
Abstract
Background:
End-of-life care for children with life-shortening conditions is provided in a range of settings including hospital, hospice and home. What home-based, end-of-life care should entail or what best practice might look like is not widely reported, particularly from the perspective of parents who experienced the death of a child at home.
Aim:
To explore the value and assess the effectiveness of an innovative model of care providing home-based, end-of-life care as perceived by families who accessed the service.
Design:
A qualitative descriptive study design was employed with in-depth semi-structured interviews conducted with bereaved parents.
Setting/participants:
Thirteen bereaved parents of 10 children supported by the home-based end-of-life care service.
Results:
Parents reported effective aspects of end-of-life care provided at home to include: (1) ability to facilitate changes in preferred place of death; (2) trusted relationships with care providers who really know the child and family; (3) provision of child and family-centred care; (4) specialist care and support provided by the service as and when needed; and (5) quality and compassionate death and bereavement care. Parents proposed recommendations for future home-based end-of-life care including shared learning, improving access to home-based care for other families and dispelling hospice myths.
Conclusion:
Parents with experience of caring for a dying child at home offer valuable input to future the policy and practice surrounding effective home-based, end-of-life care for children. New models of care or service developments should consider the key components and attributes for effective home-based end-of-life identified by bereaved parents in this study.
A family’s decision to have their child at home to die is dependent on the availability of appropriate and specialist palliative care services.
Much of the published evidence on end-of-life care at home focuses on children with oncology diagnoses with little evidence on children with other life-shortening conditions.
Addresses a gap in the evidence by providing an in-depth account of parents’ experiences of caring for a dying child at home, supported by an innovative model of care involving a partnership between a children’s hospice, hospital and community nursing team.
Highlights the five key elements of effective home-based end-of-life care identified by parents.
Recognises the need for services to maintain a degree of flexibility and responsiveness, allowing families who choose to be at home to remain there are long as possible yet be in a position to modify settings should there be a change in child’s care requirements or family circumstances. The value parents placed on this flexibility was emphasised.
Findings from this study have international relevance and can inform future development of models of care, services or programmes designed to support effective end-of-life care at home for families of children of all ages and with a range of life-shortening conditions.
New models of care or service developments should consider the key components and attributes for effective home-based end-of-life identified by bereaved parents in this study.
Introduction
The importance of paediatric palliative and end-of-life care being provided in line with the wishes of children and families is a key component of national policy within the United Kingdom (UK)1–3 and advocated by leading children’s palliative care organisations in Europe and beyond.4,5 This includes choice over the setting where end-of-life care is delivered. The current evidence base indicates that the proportion of hospital deaths remain higher than those in a children’s hospice or at home for children with life-shortening conditions.6–8 There is growing international evidence to suggest that families wish to remain at home towards the end of their child’s life supported by specialist palliative care professionals.9,10 Moreover, when specialist palliative care services are available to support death and dying at home, the prevalence of deaths in this setting increase.11–14
Whilst appropriate resources, infrastructure and services need to be in place to deliver end-of-life care at home, what provisions for end-of-life care of children within this setting should entail or what examples of best practice might look like is not well documented. Parents’ views of what effective home-based end-of-life care for children should entail is limited, yet such evidence is key to inform future service planning and provision. A systematic review of family experiences of receiving palliative care at home concluded that one of the main challenges faced by families was the lack of support from adequately skilled staff with appropriate palliative care experience. 9 Our study aims to address this gap in the evidence by providing insight into and reflecting on the experiences of bereaved parents who accessed an end-of-life care service to allow their child to die at home in line with their wishes.
Methods
Research question
What are families’ experiences of caring for their child at the end-of-life and through death with the support of a bespoke home-based specialist palliative care service?
Design
A qualitative descriptive study design was employed with in-depth semi-structured interviews conducted with bereaved parents. Reporting followed the consolidated criteria for reporting qualitative studies (COREQ) guidelines. 15 The findings from this study were used as part of the evidence gathered to support development of an initial programme theory for a realist evaluation of the full Care 24 Lothian service which will be reported separately to keep the focus of this paper on the family experience.
Setting
The study was set within Lothian, Scotland which comprises a geographical area of approximately 700 square miles and falls under the NHS Lothian Health Board. Latest available population estimates calculated 177,000 children aged 0–18 years living in this area (National Records ref). 16 Applying a prevalence rate of 47.2:10,000 17 indicates that there are 835 children with a life-shortening condition within the NHS Lothian boundaries who are likely to require input from palliative care services at some point over the trajectory of their illness. For families residing in this area, whose child has reached the end-of-life stage and their wish is for their child to die at home, a referral to the Care 24 Lothian service can be made. A detailed description of this service is provided in Box 1.
Box 1. Description of the Care 24 Lothian service
Care 24 Lothian, which came into operation in 2014, is the first and currently only formalised home-based, end-of-life care service in Scotland. It is a partnership service between the NHS and Children’s Hospices Across Scotland (CHAS) that provides end-of-life care for child and young people (aged 0–16) recognised as having reached the end-of-life stage, who have chosen delivery of care to be at home during this time. The service was designed to be responsive and quickly implemented when a child was recognised to be nearing end-of-life and then stepped down appropriately should the child’s condition stabilise or following their death.
Care 24 Lothian is a nurse-led service, supported by medical input as required, which ensures families have access to 24-h direct nursing care delivery, advice and support during their child’s end-of-life stage and following death. It aims to offer an expert level of care within the home in a way that is family-led and family oriented. Home visits typically include care assessment and planning, medication and symptom management, teaching and education, memory making interventions and psychosocial support.
Once a family has been referred to the service, a Lead Professional, whose is normally a registered nurse, is appointed to manage the process. Their role involves being a single point of contact for the family and ensuring effective coordination and provision of care. Ongoing care is then delivered primarily by the Community Children’s Nursing service, or Paediatric Oncology Outreach Nurses (POON) for children with an oncology diagnosis, during the hours of 08:00 until 18:00 and by the children’s hospice nursing team from 18:00 until 08:00. Additional key providers of the service include a Clinical Nurse Specialist in paediatric palliative care, the child’s lead medical clinician and the wider hospice care team. The intended outcomes for the service are to provide consistent, high quality care and support to families via staff with the appropriate knowledge and expertise and to ensure families have choice over their preferred place of care at their child’s end-of-life.
Population and sampling
A purposive sample of all bereaved parents who met the inclusion criteria according to the records held by CHAS and NHS Lothian were invited to take part in the study. Inclusion criteria were: parents of a child who received end-of-life care from Care 24 Lothian from the date of its inception (November 2014) to the study’s commencement date (December 2018); adult family member (⩾18 years of age); minimum of 4 months post-bereavement; and able to consent to participate.
Recruitment
Given the time that may have passed from use of the service for some parents, a member of the Care 24 Lothian team who had a relationship with the parents contacted them to inform them of the study and requested permission to send them an invitation which was then sent out by the hospice team. Following consideration of the study, parents returned an ‘Agreement to Participate’ form to the project team if they wished to take part. Contact was then made with parents to discuss the study and arrange a date, time and place for the interview.
Nineteen families received care from the service during the timeframe, all of whom met the inclusion criteria. Ten positive responses were received which led to interviews. Five additional families agreed to receive an invitation pack but did not reply. Two families declined to participate with no reason given. The remaining two families were uncontactable as the contact details held were no longer valid.
Data collection
A semi-structured interview topic guide was devised to explore parents’ experiences of and reflections on receiving end-of-life care for their child at home. The topic guide was reviewed by the steering group, including parent representatives, and was considered broad enough to address the key questions posed within the service evaluation, whilst remaining flexible enough to incorporate new areas of discussion as initiated by the participants. Topics included planning for and introduction to the service; experiences of receiving end-of-life care at home; bereavement care support; and recommendations for future home-based end-of-life care (Online Appendix). Interviews were conducted by an experienced qualitative researcher with expertise in paediatric palliative care (CM). Reflective field notes were made following each interview.
Data analysis
Interviews were audio recorded, transcribed verbatim and anonymised before transcripts were uploaded to QSR NVivo 12 data management software. Analysis focused on how parents describe and make sense of their experience of the service using the thematic framework approach (Table 1). 18 This approach to data analysis has been used widely in qualitative research and is particularly suited to comparing and contrasting interview data themes both within and between participants or ‘cases’. 19 Whilst primarily adopting a deductive approach, guided by the research questions, we also remained open to new themes emerging from the data.
Stages of the thematic framework approach.
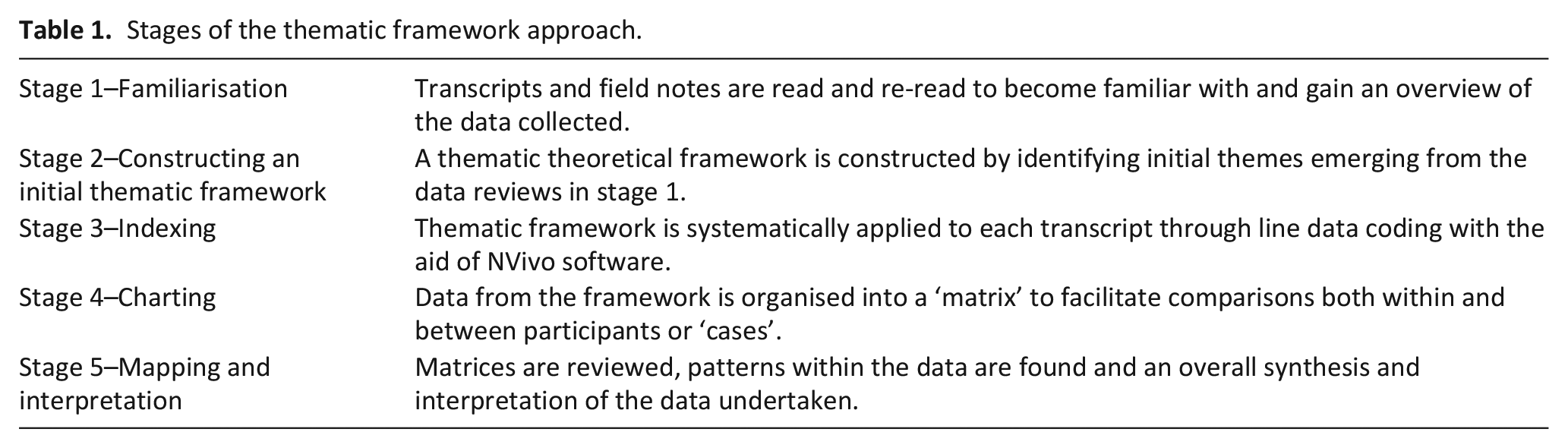
Relevant measures were taken to enhance rigour and reliability of the data. CM led the analysis and both CM and CT (project research assistant) undertook independent analysis of the interview transcripts. They met regularly to discuss and debate emerging themes and topics. The wider research team (CM, CT, KK) reviewed the final themes to reach consensus in the mapping and interpretation of the data, thus enhancing rigour and trustworthiness.
Ethics approval and ethical considerations
The study was approved by the School of Health and Social Care Research Integrity Committee, Edinburgh Napier University. Informed written consent was obtained prior to interview. Participants were offered a supportive follow-up telephone call by the hospice family support team and signposted to appropriate bereavement charities for any additional support required following the interview.
Results
Semi-structured interviews were conducted with 13 bereaved parents of 10 children. All interviews were undertaken in the family’s home between the months of February and July 2019. Interviews lasted between 30 and 73 min. Children who received the service had a range of life-threatening conditions including four with non-oncology diagnoses. The length of service use ranged from 1 to 38 days, reflecting the variable nature of children’s end-of-life care and need for rapid or sustained support in some cases. Characteristics of parents and children are outlined in Table 2.
Characteristics of bereaved parents and their children.
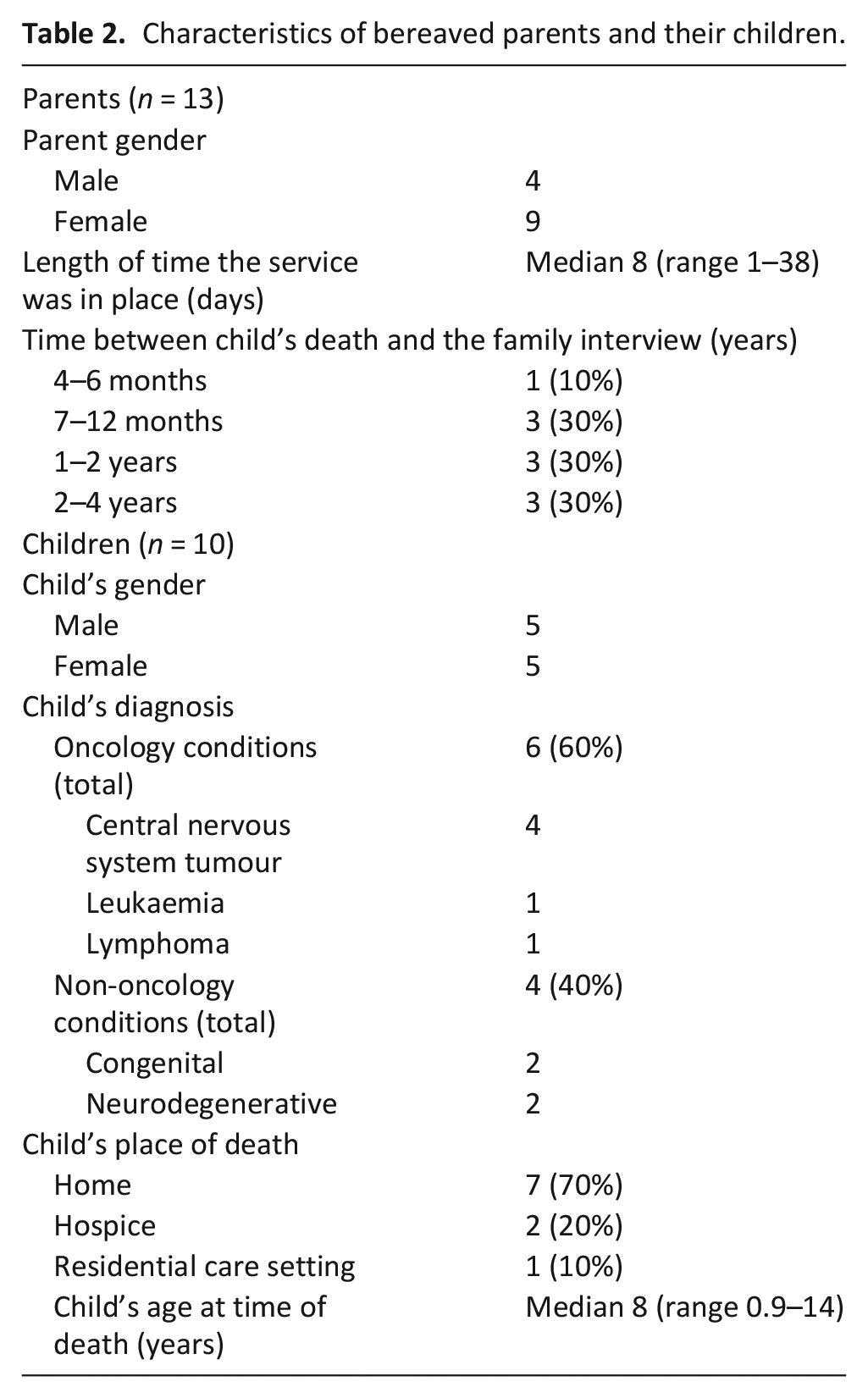
Five major themes were identified in the data relating to key aspects needed to deliver effective end-of-life care and support, and three themes encompassing recommendations for enhancing home-based end-of-life care in future. Representative quotations were presented to illustrate participants’ perspectives and experiences with unique IDs to ensure confidentiality.
Effective end-of-life care
Theme 1: Facilitating preferred place of death
Parents provided eloquent accounts of the overall impact the service had on them as a family. Its value in enabling families to remain at home for their child’s end-of-life care and death, with high quality and compassionate care and support provided by professionals, was the principal message:
I think the whole support at home was amazing. I think it would have been so much more different for me and my grief if [Child] died in hospital and we hadn’t been given that choice, or in the hospice. Now I know some people choose to take their child into hospital and I know some people choose to take them to the hospice and that’s absolutely fine but I think where I’m probably getting at is the fact that we had that choice and I will forever be grateful for that, and the support that we were given to put that in place. (Family 6)
For two families, changes in their child’s care needs and family circumstances meant home was no longer the optimal setting for end-of-life care. The service effectively facilitated a change in place of care, giving families the opportunity to remain at home for as long as possible. This was articulated by one parent:
We wanted to stay at home as long as possible. We didn’t like the idea of the hospice, but by the end we changed our mind and they were really flexible with it. We were able to change plans at the last minute and get us transferred along to [hospice]. (Family 5)
Home means different things to different families. For example, children with complex care needs and life-shortening conditions might receive long-term or respite within community residential care settings. Over time, children and families develop relationships with the care team and recognise the residential care setting as another ‘home’. This was the case for one family and the service, through expertise of their nursing and medical team, were able to support both the family and care team to deliver end-of-life care in this setting. Enabling the child and family to remain in the residential care centre would not have been possible without the input of Care 24 Lothian since the residential care team do not have the required expertise to provide palliative and end-of-life care.
Theme 2: Trusted relationships between care provider, child and family
Children and families developing relationships with the Care 24 Lothian staff was reported by parents as key to the delivery of effective care. Parents acknowledged that it takes time to develop close and trusting relationships with care providers, but such relationships are an essential aspect of effective end-of-life care. One parent shared the significance of the care team really ‘knowing’ the child as being especially supportive when providing care at the end-of-life:
From a mum’s point of view, you want people who know your child. It doesn’t feel as. . .as supportive, I guess. It feels supportive but not the same, it’s not the same as someone who you know caring for your child. (Family 2)
Parents spoke about the importance of consistency in the immediate team around the child, particularly the nursing staff, explaining how this facilitated the development of ongoing and trusted therapeutic relationships and the delivery of effective and quality care. These distinctive relationships between the family and nurses were important across the duration in which the service supported families but especially poignant at the intimate and personal time of the child’s death. In cases where a known staff member was with the family for the child’s death or to provide after-death care, this was acknowledged as being more effective than if the staff present did not know the family well:
Yeah, I couldn’t have asked for two better nurses to come in that day and my GP as well, the three of them were just. . .the three of them were amazing.
No strangers or, you know.
And they knew [Child], you know, they had got to know [Child], that’s the other thing, yeah, If somebody had been on holiday or. . .
That would have been a disaster.
Yeah, I think for us that would have changed the whole six months. (Family 8)
Theme 3: Provision of child and family-centred care
The child and family-centred approach adopted by the service was regarded by many parents as a valued feature. Parents acknowledged how the service enabled them to care for their child at the final stages of life and to remain together as a family in their own home with the presence of nurses with specialist palliative care experience as required. Parents described how care provided by the service was centred around the wishes of the child and family at all times, informed by ongoing conversations and supported decision-making:
I feel they were as interested in us, in our emotional needs and just making sure that we were getting what we wanted out of this, do you know what I mean, rather than coming in and saying ‘we need to do this, this and this’ it was very much ‘okay, this is what we can do, what do you want [Child], what do you want [Parent]?’ and at every single step of the way they were so respectful of, you know, if [Child] wanted whatever, [Child] got whatever, if I asked them about something they were there in a flash, you know. (Family 6)
Professionals and the team around the child helped parents to identify and articulate their preferences for home-based end-of-life care, in line with advance care planning processes. Parents felt that any fears and insecurities related to what end of life might look like for their child were listened to and addressed. They were reassured that preferences regarding end-of-life care may evolve over time in response to their child’s changing condition and that the family and care team would review their situation on a continual basis.
The service encouraged parents to preserve their role as being ‘parents’, continuing to make memories and spend the remaining time they had being together as a family. This involved balancing their parenting roles with the provision of clinical care. Parents commented on the importance of having positive memories of being with their child at the end-of-life and not solely being the provider of clinical care. Parents deemed the service as effective in ensuring families were not over-burdened with caregiving demands. The team recognised when parents were struggling and exhausted, identifying ways in which they could provide parents with respite and additional support. For example, community health support workers engaging in memory making activities with siblings.
Parents noted the discrete nature of the team and how they avoided being ‘intrusive’ whilst remaining present to deliver required end-of-life care:
We are quite private people and to have people in your house is quite, can be quite intrusive but they never made you feel like that did they?
No, they were just totally led by what we wanted. (Family 7)
Theme 4: Confidence in the care and support provided enabled families to remain at home
Parents recognised that an expert level of care was provided by a caring and compassionate team. The service provided them with both the confidence and security that staff with a specialist level of knowledge and skills in palliative and end-of-life care were available to the family as required. Having this level of support in place and easily accessible was considered essential for families to remain at home.
Parents also provided examples of how the service afforded a balance between staff being in contact with families and allowing them the time and space to be together at the end-of-life without the presence of a clinical care team:
They would text in the morning and say ‘do you want a phone call or visit?’ and they were never intrusive either that’s what I really felt, they were really led by us in terms of how much involvement we wanted them to have, so if we had said ‘we just want a family day today’ they would say ‘that’s absolutely fine but we’ve got the mobile on at all times if you change your mind.’ (Family 7)
Parents were cognisant of the considerable input and collaboration required between various agencies and professionals to deliver the service and commented on how effectively this was undertaken to support families to remain at home. Parents recognised and appreciated the planning and coordination that went on ‘behind the scenes’ to deliver the service. Care planning and organisation was coordinated without having to unnecessarily burden or involve families.
Having access to the service, any time of day or night, was highly valued by parents. A dedicated telephone number and single point of contact taking them directly to a team member who would be familiar with the family and their individualised care plan was regarded as essential in fostering parents’ confidence and security in being at home at the end-of-life.
Theme 5: Quality and compassionate death and bereavement care
The quality and perceived effectiveness of after-death and early bereavement care provided by the service was recognised by families. Families were encouraged to say good-bye to their child in the way they wanted, and the care team guided by the unique wishes and needs of each family. Parents commented on the empathy, respect and holistic care demonstrated by the nurses and suggested they went ‘above and beyond’ to support families. The need to have time, space, and privacy to be with and care for their child’s body following death was important and parents valued the sensitive and compassionate nature of the nurses who guided them through after death care.
Parents appreciated staff playing a key role in organising and preparing for the post-death and funeral arrangements, removing the burden from families to allow them to focus on their child and begin the grieving process. A number of parents recalled meeting with team members weeks and months following their child’s death and found it cathartic to reflect on the event. Bereavement care and support was important to families:
The staff providing this service are kind of like your family during that time, do you know what I mean? You’ve already lost your child so to lose that whole support network at the same time, and okay in our situation it was ten days from start to finish that we had these [nurses] in our lives, but we’d built up such a strong bond in that time, they were so good to [Child], they were so good to us, you know, and we really appreciated what they did and to me for them to have walked away and not had any further communication would have shown that it was a clinical thing rather than a real whole package, you know, psychosocial sort of support thing. I think it was lovely. (Family 6)
Parent recommendations for future home-based end-of-life care
Recommendation 1: Share learning from the experiences of other families
Parents who cared for a child at home at the end-of-life have individual perspectives and experiences to share which can inform service enhancements and development of resources to better support those accessing home-based end-of-life care in future.
Recommendation 2: Increase access to home-based end-of-life care service for other families
Parents provided accounts of conversations with other parents of children with life-shortening conditions regarding place of care and advised that a general lack of awareness around end-of-life care services exists. They emphasised the need for promoting the service to increase access for other families not aware that end-of-life care provided at home is an option:
I think parents have no idea that their child can stay at home. . .and I think they should know and it’s probably about how to approach someone and talk about end-of-life care. (Family 2)
Parents commented on the value of their child being able to remain at home after death with the support of equipment such as CuddleCots™ and cooling blankets. They acknowledged that not all families may choose to keep their child at home following death, the support that is available should be communicated so that families are aware of their options. Parents recognised challenges in engaging families in discussions about their child’s end-of-life but believed it to be essential in enhancing quality of care surrounding the death of a child.
Recommendation 3: Promote children’s hospice services and dispel existing myths
There was inconsistency amongst participants in how they viewed children’s hospices. As Care 24 Lothian is a joint service between the NHS and a children’s hospice, families had access to additional specialist care and respite offered by the hospice. However, some parents declined hospice services when offered, for example, a short respite break. These parents revealed how hospice care was not something they had considered or wanted for their child and several myths concerning hospice care prevailed, including hospices being yet another ‘clinical’ setting:
‘Cause even if we did choose to go to the hospice, it’s still a clinical environment no matter how many different disguises you put on it, it’s still a foreign environment.
It’s not your home. (Family 4)
For those parents who had initial preconceptions about hospice care but then went on to access support from the hospice during their child’s end-of-life phase, their perceptions of a children’s hospice and what it can offer to families altered significantly:
So at the time I didn’t want to go to the hospice but when I look back in hindsight it was the best thing for us. But I think I didn’t know any of this stuff existed and now that I’ve experienced it, it’s about trying to get across to other parents, if they’ll listen, that’s the thing, it’s whether they want to listen to it or not. (Family 10)
These accounts highlight that misconceptions about children’s hospice care continue to exist and could potentially interfere with families accessing care in this setting. Parents felt that whilst it is important to respect the view of families, it is also imperative to find ways to dispel these myths and preconceptions so families could benefit from the services available. Parents suggested ensuring children’s hospice staff were more visible within the service and not solely during out of hours, avoidance of the term ‘hospice’ referring to hospices as a supportive or respite care centre, and having bereaved parents speak to families about the positive impacts of the care they received from the hospice.
Discussion
Main findings
This paper communicates in-depth accounts of parents’ experiences of being at home for their child’s end-of-life care and death, with 24-h access to direct care, advice and support provided by a bespoke service and unique model of care. Parents described five key features of the care they received as being effective in facilitating the end-of-life care plans and wishes they had for their child. These included the ability to facilitate changes in preferred place of death should their situation require it; consistency in care providers who know the child and family and with whom they have built trusted relationships with; provision of child and family-centred care; specialist palliative care and support provided as and when needed; and quality and compassionate death and bereavement care. Several insightful suggestions for enhancing end-of-life care for other families, including raising awareness and improving access to existing services, were also put forward. It was highlighted that the term ‘hospice’ may be a barrier to some families accessing care from this joint service due to prevailing misconceptions and proposed using alternative terminology such as ‘supportive care’.
Strengths and limitations
This study provides detailed accounts of parents’ experiences of receiving home-based end-of-life care and presents a variety of perspectives, including both mothers and fathers of children who had died from a range of life-shortening conditions at different ages from infancy to early teenage years. Whilst the study has a relatively small sample, this is within the scope of qualitative research. 20 Limited information was gathered on the support needs of siblings as this was not the focus of the study but is a key area for future investigation. The retrospective nature of this study may introduce a potential for recall bias although studies have found that recalling the death of a child was not problematic for parents.21,22
We recognise limitations in the transferability of our findings since the care parents received was based in one health board area within Scotland and needs to be considered in the context of different heath care systems and models of care. However, our findings address a gap in the evidence base surrounding parents’ experiences of being at home for their child’s end-of-life and death and communicate key aspects of care and support which are deemed to be of value and effective in the provision of end-of-life care at home by parents which has international relevance for services.
What this study adds
Existing evidence on parents’ experiences of end-of-life care focuses mainly on children who died in hospital23–27 or children with a cancer diagnosis who died at home.28–30 Minimal evidence surrounding end-of-life care and death occurring at home for children with other life-shortening conditions exists. 31 Moreover, a recent review paper suggests considerable change is required to improve access to home-based end-of-life care and allow families of children with serious illnesses to die in their chosen location (Johnston et al. 2020). The authors propose the need for further research to identify innovative models of providing paediatric hospice and palliative care in the community (Johnston et al. 2020). Our study has done just this and provides original insights into what bereaved parents considered to be effective care which enabled them to achieve their wish of remaining at home for their child’s death.
The Care 24 Lothian service was put in place following a parent’s decision for their child to die at home and when their child was recognised as entering the end-of-life phase. An unintended, valued outcome for parents was the flexible and responsive approach to requested changes in care settings. In situations where it became apparent that home was not the most suitable setting for the child and family, the service was able to facilitate transfer to an alternative setting, namely a children’s hospice. Families were grateful for the opportunity to spend as much time as possible at home but recognised their need to move to a different setting prior to their child’s death. This concurs with a previous study 32 which suggests that parents being able to plan their child’s location of death may be more important, in terms of the quality of their experience, than the actual place of death. Future developments of home-based end-of-life care services should be mindful of potential changes in a family’s wishes or circumstances over the time and be in a position to facilitate prompt transfer to an alternative setting.
Parents valued the trusted relationships they built with those providing end-of-life care to their child and this resonated across interviews. The importance of developing relationships with care staff at such a personal and profoundly emotional time in their lives was central to effective care, along with consistency in the nurses providing that care. A potential challenge for those delivering home-based end-of-life care, is being able to form such relationships with families within what is often a very short timeframe between an end-of-life care plan being put in place and the child’s subsequent death. Moreover, having a small and dedicated team of nurses caring for the family at this time requires measures being in place to protect the emotional demands of this role on nursing staff.
A clear message emanating from this study was the need to preserve parents’ role as being ‘parents’ throughout the experience. Parents strived for a balance between administering clinical care and symptom management to their child and acting in their normal role of ‘mum’ or ‘dad’. The service was considered effective in enabling this, protecting parents from being overburdened and providing respite and support as required, maximising the quality time families spend together. Previous studies highlight how caring for a child at the end-of-life can lead to challenges in maintaining the fine balance between the role of being the child’s parent and being their main care provider.25,33,34 A comprehensive review recommends palliative care services providing end-of-life care examine current practices with respect to ensuring parents’ psychosocial needs as parents at their child’s end-of-life are met. 35 Whilst the review focused on end-of-life within hospital settings, the same principle can be applied to home as indicated in our findings.
Having confidence in those providing care was a key factor in enabling families to be at home. Parents were confident in and reassured by the expertise of the health care professionals delivering the service and in the compassionate and sensitive manner in which they responded to families’ needs. Having a single and consistent point of contact, in the form of a dedicated telephone number, which families could access at any time of the day or night and know that the person responding would be familiar with the child’s care needs and the family’s wishes was vital to parents. Two similar nurse-led services providing 24 access to care and symptom management for children with life-shortening conditions in their home are documented within the literature.36–39 Both services are based in England, UK and provide home-based palliative care, of which end-of-life care is one aspect of the service. An evaluation was undertaken, but unlike the current study, focused on questionnaire data as opposed to in-depth interviews with parents. However, there is consistency in how parents’ value these services, particularly, in having confidence in accessing specialist palliative care as and when required. This is a fundamental to enabling children to be cared for at home at their end-of-life.
Conclusion
This study makes a novel contribution to the evidence base surrounding provision of end-of-life care for children with life-shortening conditions at home. Parents reflected on and shared their experience of caring for their child at the end-of-life and after death with the support of a bespoke model of care providing 24-h access to specialist paediatric palliative care. They clearly articulated those elements of home-based care deemed to be effective and which enabled end-of-life care to be delivered in line with their wishes. Consideration of this evidence would be of value internationally in future planning of community-based palliative care services for children.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163211023300 – Supplemental material for What does effective end-of-life care at home for children look like? A qualitative interview study exploring the perspectives of bereaved parents
Supplemental material, sj-pdf-1-pmj-10.1177_02692163211023300 for What does effective end-of-life care at home for children look like? A qualitative interview study exploring the perspectives of bereaved parents by Cari Malcolm and Katherine Knighting in Palliative Medicine
Footnotes
Acknowledgements
The authors would like to extend our gratitude to the families participating in this project. They welcomed us into their homes and shared their very personal stories with us. Listening to their views and reflecting on their experiences will be influential in shaping end-of-life care and services moving forward. The authors would also like to thank their appointed research assistant, Charlotte Taylor, for her role in analysis of the interview data.
Author contributions
There are two main investigators/researchers and subsequent authors on this manuscript. Both (CM, KK) contributed to the conception and design and subsequently conducted the study. CM conducted all of the interviews and led the data analysis. KK contributed to the data analysis. CM led preparation of the draft manuscript and KK critically reviewed and contributed to each version. Both authors approved the final version of the manuscript prior to submission.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Children’s Hospices across Scotland (CHAS) and NHS Lothian.
Research ethics and patient consent
This study secured ethical approval from Edinburgh Napier University’s School of Health and Social Care Research Ethics Committee (SHSC/18004). Participants gave written informed consent after receiving both verbal and written information about the study. Participants were advised that they could end the interview at any time without reason or consequence.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.