’ experiences and needs. 8
There is a need for improvements in both healthcare professionals’ experiences of delivering end-of-life care, and families’ experiences of receiving this type of care for their child. In order to improve care, current provision needs to be evaluated and guidelines must be underpinned by high-quality evidence, which includes the voices of the healthcare professionals themselves.
Therefore, the aim of this study was to explore healthcare professionals’ experiences of delivering end-of-life care to infants, children and young people, their needs and the factors affecting access to and implementation, within United Kingdom National Health Service Settings.
Methods
Study design
This paper reports the second workstream of a major United Kingdom study ‘End of Life Care for Infants, Children and Young People: a mixed methods evaluation of current practice in the United Kingdom’ (the ENHANCE study). 16 This workstream used qualitative methods with online focus groups to build upon our previous findings 17 of how previously identified components of care operate in routine practice and enabled the comparison of data across different care delivery settings.
Setting
The development of palliative care services for children and young people in the United Kingdom was unplanned and developed locally. Provision often relies heavily on individual health professionals and third-sector organisations, 17 particularly children’s hospices. 6 This inequity in provision, with patchy geographical distribution, and differing models of care, means provision may be of a good quality in some areas, but in others it is unclear what is being provided, by whom, and how.
Children with life-limiting conditions are frequently admitted to hospital within the last year of their life, with more than 70% of children in the United Kingdom dying in hospital settings, 18 although admissions vary significantly across the type and number of conditions. 19 In the United Kingdom, four National Health Service settings account for the care of more than 60% of children in the last year of their life2,20 –22 and were therefore the settings focussed upon in this study 16 : principal treatment centres for cancer for children or for teenagers and young adults’, neonatal and paediatric intensive care units. Within these settings, there are multidisciplinary teams, some of which also incorporate other health professionals from other services, such as children’s hospices. The nature and level of their involvement differs depending on the model of care. Workstream 1 findings highlighted the ways in which these settings operationalised components of care and therefore how care was delivered differed. 23 Therefore, sites were selected based upon the need to capture this variation in provision.
Participants
Healthcare professionals; defined as those identified in our previous workstream 17 for example, doctors, nurse, spiritual staff, family support worker, social worker etc. working in the four settings above, were invited to take part if they were involved in the delivery of end-of-life care to infants, children and young people. Those who worked in other care settings, such as children’s hospices, which fed into the delivery of end-of-life care and regularly worked as part of a multi-disciplinary team in one of these settings, were also invited. This enabled the multidisciplinary nature of paediatric palliative care to be captured.
Sampling
Purposive sampling was used to ensure representation of all United Kingdom nations, geographical locations and diverse experiences across settings until data saturation had been reached; once no new information had been gathered (determined using codebooks and initial concepts gathered after focus groups). Data saturation was an appropriate concept for data sufficiency as this related to our use of purposeful sampling 24 ;to gather representative experiences from four unit types. Due to the need to capture variations in provision, highlighted in workstream 1; the heterogeneity of both the setting and the population; and the multidisciplinary nature of paediatric palliative care, hence the range of professionals involved, a large sample size was needed.
Recruitment
Principal investigators at participating sites circulated recruitment materials to those who were involved in the delivery of end-of-life care. Interested potential participants were provided with more detailed study information from the research team and an invitation to join an online focus group. Recruitment took place between July 2022 and July 2023. All participants provided written consent via an online form.
Data collection
Online focus groups25,26 (run by unit type) took place via video-call and were facilitated by experienced team members (all applied health researchers: EVM, JH, LB - all female; GP and AP - both male) who were previously unknown to participants. Focus groups were utilised to explore how components of care, which had been previously identified in workstream 1, 16 were operationalised within multidisciplinary teams, to explore all experiences of care delivery. Two team members facilitated each group using the semi-structured topic guide for example, topics included setting, team structure, experiences of providing care (Supplemental File 1), which acted as an aid to help cover set questions and additional topics. Field notes assisted with analysis. Focus groups were audio-recorded verbatim, transcribed and uploaded onto NVivo 12 . Transcripts were not returned to participants.
Data collection continued until saturation had been reached. 24 This was assessed throughout data collection and analysis. Throughout data collection, all researchers debriefed with JH after focus groups. Two-weekly group meetings were also held with the researchers involved in data collection (JH, EM, GP and LB) and our PPI-partner (GW). The purpose of these meetings was to debrief as a group and to discuss ideas, codes and possible themes from the focus groups. This enabled informed decisions to be made about whether to continue data collection, stop it or modify research methodologies to explore areas that lacked enough saturation. 27 Data analysis began whilst data collection continued. This enabled confidence in consistency of recurring codes and categories and ensured data had been fully explored, understood and used to their full potential to achieve the required study aims. 28
Data analysis
Data were analysed using a framework analysis method29,30 guided by the analytical framework designed in our previous workstream (Table 1). 17 The use of framework analysis assisted in managing an extensive dataset whilst still obtaining a thematic overview.29,30 The analysis process was performed by one team member EVM and reviewed with the wider team (JH, LB, GP, GW, LKF and FH). Participants did not provide feedback of the findings. There were five stages to the analysis process:
Workstream 1 findings indicator framework. 16
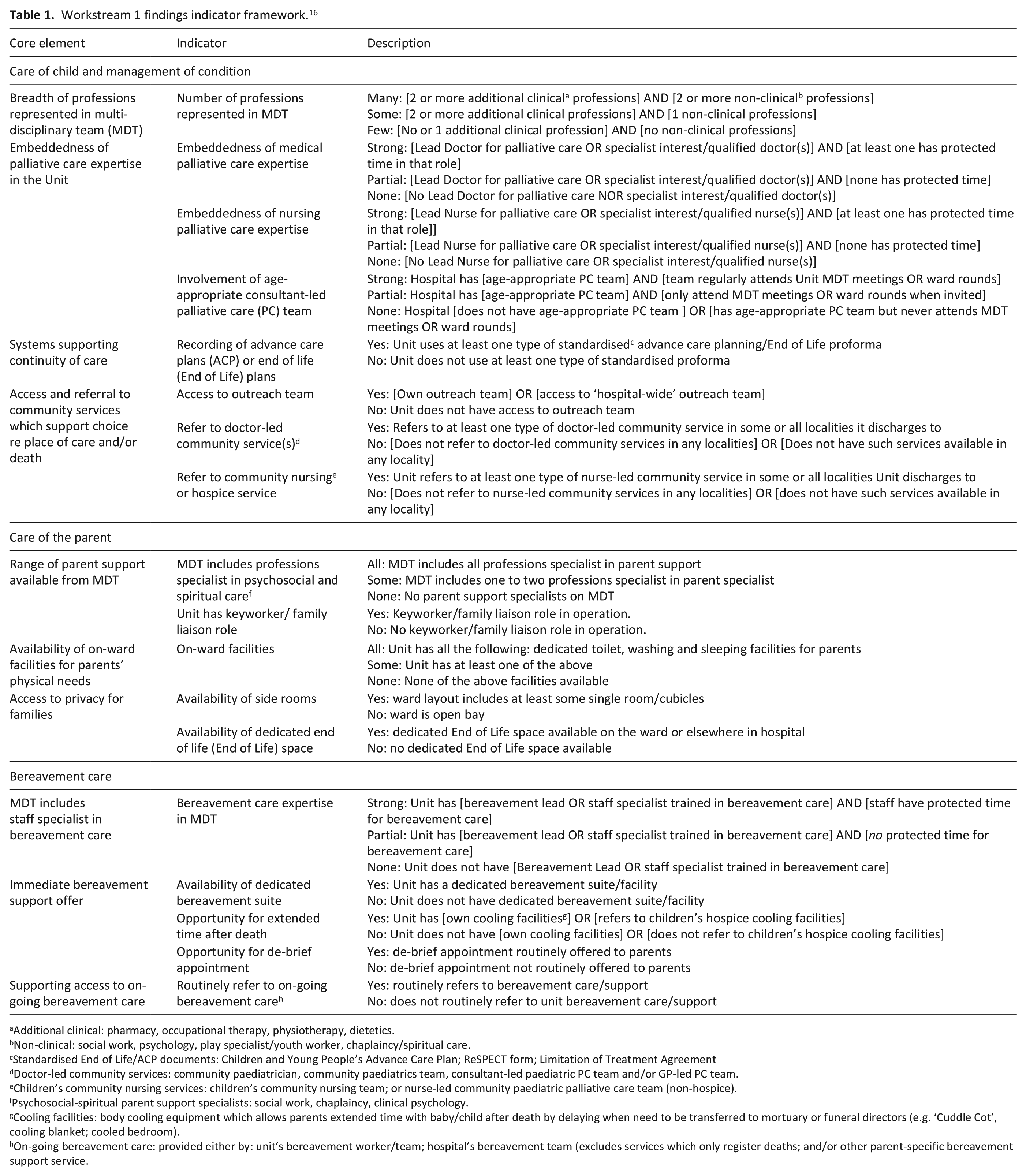
Additional clinical: pharmacy, occupational therapy, physiotherapy, dietetics.
Non-clinical: social work, psychology, play specialist/youth worker, chaplaincy/spiritual care.
Standardised End of Life/ACP documents: Children and Young People’s Advance Care Plan; ReSPECT form; Limitation of Treatment Agreement
Doctor-led community services: community paediatrician, community paediatrics team, consultant-led paediatric PC team and/or GP-led PC team.
Children’s community nursing services: children’s community nursing team; or nurse-led community paediatric palliative care team (non-hospice).
Psychosocial-spiritual parent support specialists: social work, chaplaincy, clinical psychology.
Cooling facilities: body cooling equipment which allows parents extended time with baby/child after death by delaying when need to be transferred to mortuary or funeral directors (e.g. ‘Cuddle Cot’, cooling blanket; cooled bedroom).
On-going bereavement care: provided either by: unit’s bereavement worker/team; hospital’s bereavement team (excludes services which only register deaths; and/or other parent-specific bereavement support service.
Ethical considerations
United Kingdom-wide approvals were obtained from the Health Research Authority and Health and Care Research Wales (20/01/2022, 300913) and West of Scotland Research Ethics Service (21/WS/0170).
Patient and public involvement
Bereaved parents (n = 15) who were members of the Project Advisory Group, assisted with the study design, the content and layout of the recruitment materials and the topic guide. Initial findings and analysis were shared and discussed. Our parent co-author, a bereaved parent (GW), guided the data collection and contributed to the analysis.
Reflexivity statement
Data collection and analysis members were majority female, all represented variety of perspectives (health professionals, public health, policy, methodological) with various levels of prior exposure/knowledge in end-of-life care. External stakeholders provided additional perspectives and created a more balanced gendered team. To allow for transparency, meetings (conducted at all stages) to discuss and reflect upon potential biases were held on a two-weekly bias.
Results
Sample
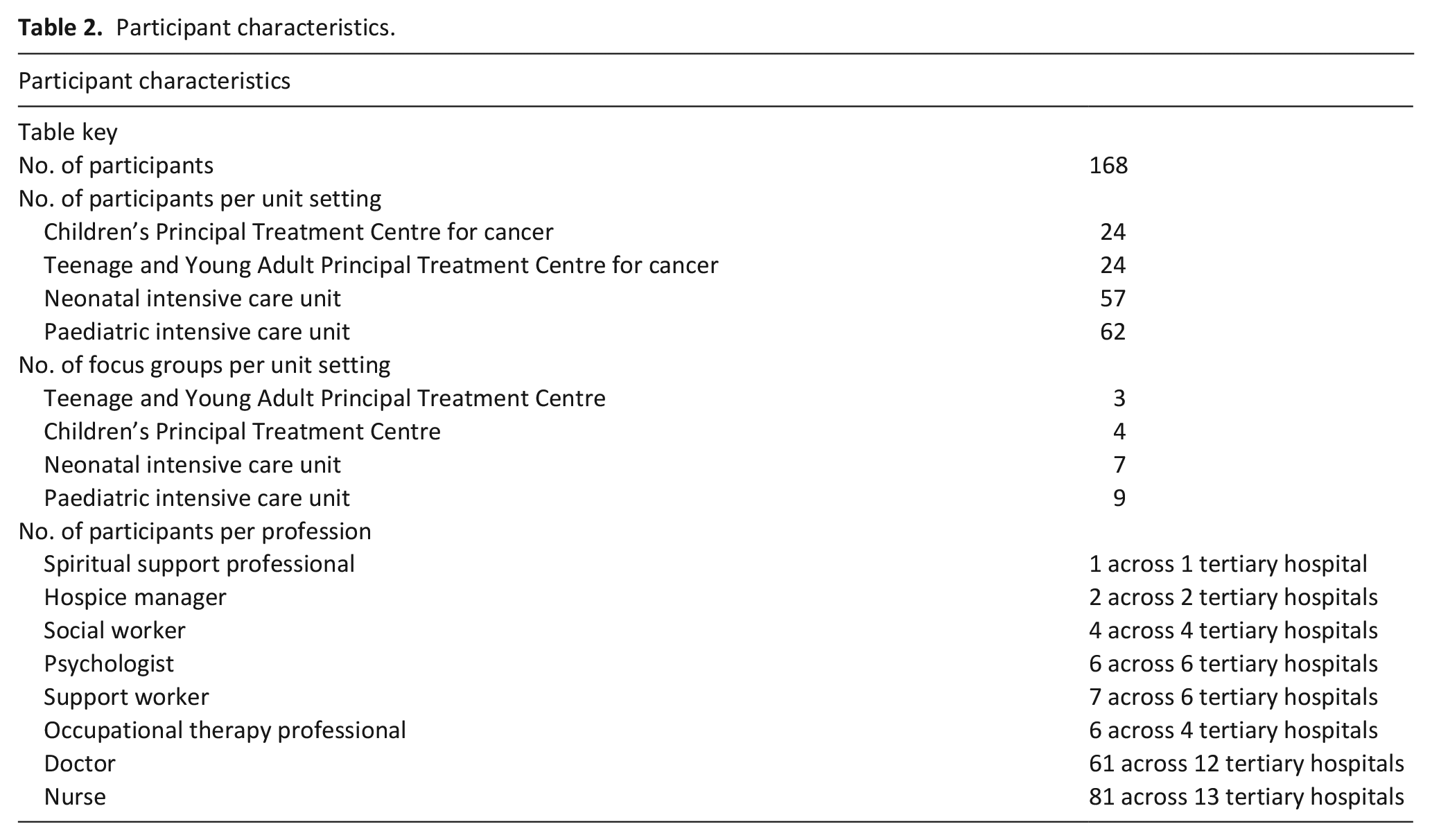
Healthcare professionals (n = 168) from 13 tertiary hospitals participated in 23 focus groups with a range of components of end-of-life care as identified in our previous workstream, 17 (Table 2). It is understood that our sample is large, however, our previous workstream identified variation within and between settings in terms of whether and how core elements of end-of-life care were provided. Distinct models of care were not able to be obtained due to the level of variation, with 10 core components of care identified. All United Kingdom nations and diverse geographical locations and experiences were represented. 17 Therefore, this resulted in a large sample size. Additionally, we wanted to ensure we had representation of all types of professionals involved in delivering paediatric end-of-life care in acute settings. Mean focus group length was 1 h 18 min (range = 1 h 07 min to 2 h 4 min).
Participant characteristics.
Themes
There are three main themes (
Theme overview.
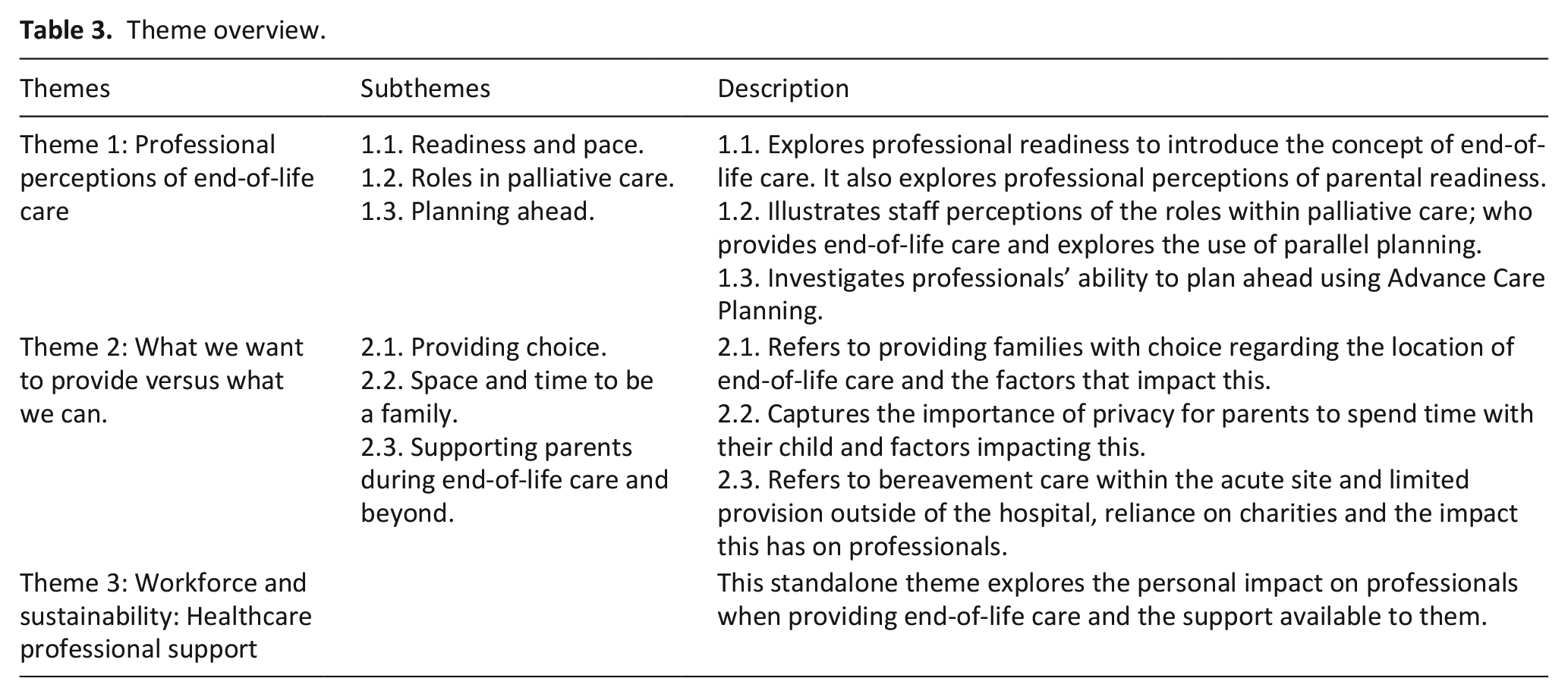
Theme 1: Professional perceptions of end-of-life care
Subtheme 1.1: Readiness and pace
Across all units, professionals believed conversations with families regarding end-of-life care should take place as early as possible as this made for a smoother process. However, professionals recognised it was necessary to be sensitive to a family’s individual situation and continue at their pace.
As a consultant, often you’re the person that’s leading those conversations, and as I have probably got more experience. . . you really have to go at the pace of the parents. (Doctor 05-117, Neonatal intensive care unit)
However, professionals found this complex as not all families were ready to discuss or think about the concept of end of life, despite professionals believing it was in the best interests of the patient. This meant that professionals found themselves advocating for both, the patient and parents.
We have had incidences where both parents are not in agreement, so then that kind of delays and then you have to try and advocate for both and what’s [in] the best interest for the baby. (Hospice manager 12-03, Neonatal intensive care unit)
There were instances of when families were thought to be focussed on curative management and were advocating for professionals to continue treatment. This had an impact on professionals, provoking feelings of emotion as both parties disagreed of which treatment approach to take.
We’ve had a few patients that, you know, maybe the parent. . . you’ll say, “No, this is not going to work” but they are insistent that you do something, and that’s something very difficult for the team. (Nurse 14-143, Children’s Principal Treatment Centre)
Neonatal and paediatric intensive care professionals felt parental expectations and focus on curative management was often influenced by their child’s previous admissions and interventions. Life-saving treatments meant parents held onto the belief that curative treatment would be successful. Success in medical advances and increased treatment options further complicated this, often meaning professionals struggled to negotiate which approach to discuss with families.
These parents that have cared for their fifteen-year-old child from the moment . . . [they had] had a hypoxic delivery . . . their world revolves around them. They believe their child does have a quality of life . . . the conversations that we try and have with them when they’re ventilated about quality of life isn’t something that’s acceptable . . . They want to do everything they can (Nurse 04-40, Paediatric intensive care unit)
Additionally, with the ease in accessing information via medical observations, and the internet, parents had more of an awareness and understanding of their child’s condition. Professionals then struggled to manage expectations.
It’s also made more challenging by foetal medicine [being] so much more advanced as a speciality . . . they get an awful lot of input and surveillance during the pregnancy . . . They’re so much more able to seek their own information . . . scenarios where things might be better than is perhaps portrayed (Doctor 10-38, Neonatal intensive care unit)
Differing perspectives on the best approach was further complicated by family’s decisions to have legal or media involvement. Professionals found this made it difficult for end-of-life care to progress.
Different opinions on, rightly or wrongly, what we’re doing with care for our children, and I think sometimes that can get quite heated at the point of death or at the point of arrest, which can then make it extra challenging for everybody. . . Cases that have been in the media [or] have gone to court (Nurse 02-25, Paediatric intensive care unit)
To progress with end-of-life care, some professionals introduced the palliative care team/consultant. However, they found this was often met with resistance from some families. To help lessen this, professionals avoided the word ‘palliative’ and would refer to it as ‘parallel planning’ in hopes that families would accept this more readily.
Some people get really uncomfortable with the word hospice, they get really uncomfortable with the word palliative so it’s about reframing what those are . . . Sometimes I don’t introduce myself as the palliative care consultant, I kind of go, “I’m here to help with symptoms” (Doctor 19-134, Paediatric intensive care unit)
Readiness to embrace a palliative approach and engage in conversations about end-of-life care were complex and multi-layered. Professionals from paediatric intensive care and cancer centres struggled as some parents did not want their child to be aware of their prognosis, leaving professionals in a difficult position. Although recognising it was an extremely difficult situation, professionals still emphasised the importance of advocating for the child to ensure their interests are at the forefront of decisions.
That’s really hard. I can’t imagine how hard it would be if you were the parent but actually, we are also advocating for the child, the child is our patient. (Doctor 07-10, Teenage and Young Adult Principal Treatment Centre)
Professionals themselves described struggling with moving to a palliative care approach. Those working in cancer units avoided direct language and the importance of maintaining hope for example, a clinical trial change the trajectory.
So, you’re maybe not saying, “Right, now this is it,” you know, it’s not to take away hope . . . “The outlook is very poor.” So, I think it’s what the family want to take from that. (Social worker 14-149, Children’s Principal Treatment Centre)
Professionals admitted to not being ready to have such conversations. They positioned this as reflected upon their desire to want to make children better. For those working in acute settings, such as paediatric intensive care, they talked about their role in a child’s care as often being about ‘fixing’ a new and urgent issue, rather than focussing on the long-term situation.
In the intensive care we’re more focused on the acute bits and sometimes we are trying to fix the problem . . . it may not be the right thing to try and fix something . . . (a) is not fixable but (b) might be causing more harm or pain to the child and maybe this is not the right time. (Doctor 19-139, Paediatric intensive care unit)
The promotion of active treatment and hesitation to include a palliative care team approach meant at times, referrals to the palliative care team and the introduction of parallel planning occurred later. For professionals, particularly those from cancer units, there were real barriers to the introduction of palliative care.
The push is for active treatment and cure for much of the journey it’s a really difficult shift to start to consider . . . that’s goes for the clinicians as well. . . . it really does take for someone . . . to say, “Maybe we need to think about palliative care.” . . . We are often introduced later [to parents] than we would wish. (Doctor 05-83, Children’s Principal Treatment Centre)
To assist with the introduction of the end of life pathway, professionals identified time to build meaningful relationships as important, but often impossible due to shift patterns and limited experience.
Shift pattern makes it nigh impossible to follow a case through to develop a natural rapport with families . . . It’s just near impossible to develop any kind of meaningful interaction with families . . . You get used to dealing with things on a shift-by-shift basis. . .“That’s tomorrow’s shift’s problem” (Doctor 10-34, Paediatric intensive care unit)
Low confidence levels and difficulties moving to a palliative approach meant operationalising and leading these conversations became disjointed. Responsibilities sometimes appeared to fall upon others.
There’s lots of staff shy away from end-of-life care and it gets to the point where there’s the same staff over and over again . . . the people that are on the bereavement team, if there’s a baby that is heading towards end-of-life care, you’ll tend to find that people will look to us as if, “Oh, you’re the only ones that can do that.” (Nurse 06-63, Neonatal intensive care unit)
This had implications for paediatric intensive care professionals as, at times, pressure was placed upon them by others to avoid discussing such topics. This meant the introduction of end-of-life care was much later.
Paediatricians generally are people that like working with kids and the thought of children dying is something they’re not very comfortable with. People think, “Well, the PICU (Paediatric intensive care unit) lot are the tough people that have these conversations and deal with that, along with palliative care” It’s just left until the eleventh hour. (Doctor 04-46, Paediatric intensive care unit)
Subtheme 1.2: Roles in palliative care
Professionals from all unit settings emphasised the importance of working together as a multidisciplinary team when taking a palliative approach. Despite believing this, the role and involvement of the palliative care team varied. In some settings, involvement would be from the very beginning for all patients, whereas others used a referral process (based upon course of illness).
From a palliative care point of view, we visit children on practically every single ward and unit in the hospital. (Nurse 02-29, Paediatric intensive care unit)
Many believed there was room for improvement in joint working. For some, there needed to be a better understanding of the role of palliative care. At times, some professionals still perceived it as only referring to the very end of life (last weeks of life) meaning that referrals and parallel planning may be later.
There’s still a way to go in terms of changing that mindset into . . ., starting those conversations earlier with parallel planning . . . really kind of taking the message that palliative care isn’t end-of-life care . . . if you’ve had a good set-up early then it makes the end-of-life conversations and approach a lot easier. (Doctor 06-66, Neonatal intensive care unit)
Professionals reflected upon automatic referrals to palliative care for specific patient groups for example, those with life-limiting conditions. This was thought beneficial in engaging families and professionals, and lessening fears and anxieties.
It’s been part of their normal care to be referred to palliative care either antenatally or just after being born, so then parents don’t feel like, “Why are you just specifically coming to us?” If they feel like it’s just part of the medical care, it’s not as scary. (Nurse 03-17, Paediatric intensive care unit)
Alternatively, there were also instances of when professionals felt the role of palliative care could be provided by themselves, without the need to refer to a specialist team unless necessary. This was particularly the case for those from cancer units.
This is a phrase that you lot are pushing upon us, you research-y types that want to make it into a special thing, and we don’t see it that way because we’re . . . specialists! . . . Who’s done . . . training, . . . in our particular service it’s unusual that we have to involve them, although we’ve got no problem at all with working with them [when asked if there was palliative care team involvement] (Doctor 04-48, Children’s Principal Treatment Centre)
Necessary involvement referred to symptom management plans or assisting specific patient groups. Although some professionals still felt that their skillset meant they could provide symptom management plans, avoiding the need for a joint approach.
For the vast majority of our babies we don’t really need complex symptom management plans. Certainly, drug-related sort of symptom management plans is very different . . . I feel we provide very comfortable end-of-life care . . . as most places do around the country without needing, you know, sort of very detailed symptom management plans (Doctor 10-38, Neonatal intensive care unit)
For many, the palliative care team was described as being designed to be a separate service within the hospital. This way of working contributed to the palliative care team not being involved. Although professionals recognised this and wanted it to change.
[Patients and parents are] not introduced to the palliative care team, which is a separate service within the hospital. . . We’re trying very, very hard to improve the working between the two teams . . . But I have to say that’s a new thing . . . certainly not the standard. (Doctor 05-79, Children’s Principal Treatment Centre)
Additionally, system-level barriers further hindered information sharing between teams via electronic systems, leaving palliative care teams with limited information.
I [palliative care consultant] can’t access the PICU (Paediatric intensive care unit) records because there’s a whole different database that I’m not allowed access to, so I haven’t got a clue about patients within my own hospital. (Doctor 19-134, Paediatric intensive care unit)
The implications of not using a joint approach were illustrated in one example as a palliative care consultant discussed the impact of not having team discussions prior to speaking with families. Families’ expectations were then misaligned due to professionals not consulting one another before delivering news.
One family were almost crushed because I had painted such a bleak picture because they had been told [that their child was] in the morning doing really well, were coming off the ventilator. It’s very much about communication, everyone saying the similar kind of things, I felt like I was very much bad cop (Doctor 19-134, Paediatric intensive care unit)
Late referral to palliative care teams and hospices meant families were reluctant to involve an external team that was considered ‘new’. Professionals believed that this impacted decision making as some families did not engage with hospices due to not building a relationship prior.
A lot of them [parents and children] prefer to stay in the hospital if they’ve been with us a long time as well because they know our staff and they just feel like they don’t want to go to a hospice . . . when it’s people they don’t know. (Occupational Therapist 05-120, Neonatal intensive care unit)
Subtheme 1.3: Planning ahead
To prevent issues raised in the previous subtheme, all settings mentioned formalised methods to plan ahead for example, Advance Care Planning. However, their completion varied. In some units, there was formal process to record discussions. For others, planning was undertaken in a much more informal way, through a series of conversations, sometimes established without a written plan.
The flexibility of those things and that it’s not I suppose strictly speaking like a classic one-off conversation . . . it’s almost like a dance that happens over many, many weeks or even months. (Social worker 14-148, Children’s Principal Treatment Centre)
Although emphasis was placed upon planning ahead using Advance Care Planning, some healthcare professionals reported inconsistent use.
There are consultants out there who will absolutely always come in for an ACP document to start having those conversations and to start them, but I think there’s a few that still need a bit of a nudge. (Nurse 02-25, Paediatric intensive care unit)
Another reasoning for inconsistent use was due to families holding onto the possibility of life-saving treatment, this could prevent professionals from planning ahead.
There’s not a huge amount of discussion in terms of ACPs . . . there’s always the silver bullets of surgery or “We can do this and we can try that” (Nurse 10-33, Paediatric intensive care unit)
If incomplete, this had implications for colleagues, particularly for paediatric intensive care professionals, as patients would be admitted to their unit without an Advance Care Plan. On some occasions, patients would be admitted from outside of the area, making this more difficult.
When we have families that are from all over the country who may or may not know whether they’ve got an ACP . . . We’re in a very challenging position of whether we approach that family, and often we do talk about end-of-life care and parallel planning but it’s difficult for them to then engage with us because they see it as an acute illness (Nurse 19-138, Paediatric intensive care unit)
Paediatric intensive care professionals believed that initiating plans was not part of their role as it should have been initiated sooner in a child’s, prior to admission and better suited to usual care teams. However, when a child was admitted without an advance care plan, these professionals found this particularly challenging.
We’re not generally the ones that write the Advance Care Plans. . . The Intensive Care Consultants don’t write them. We complain that they haven’t been written but we write don’t them. (Doctor 09-104, Paediatric intensive care unit)
The setting and deterioration of the child upon admission was thought to impact families’ wellbeing, often provoking an emotional response from professionals. They then felt it inappropriate to burden families with decision-making. Professionals were also concerned that children were unable to advocate for themselves as they were often ventilated, emphasising the importance of early discussions.
Once they’re on PICU (Paediatric intensive care unit), in my experience 99.9% of the children, they’re intubated and ventilated and they do not have the power of their voice . . . So, again, these discussions need to occur before they arrive with us. (Nurse 04-40, Paediatric intensive care unit)
Theme 2: What we want to provide versus what we can provide
Subtheme 2.1: Providing choice
In all settings, professionals emphasised the importance of offering choice in relation to the location of end-of-life care. This was valued by professionals and thought to be part of providing holistic care.
It’s all part of it, if they choose to have their end of life treatment here that’s absolutely fine. Yes, if they want to be in a hospice or want to be at home that’s also fine . . . It’s looking after the entire patient journey. (Doctor 05-75, Teenage and Young Adult Principal Treatment Centre)
While clinicians aimed to provide choice for most families, availability of some options was dependent on capacity and acute clinical change. In one of the cancer units, current pressures meant professionals struggled to offer families and patients the option to stay on the ward.
One of the big challenges that we’re certainly facing now from a hospital perspective is offering families choice if they don’t wish to die at home [because of] all the issues around capacity and pressures on service. (Nurse 07-11, Teenage and Young Adult Principal Treatment Centre)
Resources required to plan for end-of-life care outside of the ward were also time-consuming as professionals admitted to sometimes not having capacity to consider it as an option, or to omitting some key component of planning that might have made it possible.
It takes a lot of resource as well . . . to move an acutely unwell baby to a hospice or to home and to then be able to provide the support that they need, especially at home, if that child’s not going to die quickly. . . takes a lot of time. There’s a lot of admin involved . . . that might put some people off. (Doctor 04-85, Neonatal intensive care unit)
The risks of forgetting a key planning component were increased by the lack of standardised guidelines and procedures. Equally, some units had relatively limited connections with hospices, making it difficult to develop or implement integrated guidelines and procedures.
There are lots of hospitals throughout the country who have much stronger links with hospices compared to us. (Nurse 09-160, Neonatal intensive care unit)
Hospices themselves were constrained by capacity, meaning transfers were not always possible at short notice. Similarly, professionals working in cancer units identified that community provision was variable, with 24-h being unavailable in some areas meaning that providing parental choice was not always an option.
I’m referring specifically to community nursing input . . .and facilitating 24-hour care in the home, which is what we aspire to for many of our families, and that can be a real challenge . . . Some regions are better resourced than others. (Doctor 14-144, Children’s Principal Treatment Centre)
Subtheme 2.2: Space and time to be a family
In all settings, professionals perceived privacy and time as important factors in compassionately supporting a family and allowing parents space to fulfill their role, and understood the importance of getting it right.
Giving somebody a good death is like the one thing I always think that I want to do right because you’ve got one shot at it, you can’t re-choose how you go about the end, you can’t change how you do something. (Nurse 02-29, Paediatric intensive care unit)
There were distinct differences in the facilities available between the setting types. Those receiving care in neonatal intensive care units were often offered private rooms or some form of accommodation onsite or close to the hospital. Providing families with the opportunity to continue parenting after death could be facilitated as many neonatal intensive care units also had a dedicated bereavement suite.
The charity came and done up for us . . . a room with like a couch, a fridge, a telly and we put the Moses’ basket usually in there with a cuddle cot (Occupational Therapist 05-120, Neonatal intensive care unit)
However, most of these settings did not have access to dedicated end-of-life care or bereavement suites. In paediatric intensive care units and cancer settings, restrictions on space and/or staff often limited parents’ ability to spend time with their child, and end-of-life care was usually delivered on the ward. This left majority of professionals feeling constrained by their environments as restrictions meant that it was more difficult to transfer patients elsewhere.
If there’s not the nursing staff or the cubicle space to move these patients, then they end up dying in the middle of a busy bay with the curtains pulled round. (Nurse 04-40, Paediatric intensive care unit)
Rooms set aside for this purpose were often deemed unsuitable by professionals, who found themselves having to make the best of their environment to provide parents with comfort and privacy. However, this was time consuming and challenging for professionals.
It’s really, really challenging. We’ve got very little space. We’ve got no space away from other families. We find the environment is probably the biggest challenge. The [name of room}, it’s not specifically for end-of-life care so we have to make sure it looks appropriate. . .we’re constantly moving furniture, changing things (Nurse 09-160, Neonatal intensive care unit)
Some professionals felt as though they were failing families by not providing a suitable environment and had made attempts to secure necessary funding but felt that end of life facilities was not a priority. As a result, many units relied heavily on charities or fundraising for dedicated bereavement suites from bereaved parents to improve the environment.
We’ve tried and tried to get more space and a new unit, basically, but we’re fighting with other areas of the NHS who also need more funding. (Nurse 09-160, Neonatal intensive care unit)
Subtheme 2.3: Supporting parents during end-of-life care and beyond
All settings had some form of bereavement support, ranging from a bereavement lead, social worker, support coordinator or psychologist. Some units provided debrief conversations that gave families the opportunity to gain a degree of closure, ask questions and find out more information. Sometimes, these were proactively offered at specific time points, rather than reactively responding to families. Whereas other units worked more flexibly, dependent on a family’s needs.
The neonatal consultant would usually offer a bereavement appointment six to eight weeks after the baby’s passed away. (Doctor 06-67, Neonatal intensive care unit)
All settings used bereavement packs, including information about funeral planning and charity organisations, with some sending out personalised cards to notify families of memorial services.
It has information that covers things like how to organise a funeral and it will have a leaflet from the children’s hospital about what’s available to them after the death of a baby (Doctor 04-89, Neonatal intensive care unit)
While professionals acknowledged the importance of bereavement support, in practice it was typically severely constrained. Support was often limited to office hours or the period just prior to or after death, and/or were reliant solely on one individual.
It’s striking that the department and the hospital itself is dependent on one individual [referring to bereavement nurse], as [it] is for many other things and it’s absolutely crucial that that we expand that role. (Doctor 04-46, Paediatric intensive care unit)
All units in this study heavily relied on the third sector for bereavement support but acknowledged that such fragmented bereavement support services had a direct impact on professionals. They expressed feelings of guilt and wanted to improve their services, yet were constrained by the system.
We give good end-of-life care and then they die and they get nothing and that just feels terrible, but I can’t fix it myself, you know, we can’t fix it [referring to bereavement support] (Doctor 04-85, Neonatal intensive care unit)
Theme 3: Workforce and sustainability: Healthcare professional support
Professionals reflected upon the positive impacts of providing end-of-life care, with all recognising the value. Many viewed it as a privilege and understood the importance of helping to create meaningful memories for families.
We’ve had the privilege of being able to arrange weddings in the hospital . . . for the young people and their families to allow us to be part of that is a total privilege. (Nurse 05-70, Teenage and Young Adult Principal Treatment Centre)
Despite its rewarding nature, providing this type of care was emotionally difficult and left some professionals questioning the long-term impact on their well-being. This was worsened by staff shortages and limited resource added to the difficulty of providing this type of care.
We could potentially have an end of life in [location 1] and an end of life in [location 2] and there could potentially only be three of us around . . . The impact that then has on us as a Team . . . we’re physically exhausted, we’re emotionally exhausted because we’re giving as much as we can (Nurse 07-14, Teenage and Young Adult Principal Treatment Centre)
While the need to support staff was recognised in all settings this took different forms, including charity funded counselling, debriefs and psychologist support. Despite this, pressures relating to clinical demands and staff shortages meant that professionals were often unable to access support due to time restrictions. This was further illustrated by one unit where a new role had been established to improve professional wellbeing. However, clinical demands and limited capacity meant it was not possible in practice.
[I was given a role to] try and do something about . . . wellbeing, but because we’ve been so short-staffed and there’s no money, we can’t release anyone clinically to go and do anything and we can’t pay for anything either. (Nurse 03-116, Paediatric intensive care unit)
This was concerning as professionals recognised the long-term impact on their wellbeing of providing this care, worsened by external pressures and limited investment in support available. However, external pressures and limited investment in available support meant professionals believed they were unable to support staff in comparison to previous years.
That’s one of my biggest concerns really is that we’ve got this very difficult patient population, we’ve got just a difficult job with high trauma as it is and actually we’re even less able to support staff than we have been in the past because we’re all so fraught and it takes its toll. (Nurse 03-116, Paediatric intensive care unit)
To help manage their wellbeing, some professionals found themselves supressing their feelings. Ultimately, professionals across all settings were left feeling that this was an area requiring investment to better improve their own wellbeing and to prevent long-lasting implications.
We do not deal with any of this stuff and have got very minimal professional support even though the hospital genuinely is trying to get better at it . . . So, I kind of lock it away in a box and then we have to go through these things in horrible, horrible detail again in our mortality reviews . . . it’s kind of like picking the scab off (Doctor 12-158, Neonatal Intensive Care Unit)
Discussion
Main findings
Our study has gathered experiences of professionals working in environments who care for large numbers of infants, children and young people at the end of life. High societal expectations, and perceived lack of readiness on the part of parents and professionals to consider a palliative care approach, both adversely impacted on the provision of end-of-life care. Professionals acknowledged the tensions between curative and palliative care approaches across all settings. Parallel planning (anticipating and planning for both improvement and deterioration simultaneously) was not always considered. Despite recognition of the importance of palliative care teams, referrals were inconsistent due to system constraints, differing perceptions of their role, lack of professional readiness and perceived parental preferences for active treatment. This meant that there was not always a joint approach between palliative care and other paediatric services.
Professionals acknowledged and understood the quality of end-of-life care that should be provided, but were constrained by their workload, time pressures and differing perceptions of who was responsible for initiating conversations about the changing focus of management and care. Although it was seen as a privilege, providing end-of-life care had a heavy emotional impact on professionals, worsened by the limited availability and accessibility of formal support and training.
What this study adds?
This study provides the first United Kingdom wide picture of many hidden features and elements of palliative and end-of-life care from the experiences of those providing care across various settings. It provides an understanding of the context within which this type of care is delivered, 31 identifies key issues regarding care delivery, which were not previously known, and highlights those which still remain an issue, despite prior evidence for them. This picture reveals many professional, personal and organisational barriers to delivering optimal care that have not been fully articulated before. Many of these issues could be resolved by investment including funding, time to provide high-quality care and education surrounding end-of-life care.
In line with previous studies,32,33 our study has shown that professionals experience discomfort when introducing aspects of palliative and end-of-life care concepts, including Advance Care Planning. That is exacerbated by a lack of confidence and the time it may take in facilitating complex discussions. There have been attempts to ease discomfort and promote effective communication by designing a prompt list. 34 By not initiating such conversations and differing perceptions of their roles, in our study, it was not always clear which clinician was responsible for initiating or facilitating such sensitive discussions, meaning that by default it sometimes fell to intensivists. Some intensive care professionals have suggested that such conversations should usually take place prior to admission to intensive care settings.35,36
Early referral to specialist palliative care services are being reported to be beneficial in providing support and pain management.35,37 Despite previous awareness of this, our study found a lack of perceived readiness and system constraints meant this varied in practice. 34 Previous research has shown that professionals tend to understand palliative care services as only providing end-of-life care. 14 Our study echoes this and found for those working in cancer settings, it risked diminishing hope, illustrating clinician discomfort in using the term palliative. 38 This highlights that there is still a lack of awareness and a need to improve understanding of and attitudes towards paediatric palliative care through education.
Professionals understood the importance of high-quality end-of-life care such as providing choices relating to location of care 39 and environmental changes to enable privacy. Previous work 40 has found parents’ ability to spend time with their child after death, using cooling mattresses and other facilities, was found to be meaningful. Despite this, our study found that while most neonatal settings had bereavement spaces, paediatric intensive care settings often did not. Those working in neonatal and paediatric care settings battled time and capacity constraints with one cancer setting struggling to offer to remain on the ward and flagged variable and sometimes poor community provision. Professionals also experienced constraints surrounding bereavement support for parents upon leaving the acute site, an issue that problematic as previous work 41 has emphasised the bereavement process as ongoing as some struggle to adapt to their new reality.
An inability to provide a dignified death and lack of multidisciplinary working has been shown to create moral distress for paediatric intensive care professionals, leading to poor well-being. 42 Our findings echo this, clearing highlighting an emotional impact of professionals’ inability to always provide high quality end-of-life care. This was despite accessible professional support being identified as a historical problem, further exacerbated by COVID-19 pressures43,44 and calls emphasising the importance of supporting professional wellbeing,45,46 our study illustrated that the majority of professionals remain unsupported.
Strengths and limitations
This is the largest and a rigorously conducted United Kingdom-based study on end-of-life care for infants and children, conducted during a challenging time for the National Health Service. Our recruitment through clinical leads means some professionals may not have had the opportunity to participate however, we had good representation across professions and a range of levels of experience of providing end-of-life care. We acknowledge that our sample reflects a larger number of professionals from paediatric intensive care units. However, there are large numbers of this type of setting across the United Kingdom and we needed to ensure we captured all variations in provision.
Implications for practice
Systems and processes that are limiting the delivery of high-quality end-of-life care for infants and children need urgent attention from policy makers. Professionals have been described as lacking confidence in delivering aspects of end of life care, therefore training should be a priority across paediatric clinical teams. 12 Professionals require prioritisation to develop robust well-being services. Future practice should determine necessary funding to improve end-of-life and bereavement facilities. 8
Conclusion
Healthcare professionals were aware of what constitutes high-quality paediatric end-of-life care, but delivery was constrained by the system, perceived parental readiness, low confidence levels and wider societal expectations. This illustrates that the current system is not suitable, despite the rising number of children requiring palliative and end-of-life care. Many of these issues could be resolved by investment, including funding, time to provide high-quality care and better professional support, as increasingly complex care is needed.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163251320204 – Supplemental material for Healthcare professionals’ perspectives of providing end-of-life care for infants, children and young people in acute settings: A multi-site qualitative study
Supplemental material, sj-docx-1-pmj-10.1177_02692163251320204 for Healthcare professionals’ perspectives of providing end-of-life care for infants, children and young people in acute settings: A multi-site qualitative study by Emma Victoria McLorie, Julia Hackett, Laura Barrett, George Peat, Helen Weatherly, Sebastian Hinde, Gabriella Walker, Jane Noyes, Sam Oddie, Chakrapani Vasudevan, Richard G. Feltbower, Bob Phillips, Catherine Hewitt, Richard Hain, Gayathri Subramanian, Andrew Haynes, Andrew Papworth, Lorna Katharine Fraser and Fliss E.M. Murtagh in Palliative Medicine
Footnotes
Acknowledgements
Thank you to all PIs, our PPI board for their valuable input and to all participants.
Author contributions
LKF designed the study managed by JH. EVM, LB, AP, GP and JH conducted data collection. EVM and JH led the analysis and drafting the manuscript. GP, LB, FM and LKF contributed to the analysis. JH, LKF and FM provided extensive feedback on manuscript drafts. All authors approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the United Kingdom National Institute for Health and Care Research (NIHR), Health Services and Delivery (REF: NIHR129213). LKF, FM and CH are NIHR Senior Investigators. The views expressed in this article are those of the author(s) and not necessarily those of the NIHR, or the Department of Health and Social Care.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.